Hypothyroidism affected almost 17% of patients with idiopathic pulmonary fibrosis and was independently associated with their mortality, according to a report in the September issue of CHEST.
“We report, to our knowledge for the first time, an association between hypothyroidism and idiopathic pulmonary fibrosis,” wrote Dr. Justin Oldham of the pulmonary and critical care section of the University of Chicago and his associates. “Hypothyroidism, a largely autoimmune process, is common among patients with IPF and may represent an additional feature of autoimmunity in this patient population.” The retrospective study could not assess causality, but raises questions about whether autoimmune abnormalities contribte to or exacerbate IPF, and whether hypothyroidism and IPF share common underlying causes, they added.
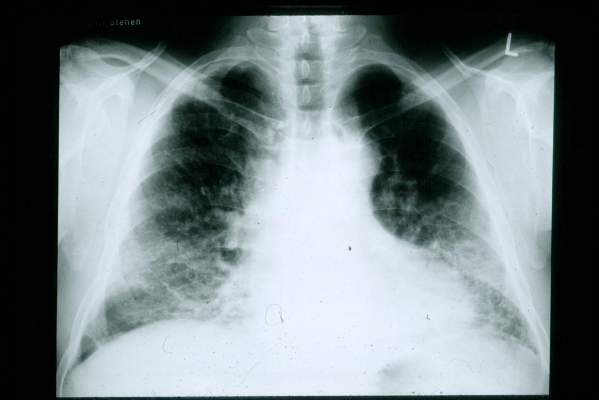 By IPFeditor (Wikimedia Commons)
By IPFeditor (Wikimedia Commons)
Scan shows lungs of patient suffering from idopathic pulmonary fibrosis.
Recent years have seen a “paradigm shift” away from immunologic or inflammatory causes of IPF in favor of alveolar injury and abnormal cellular repair mechanisms, but some studies point to autoimmunity in IPF, said the investigators. To further explore the question, they studied hypothyroidism – which in developed countries is most often autoimmune – among 196 patients with IPF with an equal number of age-and sex-matched controls with COPD (Chest 2015;148:692-700). Nearly 17% of IPF patients – including 13% of women and 28% of men – reported using thyroid replacement therapy with no history of thyroidectomy or radioactive iodine ablation. In contrast only 7% of COPD controls had a recorded diagnosis of hypothyroidism (odds ratio, 2.7; 95% confidence interval, 1.3 to 5.5; P = .01). Men and women with IPF and comorbid hypothyroidism had significantly shorter survival than did patients who had IPF only (P = .001). Hypothyroidism also independently predicted mortality in the multivariable analysis (hazard ratio, 2.1; 95% CI, 1.3 to 3.4), as did sequential increases in gender, age, and physiology (GAP) stage, the investigators said. “These conclusions held when transplant-free, transplant-excluded, and transplant-as-a-competing-event Cox regression models were constructed,” they reported. Furthermore, multivariable analyses of data from two IPF clinical trials (ACE-IPF and PANTHER) revealed similar associations among hypothyroidism, GAP stage, and mortality, they said.
Exactly how hypothyroidism contributes to IPF and IPF-related mortality is unclear, said Dr. Oldham and his associates. Because the study did not examine longitudinal changes in thyroid stage, they could not relate those trends to IPF progression, they noted. Although they excluded patients whose thyroid disease was known not to be autoimmune, they could not specifically confirm that all remaining patients with hypothyroidism had autoimmune thyroiditis, because most had been diagnosed years before. Future longitudinal studies should examine whether IPF and hypothyroidism share underlying causes, and should examine why hypothyroidism seems to increase IPF-related mortality, they concluded.
The National Institutes of Health funded the study. Dr. Oldham and five coauthors declared no competing interests. Senior author Dr. Imre Noth and one coauthor reported grant support and honoraria from NIH, Brystol-Myers Squibb, Gilead Sciences, Intermune, Medimmune, and several other pharmaceutical companies.