User login

The ASCVD Risk Estimator app is a mobile tool created to determine the 10-year and lifetime risk patients may have for developing atherosclerotic cardiovascular disease (ASCVD). Using the Pooled Cohort Equations and lifetime risk prediction tools, the app focuses on assessment of cardiovascular risk, lifestyle modifications to reduce cardiovascular risk, and management of elevated blood cholesterol and body weight in adults. The app is separated into 4 easy-to-use tabs: the estimator tool, clinician resources, patient resources, and clinical research results surrounding the development of treatment guidelines.
Estimator
The American College of Cardiology (ACC) and the American Heart Association (AHA) collaborated to create a short, 9-step calculator to estimate 10-year and lifetime risk for ASCVD. A patient’s basic health information is entered into the estimator (sex, age, race, total cholesterol, high-density lipoprotein cholesterol, systolic blood pressure, blood pressure lowering medication use, diabetes status, and smoking status) and within seconds, risk rates are output and treatment recommendations are made.
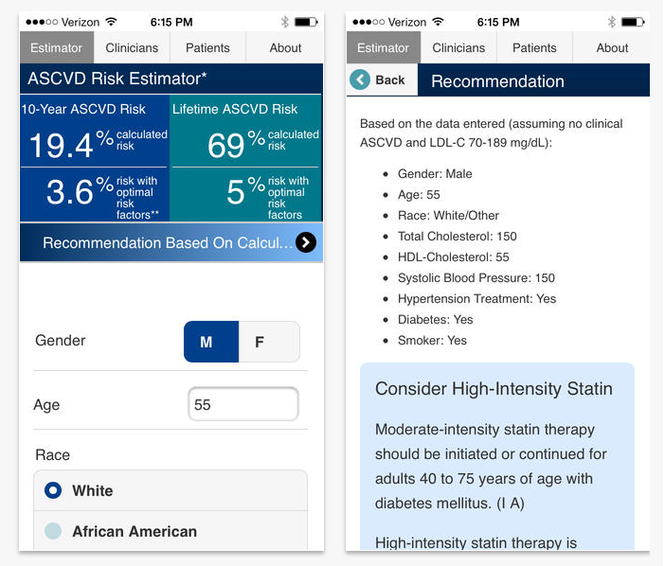
Treatment recommendations include statin and lifestyle guidance. No statins are recommended if the 10-year ASCVD risk is < 5%. Lifestyle guidance is provided regardless of the ASCVD risk rate, which includes eating a heart-healthy diet, getting regular aerobic exercise, maintaining a desirable body weight, and avoiding use of tobacco products.
The ACC and AHA recognize that factors other than the 9 estimator questions may exist for a patient and make it clear that the best way to proceed with the calculated output information is through clinician-patient discussion. They consider that factors such as primary low-density lipoprotein cholesterol of ≥ 160 mg/dL; other evidence of genetic hyperlipidemias; family history of premature ASCVD with onset at age < 55 years in a first-degree male relative or age < 65 years in a first-degree female relative; high-sensitivity C-reactive protein ≥ 2 mg/L; CAC score ≥ 300 Agatston units or ≥ 75 percentile for age, sex, and ethnicity, ankle-brachial index < 0.9; or elevated lifetime risk of ASCVD all need to be discussed and considered between the physician and the patient.
Clinician Resources
Reference materials specified for clinician use include statistical data and guideline recommendations as well as tools that facilitate use of the estimator results in clinical practice. Statistical data is presented in summaries such as “Understanding Cardiovascular Risk” and “Groups that Benefit from Statins.” Guideline recommendations are broken down by lifestyle, blood cholesterol, initiation of statin therapy, and statin safety recommendations, with links to full guidelines and more information that direct away from the app to Web pages in your mobile Internet browser.

Patient Resources
Material made available specifically for patients overlap in content with clinician references but not in presentation. Clinical data, including similar categories as “Understanding My Cardiovascular Risk” and “Groups that Benefit from Statin Therapy” found in clinician resources, present important data without clinical jargon to cloud patient understanding of their health condition. For example, a colorful infographic transforms “Groups that Benefit from Statin Therapy” from the clinical explanations into 5 charted “points to remember” about patient characteristics and how these characteristics shape a statin-benefit analysis.
An alphabetical glossary of common cardiovascular terms is a convenient reference tool for patients to understand the bare minimum of the terminology they may be confronted with at a cardiology appointment, as they read through available resources, and as they begin treatment. At the bottom of the glossary is a Web link to an expanded list at http://www.cardiosmart.org.
FINAL THOUGHTS
Although the resources offered in the app are available online, the app zeroes in on key information specifically necessary for understanding and treating ASCVD. The ACC and AHA sifted through the 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk and the 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults to highlight overview material, linking to information that will further enhance the education of clinicians and patients in the area of ASCVD.
Within the app it is noted that the 10-year risk estimates are based on data from multiple community-based populations and are applicable to African American and non-Hispanic white men and women aged 40 to 79 years. This means that for ethnic groups not listed in the available dropdown menu, users should use the equations for non-Hispanic whites, “though these estimates may underestimate the risk of persons from some race/ethnic groups.” A similar under- or overestimate possibility exists for lifetime risk estimates.
The ASCVD Risk Estimator app is a mobile tool created to determine the 10-year and lifetime risk patients may have for developing atherosclerotic cardiovascular disease (ASCVD). Using the Pooled Cohort Equations and lifetime risk prediction tools, the app focuses on assessment of cardiovascular risk, lifestyle modifications to reduce cardiovascular risk, and management of elevated blood cholesterol and body weight in adults. The app is separated into 4 easy-to-use tabs: the estimator tool, clinician resources, patient resources, and clinical research results surrounding the development of treatment guidelines.
Estimator
The American College of Cardiology (ACC) and the American Heart Association (AHA) collaborated to create a short, 9-step calculator to estimate 10-year and lifetime risk for ASCVD. A patient’s basic health information is entered into the estimator (sex, age, race, total cholesterol, high-density lipoprotein cholesterol, systolic blood pressure, blood pressure lowering medication use, diabetes status, and smoking status) and within seconds, risk rates are output and treatment recommendations are made.
Treatment recommendations include statin and lifestyle guidance. No statins are recommended if the 10-year ASCVD risk is < 5%. Lifestyle guidance is provided regardless of the ASCVD risk rate, which includes eating a heart-healthy diet, getting regular aerobic exercise, maintaining a desirable body weight, and avoiding use of tobacco products.
The ACC and AHA recognize that factors other than the 9 estimator questions may exist for a patient and make it clear that the best way to proceed with the calculated output information is through clinician-patient discussion. They consider that factors such as primary low-density lipoprotein cholesterol of ≥ 160 mg/dL; other evidence of genetic hyperlipidemias; family history of premature ASCVD with onset at age < 55 years in a first-degree male relative or age < 65 years in a first-degree female relative; high-sensitivity C-reactive protein ≥ 2 mg/L; CAC score ≥ 300 Agatston units or ≥ 75 percentile for age, sex, and ethnicity, ankle-brachial index < 0.9; or elevated lifetime risk of ASCVD all need to be discussed and considered between the physician and the patient.
Clinician Resources
Reference materials specified for clinician use include statistical data and guideline recommendations as well as tools that facilitate use of the estimator results in clinical practice. Statistical data is presented in summaries such as “Understanding Cardiovascular Risk” and “Groups that Benefit from Statins.” Guideline recommendations are broken down by lifestyle, blood cholesterol, initiation of statin therapy, and statin safety recommendations, with links to full guidelines and more information that direct away from the app to Web pages in your mobile Internet browser.
Patient Resources
Material made available specifically for patients overlap in content with clinician references but not in presentation. Clinical data, including similar categories as “Understanding My Cardiovascular Risk” and “Groups that Benefit from Statin Therapy” found in clinician resources, present important data without clinical jargon to cloud patient understanding of their health condition. For example, a colorful infographic transforms “Groups that Benefit from Statin Therapy” from the clinical explanations into 5 charted “points to remember” about patient characteristics and how these characteristics shape a statin-benefit analysis.
An alphabetical glossary of common cardiovascular terms is a convenient reference tool for patients to understand the bare minimum of the terminology they may be confronted with at a cardiology appointment, as they read through available resources, and as they begin treatment. At the bottom of the glossary is a Web link to an expanded list at http://www.cardiosmart.org.
FINAL THOUGHTS
Although the resources offered in the app are available online, the app zeroes in on key information specifically necessary for understanding and treating ASCVD. The ACC and AHA sifted through the 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk and the 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults to highlight overview material, linking to information that will further enhance the education of clinicians and patients in the area of ASCVD.
Within the app it is noted that the 10-year risk estimates are based on data from multiple community-based populations and are applicable to African American and non-Hispanic white men and women aged 40 to 79 years. This means that for ethnic groups not listed in the available dropdown menu, users should use the equations for non-Hispanic whites, “though these estimates may underestimate the risk of persons from some race/ethnic groups.” A similar under- or overestimate possibility exists for lifetime risk estimates.
The ASCVD Risk Estimator app is a mobile tool created to determine the 10-year and lifetime risk patients may have for developing atherosclerotic cardiovascular disease (ASCVD). Using the Pooled Cohort Equations and lifetime risk prediction tools, the app focuses on assessment of cardiovascular risk, lifestyle modifications to reduce cardiovascular risk, and management of elevated blood cholesterol and body weight in adults. The app is separated into 4 easy-to-use tabs: the estimator tool, clinician resources, patient resources, and clinical research results surrounding the development of treatment guidelines.
Estimator
The American College of Cardiology (ACC) and the American Heart Association (AHA) collaborated to create a short, 9-step calculator to estimate 10-year and lifetime risk for ASCVD. A patient’s basic health information is entered into the estimator (sex, age, race, total cholesterol, high-density lipoprotein cholesterol, systolic blood pressure, blood pressure lowering medication use, diabetes status, and smoking status) and within seconds, risk rates are output and treatment recommendations are made.
Treatment recommendations include statin and lifestyle guidance. No statins are recommended if the 10-year ASCVD risk is < 5%. Lifestyle guidance is provided regardless of the ASCVD risk rate, which includes eating a heart-healthy diet, getting regular aerobic exercise, maintaining a desirable body weight, and avoiding use of tobacco products.
The ACC and AHA recognize that factors other than the 9 estimator questions may exist for a patient and make it clear that the best way to proceed with the calculated output information is through clinician-patient discussion. They consider that factors such as primary low-density lipoprotein cholesterol of ≥ 160 mg/dL; other evidence of genetic hyperlipidemias; family history of premature ASCVD with onset at age < 55 years in a first-degree male relative or age < 65 years in a first-degree female relative; high-sensitivity C-reactive protein ≥ 2 mg/L; CAC score ≥ 300 Agatston units or ≥ 75 percentile for age, sex, and ethnicity, ankle-brachial index < 0.9; or elevated lifetime risk of ASCVD all need to be discussed and considered between the physician and the patient.
Clinician Resources
Reference materials specified for clinician use include statistical data and guideline recommendations as well as tools that facilitate use of the estimator results in clinical practice. Statistical data is presented in summaries such as “Understanding Cardiovascular Risk” and “Groups that Benefit from Statins.” Guideline recommendations are broken down by lifestyle, blood cholesterol, initiation of statin therapy, and statin safety recommendations, with links to full guidelines and more information that direct away from the app to Web pages in your mobile Internet browser.
Patient Resources
Material made available specifically for patients overlap in content with clinician references but not in presentation. Clinical data, including similar categories as “Understanding My Cardiovascular Risk” and “Groups that Benefit from Statin Therapy” found in clinician resources, present important data without clinical jargon to cloud patient understanding of their health condition. For example, a colorful infographic transforms “Groups that Benefit from Statin Therapy” from the clinical explanations into 5 charted “points to remember” about patient characteristics and how these characteristics shape a statin-benefit analysis.
An alphabetical glossary of common cardiovascular terms is a convenient reference tool for patients to understand the bare minimum of the terminology they may be confronted with at a cardiology appointment, as they read through available resources, and as they begin treatment. At the bottom of the glossary is a Web link to an expanded list at http://www.cardiosmart.org.
FINAL THOUGHTS
Although the resources offered in the app are available online, the app zeroes in on key information specifically necessary for understanding and treating ASCVD. The ACC and AHA sifted through the 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk and the 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults to highlight overview material, linking to information that will further enhance the education of clinicians and patients in the area of ASCVD.
Within the app it is noted that the 10-year risk estimates are based on data from multiple community-based populations and are applicable to African American and non-Hispanic white men and women aged 40 to 79 years. This means that for ethnic groups not listed in the available dropdown menu, users should use the equations for non-Hispanic whites, “though these estimates may underestimate the risk of persons from some race/ethnic groups.” A similar under- or overestimate possibility exists for lifetime risk estimates.