User login
Musculoskeletal pain affects one-quarter of the adult population and is the most common reason for self-medication and for seeking health care.1-3 It is also cited as the most common reason for the use of complementary and alternative medicine (CAM), and the lower back, head, neck, and knee are the most commonly reported areas of pain.4-8 In 2007, the estimated annual cost of managing chronic pain, adjusted for inflation, ranged from $560 to $635 billion; whereas the direct out-of-pocket cost for patients with back pain was $34 billion.9 Chronic pain persists beyond the usual course of disease or healing; generally about 3 months or longer.10-12 The most common forms of pain include those associated with musculoskeletal disorders, such as degenerative arthritis, rheumatoid arthritis, osteoarthritis, myofascial pain, chronic headache, low back pain, and bone pain.11,13-15
A large number of returning Operation Iraqi Freedom (OIF) and Operation Enduring Freedom (OEF) veterans have reported chronic pain symptoms, with back and head being the most common pain locations.7 They experienced pain related to wearing heavy gear every day, being transported in armored vehicles over crater-ridden roads, and enduring less than optimal sleeping conditions.16 Studies have found a significant number of subjects in this population who reported using CAM therapy. The OIF/OEF veterans were likely to have outpatient visits for musculoskeletal system disorders and to use CAM as an additional tool in pain management—not as a reaction to perceived inadequacies of conventional care.17,18
Complementary and alternative medicine is often used to describe various substances, procedures, and approaches outside of mainstream, Western, or conventional medicine for health promotion, treating injuries, symptoms, and illnesses.18,19 Although complementary and alternative are often used interchangeably, the 2 terms refer to different concepts. Complementary refers to the use of a nonmainstream approach with conventional medicine, whereas alternative refers to the use of a nonmainstream approach instead of conventional medicine.19 About 40% of Americans use CAM for various reasons.19
The services and self-care forms of CAM account for a large portion of out-of-pocket costs; patients are willing to pay for it themselves. In 2007, the U.S. spent $33.9 billion on out-of-pocket expenses for CAM classes, products, materials, and visits to CAM providers.20 The costs are comparable with those of conventional health care services and prescription drug use.20 One national study concluded that many patients use CAM in accordance with their beliefs, values, and philosophy concerning health and life.21 Other studies found that many patients use CAM not only because of functional status, pain severity, or self-efficacy, but also because they perceive significant benefits in pain relief.6,17,22-25 Some authors reported that CAM is used to augment and not replace conventional medicine and that it has now become part of the accepted armamentarium for managing chronic musculoskeletal pain.6,17,25
The National Center for Complementary and Alternative Medicine at the National Institutes of Health (NIH) classifies CAM in 2 ways: (1) Mind and body practices, such as acupuncture, massage therapy, meditation, movement therapies, relaxation techniques, spinal manipulation, tai chi and qi gong, yoga, healing touch, and hypnotherapy; and (2) natural products, including probiotics, herbs, and vitamins and minerals usually sold as dietary supplements.19 These products are regulated by the FDA but not as drugs. They have a different set of regulations under the Dietary Supplement Health and Education Act of 1994.26
Mind and body practices or provider-based CAM therapies such as chiropractic care, acupuncture, and massage increased significantly between 2002 and 2007, and many more patients may be willing to try these therapies for chronic low back pain if they do not have to pay out of pocket.27,28 Multiple studies have also found that these treatments in addition to herbal medicine are the most commonly reported CAM treatments used for pain relief in adults.3,17,22,23
Other commonly reported CAM therapies are garlic preparations, exercise, and yoga and meditation.22,23 A large number of veterans have reported previous use or willingness to try chiropractic care, massage therapy, herbal medicines, and acupuncture for chronic noncancer pain.17 In addition to acute care with conventional treatment, the VHA has now expanded services to allow for CAM as available treatment options for chronic musculoskeletal pain.29 The majority of VHA facilities also provide and refer patients to CAM service providers.30
This review article explores the evidence supporting the use of the most commonly reported CAM therapies; specifically acupuncture, massage therapy, and spinal manipulation for musculoskeletal pain relief. Because of the plethora of herbs and dietary supplements in the literature, these were not included in this review, although they are also reported among the most commonly used CAM therapies.1,23,31 The investigators sought to examine the effectiveness of acupuncture, spinal manipulation, or massage compared with no treatment, sham therapy, or current noninvasive first-line treatment for chronic musculoskeletal pain.
Study Selection
To find research addressing this question, the authors searched the PubMed, MEDLINE, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases and the Cochrane Library for all relevant studies published between October 31, 2003, and October 31, 2013. The combined search from all sources for randomized controlled trials (RCTs) resulted in 1,157 studies with acupuncture and chronic pain, 343 studies with spinal manipulation and chronic pain, and 416 studies with massage and chronic pain. Acupuncture and chronic musculoskeletal pain yielded 94 studies, spinal manipulation and chronic musculoskeletal pain yielded 29 studies, and massage and chronic musculoskeletal pain yielded 55 RCTs.
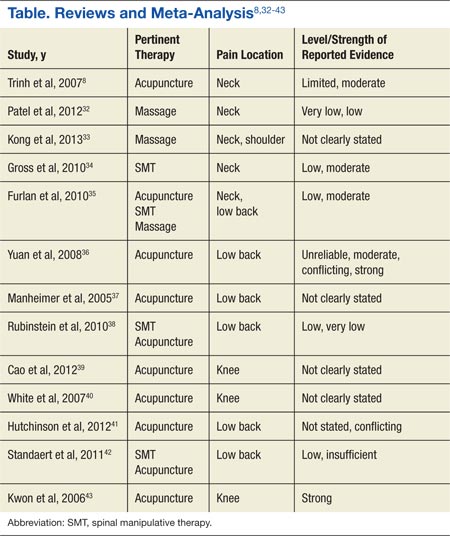
Targeted searches were then conducted within the results for systematic reviews and meta-analysis of relevant studies of RCTs, focus on adults with any type of musculoskeletal pain, written in English, and had pain level or level of pain-related improvement as its primary outcome. The results were assessed for relevance to the review based on the information provided in the title, abstract, and the National Library of Medicine Medical Subject Headings. References of the search results were also searched manually for additional studies relevant to the review. Duplicated studies and those that looked at only acute or cancer pain were excluded. Thirteen systematic reviews and meta-analyses met the inclusion criteria (Table). The investigators reviewed the full reports and agreed to use the data that were abstracted from the studies.
Study Parameters
Four different categories of outcome measuring points for posttreatment follow-up are reported in the CAM studies: immediate, short-term, intermediate, and long-term. There are inconsistencies across studies for the timing of these 4 categories. Immediate posttreatment is defined as up to 1 day.8,32-34 The duration for the short-term follow-up period is defined as between 1 day and 3 months8,32,33; ≤ 3 months35,36; closest to 3 weeks37; closest to 4 weeks34; 1 month38; closest to 8 weeks, but < 3 months after randomization39; or up to 25 weeks, but nearest to 12 weeks.40Intermediate follow-up is between 3 months and 1 year8,33,35; between 3 and 6 months38; ≥ 3 months, but < 1 year36; or closest to 6 months.34Long term is defined as >12 months8,35; closest to 6 months37; 12 months38; 1 year or more36; closest to 6 months, but >3 months after randomization34,39; or between 26 weeks and 56 weeks.40
Pain intensity and pain relief was the treatment efficacy outcome for all the studies. A variety of measuring tools were reported across studies. Eight of the 13 studies reported measurement of pain intensity using the visual analog scale (VAS).8,33,35-37,41-43 In addition to the VAS, 2 studies also used the numerical rating scale (NRS).8,36 One study used the NRS alone.38 Other studies used the McGill Pain Questionnaire35; the SF-36 bodily pain dimension, Von Korff chronic pain grading scale, or low back pain rating scale36; or the Western Ontario and McMaster Universities Osteoarthritis Index subscale for pain.39,40,43
Authors from 8 of the systematic reviews and meta-analysis reported levels of evidence, or GRADE (Grades of Recommendation, Assessment, Development, and Evaluation), used to evaluate the overall quality of the evidence and the strength of the recommendations.8,32,34-36,38,42,43 Levels of evidence were based on RCTs. The various levels were (1) “strong evidence,” consistent findings in multiple high-quality RCTs; (2) “moderate evidence,” consistent findings among multiple high-quality RTCs and/or 1 high-quality RCT; (3) “limited evidence,” low-quality RCT; (4) “conflicting evidence,” inconsistent findings among multiple RCTs; and (5) “no evidence,” no RCTs or no studies.8,36
Most studies expressed the overall strength of the body of literature in 6 different categories: (1) “high quality,” confidence that the evidence reflected the true effect and that further research is very unlikely to change confidence in the effect of size; (2) “moderate quality,” further research is likely to have an impact on confidence in the estimate of effect and may change the estimate; (3) “low quality,” further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change it; (4) “very low quality,” great uncertainty about the estimate; (5) “insufficient evidence,” either the evidence is unavailable or does not allow for a conclusion; and (6)“no evidence,” no evidence from RTCs.32,34,35,38,42,43 Kwon and colleagues reported using a modified jaded score where a total of 5 points was awarded if a study was described as randomized, used an appropriate method, if subjects were blinded to the intervention, if the evaluator was blinded to the intervention, and if there was a description of withdrawals and dropouts.43
Acupuncture
About 3 million American adults receive acupuncture each year.44 The most commonly reported reason for its use is chronic pain.44,45 Trials that examined the characteristics of those seeking and using acupuncture as adjunct to conventional treatment have found that patients who experienced positive outcomes, such as improvement in pain subscale, included females, previous failure of other therapies, and prior positive acupuncture encounters.46
Six of the studies in this review examined the evidence of acupuncture for chronic low back pain.35-38,41,42 Two of those studies found moderate evidence that acupuncture was more effective than no treatment for short-term pain relief.35,36 Manheimer and colleagues found it to be significantly more effective than no additional treatment or sham treatment for short-term pain relief.37 They however, reported a lack of evidence to suggest that it was more effective than were other active therapies.37 Hutchinson and colleagues did not differentiate among data points for intermediate, short-term, or long-term follow-up in their study.41 However, they concluded that there was some evidence to support acupuncture as more effective than no treatment and conflicting evidence of its effectiveness over other treatment modalities. Different levels of evidence were reported for intermediate pain relief with 2 of the other studies. One study found that the evidence was limited.35 The other study reported conflicting evidence that it was more effective than no treatment for immediate pain relief for those with chronic low back pain.36
Rubinstein and colleagues reported low- to very-low-quality evidence that acupuncture provided a short-term clinically relevant effect compared with waiting list control or when it was added to another intervention for chronic low back pain.38 Standaert and colleagues concluded that there was insufficient evidence to determine the relative effectiveness of acupuncture compared with either exercise or spinal manipulative therapy (SMT) in relieving chronic low back pain.42 Yuan and colleagues reported strong evidence that acupuncture combined with conventional therapy was more effective than conventional therapy alone.36
Furlan and colleagues found moderate evidence for significant improvement in pain intensity compared with subjects in physical therapy or usual care groups at short-term or immediate follow-up for chronic back pain.35 Studies that evaluated the efficacy of acupuncture for knee osteoarthritis compared acupuncture with sham acupuncture controls or no additional treatment and found that acupuncture was significantly better at relieving knee pain.39,40,43 Cao and colleagues found it to be effective both in the short term and long term.39 White and colleagues and Kwon and colleagues were unable to draw a conclusion concerning long-term effects due to the data point included in the study or the heterogeneity in the results.40,43
Trinh and colleagues reported moderate evidence that acupuncture is more effective for relief of chronic neck pain compared with inactive, sham treatments at immediate posttreatment.8 They also found moderate evidence that acupuncture was more effective than some other types of sham controls immediately posttreatment and limited evidence that it was more effective than massage at short-term follow-up.8 Furlan and colleagues found trials that applied sham acupuncture tended to produce nonstatistically significant results.35 Their meta-analysis of 2 studies indicated no significant difference between acupuncture and sham acupuncture for immediate posttreatment pain intensity. They also reported inconsistent results for the effects of acupuncture compared with medication or with spinal manipulation for chronic neck pain.35
Massage
Massage promotes health and well-being through the use of mechanical manipulation of body tissues with rhythmic pressure and stroking.47 Treatment techniques include Hoffa massage, friction massage, connective tissue massage, transverse friction massage, and trigger point massage.48 Massage is one of the most popular CAM therapies for neck and back pain.49 In their survey, White and colleagues reported that active-duty military personnel listed massage as the most frequently used CAM therapy in the previous 12 months.18
Patel and colleagues reported that the overall methodology of the trials assessed in their study was either low- or very-low-GRADE level.32 They found very-low to low-quality evidence that there is no difference in effectiveness of 3 approaches of massage therapies (ischemic compression to upper fibre of trapezius trigger point, transverse friction massage to upper fibre of trapezius, and ischemic compression to upper fibre of trapezius) for neck muscle pain. They also reported no difference between conventional Western massage and acupuncture for generalized neck muscle pain at short-term follow-up, and no difference in pain intensity compared with other therapies such as acupuncture, manual therapy, exercise, education, and multimodal interventions. The investigators concluded that the effectiveness of massage therapy for improving neck pain remains unclear, as results could not be combined due to the wide range of techniques and comparative treatments. They were unable to make any firm statement to guide clinical practice.32
Two other studies compared massage to no treatment and found it significantly improved chronic neck pain immediately after the end of treatment.33,35 Kong and colleagues also found similar effects for shoulder pain at immediate and short-term
follow-up but not for neck or shoulder pain when massage was compared with active therapies.33 Furlan and colleagues’ meta-analysis found that massage compared with relaxation or physical therapy was significantly better at reducing chronic nonspecific low back pain immediately after treatment.35
Spinal Manipultaion
Spinal manipulation is high-velocity and low-amplitude localized force directed at specific spinal segments.34 It is performed by using the hands or a device to apply a controlled force to a joint of the spine and is practiced by osteopathic physicians, naturopathic physicians, chiropractors, physical therapists, and some medical doctors.19
In a study to assess its effectiveness, Rubinstein and colleagues found low-quality evidence to very-low-quality evidence to suggest that SMT does not provide a more clinically beneficial effect compared with sham, passive modalities, or other interventions for the relief of chronic low back pain.38 Comparative interventions included usual medical care, physical therapy, exercise, physiotherapy, and multimodal treatments. Standaert and colleagues also found no difference between motor control exercise and SMT in pain relief.42 They concluded that although the evidence is low, there is an indication that structured exercise and SMT seem to offer equivalent benefits in terms of pain for those with chronic lower back pain with clinical benefits evident within 8 weeks of care.42
Gross and colleagues found that when cervical manipulation was compared with control for chronic mechanical neck pain, there was moderate-quality evidence for similar effects at short-term and intermediate follow-up.34 They also reported low-quality evidence in support of thoracic manipulation alone or in combination with electrothermal or individualized physiotherapy and suggested cervical manipulation may provide short-term but not long-term pain relief.34 Furlan and colleagues reported moderate-quality evidence that spinal manipulation provided significantly better posttreatment neck pain relief compared with placebo.35 They also found low evidence that it was significantly better than placebo, acupuncture, and pain medication at immediate follow-up.35
Conclusion
Considerable effort was made to retrieve all studies; however, the authors cannot be certain that the review was exhaustive. They also relied on other analyses of primary studies for the conclusion.
The 3 types of musculoskeletal pain in the review were low back, neck, and knee pain related to osteoarthritis. The authors found that the most common CAM modality studied for chronic musculoskeletal pain was acupuncture. Studies on massage therapy and SMT that were relevant to the review were limited.
Two studies reported strong level of evidence for acupuncture.36,40 One study reported that acupuncture was superior to no treatment or to sham acupuncture for relief of chronic knee pain.40 The other study reported that acupuncture was more effective than conventional therapy alone when it was combined with conventional therapy for chronic low back pain, but there was no difference when compared with sham acupuncture for short-term pain relief.36 The strength of the evidence for acupuncture combined with conventional treatment for low back pain was conflicting. One other review found low evidence for its benefit. Similar to Hopton and MacPherson, this review found that acupuncture treatment seemed to provide effective short-term relief of chronic low back pain.14 Evidence would also seem to support acupuncture for the short-term relief of chronic neck pain and knee pain associated with osteoarthritis.
This review also found immediate and short-term benefits, although mostly with weak evidence, for the use of SMT in the treatment of chronic neck and low back pain. There was conflicting evidence for the support of massage therapy. Furlan and colleagues, however, found that acupuncture, SMT, and massage treatments were significantly more efficacious than no treatment, placebo, physical therapy, or usual care in reducing pain immediately or at short-term after treatment.35 Inconsistencies may be related to the methodologic and clinical diversity of RCTs, which limit the extent of quantitative synthesis and complicates result interpretation.35 Also, better conclusions could be drawn if future studies use head-to-head comparisons of CAM treatments and trials comparing CAM to widely used active treatments that report on all clinically relevant outcomes.35
Although the relationship between conventional treatment and the world of CAM remains equivocal, review of the evidence suggests acupuncture and SMT may be effective treatment for various chronic painful musculoskeletal conditions.35,44,50,51 These CAM modalities are reasonable referral options to supplement conventional therapy for the treatment of chronic musculoskeletal pain when conventional therapy has not yielded satisfactory results.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Callahan LF, Wiley-Exley EK, Mielenz TJ, et al. Use of complementary and alternative medicine among patients with arthritis. Prev Chronic Dis. 2009;6(2):A44.
2. Walsh NE, Brooks P, Hazes JM, et al; Bone and Joint Decade Task Force for Standards of Care for Acute and Chronic Musculoskeletal Pain. Standards of care for acute and chronic musculoskeletal pain: the Bone and Joint Decade (2000-2010). Arch Phys Med Rehabil. 2008;89(9):1830-1845.
3. Williamson AT, Fletcher PC, Dawson KA. Complementary and alternative medicine. Use in an older population. J Gerontol Nurs. 2003;29(5):20-28.
4. Artus M, Croft P, Lewis M. The use of CAM and conventional treatments among primary care consulters with chronic musculoskeletal pain. BMC Fam Pract. 2007;8:26.
5. Cherkin DC, Sherman KJ, Kahn J, et al. A comparison of the effects of 2 types of massage and usual care on chronic low back pain: a randomized controlled trial. Ann Intern Med. 2011;155(1):1-9.
6. Fleming S, Rabago DP, Mundt MP, Fleming MF. CAM therapies among primary care patients using opioid therapy for chronic pain. BMC Complement Altern Med. 2007;7:15.
7. Lew HL, Otis JD, Tun C, Kerns RD, Clark ME, Cifu DX. Prevalence of chronic pain, posttraumatic stress disorder, and persistent post concussive symptoms in OIF/OEF veterans: polytrauma clinical triad. J Rehabil Res Dev. 2009;46(6):697-702.
8. Trinh K, Graham N, Gross A, et al. Acupuncture for neck disorders. Spine (Phila PA 1976). 2007;32(2):236-243.
9. Gaskin DJ, Richard P. Appendix C: The economic costs of pain in the United States. In: Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: National Academies Press; 2011. National Center for Biotechnology Information Website. http://www. ncbi.nlm.nih.gov/books/NBK92521. Accessed July 31, 2015.
10. American Academy of Pain Medicine. AAPM facts and figures on pain. American Academy of Pain Medicine Website. http://www.painmed.org/files/facts-and-figures-on-pain.pdf. Accessed July 31, 2015.
11. Rosenquist RW, Vrooman MD. Chronic pain management. In: Butterworth JF, Mackey DC, Wasnick JD, eds. Morgan & Mikhail’s Clinical Anesthesiology. 5th ed. New York, NY: McGraw-Hill; 2013:chap 47.
12. Rasu RS, Sohraby R, Cunningham L, Knell ME. Assessing chronic pain treatment practices and evaluating adherence to chronic pain clinical guidelines in outpatient practices in the United States. J Pain. 2013;14(6):568-578.
13. Gureje O, Von Korff M, Simon, GE, Grater R. Persistent pain and well-being: a World Health Organization study in primary care. JAMA. 1998;280(2):147-151.
14. Hopton A, MacPherson H. Acupuncture for chronic pain: is acupuncture more than an effective placebo? A systematic review of pooled data from meta-analyses. Pain Pract. 2010;10(2):94-102.
15. Kumar N. WHO Normative guidelines on pain management. World Health Organization Website. http://www.who.int/medicines/areas/quality_safety/delphi_study_pain_guidelines.pdf. Published June 2007. Accessed August 3, 2015.
16. Koffman RL. Downrange acupuncture. Med Acupunct. 2011;23(4):215-218.
17. Denneson LM, Corson K, Dobscha SK. Complementary and alternative medicine use among veterans with chronic noncancer pain. J Rehabil Res Dev. 2011;(48)9:1119-1128.
18. White MR, Jacobson IG, Smith B, et al; Millennium Cohort Study Team. Health care utilization among complementary and alternative medicine users in a large military cohort. BMC Complement Alternat Med. 2011;11:27.
19. U.S. Department of Health and Human Services, National Institutes of Health, National Center for Complementary and Alternative Medicine. Complementary, alternative, or integrative health: What’s in a name? National Center for Complementary and Alternative Medicine Website. http://nccam.nih.gov/health/whatiscam. Updated March 2015. Modified July 8, 2015. Accessed August 4, 2015.
20. Nahin RL, Barnes PM, Stussman BJ, Bloom B. Costs of complementary and alternative medicine (CAM) and frequency of visits to CAM practitioners: United States, 2007. Natl Health Stat Report. 2009;30(18):1-14.
21. Astin JA. Why patients use alternative medicine: results of a national study. JAMA. 1998;279(19):1548-1553.
22. Rosenberg EI, Genao I, Chen I, et al. Complementary and alternative medicine use in primary care patients with chronic pain. Pain Med. 2008;9(8):1065-1072.
23. Alaaeddine N, Okais J, Ballane L, Baddoura RM. Use of complementary and alternative therapy among patients with rheumatoid arthritis and osteoarthritis. J Clin Nurs. 2012;21(21-22):3198-3204.
24. Tan MG, Win MT, Khan SA. The use of complementary and alternative medicine in chronic pain patients in Singapore: a single-centre study. Ann Acad Med Singapore. 2013;42(3):133-137.
25. White P. A background to acupuncture and its use in chronic painful musculoskeletal conditions. J R Soc Promot Health. 2006;126(5):219-227.
26. U.S. Department of Health and Human Services, National Institutes of Health, Office of Dietary Supplements. Dietary Supplement Health and Education Act of 1994. National Institutes of Health Website. http://ods.od.nih.gov/About/DSHEA_Wording.aspx. Published October 25, 1994. Accessed August 4, 2015.
27. Su D, Li L. Trends in the use of complementary and alternative medicine in the United States: 2002-2007. J Health Care Poor Underserved. 2011;22(1):296-310.
28. Sherman KJ, Cherkin DC, Connelly MT, et al. Complementary and alternative medical therapies for chronic low back pain: what treatments are patients willing to try? BMC Complement Alternat Med. 2004;4:9.
29. Smeeding SJ, Bradshaw DH, Kumpfer KL, Trevithick S, Stoddard GJ. Outcome evaluation of the Veterans Affairs Salt Lake City Integrative Health Clinic for Chronic Nonmalignant Pain. Clin J Pain. 2011;27(2):146-155.
30. U.S. Department of Veterans Affairs, Veterans Health Administration, Office of the Assistant Deputy Under Secretary for Health for Policy and Planning. 2011 complementary and alternative medicine. U.S. Department of Veterans Affairs Office of Research and Development Website. http://www.research.va.gov/research_topics/2011cam_finalreport.pdf. Published September 2011. Accessed August 4, 2015.
31. Unsal A, Gözüm S. Use of complementary and alternative medicine by patients with arthritis. J Clin Nurs. 2010;19(7-8):1129-1138.
32. Patel KC, Gross A, Graham N, et al. Massage for mechanical neck disorder. Cochrane Database Syst Rev. 2012;9:CD004871.
33. Kong LJ, Zhan HS, Cheng YW, Yuan WA, Chen B, Fang M. Massage therapy for neck and shoulder pain: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:613279.
34. Gross A, Miller J, D’Sylva J, et al; COG. Manipulation or mobilisation for neck pain: a Cochrane review. Man Ther. 2010;15(4):315-333.
35. Furlan A, Yazdi F, Tsertsvadze A, et al. Complementary and alternative therapies for back Pain II. Evidence report/technology assessment No. 194. (Prepared by the University of Ottawa Evidence-based Practice Center under Contract No. 290-2007-10059-I (EPCIII). AHRQ Publication No. 10(11)E007. Rockville, MD: Agency for Healthcare Research and Quality; 2010.
36. Yuan J, Purepong N, Kerr DP, Park J, Bradbury I, McDonough S. Effectiveness of acupuncture for low back pain. Spine (Phila PA 1976). 2008;33(23):E887-E900.
37. Manheimer E, White A, Berman B, Forys K, Ernst E. Meta-analysis: acupuncture for low back pain. Ann Intern Med. 2005;142(8):651-663.
38. Rubinstein SM, van Middelkoop M, Kuijpers T, et al. A systematic review on the effectiveness of complementary and alternative medicine for chronic non-specific low-back pain. Eur Spine J. 2010;19(8):1213-1228.
39. Cao L, Zhang XL, Gao YS, Jiang Y. Needle acupuncture for osteoarthritis of the knee. A systematic review and updated meta-analysis. Saudi Med J. 2012;33(5):526-532.
40. White A, Foster NE, Cummings M, Barlas P. Acupuncture treatment for chronic knee pain: a systematic review. Rheumatology (Oxford). 2007;46(3):384-390.
41. Hutchinson AJ, Ball S, Andrews JC, Jones GG. The effectiveness of acupuncture in treating chronic non-specific low back pain: a systematic review of the literature. J Orthop Surg Res. 2012;7:36.
42. Standaert, CJ, Friedly J, Erwin MW, et al. Comparative effectiveness of exercise, acupuncture, and spinal manipulation for low back pain. Spine (Phila PA 1976). 2011;36(21 suppl):S120-S130.
43. Kwon YD, Pittler MH, Ernst E. Acupuncture for peripheral joint osteoarthritis: a systematic review and meta-analysis. Rheumatology (Oxford). 2006;45(11):1331-1337.
44. Vickers AJ, Cronin AM, Maschino AC, et al; Acupuncture Trialists’ Collaboration. Individual patient data meta-analysis of acupuncture for chronic pain: protocol of the Acupuncture Trialists’ Collaboration. Trials. 2010;11:90.
45. Kelly RB. Acupuncture for pain. Am Fam Physician. 2009;80(5):481-484.
46. Witt CM, Schützler L, Lüdtke R, Wegscheider K, Willich SN. Patient characteristics and variation in treatment outcomes: which patients benefit most from acupuncture for chronic pain? Clin J Pain. 2011;27(6):550-555.
47. Cafarelli E, Flint F. The role of massage in preparation for and recovery from exercise: an overview. Sports Med. 1992;14(1):1-9.
48. Prentice WE. Therapeutic massage. In: Prentice WE. Therapeutic Modalities in Rehabilitation. 4th ed. New York, NY: McGraw-Hill; 2011:chap 16.
49. Wolsko PM, Eisenberg DM, Davis RB, Kessler R, Phillips RS. Patterns and perceptions of care for treatment of back and neck pain: results of a national survey. Spine (Phila PA 1976). 2003;28(3):292-297.
50. Perlman AI, Sabina A, Williams AL, Njike VY, Katz DL. Massage therapy for osteoarthritis of the knee: a randomized controlled trial. Arch Intern Med. 2006;166(22):2533-2538.
51. Tsao JCI. Effectiveness of massage therapy for chronic, non-malignant pain: a review. Evid Based Complement Alternat Med. 2007;4(2):165-179.
Musculoskeletal pain affects one-quarter of the adult population and is the most common reason for self-medication and for seeking health care.1-3 It is also cited as the most common reason for the use of complementary and alternative medicine (CAM), and the lower back, head, neck, and knee are the most commonly reported areas of pain.4-8 In 2007, the estimated annual cost of managing chronic pain, adjusted for inflation, ranged from $560 to $635 billion; whereas the direct out-of-pocket cost for patients with back pain was $34 billion.9 Chronic pain persists beyond the usual course of disease or healing; generally about 3 months or longer.10-12 The most common forms of pain include those associated with musculoskeletal disorders, such as degenerative arthritis, rheumatoid arthritis, osteoarthritis, myofascial pain, chronic headache, low back pain, and bone pain.11,13-15
A large number of returning Operation Iraqi Freedom (OIF) and Operation Enduring Freedom (OEF) veterans have reported chronic pain symptoms, with back and head being the most common pain locations.7 They experienced pain related to wearing heavy gear every day, being transported in armored vehicles over crater-ridden roads, and enduring less than optimal sleeping conditions.16 Studies have found a significant number of subjects in this population who reported using CAM therapy. The OIF/OEF veterans were likely to have outpatient visits for musculoskeletal system disorders and to use CAM as an additional tool in pain management—not as a reaction to perceived inadequacies of conventional care.17,18
Complementary and alternative medicine is often used to describe various substances, procedures, and approaches outside of mainstream, Western, or conventional medicine for health promotion, treating injuries, symptoms, and illnesses.18,19 Although complementary and alternative are often used interchangeably, the 2 terms refer to different concepts. Complementary refers to the use of a nonmainstream approach with conventional medicine, whereas alternative refers to the use of a nonmainstream approach instead of conventional medicine.19 About 40% of Americans use CAM for various reasons.19
The services and self-care forms of CAM account for a large portion of out-of-pocket costs; patients are willing to pay for it themselves. In 2007, the U.S. spent $33.9 billion on out-of-pocket expenses for CAM classes, products, materials, and visits to CAM providers.20 The costs are comparable with those of conventional health care services and prescription drug use.20 One national study concluded that many patients use CAM in accordance with their beliefs, values, and philosophy concerning health and life.21 Other studies found that many patients use CAM not only because of functional status, pain severity, or self-efficacy, but also because they perceive significant benefits in pain relief.6,17,22-25 Some authors reported that CAM is used to augment and not replace conventional medicine and that it has now become part of the accepted armamentarium for managing chronic musculoskeletal pain.6,17,25
The National Center for Complementary and Alternative Medicine at the National Institutes of Health (NIH) classifies CAM in 2 ways: (1) Mind and body practices, such as acupuncture, massage therapy, meditation, movement therapies, relaxation techniques, spinal manipulation, tai chi and qi gong, yoga, healing touch, and hypnotherapy; and (2) natural products, including probiotics, herbs, and vitamins and minerals usually sold as dietary supplements.19 These products are regulated by the FDA but not as drugs. They have a different set of regulations under the Dietary Supplement Health and Education Act of 1994.26
Mind and body practices or provider-based CAM therapies such as chiropractic care, acupuncture, and massage increased significantly between 2002 and 2007, and many more patients may be willing to try these therapies for chronic low back pain if they do not have to pay out of pocket.27,28 Multiple studies have also found that these treatments in addition to herbal medicine are the most commonly reported CAM treatments used for pain relief in adults.3,17,22,23
Other commonly reported CAM therapies are garlic preparations, exercise, and yoga and meditation.22,23 A large number of veterans have reported previous use or willingness to try chiropractic care, massage therapy, herbal medicines, and acupuncture for chronic noncancer pain.17 In addition to acute care with conventional treatment, the VHA has now expanded services to allow for CAM as available treatment options for chronic musculoskeletal pain.29 The majority of VHA facilities also provide and refer patients to CAM service providers.30
This review article explores the evidence supporting the use of the most commonly reported CAM therapies; specifically acupuncture, massage therapy, and spinal manipulation for musculoskeletal pain relief. Because of the plethora of herbs and dietary supplements in the literature, these were not included in this review, although they are also reported among the most commonly used CAM therapies.1,23,31 The investigators sought to examine the effectiveness of acupuncture, spinal manipulation, or massage compared with no treatment, sham therapy, or current noninvasive first-line treatment for chronic musculoskeletal pain.
Study Selection
To find research addressing this question, the authors searched the PubMed, MEDLINE, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases and the Cochrane Library for all relevant studies published between October 31, 2003, and October 31, 2013. The combined search from all sources for randomized controlled trials (RCTs) resulted in 1,157 studies with acupuncture and chronic pain, 343 studies with spinal manipulation and chronic pain, and 416 studies with massage and chronic pain. Acupuncture and chronic musculoskeletal pain yielded 94 studies, spinal manipulation and chronic musculoskeletal pain yielded 29 studies, and massage and chronic musculoskeletal pain yielded 55 RCTs.
Targeted searches were then conducted within the results for systematic reviews and meta-analysis of relevant studies of RCTs, focus on adults with any type of musculoskeletal pain, written in English, and had pain level or level of pain-related improvement as its primary outcome. The results were assessed for relevance to the review based on the information provided in the title, abstract, and the National Library of Medicine Medical Subject Headings. References of the search results were also searched manually for additional studies relevant to the review. Duplicated studies and those that looked at only acute or cancer pain were excluded. Thirteen systematic reviews and meta-analyses met the inclusion criteria (Table). The investigators reviewed the full reports and agreed to use the data that were abstracted from the studies.
Study Parameters
Four different categories of outcome measuring points for posttreatment follow-up are reported in the CAM studies: immediate, short-term, intermediate, and long-term. There are inconsistencies across studies for the timing of these 4 categories. Immediate posttreatment is defined as up to 1 day.8,32-34 The duration for the short-term follow-up period is defined as between 1 day and 3 months8,32,33; ≤ 3 months35,36; closest to 3 weeks37; closest to 4 weeks34; 1 month38; closest to 8 weeks, but < 3 months after randomization39; or up to 25 weeks, but nearest to 12 weeks.40Intermediate follow-up is between 3 months and 1 year8,33,35; between 3 and 6 months38; ≥ 3 months, but < 1 year36; or closest to 6 months.34Long term is defined as >12 months8,35; closest to 6 months37; 12 months38; 1 year or more36; closest to 6 months, but >3 months after randomization34,39; or between 26 weeks and 56 weeks.40
Pain intensity and pain relief was the treatment efficacy outcome for all the studies. A variety of measuring tools were reported across studies. Eight of the 13 studies reported measurement of pain intensity using the visual analog scale (VAS).8,33,35-37,41-43 In addition to the VAS, 2 studies also used the numerical rating scale (NRS).8,36 One study used the NRS alone.38 Other studies used the McGill Pain Questionnaire35; the SF-36 bodily pain dimension, Von Korff chronic pain grading scale, or low back pain rating scale36; or the Western Ontario and McMaster Universities Osteoarthritis Index subscale for pain.39,40,43
Authors from 8 of the systematic reviews and meta-analysis reported levels of evidence, or GRADE (Grades of Recommendation, Assessment, Development, and Evaluation), used to evaluate the overall quality of the evidence and the strength of the recommendations.8,32,34-36,38,42,43 Levels of evidence were based on RCTs. The various levels were (1) “strong evidence,” consistent findings in multiple high-quality RCTs; (2) “moderate evidence,” consistent findings among multiple high-quality RTCs and/or 1 high-quality RCT; (3) “limited evidence,” low-quality RCT; (4) “conflicting evidence,” inconsistent findings among multiple RCTs; and (5) “no evidence,” no RCTs or no studies.8,36
Most studies expressed the overall strength of the body of literature in 6 different categories: (1) “high quality,” confidence that the evidence reflected the true effect and that further research is very unlikely to change confidence in the effect of size; (2) “moderate quality,” further research is likely to have an impact on confidence in the estimate of effect and may change the estimate; (3) “low quality,” further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change it; (4) “very low quality,” great uncertainty about the estimate; (5) “insufficient evidence,” either the evidence is unavailable or does not allow for a conclusion; and (6)“no evidence,” no evidence from RTCs.32,34,35,38,42,43 Kwon and colleagues reported using a modified jaded score where a total of 5 points was awarded if a study was described as randomized, used an appropriate method, if subjects were blinded to the intervention, if the evaluator was blinded to the intervention, and if there was a description of withdrawals and dropouts.43
Acupuncture
About 3 million American adults receive acupuncture each year.44 The most commonly reported reason for its use is chronic pain.44,45 Trials that examined the characteristics of those seeking and using acupuncture as adjunct to conventional treatment have found that patients who experienced positive outcomes, such as improvement in pain subscale, included females, previous failure of other therapies, and prior positive acupuncture encounters.46
Six of the studies in this review examined the evidence of acupuncture for chronic low back pain.35-38,41,42 Two of those studies found moderate evidence that acupuncture was more effective than no treatment for short-term pain relief.35,36 Manheimer and colleagues found it to be significantly more effective than no additional treatment or sham treatment for short-term pain relief.37 They however, reported a lack of evidence to suggest that it was more effective than were other active therapies.37 Hutchinson and colleagues did not differentiate among data points for intermediate, short-term, or long-term follow-up in their study.41 However, they concluded that there was some evidence to support acupuncture as more effective than no treatment and conflicting evidence of its effectiveness over other treatment modalities. Different levels of evidence were reported for intermediate pain relief with 2 of the other studies. One study found that the evidence was limited.35 The other study reported conflicting evidence that it was more effective than no treatment for immediate pain relief for those with chronic low back pain.36
Rubinstein and colleagues reported low- to very-low-quality evidence that acupuncture provided a short-term clinically relevant effect compared with waiting list control or when it was added to another intervention for chronic low back pain.38 Standaert and colleagues concluded that there was insufficient evidence to determine the relative effectiveness of acupuncture compared with either exercise or spinal manipulative therapy (SMT) in relieving chronic low back pain.42 Yuan and colleagues reported strong evidence that acupuncture combined with conventional therapy was more effective than conventional therapy alone.36
Furlan and colleagues found moderate evidence for significant improvement in pain intensity compared with subjects in physical therapy or usual care groups at short-term or immediate follow-up for chronic back pain.35 Studies that evaluated the efficacy of acupuncture for knee osteoarthritis compared acupuncture with sham acupuncture controls or no additional treatment and found that acupuncture was significantly better at relieving knee pain.39,40,43 Cao and colleagues found it to be effective both in the short term and long term.39 White and colleagues and Kwon and colleagues were unable to draw a conclusion concerning long-term effects due to the data point included in the study or the heterogeneity in the results.40,43
Trinh and colleagues reported moderate evidence that acupuncture is more effective for relief of chronic neck pain compared with inactive, sham treatments at immediate posttreatment.8 They also found moderate evidence that acupuncture was more effective than some other types of sham controls immediately posttreatment and limited evidence that it was more effective than massage at short-term follow-up.8 Furlan and colleagues found trials that applied sham acupuncture tended to produce nonstatistically significant results.35 Their meta-analysis of 2 studies indicated no significant difference between acupuncture and sham acupuncture for immediate posttreatment pain intensity. They also reported inconsistent results for the effects of acupuncture compared with medication or with spinal manipulation for chronic neck pain.35
Massage
Massage promotes health and well-being through the use of mechanical manipulation of body tissues with rhythmic pressure and stroking.47 Treatment techniques include Hoffa massage, friction massage, connective tissue massage, transverse friction massage, and trigger point massage.48 Massage is one of the most popular CAM therapies for neck and back pain.49 In their survey, White and colleagues reported that active-duty military personnel listed massage as the most frequently used CAM therapy in the previous 12 months.18
Patel and colleagues reported that the overall methodology of the trials assessed in their study was either low- or very-low-GRADE level.32 They found very-low to low-quality evidence that there is no difference in effectiveness of 3 approaches of massage therapies (ischemic compression to upper fibre of trapezius trigger point, transverse friction massage to upper fibre of trapezius, and ischemic compression to upper fibre of trapezius) for neck muscle pain. They also reported no difference between conventional Western massage and acupuncture for generalized neck muscle pain at short-term follow-up, and no difference in pain intensity compared with other therapies such as acupuncture, manual therapy, exercise, education, and multimodal interventions. The investigators concluded that the effectiveness of massage therapy for improving neck pain remains unclear, as results could not be combined due to the wide range of techniques and comparative treatments. They were unable to make any firm statement to guide clinical practice.32
Two other studies compared massage to no treatment and found it significantly improved chronic neck pain immediately after the end of treatment.33,35 Kong and colleagues also found similar effects for shoulder pain at immediate and short-term
follow-up but not for neck or shoulder pain when massage was compared with active therapies.33 Furlan and colleagues’ meta-analysis found that massage compared with relaxation or physical therapy was significantly better at reducing chronic nonspecific low back pain immediately after treatment.35
Spinal Manipultaion
Spinal manipulation is high-velocity and low-amplitude localized force directed at specific spinal segments.34 It is performed by using the hands or a device to apply a controlled force to a joint of the spine and is practiced by osteopathic physicians, naturopathic physicians, chiropractors, physical therapists, and some medical doctors.19
In a study to assess its effectiveness, Rubinstein and colleagues found low-quality evidence to very-low-quality evidence to suggest that SMT does not provide a more clinically beneficial effect compared with sham, passive modalities, or other interventions for the relief of chronic low back pain.38 Comparative interventions included usual medical care, physical therapy, exercise, physiotherapy, and multimodal treatments. Standaert and colleagues also found no difference between motor control exercise and SMT in pain relief.42 They concluded that although the evidence is low, there is an indication that structured exercise and SMT seem to offer equivalent benefits in terms of pain for those with chronic lower back pain with clinical benefits evident within 8 weeks of care.42
Gross and colleagues found that when cervical manipulation was compared with control for chronic mechanical neck pain, there was moderate-quality evidence for similar effects at short-term and intermediate follow-up.34 They also reported low-quality evidence in support of thoracic manipulation alone or in combination with electrothermal or individualized physiotherapy and suggested cervical manipulation may provide short-term but not long-term pain relief.34 Furlan and colleagues reported moderate-quality evidence that spinal manipulation provided significantly better posttreatment neck pain relief compared with placebo.35 They also found low evidence that it was significantly better than placebo, acupuncture, and pain medication at immediate follow-up.35
Conclusion
Considerable effort was made to retrieve all studies; however, the authors cannot be certain that the review was exhaustive. They also relied on other analyses of primary studies for the conclusion.
The 3 types of musculoskeletal pain in the review were low back, neck, and knee pain related to osteoarthritis. The authors found that the most common CAM modality studied for chronic musculoskeletal pain was acupuncture. Studies on massage therapy and SMT that were relevant to the review were limited.
Two studies reported strong level of evidence for acupuncture.36,40 One study reported that acupuncture was superior to no treatment or to sham acupuncture for relief of chronic knee pain.40 The other study reported that acupuncture was more effective than conventional therapy alone when it was combined with conventional therapy for chronic low back pain, but there was no difference when compared with sham acupuncture for short-term pain relief.36 The strength of the evidence for acupuncture combined with conventional treatment for low back pain was conflicting. One other review found low evidence for its benefit. Similar to Hopton and MacPherson, this review found that acupuncture treatment seemed to provide effective short-term relief of chronic low back pain.14 Evidence would also seem to support acupuncture for the short-term relief of chronic neck pain and knee pain associated with osteoarthritis.
This review also found immediate and short-term benefits, although mostly with weak evidence, for the use of SMT in the treatment of chronic neck and low back pain. There was conflicting evidence for the support of massage therapy. Furlan and colleagues, however, found that acupuncture, SMT, and massage treatments were significantly more efficacious than no treatment, placebo, physical therapy, or usual care in reducing pain immediately or at short-term after treatment.35 Inconsistencies may be related to the methodologic and clinical diversity of RCTs, which limit the extent of quantitative synthesis and complicates result interpretation.35 Also, better conclusions could be drawn if future studies use head-to-head comparisons of CAM treatments and trials comparing CAM to widely used active treatments that report on all clinically relevant outcomes.35
Although the relationship between conventional treatment and the world of CAM remains equivocal, review of the evidence suggests acupuncture and SMT may be effective treatment for various chronic painful musculoskeletal conditions.35,44,50,51 These CAM modalities are reasonable referral options to supplement conventional therapy for the treatment of chronic musculoskeletal pain when conventional therapy has not yielded satisfactory results.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Musculoskeletal pain affects one-quarter of the adult population and is the most common reason for self-medication and for seeking health care.1-3 It is also cited as the most common reason for the use of complementary and alternative medicine (CAM), and the lower back, head, neck, and knee are the most commonly reported areas of pain.4-8 In 2007, the estimated annual cost of managing chronic pain, adjusted for inflation, ranged from $560 to $635 billion; whereas the direct out-of-pocket cost for patients with back pain was $34 billion.9 Chronic pain persists beyond the usual course of disease or healing; generally about 3 months or longer.10-12 The most common forms of pain include those associated with musculoskeletal disorders, such as degenerative arthritis, rheumatoid arthritis, osteoarthritis, myofascial pain, chronic headache, low back pain, and bone pain.11,13-15
A large number of returning Operation Iraqi Freedom (OIF) and Operation Enduring Freedom (OEF) veterans have reported chronic pain symptoms, with back and head being the most common pain locations.7 They experienced pain related to wearing heavy gear every day, being transported in armored vehicles over crater-ridden roads, and enduring less than optimal sleeping conditions.16 Studies have found a significant number of subjects in this population who reported using CAM therapy. The OIF/OEF veterans were likely to have outpatient visits for musculoskeletal system disorders and to use CAM as an additional tool in pain management—not as a reaction to perceived inadequacies of conventional care.17,18
Complementary and alternative medicine is often used to describe various substances, procedures, and approaches outside of mainstream, Western, or conventional medicine for health promotion, treating injuries, symptoms, and illnesses.18,19 Although complementary and alternative are often used interchangeably, the 2 terms refer to different concepts. Complementary refers to the use of a nonmainstream approach with conventional medicine, whereas alternative refers to the use of a nonmainstream approach instead of conventional medicine.19 About 40% of Americans use CAM for various reasons.19
The services and self-care forms of CAM account for a large portion of out-of-pocket costs; patients are willing to pay for it themselves. In 2007, the U.S. spent $33.9 billion on out-of-pocket expenses for CAM classes, products, materials, and visits to CAM providers.20 The costs are comparable with those of conventional health care services and prescription drug use.20 One national study concluded that many patients use CAM in accordance with their beliefs, values, and philosophy concerning health and life.21 Other studies found that many patients use CAM not only because of functional status, pain severity, or self-efficacy, but also because they perceive significant benefits in pain relief.6,17,22-25 Some authors reported that CAM is used to augment and not replace conventional medicine and that it has now become part of the accepted armamentarium for managing chronic musculoskeletal pain.6,17,25
The National Center for Complementary and Alternative Medicine at the National Institutes of Health (NIH) classifies CAM in 2 ways: (1) Mind and body practices, such as acupuncture, massage therapy, meditation, movement therapies, relaxation techniques, spinal manipulation, tai chi and qi gong, yoga, healing touch, and hypnotherapy; and (2) natural products, including probiotics, herbs, and vitamins and minerals usually sold as dietary supplements.19 These products are regulated by the FDA but not as drugs. They have a different set of regulations under the Dietary Supplement Health and Education Act of 1994.26
Mind and body practices or provider-based CAM therapies such as chiropractic care, acupuncture, and massage increased significantly between 2002 and 2007, and many more patients may be willing to try these therapies for chronic low back pain if they do not have to pay out of pocket.27,28 Multiple studies have also found that these treatments in addition to herbal medicine are the most commonly reported CAM treatments used for pain relief in adults.3,17,22,23
Other commonly reported CAM therapies are garlic preparations, exercise, and yoga and meditation.22,23 A large number of veterans have reported previous use or willingness to try chiropractic care, massage therapy, herbal medicines, and acupuncture for chronic noncancer pain.17 In addition to acute care with conventional treatment, the VHA has now expanded services to allow for CAM as available treatment options for chronic musculoskeletal pain.29 The majority of VHA facilities also provide and refer patients to CAM service providers.30
This review article explores the evidence supporting the use of the most commonly reported CAM therapies; specifically acupuncture, massage therapy, and spinal manipulation for musculoskeletal pain relief. Because of the plethora of herbs and dietary supplements in the literature, these were not included in this review, although they are also reported among the most commonly used CAM therapies.1,23,31 The investigators sought to examine the effectiveness of acupuncture, spinal manipulation, or massage compared with no treatment, sham therapy, or current noninvasive first-line treatment for chronic musculoskeletal pain.
Study Selection
To find research addressing this question, the authors searched the PubMed, MEDLINE, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases and the Cochrane Library for all relevant studies published between October 31, 2003, and October 31, 2013. The combined search from all sources for randomized controlled trials (RCTs) resulted in 1,157 studies with acupuncture and chronic pain, 343 studies with spinal manipulation and chronic pain, and 416 studies with massage and chronic pain. Acupuncture and chronic musculoskeletal pain yielded 94 studies, spinal manipulation and chronic musculoskeletal pain yielded 29 studies, and massage and chronic musculoskeletal pain yielded 55 RCTs.
Targeted searches were then conducted within the results for systematic reviews and meta-analysis of relevant studies of RCTs, focus on adults with any type of musculoskeletal pain, written in English, and had pain level or level of pain-related improvement as its primary outcome. The results were assessed for relevance to the review based on the information provided in the title, abstract, and the National Library of Medicine Medical Subject Headings. References of the search results were also searched manually for additional studies relevant to the review. Duplicated studies and those that looked at only acute or cancer pain were excluded. Thirteen systematic reviews and meta-analyses met the inclusion criteria (Table). The investigators reviewed the full reports and agreed to use the data that were abstracted from the studies.
Study Parameters
Four different categories of outcome measuring points for posttreatment follow-up are reported in the CAM studies: immediate, short-term, intermediate, and long-term. There are inconsistencies across studies for the timing of these 4 categories. Immediate posttreatment is defined as up to 1 day.8,32-34 The duration for the short-term follow-up period is defined as between 1 day and 3 months8,32,33; ≤ 3 months35,36; closest to 3 weeks37; closest to 4 weeks34; 1 month38; closest to 8 weeks, but < 3 months after randomization39; or up to 25 weeks, but nearest to 12 weeks.40Intermediate follow-up is between 3 months and 1 year8,33,35; between 3 and 6 months38; ≥ 3 months, but < 1 year36; or closest to 6 months.34Long term is defined as >12 months8,35; closest to 6 months37; 12 months38; 1 year or more36; closest to 6 months, but >3 months after randomization34,39; or between 26 weeks and 56 weeks.40
Pain intensity and pain relief was the treatment efficacy outcome for all the studies. A variety of measuring tools were reported across studies. Eight of the 13 studies reported measurement of pain intensity using the visual analog scale (VAS).8,33,35-37,41-43 In addition to the VAS, 2 studies also used the numerical rating scale (NRS).8,36 One study used the NRS alone.38 Other studies used the McGill Pain Questionnaire35; the SF-36 bodily pain dimension, Von Korff chronic pain grading scale, or low back pain rating scale36; or the Western Ontario and McMaster Universities Osteoarthritis Index subscale for pain.39,40,43
Authors from 8 of the systematic reviews and meta-analysis reported levels of evidence, or GRADE (Grades of Recommendation, Assessment, Development, and Evaluation), used to evaluate the overall quality of the evidence and the strength of the recommendations.8,32,34-36,38,42,43 Levels of evidence were based on RCTs. The various levels were (1) “strong evidence,” consistent findings in multiple high-quality RCTs; (2) “moderate evidence,” consistent findings among multiple high-quality RTCs and/or 1 high-quality RCT; (3) “limited evidence,” low-quality RCT; (4) “conflicting evidence,” inconsistent findings among multiple RCTs; and (5) “no evidence,” no RCTs or no studies.8,36
Most studies expressed the overall strength of the body of literature in 6 different categories: (1) “high quality,” confidence that the evidence reflected the true effect and that further research is very unlikely to change confidence in the effect of size; (2) “moderate quality,” further research is likely to have an impact on confidence in the estimate of effect and may change the estimate; (3) “low quality,” further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change it; (4) “very low quality,” great uncertainty about the estimate; (5) “insufficient evidence,” either the evidence is unavailable or does not allow for a conclusion; and (6)“no evidence,” no evidence from RTCs.32,34,35,38,42,43 Kwon and colleagues reported using a modified jaded score where a total of 5 points was awarded if a study was described as randomized, used an appropriate method, if subjects were blinded to the intervention, if the evaluator was blinded to the intervention, and if there was a description of withdrawals and dropouts.43
Acupuncture
About 3 million American adults receive acupuncture each year.44 The most commonly reported reason for its use is chronic pain.44,45 Trials that examined the characteristics of those seeking and using acupuncture as adjunct to conventional treatment have found that patients who experienced positive outcomes, such as improvement in pain subscale, included females, previous failure of other therapies, and prior positive acupuncture encounters.46
Six of the studies in this review examined the evidence of acupuncture for chronic low back pain.35-38,41,42 Two of those studies found moderate evidence that acupuncture was more effective than no treatment for short-term pain relief.35,36 Manheimer and colleagues found it to be significantly more effective than no additional treatment or sham treatment for short-term pain relief.37 They however, reported a lack of evidence to suggest that it was more effective than were other active therapies.37 Hutchinson and colleagues did not differentiate among data points for intermediate, short-term, or long-term follow-up in their study.41 However, they concluded that there was some evidence to support acupuncture as more effective than no treatment and conflicting evidence of its effectiveness over other treatment modalities. Different levels of evidence were reported for intermediate pain relief with 2 of the other studies. One study found that the evidence was limited.35 The other study reported conflicting evidence that it was more effective than no treatment for immediate pain relief for those with chronic low back pain.36
Rubinstein and colleagues reported low- to very-low-quality evidence that acupuncture provided a short-term clinically relevant effect compared with waiting list control or when it was added to another intervention for chronic low back pain.38 Standaert and colleagues concluded that there was insufficient evidence to determine the relative effectiveness of acupuncture compared with either exercise or spinal manipulative therapy (SMT) in relieving chronic low back pain.42 Yuan and colleagues reported strong evidence that acupuncture combined with conventional therapy was more effective than conventional therapy alone.36
Furlan and colleagues found moderate evidence for significant improvement in pain intensity compared with subjects in physical therapy or usual care groups at short-term or immediate follow-up for chronic back pain.35 Studies that evaluated the efficacy of acupuncture for knee osteoarthritis compared acupuncture with sham acupuncture controls or no additional treatment and found that acupuncture was significantly better at relieving knee pain.39,40,43 Cao and colleagues found it to be effective both in the short term and long term.39 White and colleagues and Kwon and colleagues were unable to draw a conclusion concerning long-term effects due to the data point included in the study or the heterogeneity in the results.40,43
Trinh and colleagues reported moderate evidence that acupuncture is more effective for relief of chronic neck pain compared with inactive, sham treatments at immediate posttreatment.8 They also found moderate evidence that acupuncture was more effective than some other types of sham controls immediately posttreatment and limited evidence that it was more effective than massage at short-term follow-up.8 Furlan and colleagues found trials that applied sham acupuncture tended to produce nonstatistically significant results.35 Their meta-analysis of 2 studies indicated no significant difference between acupuncture and sham acupuncture for immediate posttreatment pain intensity. They also reported inconsistent results for the effects of acupuncture compared with medication or with spinal manipulation for chronic neck pain.35
Massage
Massage promotes health and well-being through the use of mechanical manipulation of body tissues with rhythmic pressure and stroking.47 Treatment techniques include Hoffa massage, friction massage, connective tissue massage, transverse friction massage, and trigger point massage.48 Massage is one of the most popular CAM therapies for neck and back pain.49 In their survey, White and colleagues reported that active-duty military personnel listed massage as the most frequently used CAM therapy in the previous 12 months.18
Patel and colleagues reported that the overall methodology of the trials assessed in their study was either low- or very-low-GRADE level.32 They found very-low to low-quality evidence that there is no difference in effectiveness of 3 approaches of massage therapies (ischemic compression to upper fibre of trapezius trigger point, transverse friction massage to upper fibre of trapezius, and ischemic compression to upper fibre of trapezius) for neck muscle pain. They also reported no difference between conventional Western massage and acupuncture for generalized neck muscle pain at short-term follow-up, and no difference in pain intensity compared with other therapies such as acupuncture, manual therapy, exercise, education, and multimodal interventions. The investigators concluded that the effectiveness of massage therapy for improving neck pain remains unclear, as results could not be combined due to the wide range of techniques and comparative treatments. They were unable to make any firm statement to guide clinical practice.32
Two other studies compared massage to no treatment and found it significantly improved chronic neck pain immediately after the end of treatment.33,35 Kong and colleagues also found similar effects for shoulder pain at immediate and short-term
follow-up but not for neck or shoulder pain when massage was compared with active therapies.33 Furlan and colleagues’ meta-analysis found that massage compared with relaxation or physical therapy was significantly better at reducing chronic nonspecific low back pain immediately after treatment.35
Spinal Manipultaion
Spinal manipulation is high-velocity and low-amplitude localized force directed at specific spinal segments.34 It is performed by using the hands or a device to apply a controlled force to a joint of the spine and is practiced by osteopathic physicians, naturopathic physicians, chiropractors, physical therapists, and some medical doctors.19
In a study to assess its effectiveness, Rubinstein and colleagues found low-quality evidence to very-low-quality evidence to suggest that SMT does not provide a more clinically beneficial effect compared with sham, passive modalities, or other interventions for the relief of chronic low back pain.38 Comparative interventions included usual medical care, physical therapy, exercise, physiotherapy, and multimodal treatments. Standaert and colleagues also found no difference between motor control exercise and SMT in pain relief.42 They concluded that although the evidence is low, there is an indication that structured exercise and SMT seem to offer equivalent benefits in terms of pain for those with chronic lower back pain with clinical benefits evident within 8 weeks of care.42
Gross and colleagues found that when cervical manipulation was compared with control for chronic mechanical neck pain, there was moderate-quality evidence for similar effects at short-term and intermediate follow-up.34 They also reported low-quality evidence in support of thoracic manipulation alone or in combination with electrothermal or individualized physiotherapy and suggested cervical manipulation may provide short-term but not long-term pain relief.34 Furlan and colleagues reported moderate-quality evidence that spinal manipulation provided significantly better posttreatment neck pain relief compared with placebo.35 They also found low evidence that it was significantly better than placebo, acupuncture, and pain medication at immediate follow-up.35
Conclusion
Considerable effort was made to retrieve all studies; however, the authors cannot be certain that the review was exhaustive. They also relied on other analyses of primary studies for the conclusion.
The 3 types of musculoskeletal pain in the review were low back, neck, and knee pain related to osteoarthritis. The authors found that the most common CAM modality studied for chronic musculoskeletal pain was acupuncture. Studies on massage therapy and SMT that were relevant to the review were limited.
Two studies reported strong level of evidence for acupuncture.36,40 One study reported that acupuncture was superior to no treatment or to sham acupuncture for relief of chronic knee pain.40 The other study reported that acupuncture was more effective than conventional therapy alone when it was combined with conventional therapy for chronic low back pain, but there was no difference when compared with sham acupuncture for short-term pain relief.36 The strength of the evidence for acupuncture combined with conventional treatment for low back pain was conflicting. One other review found low evidence for its benefit. Similar to Hopton and MacPherson, this review found that acupuncture treatment seemed to provide effective short-term relief of chronic low back pain.14 Evidence would also seem to support acupuncture for the short-term relief of chronic neck pain and knee pain associated with osteoarthritis.
This review also found immediate and short-term benefits, although mostly with weak evidence, for the use of SMT in the treatment of chronic neck and low back pain. There was conflicting evidence for the support of massage therapy. Furlan and colleagues, however, found that acupuncture, SMT, and massage treatments were significantly more efficacious than no treatment, placebo, physical therapy, or usual care in reducing pain immediately or at short-term after treatment.35 Inconsistencies may be related to the methodologic and clinical diversity of RCTs, which limit the extent of quantitative synthesis and complicates result interpretation.35 Also, better conclusions could be drawn if future studies use head-to-head comparisons of CAM treatments and trials comparing CAM to widely used active treatments that report on all clinically relevant outcomes.35
Although the relationship between conventional treatment and the world of CAM remains equivocal, review of the evidence suggests acupuncture and SMT may be effective treatment for various chronic painful musculoskeletal conditions.35,44,50,51 These CAM modalities are reasonable referral options to supplement conventional therapy for the treatment of chronic musculoskeletal pain when conventional therapy has not yielded satisfactory results.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Callahan LF, Wiley-Exley EK, Mielenz TJ, et al. Use of complementary and alternative medicine among patients with arthritis. Prev Chronic Dis. 2009;6(2):A44.
2. Walsh NE, Brooks P, Hazes JM, et al; Bone and Joint Decade Task Force for Standards of Care for Acute and Chronic Musculoskeletal Pain. Standards of care for acute and chronic musculoskeletal pain: the Bone and Joint Decade (2000-2010). Arch Phys Med Rehabil. 2008;89(9):1830-1845.
3. Williamson AT, Fletcher PC, Dawson KA. Complementary and alternative medicine. Use in an older population. J Gerontol Nurs. 2003;29(5):20-28.
4. Artus M, Croft P, Lewis M. The use of CAM and conventional treatments among primary care consulters with chronic musculoskeletal pain. BMC Fam Pract. 2007;8:26.
5. Cherkin DC, Sherman KJ, Kahn J, et al. A comparison of the effects of 2 types of massage and usual care on chronic low back pain: a randomized controlled trial. Ann Intern Med. 2011;155(1):1-9.
6. Fleming S, Rabago DP, Mundt MP, Fleming MF. CAM therapies among primary care patients using opioid therapy for chronic pain. BMC Complement Altern Med. 2007;7:15.
7. Lew HL, Otis JD, Tun C, Kerns RD, Clark ME, Cifu DX. Prevalence of chronic pain, posttraumatic stress disorder, and persistent post concussive symptoms in OIF/OEF veterans: polytrauma clinical triad. J Rehabil Res Dev. 2009;46(6):697-702.
8. Trinh K, Graham N, Gross A, et al. Acupuncture for neck disorders. Spine (Phila PA 1976). 2007;32(2):236-243.
9. Gaskin DJ, Richard P. Appendix C: The economic costs of pain in the United States. In: Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: National Academies Press; 2011. National Center for Biotechnology Information Website. http://www. ncbi.nlm.nih.gov/books/NBK92521. Accessed July 31, 2015.
10. American Academy of Pain Medicine. AAPM facts and figures on pain. American Academy of Pain Medicine Website. http://www.painmed.org/files/facts-and-figures-on-pain.pdf. Accessed July 31, 2015.
11. Rosenquist RW, Vrooman MD. Chronic pain management. In: Butterworth JF, Mackey DC, Wasnick JD, eds. Morgan & Mikhail’s Clinical Anesthesiology. 5th ed. New York, NY: McGraw-Hill; 2013:chap 47.
12. Rasu RS, Sohraby R, Cunningham L, Knell ME. Assessing chronic pain treatment practices and evaluating adherence to chronic pain clinical guidelines in outpatient practices in the United States. J Pain. 2013;14(6):568-578.
13. Gureje O, Von Korff M, Simon, GE, Grater R. Persistent pain and well-being: a World Health Organization study in primary care. JAMA. 1998;280(2):147-151.
14. Hopton A, MacPherson H. Acupuncture for chronic pain: is acupuncture more than an effective placebo? A systematic review of pooled data from meta-analyses. Pain Pract. 2010;10(2):94-102.
15. Kumar N. WHO Normative guidelines on pain management. World Health Organization Website. http://www.who.int/medicines/areas/quality_safety/delphi_study_pain_guidelines.pdf. Published June 2007. Accessed August 3, 2015.
16. Koffman RL. Downrange acupuncture. Med Acupunct. 2011;23(4):215-218.
17. Denneson LM, Corson K, Dobscha SK. Complementary and alternative medicine use among veterans with chronic noncancer pain. J Rehabil Res Dev. 2011;(48)9:1119-1128.
18. White MR, Jacobson IG, Smith B, et al; Millennium Cohort Study Team. Health care utilization among complementary and alternative medicine users in a large military cohort. BMC Complement Alternat Med. 2011;11:27.
19. U.S. Department of Health and Human Services, National Institutes of Health, National Center for Complementary and Alternative Medicine. Complementary, alternative, or integrative health: What’s in a name? National Center for Complementary and Alternative Medicine Website. http://nccam.nih.gov/health/whatiscam. Updated March 2015. Modified July 8, 2015. Accessed August 4, 2015.
20. Nahin RL, Barnes PM, Stussman BJ, Bloom B. Costs of complementary and alternative medicine (CAM) and frequency of visits to CAM practitioners: United States, 2007. Natl Health Stat Report. 2009;30(18):1-14.
21. Astin JA. Why patients use alternative medicine: results of a national study. JAMA. 1998;279(19):1548-1553.
22. Rosenberg EI, Genao I, Chen I, et al. Complementary and alternative medicine use in primary care patients with chronic pain. Pain Med. 2008;9(8):1065-1072.
23. Alaaeddine N, Okais J, Ballane L, Baddoura RM. Use of complementary and alternative therapy among patients with rheumatoid arthritis and osteoarthritis. J Clin Nurs. 2012;21(21-22):3198-3204.
24. Tan MG, Win MT, Khan SA. The use of complementary and alternative medicine in chronic pain patients in Singapore: a single-centre study. Ann Acad Med Singapore. 2013;42(3):133-137.
25. White P. A background to acupuncture and its use in chronic painful musculoskeletal conditions. J R Soc Promot Health. 2006;126(5):219-227.
26. U.S. Department of Health and Human Services, National Institutes of Health, Office of Dietary Supplements. Dietary Supplement Health and Education Act of 1994. National Institutes of Health Website. http://ods.od.nih.gov/About/DSHEA_Wording.aspx. Published October 25, 1994. Accessed August 4, 2015.
27. Su D, Li L. Trends in the use of complementary and alternative medicine in the United States: 2002-2007. J Health Care Poor Underserved. 2011;22(1):296-310.
28. Sherman KJ, Cherkin DC, Connelly MT, et al. Complementary and alternative medical therapies for chronic low back pain: what treatments are patients willing to try? BMC Complement Alternat Med. 2004;4:9.
29. Smeeding SJ, Bradshaw DH, Kumpfer KL, Trevithick S, Stoddard GJ. Outcome evaluation of the Veterans Affairs Salt Lake City Integrative Health Clinic for Chronic Nonmalignant Pain. Clin J Pain. 2011;27(2):146-155.
30. U.S. Department of Veterans Affairs, Veterans Health Administration, Office of the Assistant Deputy Under Secretary for Health for Policy and Planning. 2011 complementary and alternative medicine. U.S. Department of Veterans Affairs Office of Research and Development Website. http://www.research.va.gov/research_topics/2011cam_finalreport.pdf. Published September 2011. Accessed August 4, 2015.
31. Unsal A, Gözüm S. Use of complementary and alternative medicine by patients with arthritis. J Clin Nurs. 2010;19(7-8):1129-1138.
32. Patel KC, Gross A, Graham N, et al. Massage for mechanical neck disorder. Cochrane Database Syst Rev. 2012;9:CD004871.
33. Kong LJ, Zhan HS, Cheng YW, Yuan WA, Chen B, Fang M. Massage therapy for neck and shoulder pain: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:613279.
34. Gross A, Miller J, D’Sylva J, et al; COG. Manipulation or mobilisation for neck pain: a Cochrane review. Man Ther. 2010;15(4):315-333.
35. Furlan A, Yazdi F, Tsertsvadze A, et al. Complementary and alternative therapies for back Pain II. Evidence report/technology assessment No. 194. (Prepared by the University of Ottawa Evidence-based Practice Center under Contract No. 290-2007-10059-I (EPCIII). AHRQ Publication No. 10(11)E007. Rockville, MD: Agency for Healthcare Research and Quality; 2010.
36. Yuan J, Purepong N, Kerr DP, Park J, Bradbury I, McDonough S. Effectiveness of acupuncture for low back pain. Spine (Phila PA 1976). 2008;33(23):E887-E900.
37. Manheimer E, White A, Berman B, Forys K, Ernst E. Meta-analysis: acupuncture for low back pain. Ann Intern Med. 2005;142(8):651-663.
38. Rubinstein SM, van Middelkoop M, Kuijpers T, et al. A systematic review on the effectiveness of complementary and alternative medicine for chronic non-specific low-back pain. Eur Spine J. 2010;19(8):1213-1228.
39. Cao L, Zhang XL, Gao YS, Jiang Y. Needle acupuncture for osteoarthritis of the knee. A systematic review and updated meta-analysis. Saudi Med J. 2012;33(5):526-532.
40. White A, Foster NE, Cummings M, Barlas P. Acupuncture treatment for chronic knee pain: a systematic review. Rheumatology (Oxford). 2007;46(3):384-390.
41. Hutchinson AJ, Ball S, Andrews JC, Jones GG. The effectiveness of acupuncture in treating chronic non-specific low back pain: a systematic review of the literature. J Orthop Surg Res. 2012;7:36.
42. Standaert, CJ, Friedly J, Erwin MW, et al. Comparative effectiveness of exercise, acupuncture, and spinal manipulation for low back pain. Spine (Phila PA 1976). 2011;36(21 suppl):S120-S130.
43. Kwon YD, Pittler MH, Ernst E. Acupuncture for peripheral joint osteoarthritis: a systematic review and meta-analysis. Rheumatology (Oxford). 2006;45(11):1331-1337.
44. Vickers AJ, Cronin AM, Maschino AC, et al; Acupuncture Trialists’ Collaboration. Individual patient data meta-analysis of acupuncture for chronic pain: protocol of the Acupuncture Trialists’ Collaboration. Trials. 2010;11:90.
45. Kelly RB. Acupuncture for pain. Am Fam Physician. 2009;80(5):481-484.
46. Witt CM, Schützler L, Lüdtke R, Wegscheider K, Willich SN. Patient characteristics and variation in treatment outcomes: which patients benefit most from acupuncture for chronic pain? Clin J Pain. 2011;27(6):550-555.
47. Cafarelli E, Flint F. The role of massage in preparation for and recovery from exercise: an overview. Sports Med. 1992;14(1):1-9.
48. Prentice WE. Therapeutic massage. In: Prentice WE. Therapeutic Modalities in Rehabilitation. 4th ed. New York, NY: McGraw-Hill; 2011:chap 16.
49. Wolsko PM, Eisenberg DM, Davis RB, Kessler R, Phillips RS. Patterns and perceptions of care for treatment of back and neck pain: results of a national survey. Spine (Phila PA 1976). 2003;28(3):292-297.
50. Perlman AI, Sabina A, Williams AL, Njike VY, Katz DL. Massage therapy for osteoarthritis of the knee: a randomized controlled trial. Arch Intern Med. 2006;166(22):2533-2538.
51. Tsao JCI. Effectiveness of massage therapy for chronic, non-malignant pain: a review. Evid Based Complement Alternat Med. 2007;4(2):165-179.
1. Callahan LF, Wiley-Exley EK, Mielenz TJ, et al. Use of complementary and alternative medicine among patients with arthritis. Prev Chronic Dis. 2009;6(2):A44.
2. Walsh NE, Brooks P, Hazes JM, et al; Bone and Joint Decade Task Force for Standards of Care for Acute and Chronic Musculoskeletal Pain. Standards of care for acute and chronic musculoskeletal pain: the Bone and Joint Decade (2000-2010). Arch Phys Med Rehabil. 2008;89(9):1830-1845.
3. Williamson AT, Fletcher PC, Dawson KA. Complementary and alternative medicine. Use in an older population. J Gerontol Nurs. 2003;29(5):20-28.
4. Artus M, Croft P, Lewis M. The use of CAM and conventional treatments among primary care consulters with chronic musculoskeletal pain. BMC Fam Pract. 2007;8:26.
5. Cherkin DC, Sherman KJ, Kahn J, et al. A comparison of the effects of 2 types of massage and usual care on chronic low back pain: a randomized controlled trial. Ann Intern Med. 2011;155(1):1-9.
6. Fleming S, Rabago DP, Mundt MP, Fleming MF. CAM therapies among primary care patients using opioid therapy for chronic pain. BMC Complement Altern Med. 2007;7:15.
7. Lew HL, Otis JD, Tun C, Kerns RD, Clark ME, Cifu DX. Prevalence of chronic pain, posttraumatic stress disorder, and persistent post concussive symptoms in OIF/OEF veterans: polytrauma clinical triad. J Rehabil Res Dev. 2009;46(6):697-702.
8. Trinh K, Graham N, Gross A, et al. Acupuncture for neck disorders. Spine (Phila PA 1976). 2007;32(2):236-243.
9. Gaskin DJ, Richard P. Appendix C: The economic costs of pain in the United States. In: Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: National Academies Press; 2011. National Center for Biotechnology Information Website. http://www. ncbi.nlm.nih.gov/books/NBK92521. Accessed July 31, 2015.
10. American Academy of Pain Medicine. AAPM facts and figures on pain. American Academy of Pain Medicine Website. http://www.painmed.org/files/facts-and-figures-on-pain.pdf. Accessed July 31, 2015.
11. Rosenquist RW, Vrooman MD. Chronic pain management. In: Butterworth JF, Mackey DC, Wasnick JD, eds. Morgan & Mikhail’s Clinical Anesthesiology. 5th ed. New York, NY: McGraw-Hill; 2013:chap 47.
12. Rasu RS, Sohraby R, Cunningham L, Knell ME. Assessing chronic pain treatment practices and evaluating adherence to chronic pain clinical guidelines in outpatient practices in the United States. J Pain. 2013;14(6):568-578.
13. Gureje O, Von Korff M, Simon, GE, Grater R. Persistent pain and well-being: a World Health Organization study in primary care. JAMA. 1998;280(2):147-151.
14. Hopton A, MacPherson H. Acupuncture for chronic pain: is acupuncture more than an effective placebo? A systematic review of pooled data from meta-analyses. Pain Pract. 2010;10(2):94-102.
15. Kumar N. WHO Normative guidelines on pain management. World Health Organization Website. http://www.who.int/medicines/areas/quality_safety/delphi_study_pain_guidelines.pdf. Published June 2007. Accessed August 3, 2015.
16. Koffman RL. Downrange acupuncture. Med Acupunct. 2011;23(4):215-218.
17. Denneson LM, Corson K, Dobscha SK. Complementary and alternative medicine use among veterans with chronic noncancer pain. J Rehabil Res Dev. 2011;(48)9:1119-1128.
18. White MR, Jacobson IG, Smith B, et al; Millennium Cohort Study Team. Health care utilization among complementary and alternative medicine users in a large military cohort. BMC Complement Alternat Med. 2011;11:27.
19. U.S. Department of Health and Human Services, National Institutes of Health, National Center for Complementary and Alternative Medicine. Complementary, alternative, or integrative health: What’s in a name? National Center for Complementary and Alternative Medicine Website. http://nccam.nih.gov/health/whatiscam. Updated March 2015. Modified July 8, 2015. Accessed August 4, 2015.
20. Nahin RL, Barnes PM, Stussman BJ, Bloom B. Costs of complementary and alternative medicine (CAM) and frequency of visits to CAM practitioners: United States, 2007. Natl Health Stat Report. 2009;30(18):1-14.
21. Astin JA. Why patients use alternative medicine: results of a national study. JAMA. 1998;279(19):1548-1553.
22. Rosenberg EI, Genao I, Chen I, et al. Complementary and alternative medicine use in primary care patients with chronic pain. Pain Med. 2008;9(8):1065-1072.
23. Alaaeddine N, Okais J, Ballane L, Baddoura RM. Use of complementary and alternative therapy among patients with rheumatoid arthritis and osteoarthritis. J Clin Nurs. 2012;21(21-22):3198-3204.
24. Tan MG, Win MT, Khan SA. The use of complementary and alternative medicine in chronic pain patients in Singapore: a single-centre study. Ann Acad Med Singapore. 2013;42(3):133-137.
25. White P. A background to acupuncture and its use in chronic painful musculoskeletal conditions. J R Soc Promot Health. 2006;126(5):219-227.
26. U.S. Department of Health and Human Services, National Institutes of Health, Office of Dietary Supplements. Dietary Supplement Health and Education Act of 1994. National Institutes of Health Website. http://ods.od.nih.gov/About/DSHEA_Wording.aspx. Published October 25, 1994. Accessed August 4, 2015.
27. Su D, Li L. Trends in the use of complementary and alternative medicine in the United States: 2002-2007. J Health Care Poor Underserved. 2011;22(1):296-310.
28. Sherman KJ, Cherkin DC, Connelly MT, et al. Complementary and alternative medical therapies for chronic low back pain: what treatments are patients willing to try? BMC Complement Alternat Med. 2004;4:9.
29. Smeeding SJ, Bradshaw DH, Kumpfer KL, Trevithick S, Stoddard GJ. Outcome evaluation of the Veterans Affairs Salt Lake City Integrative Health Clinic for Chronic Nonmalignant Pain. Clin J Pain. 2011;27(2):146-155.
30. U.S. Department of Veterans Affairs, Veterans Health Administration, Office of the Assistant Deputy Under Secretary for Health for Policy and Planning. 2011 complementary and alternative medicine. U.S. Department of Veterans Affairs Office of Research and Development Website. http://www.research.va.gov/research_topics/2011cam_finalreport.pdf. Published September 2011. Accessed August 4, 2015.
31. Unsal A, Gözüm S. Use of complementary and alternative medicine by patients with arthritis. J Clin Nurs. 2010;19(7-8):1129-1138.
32. Patel KC, Gross A, Graham N, et al. Massage for mechanical neck disorder. Cochrane Database Syst Rev. 2012;9:CD004871.
33. Kong LJ, Zhan HS, Cheng YW, Yuan WA, Chen B, Fang M. Massage therapy for neck and shoulder pain: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:613279.
34. Gross A, Miller J, D’Sylva J, et al; COG. Manipulation or mobilisation for neck pain: a Cochrane review. Man Ther. 2010;15(4):315-333.
35. Furlan A, Yazdi F, Tsertsvadze A, et al. Complementary and alternative therapies for back Pain II. Evidence report/technology assessment No. 194. (Prepared by the University of Ottawa Evidence-based Practice Center under Contract No. 290-2007-10059-I (EPCIII). AHRQ Publication No. 10(11)E007. Rockville, MD: Agency for Healthcare Research and Quality; 2010.
36. Yuan J, Purepong N, Kerr DP, Park J, Bradbury I, McDonough S. Effectiveness of acupuncture for low back pain. Spine (Phila PA 1976). 2008;33(23):E887-E900.
37. Manheimer E, White A, Berman B, Forys K, Ernst E. Meta-analysis: acupuncture for low back pain. Ann Intern Med. 2005;142(8):651-663.
38. Rubinstein SM, van Middelkoop M, Kuijpers T, et al. A systematic review on the effectiveness of complementary and alternative medicine for chronic non-specific low-back pain. Eur Spine J. 2010;19(8):1213-1228.
39. Cao L, Zhang XL, Gao YS, Jiang Y. Needle acupuncture for osteoarthritis of the knee. A systematic review and updated meta-analysis. Saudi Med J. 2012;33(5):526-532.
40. White A, Foster NE, Cummings M, Barlas P. Acupuncture treatment for chronic knee pain: a systematic review. Rheumatology (Oxford). 2007;46(3):384-390.
41. Hutchinson AJ, Ball S, Andrews JC, Jones GG. The effectiveness of acupuncture in treating chronic non-specific low back pain: a systematic review of the literature. J Orthop Surg Res. 2012;7:36.
42. Standaert, CJ, Friedly J, Erwin MW, et al. Comparative effectiveness of exercise, acupuncture, and spinal manipulation for low back pain. Spine (Phila PA 1976). 2011;36(21 suppl):S120-S130.
43. Kwon YD, Pittler MH, Ernst E. Acupuncture for peripheral joint osteoarthritis: a systematic review and meta-analysis. Rheumatology (Oxford). 2006;45(11):1331-1337.
44. Vickers AJ, Cronin AM, Maschino AC, et al; Acupuncture Trialists’ Collaboration. Individual patient data meta-analysis of acupuncture for chronic pain: protocol of the Acupuncture Trialists’ Collaboration. Trials. 2010;11:90.
45. Kelly RB. Acupuncture for pain. Am Fam Physician. 2009;80(5):481-484.
46. Witt CM, Schützler L, Lüdtke R, Wegscheider K, Willich SN. Patient characteristics and variation in treatment outcomes: which patients benefit most from acupuncture for chronic pain? Clin J Pain. 2011;27(6):550-555.
47. Cafarelli E, Flint F. The role of massage in preparation for and recovery from exercise: an overview. Sports Med. 1992;14(1):1-9.
48. Prentice WE. Therapeutic massage. In: Prentice WE. Therapeutic Modalities in Rehabilitation. 4th ed. New York, NY: McGraw-Hill; 2011:chap 16.
49. Wolsko PM, Eisenberg DM, Davis RB, Kessler R, Phillips RS. Patterns and perceptions of care for treatment of back and neck pain: results of a national survey. Spine (Phila PA 1976). 2003;28(3):292-297.
50. Perlman AI, Sabina A, Williams AL, Njike VY, Katz DL. Massage therapy for osteoarthritis of the knee: a randomized controlled trial. Arch Intern Med. 2006;166(22):2533-2538.
51. Tsao JCI. Effectiveness of massage therapy for chronic, non-malignant pain: a review. Evid Based Complement Alternat Med. 2007;4(2):165-179.