User login
A 73-year-old woman is urgently referred to dermatology for evaluation of a facial lesion. It is unclear how long the lesion has been present, but it has caused great alarm to the patient's visiting relatives. The patient herself is not at all worried, saying that she doubts “a little thing like that could cause too much trouble.”
She denies any symptoms associated with the lesion and claims to be in good health. There is no history of weight loss, cough, or changes in mentation or gastrointestinal/genitourinary function. She admits to some sun exposure as a young adult but claims she has never been sunburned; she reports tanning easily and holding a tan well.
EXAMINATION
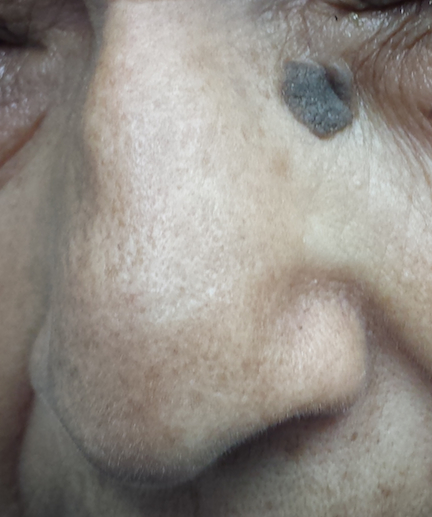
The lesion is a 1.4-cm round epidermal plaque with a rough, warty surface. It is located in the left lower medial epicanthal area, verging on the upper nasal sidewall. Its dark brown color is uniform, as is its surface texture. It appears in the context of the patient’s relatively dark type III skin, which is largely free of signs of sun damage.
PROCEDURE
After potential treatments are discussed with the patient, she opts to have cryosurgery. During the procedure, it is noted that the lesion remained white for several seconds after it was frozen.
Two months later, the site is rechecked. The lesion is virtually gone, except for a faint shadow of hyperpigmentation in the treated area.
Continue for Joe Monroe's discussion >>
DISCUSSION
The top three problems for which patients are seen in dermatology are acne, warts, and seborrheic keratoses (SK). The last are, hands down, the most common problem I see. With their dark color and raised surface, they epitomize what patients imagine skin cancer to look like.
Very likely, given the lesion’s size and location, it had been there for quite some time. But to the visiting relatives who hadn’t seen the patient in a while, it was new and alarming. (“Are you sure?” one of them asked when the patient shrugged off any concerns. “It looks so ugly!”)
I understand why SKs are worrisome to patients and their families. But, as a matter of fact, I was sure this lesion was safe. Why? Here are some reasons:
1. The lesion was epidermal in nature—that is, “stuck on” the surface of the skin, as opposed to being in, or part of, it. Epidermal lesions are almost always safe; intradermal ones, while not necessarily "bad," tend to require more attention.
2. Warty and rough are both good signs, dermatologically speaking.
3. Uniformity in color, texture, and borders is also usually positive; the "bad stuff" tends to be somewhat irregular in all three respects.
4. Cryo-white is our term for “stays white after treatment with liquid nitrogen." By contrast, things like skin cancer thaw almost instantly. Why? The blood supply to a cancerous lesion is far better than that to an epidermal SK, which has little if any vascularization. Warm blood dissipates the cold quickly.
5. Liquid nitrogen also highlights another diagnostic feature of SKs: pseudocysts. Peculiar to SKs, these porelike surface features are usually seen as minute follicular orifices.
6. Other diagnostic features of SKs: Most affected patients have several similar lesions. Usually, the history of SK is that it’s "been there forever,” although this case illustrates an exception. SKs are typically seen in older people, but I’ve seen them on teenagers, too.
The introduction of the liquid nitrogen gun 35 years ago made SK treatment much easier and provided a potential diagnostic tool. We often use cryotherapy as a kind of final test of whether a lesion is benign or malignant. If the lesion responds to routine cryotherapy by resolving, chances are quite good it was benign. If it doesn’t, you may need to reconsider your diagnosis.
TAKE-HOME LEARNING POINTS
• SKs are extremely common, often numerous, and favor older patients.
• SKs are usually rough, epidermal, round to oval, and tan to dark brown.
• SKs, treated with liquid nitrogen, turn white and stay that way for a few seconds at least, while the dangerous lookalikes (eg, melanoma) thaw much more quickly.
• Liquid nitrogen treatment can help with diagnosis: If the treated lesion fails to disappear as intended, it might not be an SK after all. (Note, however, that this process can take up to two weeks.)
• Liquid nitrogen also highlights surface pseudocysts, which are pathognomic for SKs.
• When cryotherapy fails to elicit the desired changes, the lesion needs to be biopsied.
A 73-year-old woman is urgently referred to dermatology for evaluation of a facial lesion. It is unclear how long the lesion has been present, but it has caused great alarm to the patient's visiting relatives. The patient herself is not at all worried, saying that she doubts “a little thing like that could cause too much trouble.”
She denies any symptoms associated with the lesion and claims to be in good health. There is no history of weight loss, cough, or changes in mentation or gastrointestinal/genitourinary function. She admits to some sun exposure as a young adult but claims she has never been sunburned; she reports tanning easily and holding a tan well.
EXAMINATION
The lesion is a 1.4-cm round epidermal plaque with a rough, warty surface. It is located in the left lower medial epicanthal area, verging on the upper nasal sidewall. Its dark brown color is uniform, as is its surface texture. It appears in the context of the patient’s relatively dark type III skin, which is largely free of signs of sun damage.
PROCEDURE
After potential treatments are discussed with the patient, she opts to have cryosurgery. During the procedure, it is noted that the lesion remained white for several seconds after it was frozen.
Two months later, the site is rechecked. The lesion is virtually gone, except for a faint shadow of hyperpigmentation in the treated area.
Continue for Joe Monroe's discussion >>
DISCUSSION
The top three problems for which patients are seen in dermatology are acne, warts, and seborrheic keratoses (SK). The last are, hands down, the most common problem I see. With their dark color and raised surface, they epitomize what patients imagine skin cancer to look like.
Very likely, given the lesion’s size and location, it had been there for quite some time. But to the visiting relatives who hadn’t seen the patient in a while, it was new and alarming. (“Are you sure?” one of them asked when the patient shrugged off any concerns. “It looks so ugly!”)
I understand why SKs are worrisome to patients and their families. But, as a matter of fact, I was sure this lesion was safe. Why? Here are some reasons:
1. The lesion was epidermal in nature—that is, “stuck on” the surface of the skin, as opposed to being in, or part of, it. Epidermal lesions are almost always safe; intradermal ones, while not necessarily "bad," tend to require more attention.
2. Warty and rough are both good signs, dermatologically speaking.
3. Uniformity in color, texture, and borders is also usually positive; the "bad stuff" tends to be somewhat irregular in all three respects.
4. Cryo-white is our term for “stays white after treatment with liquid nitrogen." By contrast, things like skin cancer thaw almost instantly. Why? The blood supply to a cancerous lesion is far better than that to an epidermal SK, which has little if any vascularization. Warm blood dissipates the cold quickly.
5. Liquid nitrogen also highlights another diagnostic feature of SKs: pseudocysts. Peculiar to SKs, these porelike surface features are usually seen as minute follicular orifices.
6. Other diagnostic features of SKs: Most affected patients have several similar lesions. Usually, the history of SK is that it’s "been there forever,” although this case illustrates an exception. SKs are typically seen in older people, but I’ve seen them on teenagers, too.
The introduction of the liquid nitrogen gun 35 years ago made SK treatment much easier and provided a potential diagnostic tool. We often use cryotherapy as a kind of final test of whether a lesion is benign or malignant. If the lesion responds to routine cryotherapy by resolving, chances are quite good it was benign. If it doesn’t, you may need to reconsider your diagnosis.
TAKE-HOME LEARNING POINTS
• SKs are extremely common, often numerous, and favor older patients.
• SKs are usually rough, epidermal, round to oval, and tan to dark brown.
• SKs, treated with liquid nitrogen, turn white and stay that way for a few seconds at least, while the dangerous lookalikes (eg, melanoma) thaw much more quickly.
• Liquid nitrogen treatment can help with diagnosis: If the treated lesion fails to disappear as intended, it might not be an SK after all. (Note, however, that this process can take up to two weeks.)
• Liquid nitrogen also highlights surface pseudocysts, which are pathognomic for SKs.
• When cryotherapy fails to elicit the desired changes, the lesion needs to be biopsied.
A 73-year-old woman is urgently referred to dermatology for evaluation of a facial lesion. It is unclear how long the lesion has been present, but it has caused great alarm to the patient's visiting relatives. The patient herself is not at all worried, saying that she doubts “a little thing like that could cause too much trouble.”
She denies any symptoms associated with the lesion and claims to be in good health. There is no history of weight loss, cough, or changes in mentation or gastrointestinal/genitourinary function. She admits to some sun exposure as a young adult but claims she has never been sunburned; she reports tanning easily and holding a tan well.
EXAMINATION
The lesion is a 1.4-cm round epidermal plaque with a rough, warty surface. It is located in the left lower medial epicanthal area, verging on the upper nasal sidewall. Its dark brown color is uniform, as is its surface texture. It appears in the context of the patient’s relatively dark type III skin, which is largely free of signs of sun damage.
PROCEDURE
After potential treatments are discussed with the patient, she opts to have cryosurgery. During the procedure, it is noted that the lesion remained white for several seconds after it was frozen.
Two months later, the site is rechecked. The lesion is virtually gone, except for a faint shadow of hyperpigmentation in the treated area.
Continue for Joe Monroe's discussion >>
DISCUSSION
The top three problems for which patients are seen in dermatology are acne, warts, and seborrheic keratoses (SK). The last are, hands down, the most common problem I see. With their dark color and raised surface, they epitomize what patients imagine skin cancer to look like.
Very likely, given the lesion’s size and location, it had been there for quite some time. But to the visiting relatives who hadn’t seen the patient in a while, it was new and alarming. (“Are you sure?” one of them asked when the patient shrugged off any concerns. “It looks so ugly!”)
I understand why SKs are worrisome to patients and their families. But, as a matter of fact, I was sure this lesion was safe. Why? Here are some reasons:
1. The lesion was epidermal in nature—that is, “stuck on” the surface of the skin, as opposed to being in, or part of, it. Epidermal lesions are almost always safe; intradermal ones, while not necessarily "bad," tend to require more attention.
2. Warty and rough are both good signs, dermatologically speaking.
3. Uniformity in color, texture, and borders is also usually positive; the "bad stuff" tends to be somewhat irregular in all three respects.
4. Cryo-white is our term for “stays white after treatment with liquid nitrogen." By contrast, things like skin cancer thaw almost instantly. Why? The blood supply to a cancerous lesion is far better than that to an epidermal SK, which has little if any vascularization. Warm blood dissipates the cold quickly.
5. Liquid nitrogen also highlights another diagnostic feature of SKs: pseudocysts. Peculiar to SKs, these porelike surface features are usually seen as minute follicular orifices.
6. Other diagnostic features of SKs: Most affected patients have several similar lesions. Usually, the history of SK is that it’s "been there forever,” although this case illustrates an exception. SKs are typically seen in older people, but I’ve seen them on teenagers, too.
The introduction of the liquid nitrogen gun 35 years ago made SK treatment much easier and provided a potential diagnostic tool. We often use cryotherapy as a kind of final test of whether a lesion is benign or malignant. If the lesion responds to routine cryotherapy by resolving, chances are quite good it was benign. If it doesn’t, you may need to reconsider your diagnosis.
TAKE-HOME LEARNING POINTS
• SKs are extremely common, often numerous, and favor older patients.
• SKs are usually rough, epidermal, round to oval, and tan to dark brown.
• SKs, treated with liquid nitrogen, turn white and stay that way for a few seconds at least, while the dangerous lookalikes (eg, melanoma) thaw much more quickly.
• Liquid nitrogen treatment can help with diagnosis: If the treated lesion fails to disappear as intended, it might not be an SK after all. (Note, however, that this process can take up to two weeks.)
• Liquid nitrogen also highlights surface pseudocysts, which are pathognomic for SKs.
• When cryotherapy fails to elicit the desired changes, the lesion needs to be biopsied.
