User login
Investigators involved in heart-brain medicine are dedicated to defining the physiology associated with interactions of the neurological and cardiovascular systems. In 2004 the Bakken Heart-Brain Institute was founded at Cleveland Clinic because we believed that furthering our understanding of this physiology could lead to a better understanding of chronic disease, define novel therapies, and improve patient outcomes.
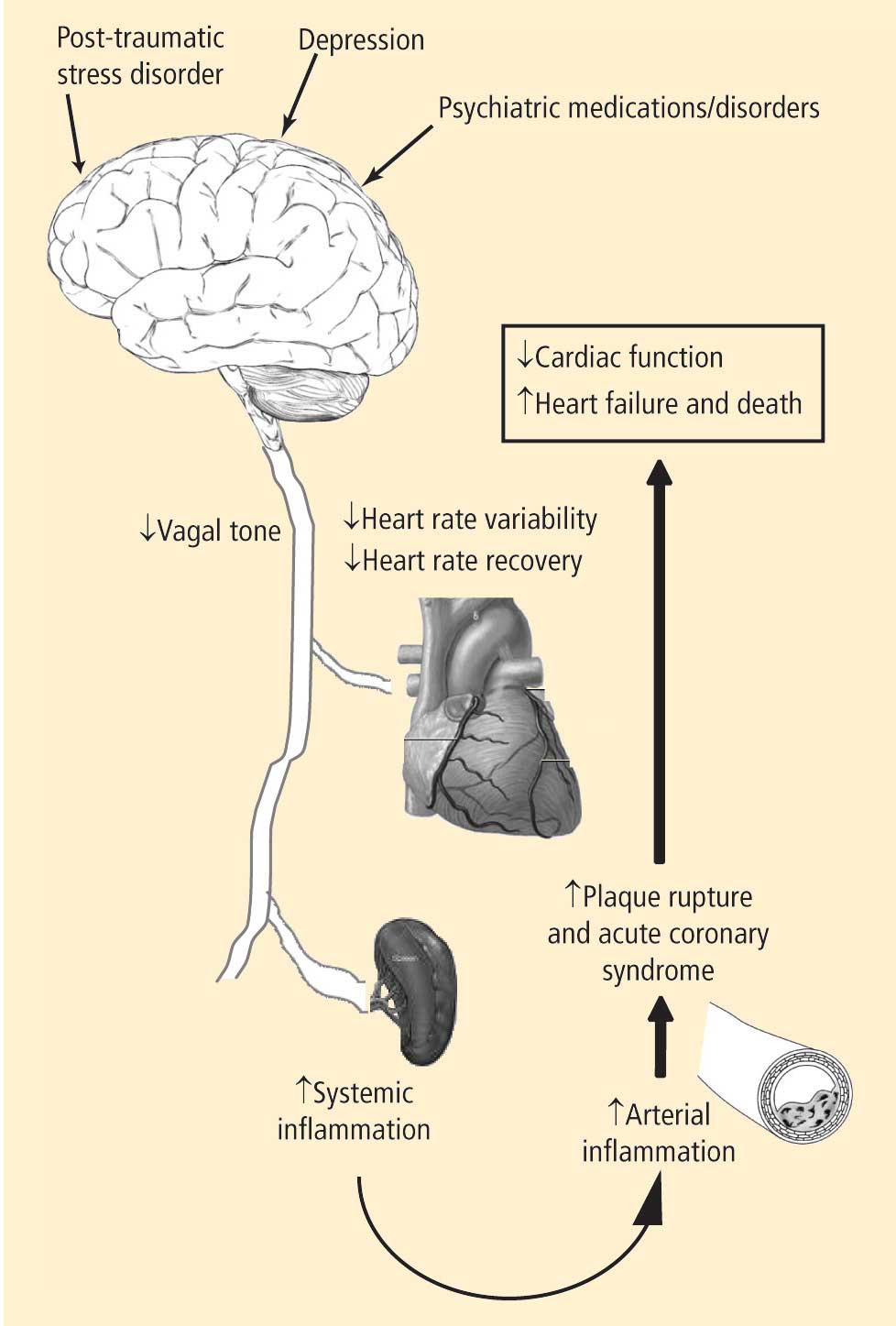
- Depression leads to decreased vagal tone
- Decreased vagal tone leads to increased inflammation
- Increased inflammation leads to acute coronary syndrome.
Speakers at the 2008 Summit offered insights into the physiology, clinical measures, and molecular pathways involved in linking the heart and the brain, including:
- Measures of heart rate variability in depression
- The utility of heart rate variability and heart rate recovery in quantifying vagal tone and outcome in patients with and without coronary artery disease
- Pathways of inflammation involved in acute coronary syndrome.
MOUNTING CLINICAL EVIDENCE LINKING DEPRESSION WITH CARDIAC OUTCOMES
The 2007 and 2008 Summits highlighted the link between depression and outcomes in patients with atherosclerosis (2007)1 and the potential associated mechanisms (2008). Just as exciting are the developments since last June: numerous papers have been published demonstrating this link in clinical populations, and depression screening has been included in recommendations from the American Heart Association on the treatment of patients with coronary artery disease—recommendations that are endorsed by the American Psychiatric Association.2
The studies published since June 2008 demonstrate clear links between depression and morbidity and mortality from cardiovascular causes. A recent paper from the Nurses’ Health Study showed that individuals with depression had a higher incidence of cardiovascular death.3 Notably, subjects in the Nurses’ Health Study had no clinical evidence of atherosclerotic heart disease at enrollment. In another recent study, depression was associated with worse outcomes in patients following coronary stenting.4 Finally, and most interestingly, depression was recently associated with endothelial dysfunction in patients with atypical angina and angiographically normal coronary arteries.5 Thus, regardless of the degree of underlying atherosclerosis, depression is associated with cardiovascular morbidity or mortality.
Less clear is the relationship between depression and inflammation as measured by surrogate inflammatory markers. An analysis of the Canadian Nova Scotia Health Survey [NSHS95] Prospective Population Study suggested that increased inflammatory markers accounted for only a small portion of the risk of coronary heart disease associated with depression.6 Conversely, a recent analysis of patients with stable coronary artery disease demonstrated a strong correlation between major depressive disorders and highsensitivity C-reactive protein.7
Clearly, significant work has yet to be done to fully elucidate the molecular pathways that link depression and adverse outcomes in patients at risk for coronary artery disease. That said, it is very encouraging that professional societies are beginning to recognize the value and importance of heart-brain medicine in identifying novel strategies for improving patient outcomes.
STILL ELUSIVE: EVIDENCE THAT DEPRESSION THERAPY IMPROVES CARDIAC OUTCOMES
At the 2008 Summit there was clear enthusiasm among attendees and faculty for advances in our understanding of the pathways discussed above. Since then, as reviewed above, significant publications have furthered the link between heart and brain in the setting of atherosclerotic heart disease. That said, the missing piece—the demonstration that treating depression leads to improved outcomes in patients with coronary artery disease—remains missing.
Some advances in this regard have been made. A recent study from the Enhancing Recovery In Coronary Heart Disease (ENRICHD) clinical trial demonstrated that major depression in any patient who survived myocardial infarction decreased survival over 2.5 years.8 Interestingly, and perhaps critical for an event-driven treatment trial in the future, this analysis showed an even worse outcome in patients who experienced their initial episode of major depression after their myocardial infarction.8 The need, ethics, and design of clinical trials to determine whether treatment of depression leads to improved outcomes in patients with coronary artery disease will be a major topic of the 4th Annual Heart-Brain Summit, to be held in Chicago on October 15–16, 2009.
OTHER HIGHLIGHTS, INCLUDING ROLE OF THE HEALING ENVIRONMENT
While much of the early focus of the 2008 Heart-Brain Summit was on the interaction of depression, inflammation, and outcomes in patients with coronary artery disease, a significant portion of the Summit identified other disease states and opportunities. The disease states discussed can be divided into primary cardiac, primary psychiatric, and primary neurologic. Cardiac topics under continued investigation include the role of vagal tone on the inflammatory response that regulates left ventricular remodeling following acute myocardial infarction9 as well as the role of spinal stimulation for treatment of refractory myocardial ischemia. Psychiatric disorders of interest that have been shown to modulate vagal tone include post-traumatic stress disorder,10 which has also been shown to increase the risk for coronary heart disease.11,12 Neurologically, advances concerning the polyvagal theory of autonomic nervous system control and cardiac control were discussed.13,14
On the Summit’s final day, the discussions of neuropathways, inflammation, and cardiac control gave way to presentations on the role of the healing environment. Following discussions of how depression can have significant ramifications on systemic inflammation and acute coronary syndrome, it was interesting to review data on how the presence of family and the patient environment can improve patient outcomes.
Many of the topics touched on above are discussed in greater detail in the following pages of this proceedings of the 2008 Bakken Heart-Brain Summit. We are gratified to see the advancements in the field of heartbrain medicine over the past 5 years, and especially to see the recognition the discipline is receiving in our attempt to improve patient outcomes.
FAR MORE QUESTIONS REMAIN
Without a doubt there are more questions than answers at this time. That said, by continuing the rigorous multidisciplinary approach that has served this field well to date, many questions will be answered. We hope you will join us in Chicago on October 15–16, 2009, for the 4th Annual Heart-Brain Summit, which will be jointly hosted by the Society of Heart-Brain Medicine and the Bakken Heart-Brain Institute.
- Penn MS, Bakken EE. Heart-brain medicine: update 2007. Cleve Clin J Med 2008; 75( suppl 2):S3–S4.
- Lichtman JH, Bigger JT, Blumenthal JA, et al. Depression and coronary heart disease: recommendations for screening, referral, and treatment: a science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care and Outcomes Research. Endorsed by the American Psychiatric Association. Circulation 2008; 118:1768–1775.
- Whang W, Kubzansky LD, Kawachi I, et al. Depression and risk of sudden cardiac death and coronary heart disease in women: results from the Nurses’ Health Study. J Am Coll Cardiol 2009; 53:950–958.
- Frazier L, Vaughn W, Willerson J, Ballantyne C, Boerwinkle E Inflammatory protein levels and depression screening after coronary stenting predict major adverse coronary events [published online ahead of print February 26, 2009]. Biol Res Nurs. doi:10.1177/1099800409332801.
- Kim JH, Kim JW, Ko YH, et al Coronary endothelial dysfunction associated with a depressive mood in patients with atypical angina but angiographically normal coronary artery [published online ahead of print March 7, 2009]. Int J Cardiol. doi:10.1016/j.ijcard.2009.02.004.
- Davidson KW, Schwartz JE, Kirkland SA, et al. Relation of inflammation to depression and incident coronary heart disease (from the Canadian Nova Scotia Health Survey [NSHS95] Prospective Population Study). Am J Cardiol 2009; 103:755–761.
- Bankier B, Barajas J, Martinez-Rumayor A, Januzzi JL. Association between major depressive disorder and C-reactive protein levels in stable coronary heart disease patients. J Psychosom Res 2009; 66:189–194.
- Carney RM, Freedland KE, Steinmeyer B, et al History of depression and survival after acute myocardial infarction [published online ahead of print February 27, 2009]. Psychosom Med. doi:10.1097/PSY.0b013e31819b69e3.
- Vasilyev N, Williams T, Brennan ML, et al. Myeloperoxidase-generated oxidants modulate left ventricular remodeling but not infarct size after myocardial infarction. Circulation 2005; 112:2812–2820.
- Sack M, Hopper JW, Lamprecht F. Low respiratory sinus arrhythmia and prolonged psychophysiological arousal in posttraumatic stress disorder: heart rate dynamics and individual differences in arousal regulation. Biol Psychiatry 2004; 55:284–290.
- Kubzansky LD, Koenen KC, Jones C, Eaton WW. A prospective study of posttraumatic stress disorder symptoms and coronary heart disease in women. Health Psychol 2009; 28:125–130.
- Kubzansky LD, Koenen KC, Spiro A, Vokonas PS, Sparrow D. Prospective study of posttraumatic stress disorder symptoms and coronary heart disease in the Normative Aging Study. Arch Gen Psychiatry 2007; 64:109–116.
- Porges SW. The polyvagal perspective. Biol Psychol 2007; 74:116–143.
- Porges SW. The polyvagal theory: phylogenetic substrates of a social nervous system. Int J Psychophysiol 2001; 42:123–146.
Investigators involved in heart-brain medicine are dedicated to defining the physiology associated with interactions of the neurological and cardiovascular systems. In 2004 the Bakken Heart-Brain Institute was founded at Cleveland Clinic because we believed that furthering our understanding of this physiology could lead to a better understanding of chronic disease, define novel therapies, and improve patient outcomes.
- Depression leads to decreased vagal tone
- Decreased vagal tone leads to increased inflammation
- Increased inflammation leads to acute coronary syndrome.
Speakers at the 2008 Summit offered insights into the physiology, clinical measures, and molecular pathways involved in linking the heart and the brain, including:
- Measures of heart rate variability in depression
- The utility of heart rate variability and heart rate recovery in quantifying vagal tone and outcome in patients with and without coronary artery disease
- Pathways of inflammation involved in acute coronary syndrome.
MOUNTING CLINICAL EVIDENCE LINKING DEPRESSION WITH CARDIAC OUTCOMES
The 2007 and 2008 Summits highlighted the link between depression and outcomes in patients with atherosclerosis (2007)1 and the potential associated mechanisms (2008). Just as exciting are the developments since last June: numerous papers have been published demonstrating this link in clinical populations, and depression screening has been included in recommendations from the American Heart Association on the treatment of patients with coronary artery disease—recommendations that are endorsed by the American Psychiatric Association.2
The studies published since June 2008 demonstrate clear links between depression and morbidity and mortality from cardiovascular causes. A recent paper from the Nurses’ Health Study showed that individuals with depression had a higher incidence of cardiovascular death.3 Notably, subjects in the Nurses’ Health Study had no clinical evidence of atherosclerotic heart disease at enrollment. In another recent study, depression was associated with worse outcomes in patients following coronary stenting.4 Finally, and most interestingly, depression was recently associated with endothelial dysfunction in patients with atypical angina and angiographically normal coronary arteries.5 Thus, regardless of the degree of underlying atherosclerosis, depression is associated with cardiovascular morbidity or mortality.
Less clear is the relationship between depression and inflammation as measured by surrogate inflammatory markers. An analysis of the Canadian Nova Scotia Health Survey [NSHS95] Prospective Population Study suggested that increased inflammatory markers accounted for only a small portion of the risk of coronary heart disease associated with depression.6 Conversely, a recent analysis of patients with stable coronary artery disease demonstrated a strong correlation between major depressive disorders and highsensitivity C-reactive protein.7
Clearly, significant work has yet to be done to fully elucidate the molecular pathways that link depression and adverse outcomes in patients at risk for coronary artery disease. That said, it is very encouraging that professional societies are beginning to recognize the value and importance of heart-brain medicine in identifying novel strategies for improving patient outcomes.
STILL ELUSIVE: EVIDENCE THAT DEPRESSION THERAPY IMPROVES CARDIAC OUTCOMES
At the 2008 Summit there was clear enthusiasm among attendees and faculty for advances in our understanding of the pathways discussed above. Since then, as reviewed above, significant publications have furthered the link between heart and brain in the setting of atherosclerotic heart disease. That said, the missing piece—the demonstration that treating depression leads to improved outcomes in patients with coronary artery disease—remains missing.
Some advances in this regard have been made. A recent study from the Enhancing Recovery In Coronary Heart Disease (ENRICHD) clinical trial demonstrated that major depression in any patient who survived myocardial infarction decreased survival over 2.5 years.8 Interestingly, and perhaps critical for an event-driven treatment trial in the future, this analysis showed an even worse outcome in patients who experienced their initial episode of major depression after their myocardial infarction.8 The need, ethics, and design of clinical trials to determine whether treatment of depression leads to improved outcomes in patients with coronary artery disease will be a major topic of the 4th Annual Heart-Brain Summit, to be held in Chicago on October 15–16, 2009.
OTHER HIGHLIGHTS, INCLUDING ROLE OF THE HEALING ENVIRONMENT
While much of the early focus of the 2008 Heart-Brain Summit was on the interaction of depression, inflammation, and outcomes in patients with coronary artery disease, a significant portion of the Summit identified other disease states and opportunities. The disease states discussed can be divided into primary cardiac, primary psychiatric, and primary neurologic. Cardiac topics under continued investigation include the role of vagal tone on the inflammatory response that regulates left ventricular remodeling following acute myocardial infarction9 as well as the role of spinal stimulation for treatment of refractory myocardial ischemia. Psychiatric disorders of interest that have been shown to modulate vagal tone include post-traumatic stress disorder,10 which has also been shown to increase the risk for coronary heart disease.11,12 Neurologically, advances concerning the polyvagal theory of autonomic nervous system control and cardiac control were discussed.13,14
On the Summit’s final day, the discussions of neuropathways, inflammation, and cardiac control gave way to presentations on the role of the healing environment. Following discussions of how depression can have significant ramifications on systemic inflammation and acute coronary syndrome, it was interesting to review data on how the presence of family and the patient environment can improve patient outcomes.
Many of the topics touched on above are discussed in greater detail in the following pages of this proceedings of the 2008 Bakken Heart-Brain Summit. We are gratified to see the advancements in the field of heartbrain medicine over the past 5 years, and especially to see the recognition the discipline is receiving in our attempt to improve patient outcomes.
FAR MORE QUESTIONS REMAIN
Without a doubt there are more questions than answers at this time. That said, by continuing the rigorous multidisciplinary approach that has served this field well to date, many questions will be answered. We hope you will join us in Chicago on October 15–16, 2009, for the 4th Annual Heart-Brain Summit, which will be jointly hosted by the Society of Heart-Brain Medicine and the Bakken Heart-Brain Institute.
Investigators involved in heart-brain medicine are dedicated to defining the physiology associated with interactions of the neurological and cardiovascular systems. In 2004 the Bakken Heart-Brain Institute was founded at Cleveland Clinic because we believed that furthering our understanding of this physiology could lead to a better understanding of chronic disease, define novel therapies, and improve patient outcomes.
- Depression leads to decreased vagal tone
- Decreased vagal tone leads to increased inflammation
- Increased inflammation leads to acute coronary syndrome.
Speakers at the 2008 Summit offered insights into the physiology, clinical measures, and molecular pathways involved in linking the heart and the brain, including:
- Measures of heart rate variability in depression
- The utility of heart rate variability and heart rate recovery in quantifying vagal tone and outcome in patients with and without coronary artery disease
- Pathways of inflammation involved in acute coronary syndrome.
MOUNTING CLINICAL EVIDENCE LINKING DEPRESSION WITH CARDIAC OUTCOMES
The 2007 and 2008 Summits highlighted the link between depression and outcomes in patients with atherosclerosis (2007)1 and the potential associated mechanisms (2008). Just as exciting are the developments since last June: numerous papers have been published demonstrating this link in clinical populations, and depression screening has been included in recommendations from the American Heart Association on the treatment of patients with coronary artery disease—recommendations that are endorsed by the American Psychiatric Association.2
The studies published since June 2008 demonstrate clear links between depression and morbidity and mortality from cardiovascular causes. A recent paper from the Nurses’ Health Study showed that individuals with depression had a higher incidence of cardiovascular death.3 Notably, subjects in the Nurses’ Health Study had no clinical evidence of atherosclerotic heart disease at enrollment. In another recent study, depression was associated with worse outcomes in patients following coronary stenting.4 Finally, and most interestingly, depression was recently associated with endothelial dysfunction in patients with atypical angina and angiographically normal coronary arteries.5 Thus, regardless of the degree of underlying atherosclerosis, depression is associated with cardiovascular morbidity or mortality.
Less clear is the relationship between depression and inflammation as measured by surrogate inflammatory markers. An analysis of the Canadian Nova Scotia Health Survey [NSHS95] Prospective Population Study suggested that increased inflammatory markers accounted for only a small portion of the risk of coronary heart disease associated with depression.6 Conversely, a recent analysis of patients with stable coronary artery disease demonstrated a strong correlation between major depressive disorders and highsensitivity C-reactive protein.7
Clearly, significant work has yet to be done to fully elucidate the molecular pathways that link depression and adverse outcomes in patients at risk for coronary artery disease. That said, it is very encouraging that professional societies are beginning to recognize the value and importance of heart-brain medicine in identifying novel strategies for improving patient outcomes.
STILL ELUSIVE: EVIDENCE THAT DEPRESSION THERAPY IMPROVES CARDIAC OUTCOMES
At the 2008 Summit there was clear enthusiasm among attendees and faculty for advances in our understanding of the pathways discussed above. Since then, as reviewed above, significant publications have furthered the link between heart and brain in the setting of atherosclerotic heart disease. That said, the missing piece—the demonstration that treating depression leads to improved outcomes in patients with coronary artery disease—remains missing.
Some advances in this regard have been made. A recent study from the Enhancing Recovery In Coronary Heart Disease (ENRICHD) clinical trial demonstrated that major depression in any patient who survived myocardial infarction decreased survival over 2.5 years.8 Interestingly, and perhaps critical for an event-driven treatment trial in the future, this analysis showed an even worse outcome in patients who experienced their initial episode of major depression after their myocardial infarction.8 The need, ethics, and design of clinical trials to determine whether treatment of depression leads to improved outcomes in patients with coronary artery disease will be a major topic of the 4th Annual Heart-Brain Summit, to be held in Chicago on October 15–16, 2009.
OTHER HIGHLIGHTS, INCLUDING ROLE OF THE HEALING ENVIRONMENT
While much of the early focus of the 2008 Heart-Brain Summit was on the interaction of depression, inflammation, and outcomes in patients with coronary artery disease, a significant portion of the Summit identified other disease states and opportunities. The disease states discussed can be divided into primary cardiac, primary psychiatric, and primary neurologic. Cardiac topics under continued investigation include the role of vagal tone on the inflammatory response that regulates left ventricular remodeling following acute myocardial infarction9 as well as the role of spinal stimulation for treatment of refractory myocardial ischemia. Psychiatric disorders of interest that have been shown to modulate vagal tone include post-traumatic stress disorder,10 which has also been shown to increase the risk for coronary heart disease.11,12 Neurologically, advances concerning the polyvagal theory of autonomic nervous system control and cardiac control were discussed.13,14
On the Summit’s final day, the discussions of neuropathways, inflammation, and cardiac control gave way to presentations on the role of the healing environment. Following discussions of how depression can have significant ramifications on systemic inflammation and acute coronary syndrome, it was interesting to review data on how the presence of family and the patient environment can improve patient outcomes.
Many of the topics touched on above are discussed in greater detail in the following pages of this proceedings of the 2008 Bakken Heart-Brain Summit. We are gratified to see the advancements in the field of heartbrain medicine over the past 5 years, and especially to see the recognition the discipline is receiving in our attempt to improve patient outcomes.
FAR MORE QUESTIONS REMAIN
Without a doubt there are more questions than answers at this time. That said, by continuing the rigorous multidisciplinary approach that has served this field well to date, many questions will be answered. We hope you will join us in Chicago on October 15–16, 2009, for the 4th Annual Heart-Brain Summit, which will be jointly hosted by the Society of Heart-Brain Medicine and the Bakken Heart-Brain Institute.
- Penn MS, Bakken EE. Heart-brain medicine: update 2007. Cleve Clin J Med 2008; 75( suppl 2):S3–S4.
- Lichtman JH, Bigger JT, Blumenthal JA, et al. Depression and coronary heart disease: recommendations for screening, referral, and treatment: a science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care and Outcomes Research. Endorsed by the American Psychiatric Association. Circulation 2008; 118:1768–1775.
- Whang W, Kubzansky LD, Kawachi I, et al. Depression and risk of sudden cardiac death and coronary heart disease in women: results from the Nurses’ Health Study. J Am Coll Cardiol 2009; 53:950–958.
- Frazier L, Vaughn W, Willerson J, Ballantyne C, Boerwinkle E Inflammatory protein levels and depression screening after coronary stenting predict major adverse coronary events [published online ahead of print February 26, 2009]. Biol Res Nurs. doi:10.1177/1099800409332801.
- Kim JH, Kim JW, Ko YH, et al Coronary endothelial dysfunction associated with a depressive mood in patients with atypical angina but angiographically normal coronary artery [published online ahead of print March 7, 2009]. Int J Cardiol. doi:10.1016/j.ijcard.2009.02.004.
- Davidson KW, Schwartz JE, Kirkland SA, et al. Relation of inflammation to depression and incident coronary heart disease (from the Canadian Nova Scotia Health Survey [NSHS95] Prospective Population Study). Am J Cardiol 2009; 103:755–761.
- Bankier B, Barajas J, Martinez-Rumayor A, Januzzi JL. Association between major depressive disorder and C-reactive protein levels in stable coronary heart disease patients. J Psychosom Res 2009; 66:189–194.
- Carney RM, Freedland KE, Steinmeyer B, et al History of depression and survival after acute myocardial infarction [published online ahead of print February 27, 2009]. Psychosom Med. doi:10.1097/PSY.0b013e31819b69e3.
- Vasilyev N, Williams T, Brennan ML, et al. Myeloperoxidase-generated oxidants modulate left ventricular remodeling but not infarct size after myocardial infarction. Circulation 2005; 112:2812–2820.
- Sack M, Hopper JW, Lamprecht F. Low respiratory sinus arrhythmia and prolonged psychophysiological arousal in posttraumatic stress disorder: heart rate dynamics and individual differences in arousal regulation. Biol Psychiatry 2004; 55:284–290.
- Kubzansky LD, Koenen KC, Jones C, Eaton WW. A prospective study of posttraumatic stress disorder symptoms and coronary heart disease in women. Health Psychol 2009; 28:125–130.
- Kubzansky LD, Koenen KC, Spiro A, Vokonas PS, Sparrow D. Prospective study of posttraumatic stress disorder symptoms and coronary heart disease in the Normative Aging Study. Arch Gen Psychiatry 2007; 64:109–116.
- Porges SW. The polyvagal perspective. Biol Psychol 2007; 74:116–143.
- Porges SW. The polyvagal theory: phylogenetic substrates of a social nervous system. Int J Psychophysiol 2001; 42:123–146.
- Penn MS, Bakken EE. Heart-brain medicine: update 2007. Cleve Clin J Med 2008; 75( suppl 2):S3–S4.
- Lichtman JH, Bigger JT, Blumenthal JA, et al. Depression and coronary heart disease: recommendations for screening, referral, and treatment: a science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care and Outcomes Research. Endorsed by the American Psychiatric Association. Circulation 2008; 118:1768–1775.
- Whang W, Kubzansky LD, Kawachi I, et al. Depression and risk of sudden cardiac death and coronary heart disease in women: results from the Nurses’ Health Study. J Am Coll Cardiol 2009; 53:950–958.
- Frazier L, Vaughn W, Willerson J, Ballantyne C, Boerwinkle E Inflammatory protein levels and depression screening after coronary stenting predict major adverse coronary events [published online ahead of print February 26, 2009]. Biol Res Nurs. doi:10.1177/1099800409332801.
- Kim JH, Kim JW, Ko YH, et al Coronary endothelial dysfunction associated with a depressive mood in patients with atypical angina but angiographically normal coronary artery [published online ahead of print March 7, 2009]. Int J Cardiol. doi:10.1016/j.ijcard.2009.02.004.
- Davidson KW, Schwartz JE, Kirkland SA, et al. Relation of inflammation to depression and incident coronary heart disease (from the Canadian Nova Scotia Health Survey [NSHS95] Prospective Population Study). Am J Cardiol 2009; 103:755–761.
- Bankier B, Barajas J, Martinez-Rumayor A, Januzzi JL. Association between major depressive disorder and C-reactive protein levels in stable coronary heart disease patients. J Psychosom Res 2009; 66:189–194.
- Carney RM, Freedland KE, Steinmeyer B, et al History of depression and survival after acute myocardial infarction [published online ahead of print February 27, 2009]. Psychosom Med. doi:10.1097/PSY.0b013e31819b69e3.
- Vasilyev N, Williams T, Brennan ML, et al. Myeloperoxidase-generated oxidants modulate left ventricular remodeling but not infarct size after myocardial infarction. Circulation 2005; 112:2812–2820.
- Sack M, Hopper JW, Lamprecht F. Low respiratory sinus arrhythmia and prolonged psychophysiological arousal in posttraumatic stress disorder: heart rate dynamics and individual differences in arousal regulation. Biol Psychiatry 2004; 55:284–290.
- Kubzansky LD, Koenen KC, Jones C, Eaton WW. A prospective study of posttraumatic stress disorder symptoms and coronary heart disease in women. Health Psychol 2009; 28:125–130.
- Kubzansky LD, Koenen KC, Spiro A, Vokonas PS, Sparrow D. Prospective study of posttraumatic stress disorder symptoms and coronary heart disease in the Normative Aging Study. Arch Gen Psychiatry 2007; 64:109–116.
- Porges SW. The polyvagal perspective. Biol Psychol 2007; 74:116–143.
- Porges SW. The polyvagal theory: phylogenetic substrates of a social nervous system. Int J Psychophysiol 2001; 42:123–146.