User login
CASE Postmenopausal dyspareunia
A 60-year-old widow who recently remarried complains of dyspareunia. Examination of the vulva reveals firm but thin white skin over the periclitoral area and labia minora and shrinking of the vulvar skin.
What is the likely diagnosis?
Lichen sclerosus is the probable diagnosis, given her age and the appearance of the vulva, although it is impossible to assure the diagnosis without a biopsy. The preferred treatment is clobetasol, an ultrapotent steroid, applied daily.
True, powerful steroids can cause atrophy if applied regularly to other areas of the skin, but clobetasol does not cause atrophy of vulvar skin. After several weeks of nightly application, the skin should be softer and more pliable, and dyspareunia should be resolved. The patient can then reduce the clobetasol application to twice weekly—but she must continue the treatment indefinitely.
The vulva over the lifespan
The vulva is sensitive to both physiologic and pathologic changes, as well as to the sex hormones that govern the menstrual cycle. The mucosa on the inner aspects of the labia minora is very similar to the skin of the vagina and thus very sensitive to estrogen. The skin of the labia majora and the outer surface of the labia minora is more consistent with hair-bearing skin in the perineal area and more sensitive to androgens, which help thicken the skin. At menopause, the loss of estrogen leads to atrophy, and the vulvar epithelium is reduced to a few layers of mostly intermediate and parabasal cell types. The labia minora and majora as well as the clitoris gradually become less prominent with age.
The skin of the vulva consists of both dermis and epidermis, which interact with each other and respond to different nutritional and hormonal influences. For example, estrogen has little effect on vulvar epidermis, but considerable effect on the dermis, thickening the skin and preventing atrophy.
Postmenopausal atrophic changes can become a clinical problem when a woman resumes sexual intercourse after a long period of abstinence, as in the opening case. If atrophy is the main complaint, estrogen replacement therapy will alleviate symptoms of tightness, irritation, and dyspareunia, but it may take 6 weeks to 6 months to achieve optimal results. In the interim, women need to be reassured that reasonable function can be achieved.
Hygienic considerations
With any vulvar irritation, the patient should discontinue the use of synthetic undergarments in favor of cotton panties, which permit more adequate circulation and do not trap moisture.
Sitz baths often help relieve local discomfort, but should be followed by thorough drying.
The new ACOG Committee Opinion reflects recommendations of the American Society for Colposcopy and Cervical Pathology.17
Vulvodynia. American College of Obstetricians and Gynecologists Committee Opinion No. 345. Obstet Gynecol. October 2006;108:1049–1052.
Vulvar dystrophies: Think “white”
In the past, these diseases have been defined as non-neoplastic epithelial disorders of the vulva. Although there have been many attempts to more accurately define vulvar dystrophies, none have completely described the wide variety of clinical presentations.
In general, dystrophies are disorders of epithelial growth and nutrition that often result in a white surface color change. This definition includes intraepithelial neoplasia and Paget’s disease of the vulva. The International Society for the Study of Vulvovaginal Disease has proposed multiple classifications since 1975. I prefer the clarity of the 1987 classification system.1 I also consider these terms out-of-date: lichen sclerosus et atrophicus, carcinoma simplex, leukoplakic vulvitis, leukoplakia, hyperplastic vulvitis, neurodermatitis, kraurosis vulvae, leukokeratosis, erythroplasia of Queyrat, and Bowen’s disease.
What makes the lesions white?
The white appearance of dystrophic lesions is due to excessive keratin, at times deep pigmentation, and relative avascularity. All 3 of these characteristics are present in the spectrum of vulvar dystrophies. Biopsy of the affected skin is the key to accurate diagnosis and successful therapy.
Lichen sclerosus
Does not raise risk of carcinoma
The most common of the 3 groups of white lesions described in the 1987 classification of dystrophies, lichen sclerosus usually occurs in postmenopausal women, but can appear at any age, including childhood (FIGURE 1). Despite claims to the contrary, there is no good evidence that women with lichen sclerosus face a higher risk for vulvar carcinoma.
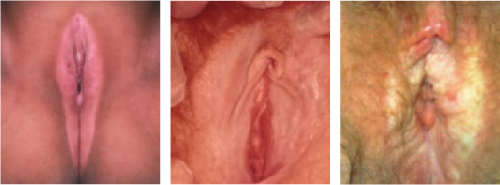
FIGURE 1
Lichen sclerosus affects all ages
3-year-old child. Note the inflammation secondary to excoriations.
20-year-old woman. The glans clitoris has begun the hooding process.
70-year-old woman. The introitus has shrunk, making intercourse impossible.
Signs and symptoms
In lichen sclerosus, the skin of the vulva appears very thin, atrophic, and dry, resembling parchment. It is also white, with loss of pigmentation.
Pruritus is the most common symptom and is usually the presenting symptom. Scratching during sleep may create ulcerations and areas of ecchymosis, and there is generalized shrinking of the vulvar skin, with eventual loss of the labia minora.
The edema and shrinking that occur around the clitoris cause a “hooding” of the glans clitoris. If the process continues unchecked, it can involve the labia majora as well as the skin of the inner thigh and anal region.
Prescribe clobetasol ointment
The patient should be instructed to use clobetasol 0.05% ointment on a continuing basis. This drug is so successful it has eclipsed the use of testosterone propionate for this indication. Lorenz and colleagues2 found very high success rates in 81 symptomatic patients with biopsy-proven disease who had failed previous therapy.
For reasons that are unknown, persistent use of this steroid on vulvar skin does not cause the atrophy commonly seen with prolonged use of high-potency steroids on other areas of the skin.
Start with twice-daily application and taper to less frequent use as the symptoms come under control. Most patients in remission can be maintained with twice-weekly application. Pruritus should disappear completely, and the skin itself will become less “leathery.”
Surgical treatment is not advised
Surgery does not appear to have a role because lichen sclerosus often recurs outside excised areas. Several reports have even described the return of disease in skin grafts used to replace large diseased areas.
I do not recommend surgery except in dire circumstances, when symptom relief is essential to the patient’s quality of life and all other therapies have failed.
Squamous cell hyperplasia
This disease is probably the same entity as lichen simplex chronicus. Changes in vulvar skin appear to result from chronic scratching secondary to intense pruritus. This complaint often involves a vicious cycle of scratching, increased pruritus, and more scratching, until excoriations occur. The aim of therapy is to eliminate the pruritus (FIGURE 2).

FIGURE 2
Squamous cell hyperplasia
75-year-old woman. The skin is thickened and may be leathery.
Intense pruritus and aggressive scratching lead to excoriations.
Signs and symptoms
Vulvar skin is typically white or pink. Biopsy will confirm the diagnosis, revealing a markedly thickened keratin layer (hyperkeratosis) and irregular thickening of the Malpighian ridges (acanthosis).
Inflammatory changes are also present, especially when there are areas of excoriation.
Treatment is similar to therapy for lichen sclerosus
Potent topical corticosteroids are the backbone of treatment; clobetasol is the preferred drug. The frequency of application is identical to that described for lichen sclerosus, and response to therapy usually takes 2 months. In the interim, it is advisable to prescribe other medications for the pruritus.
Lichen sclerosus and squamous cell hyperplasia sometimes coincide. Fortunately, the therapies are quite similar and both conditions tend to respond.
Vulvodynia
This disorder consists of chronic vulvar discomfort due to itching, burning, and/or pain that causes physical, sexual, and psychological distress.3,4 Once referred to as essential vulvodynia, it now is defined as generalized vulvar dysesthesia.
Signs and symptoms
Women with this condition tend to have difficulty localizing their pain. They often present with a complaint of recurrent yeast infection or constant irritation at the introitus. Dyspareunia may or may not be a presenting symptom, although intercourse often triggers this condition. Tight pants or rough undergarments also may trigger symptoms.
Common symptoms. In a study by Sadownik,5 women with vulvar dysesthesia reported the following symptoms:
Women with vulvar dysesthesia who appear to have urinary tract symptoms should undergo a urine culture, though it will often be negative and antibiotic therapy will have little effect.
A diagnosis of exclusion
The pain of dysesthesia appears to be neuropathic in origin in that it mimics pain of the sensory nervous system. It may be diffuse or focal, unilateral or bilateral, constant or sporadic. Thus, it is a diagnosis of exclusion.
Recommended therapies
Vulvar dysesthesia should be regarded as a chronic pain syndrome and treated accordingly, with emphasis on generalized improvements in health and attitude rather than single-therapy approaches.
Potent topical corticosteroids are usually of no benefit. Nor does topical estrogen produce long-term relief.
Once all possible causes of symptoms are excluded, refer the patient for education, support, and treatment of depression, if present. Occasionally, topical anesthetics will provide short-term relief.
At least 2 vulvar pain societies—the National Vulvodynia Association and the Vulvar Pain Foundation—have newsletters, outreach programs, and Web sites.
Vulvar vestibulitis
A more readily definable condition in the same category as vulvodynia is so-called vulvar vestibulitis, also known as localized vulvodynia (as classified by the new ACOG Committee Opinion on vulvodynia).
Signs and symptoms
The defining presentation is severe pain on vestibular touch (eg, entry at intercourse), with tenderness to pressure localized within the vulvar vestibule in a horseshoe distribution pattern encompassing 3, 6, and 9 o’clock on the vestibule. Erythema is often present, especially at the 5 and 7 o’clock positions (FIGURE 3).
Patients have no symptoms during normal daily activities, but complain of dyspareunia and an inability to use tampons.
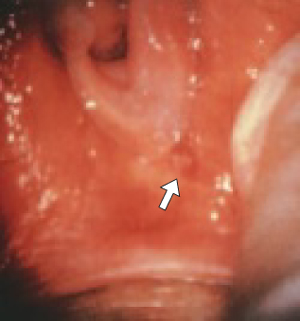
FIGURE 3
Vestibular adenitis
Intense erythema at the 5 o’clock position in the vestibule.
Diagnostic strategies
Vulvar vestibulitis can be diagnosed using a moistened cotton-tip applicator. Pressure applied in the area of the urethral meatus will result in minimal discomfort, but pressure in the horseshoe area of the vestibule will cause exquisite discomfort.
Careful inspection at 5 and 7 o’clock in the vestibule usually uncovers intense erythema over an area of 4 or 5 mm. To distinguish vestibulitis from dysesthesia, see the comparison in TABLE 1.
TABLE 1
Distinguishing vulvar vestibulitis and dysesthesia
| VULVAR VESTIBULITIS | ESSENTIAL VULVAR DYSESTHESIA |
|---|---|
| Pain is usually not constant | Pain is a constant burning sensation |
| Erythema in sensitive areas | No erythema or abnormal appearance |
| Lidocaine quells sensitivity | Lidocaine has no effect |
| Cause is dermal inflammation | Cause is allodynia (heightened nerve sensitivity) |
Recommended therapies
Treatment of vulvar vestibulitis is complex. It is important to see the patient often to ensure that this syndrome is truly present rather than vulvar dysesthesia. Xylocaine jelly should be given in an attempt to relieve symptoms; topical steroid ointments are another option.
Women with persistent symptoms are difficult to treat medically. Earlier theories pointing to infection as the cause of vestibulitis have been discounted.
Some experts believe that foods containing oxalates precipitate these symptoms. It may be advisable to have the patient reduce the content of oxalates in her diet in an effort to address all possible remedies.
For refractory cases, consider surgery
Consider surgical removal of the tender vestibule if all other therapies fail to provide adequate relief. Surgery for this indication has a high success rate (TABLE 2).7
Some surgeons have attempted treatment with laser ablation, but most have found excision more satisfactory, with faster recovery and excellent cosmesis.
Schneider and colleagues8 had 69 women complete a questionnaire 6 months after surgery, 54 (78%) of whom replied. Moderate to excellent improvement was reported by 45 women (83%); 7 had repeat surgery, after which 4 improved.
TABLE 2
Impressive track record for surgical treatment of vestibulitis
| % RESPONSE | |||
|---|---|---|---|
| STUDY | COMPLETE | PARTIAL | NONE |
| Bornstein et al7 | 76 | 24 | 0 |
| Bergeron et al12 | 63 | 37 | 0 |
| Kehoe and Luesley13 | 60 | 29 | 11 |
| Mann et al14 | 66 | 21 | 13 |
| Schover et al15 | 47 | 37 | 16 |
| Marinoff and Turner16 | 82 | 15 | 3 |
| Adapted from Bornstein et al7 | |||
Pigmented lesions
Are they cancer precursors?
Precursors of malignant melanoma of the vulva have yet to be clearly defined. The majority of these melanomas appear to arise de novo; however, some are associated with precursor nevi, especially junctional nevi. The 3 most common types of nevi that appear on the vulva are:
Assessing malignant potential
Only a small number of dysplastic nevi progress to malignant melanoma, but the frequency increases when the dysplastic nevus is familial and not acquired.
In general, the more severe the dysplasia, the greater the likelihood it will progress to malignancy. In dysplastic nevi, the pattern and appearance of the melanocytic cells are atypical. Bridging of melanocytic clusters of atypical cells may occur. Often, the atypical melanocytes are varied in size and shape, increasing in cell and nuclear size as severity increases. In the most severe cases, nucleoli are very prominent.
Many pigmented lesions of the vulva are lentigines, similar to freckles. Distinguishing one pigmented lesion from another is difficult even with magnification, and the clinician often must decide whether or not to biopsy. One set of guidelines recommends excisional biopsy of vulvar nevi when there is a change in:
Note that a reddish lesion may be basal cell hyperplasia, which has been associated with the development of basal cell carcinoma (FIGURE 4).

FIGURE 4
Basal cell carcinoma
An uncommon type of vulvar cancer, this tumor rarely metastasizes.
Premalignant lesions of squamous epithelium
The variable appearance of vulvar intraepithelial neoplasia (VIN) necessitates the liberal use of diagnostic biopsies, particularly when lesions persist or recur. VIN can present as a white lesion, or as pseudopigmented, pink, or raised and eroded.
Cigarette smoking is a risk factor.
Clinical appearance
Macroscopically, VIN lesions are often multiple and appear slightly raised and papular. Hyper- or pseudopigmented lesions are seen in about 30% of cases.
A confluence of VIN can create an appearance of diffuse plaques. In VIN, as for CIN, carcinoma in situ involves a full-thickness abnormality.
Terminology
If the abnormal parabasal layer extends to one half to two thirds of the epithelium, moderate dysplasia is present. A lower degree of involvement is called mild dysplasia, and full-thickness involvement is severe dysplasia or carcinoma in situ.
High rate of persistence, recurrence
Herod and colleagues9 reported on a 15-year follow-up of VIN and found that disease persisted or recurred in 48% of women managed surgically, and 7% of patients progressed to frankly invasive carcinoma. These investigators used the following classification system:
Joura et al10 strongly suggested that the incidence of this condition is increasing, especially in women prior to the 7th decade of life. Whether this increase is due to better recognition or a true rise in prevalence has been debated.
Diagnostic strategies
Application of 5% acetic acid to the vulvar skin will, after 3 to 5 minutes, allow areas of involvement to be readily seen with a handheld magnifying glass. Colposcopy can be used, but is slower and not as efficient as a simple magnifying lens. Most clinicians have abandoned the use of toluidine blue to identify multicentric lesions, since acetic acid appears to be less cumbersome and just as efficient.
White or pseudopigmented lesions (FIGURE 5) can be seen anywhere on the vulva and represent 2 of the 3 presentations of VIN. Pink lesions (FIGURE 5) are usually seen on moist surfaces near mucous membranes, whereas the white or pseudopigmented lesions are usually seen on the drier, hair-bearing areas of the vulva. Biopsy reveals similar histology.
The cause of the pseudopigmented lesions is unclear, but is unrelated to a disturbance of the melanin cells. As with other vulvar lesions, biopsy is essential for a correct diagnosis.

FIGURE 5
VIN III lesions: A trio of presentations
White lesion.
Pseudopigmented lesions.
Pink lesion.
Recommended therapies
VIN is treated by destroying or excising the epithelium involved. When the area is limited in size, simple excision or laser vaporization is preferred. A 2- to 3-mm margin is adequate, because these lesions have sharp borders.
Laser therapy warrants extra care because the epithelium is rarely thicker than 0.5 mm. For this reason, vaporization of the vulva should be limited to the following depths:
These limits will speed healing and prevent the unnecessary destruction of dermis.
Also be aware that the depth of hair-follicle involvement rarely exceeds 1 mm. Vaporization of the full thickness of the dermis will lead to alopecia and vulvar dryness.
When disease is multifocal or confluent, treatment is more challenging. Several decades ago, simple vulvectomy was performed, but the patient was left a sexual cripple.
Since then, laser therapy has been attempted in these cases, and has proved to be effective when the area treated does not exceed 25% of the total area of the vulva. Extensive laser therapy leads to considerable postoperative pain and an unhappy result.
Extensive involvement may necessitate laser treatment by quadrant to achieve the best results. Another option is “skinning vulvectomy” using a skin graft. This procedure, first described by Felix Rutledge,11 requires a 7- or 8-day hospitalization, but allows for complete therapy in 1 session.
Paget’s disease of the vulva
This disease is most frequently seen in the breast nipple (FIGURE 6), where it is usually associated with an underlying infiltrating ductal carcinoma. Extramammary sites include the vulvar, perianal, and axillary regions. The disease has also been seen in the ear canal.
Paget’s disease is an intraepithelial adenocarcinoma of eccrine or apocrine origin.

FIGURE 6
Paget disease: Not just a breast complaint
Paget disease of the nipple with underlying ductal adenocarcinoma.
Vulvar Paget disease: lesion (left) and photomicrograph of the lesion.
Clinical appearance
Paget’s disease of the vulva appears as a superficial, red to pink, velvety, eczematoid lesion (FIGURE 6), which is very pruritic and often associated with exfoliation. Margins are difficult to identify grossly.
On rare occasions, a nodular tumor can be found in the middle of the skin involvement, but in most cases no invasive malignancy is found at extramammary sites on the vulva.
Diagnostic strategies
Microscopic appearance of Paget cells (FIGURE 6) are pathognomonic of the disease.
Older textbooks suggest that 10% to 20% of patients have an associated, underlying, invasive carcinoma of a skin appendage, Bartholin’s gland, urinary tract, or bowel or rectal site, but later experience has not confirmed this. Rather, the likelihood of concomitant invasive disease is much lower than 10%.
Excision is the treatment of choice
Any attempt to achieve negative margins must utilize frozen section. Some studies have suggested that negative margins are not associated with a reduced rate of recurrence, but these findings have been inconsistent.
Recurrence is common
Paget’s disease of the vulva often recurs, especially when the initial lesion is large. Close monitoring will detect these recurrences when they’re quite small and easily removed via local excision. Occasionally, the initial disease is so extensive that skin grafting may be necessary to cover the defect.
The author reports no financial relationships relevant to this article.
1. Voet RL. Classification of vulvar dystrophies and premalignant squamous lesions. J Cutan Pathol. 1994;21:86-90.
2. Lorenz B, Kaufman RH, Kutzner SK. Lichen sclerosus. Therapy with clobetasol propionate. J Reprod Med. 1998;43:790-794.
3. Proceedings of the XVth World Congress. International Society for the Study of Vulvovaginal Disease, Santa Fe, NM; September 26-30, 1999. International Society for the Study of Vulvovaginal Disease Newsletter, Summer 2000.
4. Masheb RM, Nash JM, Brondolo E, Kerns RD. Vulvodynia: an introduction and critical review of a chronic pain condition. Pain. 2000;86-93.
5. Sadownik A. Clinical profile of vulvodynia patients. J Reprod Med. 2000;45:679-684.
6. Edwards A, Wojnarowska F. The vulvar pain syndromes. Int J STD AIDS. 1998;9:74-78.
7. Bornstein J, Zarfati D, Goldik Z, Abramovici H. Vulvar vestibulitis: physical or psychosexual problem? Obstet Gynecol. 1999;93(5 Pt 2):876-880.
8. Schneider D, Yaron M, Bukovsky I, Soffer Y, Halpern R. Outcome of surgical treatment for superficial dyspareunia from vulvar vestibulitis. J Reprod Med. 2001;46:227-231.
9. Herod JJ, Shafi MI, Rollason TP, Jordan JA, Luesley DM. Vulvar intraepithelial neoplasia: long-term follow-up of treated and untreated women. Br J Obstet Gynaecol. 1996;103:446-452.
10. Joura EA, Lösch A, Haider-Angeler M-G, Breitenecker G, Leodolter S. Trends in vulvar neoplasia. J Reprod Med. 2000;45:613-615.
11. Rutledge F, Sinclair M. Treatment of intraepithelial carcinoma of the vulva by skin excision and graft. Am J Obstet Gynecol. 1968;102:807-818.
12. Bergeron S, Bouchard C, Fortier M, Binik YM, Khalife S. The surgical treatment of vulvar vestibulitis syndrome: a follow-up study. J Sex Marital Ther. 1997;23:317-325.
13. Kehoe S, Luesley D. An evaluation of modified vestibulectomy in the treatment of vulvar vestibulitis: preliminary results. Acta Obstet Gynecol Scand. 1996;75:676-677.
14. Mann MS, Kaufman RH, Brown D, Jr, Adam E. Vulvar vestibulitis: significant clinical variables and treatment outcome. Obstet Gynecol. 1992;79:122-125.
15. Schover LR, Youngs DD, Cannata R. Psychosexual aspects of the evaluation and management of vulvar vestibulitis. Am J Obstet Gynecol. 1992;167:630-636.
16. Marinoff SC, Turner ML. Vulvar vestibulitis syndrome: an overview. Am J Obstet Gynecol. 1991;165:1228-1233.
17. Haefner HK, Collins ME, Davis GD, et al. The vulvodynia guideline. J Low Genit Tract Dis. 2005;9:45-51.
CASE Postmenopausal dyspareunia
A 60-year-old widow who recently remarried complains of dyspareunia. Examination of the vulva reveals firm but thin white skin over the periclitoral area and labia minora and shrinking of the vulvar skin.
What is the likely diagnosis?
Lichen sclerosus is the probable diagnosis, given her age and the appearance of the vulva, although it is impossible to assure the diagnosis without a biopsy. The preferred treatment is clobetasol, an ultrapotent steroid, applied daily.
True, powerful steroids can cause atrophy if applied regularly to other areas of the skin, but clobetasol does not cause atrophy of vulvar skin. After several weeks of nightly application, the skin should be softer and more pliable, and dyspareunia should be resolved. The patient can then reduce the clobetasol application to twice weekly—but she must continue the treatment indefinitely.
The vulva over the lifespan
The vulva is sensitive to both physiologic and pathologic changes, as well as to the sex hormones that govern the menstrual cycle. The mucosa on the inner aspects of the labia minora is very similar to the skin of the vagina and thus very sensitive to estrogen. The skin of the labia majora and the outer surface of the labia minora is more consistent with hair-bearing skin in the perineal area and more sensitive to androgens, which help thicken the skin. At menopause, the loss of estrogen leads to atrophy, and the vulvar epithelium is reduced to a few layers of mostly intermediate and parabasal cell types. The labia minora and majora as well as the clitoris gradually become less prominent with age.
The skin of the vulva consists of both dermis and epidermis, which interact with each other and respond to different nutritional and hormonal influences. For example, estrogen has little effect on vulvar epidermis, but considerable effect on the dermis, thickening the skin and preventing atrophy.
Postmenopausal atrophic changes can become a clinical problem when a woman resumes sexual intercourse after a long period of abstinence, as in the opening case. If atrophy is the main complaint, estrogen replacement therapy will alleviate symptoms of tightness, irritation, and dyspareunia, but it may take 6 weeks to 6 months to achieve optimal results. In the interim, women need to be reassured that reasonable function can be achieved.
Hygienic considerations
With any vulvar irritation, the patient should discontinue the use of synthetic undergarments in favor of cotton panties, which permit more adequate circulation and do not trap moisture.
Sitz baths often help relieve local discomfort, but should be followed by thorough drying.
The new ACOG Committee Opinion reflects recommendations of the American Society for Colposcopy and Cervical Pathology.17
Vulvodynia. American College of Obstetricians and Gynecologists Committee Opinion No. 345. Obstet Gynecol. October 2006;108:1049–1052.
Vulvar dystrophies: Think “white”
In the past, these diseases have been defined as non-neoplastic epithelial disorders of the vulva. Although there have been many attempts to more accurately define vulvar dystrophies, none have completely described the wide variety of clinical presentations.
In general, dystrophies are disorders of epithelial growth and nutrition that often result in a white surface color change. This definition includes intraepithelial neoplasia and Paget’s disease of the vulva. The International Society for the Study of Vulvovaginal Disease has proposed multiple classifications since 1975. I prefer the clarity of the 1987 classification system.1 I also consider these terms out-of-date: lichen sclerosus et atrophicus, carcinoma simplex, leukoplakic vulvitis, leukoplakia, hyperplastic vulvitis, neurodermatitis, kraurosis vulvae, leukokeratosis, erythroplasia of Queyrat, and Bowen’s disease.
What makes the lesions white?
The white appearance of dystrophic lesions is due to excessive keratin, at times deep pigmentation, and relative avascularity. All 3 of these characteristics are present in the spectrum of vulvar dystrophies. Biopsy of the affected skin is the key to accurate diagnosis and successful therapy.
Lichen sclerosus
Does not raise risk of carcinoma
The most common of the 3 groups of white lesions described in the 1987 classification of dystrophies, lichen sclerosus usually occurs in postmenopausal women, but can appear at any age, including childhood (FIGURE 1). Despite claims to the contrary, there is no good evidence that women with lichen sclerosus face a higher risk for vulvar carcinoma.
FIGURE 1
Lichen sclerosus affects all ages
3-year-old child. Note the inflammation secondary to excoriations.
20-year-old woman. The glans clitoris has begun the hooding process.
70-year-old woman. The introitus has shrunk, making intercourse impossible.
Signs and symptoms
In lichen sclerosus, the skin of the vulva appears very thin, atrophic, and dry, resembling parchment. It is also white, with loss of pigmentation.
Pruritus is the most common symptom and is usually the presenting symptom. Scratching during sleep may create ulcerations and areas of ecchymosis, and there is generalized shrinking of the vulvar skin, with eventual loss of the labia minora.
The edema and shrinking that occur around the clitoris cause a “hooding” of the glans clitoris. If the process continues unchecked, it can involve the labia majora as well as the skin of the inner thigh and anal region.
Prescribe clobetasol ointment
The patient should be instructed to use clobetasol 0.05% ointment on a continuing basis. This drug is so successful it has eclipsed the use of testosterone propionate for this indication. Lorenz and colleagues2 found very high success rates in 81 symptomatic patients with biopsy-proven disease who had failed previous therapy.
For reasons that are unknown, persistent use of this steroid on vulvar skin does not cause the atrophy commonly seen with prolonged use of high-potency steroids on other areas of the skin.
Start with twice-daily application and taper to less frequent use as the symptoms come under control. Most patients in remission can be maintained with twice-weekly application. Pruritus should disappear completely, and the skin itself will become less “leathery.”
Surgical treatment is not advised
Surgery does not appear to have a role because lichen sclerosus often recurs outside excised areas. Several reports have even described the return of disease in skin grafts used to replace large diseased areas.
I do not recommend surgery except in dire circumstances, when symptom relief is essential to the patient’s quality of life and all other therapies have failed.
Squamous cell hyperplasia
This disease is probably the same entity as lichen simplex chronicus. Changes in vulvar skin appear to result from chronic scratching secondary to intense pruritus. This complaint often involves a vicious cycle of scratching, increased pruritus, and more scratching, until excoriations occur. The aim of therapy is to eliminate the pruritus (FIGURE 2).
FIGURE 2
Squamous cell hyperplasia
75-year-old woman. The skin is thickened and may be leathery.
Intense pruritus and aggressive scratching lead to excoriations.
Signs and symptoms
Vulvar skin is typically white or pink. Biopsy will confirm the diagnosis, revealing a markedly thickened keratin layer (hyperkeratosis) and irregular thickening of the Malpighian ridges (acanthosis).
Inflammatory changes are also present, especially when there are areas of excoriation.
Treatment is similar to therapy for lichen sclerosus
Potent topical corticosteroids are the backbone of treatment; clobetasol is the preferred drug. The frequency of application is identical to that described for lichen sclerosus, and response to therapy usually takes 2 months. In the interim, it is advisable to prescribe other medications for the pruritus.
Lichen sclerosus and squamous cell hyperplasia sometimes coincide. Fortunately, the therapies are quite similar and both conditions tend to respond.
Vulvodynia
This disorder consists of chronic vulvar discomfort due to itching, burning, and/or pain that causes physical, sexual, and psychological distress.3,4 Once referred to as essential vulvodynia, it now is defined as generalized vulvar dysesthesia.
Signs and symptoms
Women with this condition tend to have difficulty localizing their pain. They often present with a complaint of recurrent yeast infection or constant irritation at the introitus. Dyspareunia may or may not be a presenting symptom, although intercourse often triggers this condition. Tight pants or rough undergarments also may trigger symptoms.
Common symptoms. In a study by Sadownik,5 women with vulvar dysesthesia reported the following symptoms:
Women with vulvar dysesthesia who appear to have urinary tract symptoms should undergo a urine culture, though it will often be negative and antibiotic therapy will have little effect.
A diagnosis of exclusion
The pain of dysesthesia appears to be neuropathic in origin in that it mimics pain of the sensory nervous system. It may be diffuse or focal, unilateral or bilateral, constant or sporadic. Thus, it is a diagnosis of exclusion.
Recommended therapies
Vulvar dysesthesia should be regarded as a chronic pain syndrome and treated accordingly, with emphasis on generalized improvements in health and attitude rather than single-therapy approaches.
Potent topical corticosteroids are usually of no benefit. Nor does topical estrogen produce long-term relief.
Once all possible causes of symptoms are excluded, refer the patient for education, support, and treatment of depression, if present. Occasionally, topical anesthetics will provide short-term relief.
At least 2 vulvar pain societies—the National Vulvodynia Association and the Vulvar Pain Foundation—have newsletters, outreach programs, and Web sites.
Vulvar vestibulitis
A more readily definable condition in the same category as vulvodynia is so-called vulvar vestibulitis, also known as localized vulvodynia (as classified by the new ACOG Committee Opinion on vulvodynia).
Signs and symptoms
The defining presentation is severe pain on vestibular touch (eg, entry at intercourse), with tenderness to pressure localized within the vulvar vestibule in a horseshoe distribution pattern encompassing 3, 6, and 9 o’clock on the vestibule. Erythema is often present, especially at the 5 and 7 o’clock positions (FIGURE 3).
Patients have no symptoms during normal daily activities, but complain of dyspareunia and an inability to use tampons.
FIGURE 3
Vestibular adenitis
Intense erythema at the 5 o’clock position in the vestibule.
Diagnostic strategies
Vulvar vestibulitis can be diagnosed using a moistened cotton-tip applicator. Pressure applied in the area of the urethral meatus will result in minimal discomfort, but pressure in the horseshoe area of the vestibule will cause exquisite discomfort.
Careful inspection at 5 and 7 o’clock in the vestibule usually uncovers intense erythema over an area of 4 or 5 mm. To distinguish vestibulitis from dysesthesia, see the comparison in TABLE 1.
TABLE 1
Distinguishing vulvar vestibulitis and dysesthesia
| VULVAR VESTIBULITIS | ESSENTIAL VULVAR DYSESTHESIA |
|---|---|
| Pain is usually not constant | Pain is a constant burning sensation |
| Erythema in sensitive areas | No erythema or abnormal appearance |
| Lidocaine quells sensitivity | Lidocaine has no effect |
| Cause is dermal inflammation | Cause is allodynia (heightened nerve sensitivity) |
Recommended therapies
Treatment of vulvar vestibulitis is complex. It is important to see the patient often to ensure that this syndrome is truly present rather than vulvar dysesthesia. Xylocaine jelly should be given in an attempt to relieve symptoms; topical steroid ointments are another option.
Women with persistent symptoms are difficult to treat medically. Earlier theories pointing to infection as the cause of vestibulitis have been discounted.
Some experts believe that foods containing oxalates precipitate these symptoms. It may be advisable to have the patient reduce the content of oxalates in her diet in an effort to address all possible remedies.
For refractory cases, consider surgery
Consider surgical removal of the tender vestibule if all other therapies fail to provide adequate relief. Surgery for this indication has a high success rate (TABLE 2).7
Some surgeons have attempted treatment with laser ablation, but most have found excision more satisfactory, with faster recovery and excellent cosmesis.
Schneider and colleagues8 had 69 women complete a questionnaire 6 months after surgery, 54 (78%) of whom replied. Moderate to excellent improvement was reported by 45 women (83%); 7 had repeat surgery, after which 4 improved.
TABLE 2
Impressive track record for surgical treatment of vestibulitis
| % RESPONSE | |||
|---|---|---|---|
| STUDY | COMPLETE | PARTIAL | NONE |
| Bornstein et al7 | 76 | 24 | 0 |
| Bergeron et al12 | 63 | 37 | 0 |
| Kehoe and Luesley13 | 60 | 29 | 11 |
| Mann et al14 | 66 | 21 | 13 |
| Schover et al15 | 47 | 37 | 16 |
| Marinoff and Turner16 | 82 | 15 | 3 |
| Adapted from Bornstein et al7 | |||
Pigmented lesions
Are they cancer precursors?
Precursors of malignant melanoma of the vulva have yet to be clearly defined. The majority of these melanomas appear to arise de novo; however, some are associated with precursor nevi, especially junctional nevi. The 3 most common types of nevi that appear on the vulva are:
Assessing malignant potential
Only a small number of dysplastic nevi progress to malignant melanoma, but the frequency increases when the dysplastic nevus is familial and not acquired.
In general, the more severe the dysplasia, the greater the likelihood it will progress to malignancy. In dysplastic nevi, the pattern and appearance of the melanocytic cells are atypical. Bridging of melanocytic clusters of atypical cells may occur. Often, the atypical melanocytes are varied in size and shape, increasing in cell and nuclear size as severity increases. In the most severe cases, nucleoli are very prominent.
Many pigmented lesions of the vulva are lentigines, similar to freckles. Distinguishing one pigmented lesion from another is difficult even with magnification, and the clinician often must decide whether or not to biopsy. One set of guidelines recommends excisional biopsy of vulvar nevi when there is a change in:
Note that a reddish lesion may be basal cell hyperplasia, which has been associated with the development of basal cell carcinoma (FIGURE 4).
FIGURE 4
Basal cell carcinoma
An uncommon type of vulvar cancer, this tumor rarely metastasizes.
Premalignant lesions of squamous epithelium
The variable appearance of vulvar intraepithelial neoplasia (VIN) necessitates the liberal use of diagnostic biopsies, particularly when lesions persist or recur. VIN can present as a white lesion, or as pseudopigmented, pink, or raised and eroded.
Cigarette smoking is a risk factor.
Clinical appearance
Macroscopically, VIN lesions are often multiple and appear slightly raised and papular. Hyper- or pseudopigmented lesions are seen in about 30% of cases.
A confluence of VIN can create an appearance of diffuse plaques. In VIN, as for CIN, carcinoma in situ involves a full-thickness abnormality.
Terminology
If the abnormal parabasal layer extends to one half to two thirds of the epithelium, moderate dysplasia is present. A lower degree of involvement is called mild dysplasia, and full-thickness involvement is severe dysplasia or carcinoma in situ.
High rate of persistence, recurrence
Herod and colleagues9 reported on a 15-year follow-up of VIN and found that disease persisted or recurred in 48% of women managed surgically, and 7% of patients progressed to frankly invasive carcinoma. These investigators used the following classification system:
Joura et al10 strongly suggested that the incidence of this condition is increasing, especially in women prior to the 7th decade of life. Whether this increase is due to better recognition or a true rise in prevalence has been debated.
Diagnostic strategies
Application of 5% acetic acid to the vulvar skin will, after 3 to 5 minutes, allow areas of involvement to be readily seen with a handheld magnifying glass. Colposcopy can be used, but is slower and not as efficient as a simple magnifying lens. Most clinicians have abandoned the use of toluidine blue to identify multicentric lesions, since acetic acid appears to be less cumbersome and just as efficient.
White or pseudopigmented lesions (FIGURE 5) can be seen anywhere on the vulva and represent 2 of the 3 presentations of VIN. Pink lesions (FIGURE 5) are usually seen on moist surfaces near mucous membranes, whereas the white or pseudopigmented lesions are usually seen on the drier, hair-bearing areas of the vulva. Biopsy reveals similar histology.
The cause of the pseudopigmented lesions is unclear, but is unrelated to a disturbance of the melanin cells. As with other vulvar lesions, biopsy is essential for a correct diagnosis.
FIGURE 5
VIN III lesions: A trio of presentations
White lesion.
Pseudopigmented lesions.
Pink lesion.
Recommended therapies
VIN is treated by destroying or excising the epithelium involved. When the area is limited in size, simple excision or laser vaporization is preferred. A 2- to 3-mm margin is adequate, because these lesions have sharp borders.
Laser therapy warrants extra care because the epithelium is rarely thicker than 0.5 mm. For this reason, vaporization of the vulva should be limited to the following depths:
These limits will speed healing and prevent the unnecessary destruction of dermis.
Also be aware that the depth of hair-follicle involvement rarely exceeds 1 mm. Vaporization of the full thickness of the dermis will lead to alopecia and vulvar dryness.
When disease is multifocal or confluent, treatment is more challenging. Several decades ago, simple vulvectomy was performed, but the patient was left a sexual cripple.
Since then, laser therapy has been attempted in these cases, and has proved to be effective when the area treated does not exceed 25% of the total area of the vulva. Extensive laser therapy leads to considerable postoperative pain and an unhappy result.
Extensive involvement may necessitate laser treatment by quadrant to achieve the best results. Another option is “skinning vulvectomy” using a skin graft. This procedure, first described by Felix Rutledge,11 requires a 7- or 8-day hospitalization, but allows for complete therapy in 1 session.
Paget’s disease of the vulva
This disease is most frequently seen in the breast nipple (FIGURE 6), where it is usually associated with an underlying infiltrating ductal carcinoma. Extramammary sites include the vulvar, perianal, and axillary regions. The disease has also been seen in the ear canal.
Paget’s disease is an intraepithelial adenocarcinoma of eccrine or apocrine origin.
FIGURE 6
Paget disease: Not just a breast complaint
Paget disease of the nipple with underlying ductal adenocarcinoma.
Vulvar Paget disease: lesion (left) and photomicrograph of the lesion.
Clinical appearance
Paget’s disease of the vulva appears as a superficial, red to pink, velvety, eczematoid lesion (FIGURE 6), which is very pruritic and often associated with exfoliation. Margins are difficult to identify grossly.
On rare occasions, a nodular tumor can be found in the middle of the skin involvement, but in most cases no invasive malignancy is found at extramammary sites on the vulva.
Diagnostic strategies
Microscopic appearance of Paget cells (FIGURE 6) are pathognomonic of the disease.
Older textbooks suggest that 10% to 20% of patients have an associated, underlying, invasive carcinoma of a skin appendage, Bartholin’s gland, urinary tract, or bowel or rectal site, but later experience has not confirmed this. Rather, the likelihood of concomitant invasive disease is much lower than 10%.
Excision is the treatment of choice
Any attempt to achieve negative margins must utilize frozen section. Some studies have suggested that negative margins are not associated with a reduced rate of recurrence, but these findings have been inconsistent.
Recurrence is common
Paget’s disease of the vulva often recurs, especially when the initial lesion is large. Close monitoring will detect these recurrences when they’re quite small and easily removed via local excision. Occasionally, the initial disease is so extensive that skin grafting may be necessary to cover the defect.
The author reports no financial relationships relevant to this article.
CASE Postmenopausal dyspareunia
A 60-year-old widow who recently remarried complains of dyspareunia. Examination of the vulva reveals firm but thin white skin over the periclitoral area and labia minora and shrinking of the vulvar skin.
What is the likely diagnosis?
Lichen sclerosus is the probable diagnosis, given her age and the appearance of the vulva, although it is impossible to assure the diagnosis without a biopsy. The preferred treatment is clobetasol, an ultrapotent steroid, applied daily.
True, powerful steroids can cause atrophy if applied regularly to other areas of the skin, but clobetasol does not cause atrophy of vulvar skin. After several weeks of nightly application, the skin should be softer and more pliable, and dyspareunia should be resolved. The patient can then reduce the clobetasol application to twice weekly—but she must continue the treatment indefinitely.
The vulva over the lifespan
The vulva is sensitive to both physiologic and pathologic changes, as well as to the sex hormones that govern the menstrual cycle. The mucosa on the inner aspects of the labia minora is very similar to the skin of the vagina and thus very sensitive to estrogen. The skin of the labia majora and the outer surface of the labia minora is more consistent with hair-bearing skin in the perineal area and more sensitive to androgens, which help thicken the skin. At menopause, the loss of estrogen leads to atrophy, and the vulvar epithelium is reduced to a few layers of mostly intermediate and parabasal cell types. The labia minora and majora as well as the clitoris gradually become less prominent with age.
The skin of the vulva consists of both dermis and epidermis, which interact with each other and respond to different nutritional and hormonal influences. For example, estrogen has little effect on vulvar epidermis, but considerable effect on the dermis, thickening the skin and preventing atrophy.
Postmenopausal atrophic changes can become a clinical problem when a woman resumes sexual intercourse after a long period of abstinence, as in the opening case. If atrophy is the main complaint, estrogen replacement therapy will alleviate symptoms of tightness, irritation, and dyspareunia, but it may take 6 weeks to 6 months to achieve optimal results. In the interim, women need to be reassured that reasonable function can be achieved.
Hygienic considerations
With any vulvar irritation, the patient should discontinue the use of synthetic undergarments in favor of cotton panties, which permit more adequate circulation and do not trap moisture.
Sitz baths often help relieve local discomfort, but should be followed by thorough drying.
The new ACOG Committee Opinion reflects recommendations of the American Society for Colposcopy and Cervical Pathology.17
Vulvodynia. American College of Obstetricians and Gynecologists Committee Opinion No. 345. Obstet Gynecol. October 2006;108:1049–1052.
Vulvar dystrophies: Think “white”
In the past, these diseases have been defined as non-neoplastic epithelial disorders of the vulva. Although there have been many attempts to more accurately define vulvar dystrophies, none have completely described the wide variety of clinical presentations.
In general, dystrophies are disorders of epithelial growth and nutrition that often result in a white surface color change. This definition includes intraepithelial neoplasia and Paget’s disease of the vulva. The International Society for the Study of Vulvovaginal Disease has proposed multiple classifications since 1975. I prefer the clarity of the 1987 classification system.1 I also consider these terms out-of-date: lichen sclerosus et atrophicus, carcinoma simplex, leukoplakic vulvitis, leukoplakia, hyperplastic vulvitis, neurodermatitis, kraurosis vulvae, leukokeratosis, erythroplasia of Queyrat, and Bowen’s disease.
What makes the lesions white?
The white appearance of dystrophic lesions is due to excessive keratin, at times deep pigmentation, and relative avascularity. All 3 of these characteristics are present in the spectrum of vulvar dystrophies. Biopsy of the affected skin is the key to accurate diagnosis and successful therapy.
Lichen sclerosus
Does not raise risk of carcinoma
The most common of the 3 groups of white lesions described in the 1987 classification of dystrophies, lichen sclerosus usually occurs in postmenopausal women, but can appear at any age, including childhood (FIGURE 1). Despite claims to the contrary, there is no good evidence that women with lichen sclerosus face a higher risk for vulvar carcinoma.
FIGURE 1
Lichen sclerosus affects all ages
3-year-old child. Note the inflammation secondary to excoriations.
20-year-old woman. The glans clitoris has begun the hooding process.
70-year-old woman. The introitus has shrunk, making intercourse impossible.
Signs and symptoms
In lichen sclerosus, the skin of the vulva appears very thin, atrophic, and dry, resembling parchment. It is also white, with loss of pigmentation.
Pruritus is the most common symptom and is usually the presenting symptom. Scratching during sleep may create ulcerations and areas of ecchymosis, and there is generalized shrinking of the vulvar skin, with eventual loss of the labia minora.
The edema and shrinking that occur around the clitoris cause a “hooding” of the glans clitoris. If the process continues unchecked, it can involve the labia majora as well as the skin of the inner thigh and anal region.
Prescribe clobetasol ointment
The patient should be instructed to use clobetasol 0.05% ointment on a continuing basis. This drug is so successful it has eclipsed the use of testosterone propionate for this indication. Lorenz and colleagues2 found very high success rates in 81 symptomatic patients with biopsy-proven disease who had failed previous therapy.
For reasons that are unknown, persistent use of this steroid on vulvar skin does not cause the atrophy commonly seen with prolonged use of high-potency steroids on other areas of the skin.
Start with twice-daily application and taper to less frequent use as the symptoms come under control. Most patients in remission can be maintained with twice-weekly application. Pruritus should disappear completely, and the skin itself will become less “leathery.”
Surgical treatment is not advised
Surgery does not appear to have a role because lichen sclerosus often recurs outside excised areas. Several reports have even described the return of disease in skin grafts used to replace large diseased areas.
I do not recommend surgery except in dire circumstances, when symptom relief is essential to the patient’s quality of life and all other therapies have failed.
Squamous cell hyperplasia
This disease is probably the same entity as lichen simplex chronicus. Changes in vulvar skin appear to result from chronic scratching secondary to intense pruritus. This complaint often involves a vicious cycle of scratching, increased pruritus, and more scratching, until excoriations occur. The aim of therapy is to eliminate the pruritus (FIGURE 2).
FIGURE 2
Squamous cell hyperplasia
75-year-old woman. The skin is thickened and may be leathery.
Intense pruritus and aggressive scratching lead to excoriations.
Signs and symptoms
Vulvar skin is typically white or pink. Biopsy will confirm the diagnosis, revealing a markedly thickened keratin layer (hyperkeratosis) and irregular thickening of the Malpighian ridges (acanthosis).
Inflammatory changes are also present, especially when there are areas of excoriation.
Treatment is similar to therapy for lichen sclerosus
Potent topical corticosteroids are the backbone of treatment; clobetasol is the preferred drug. The frequency of application is identical to that described for lichen sclerosus, and response to therapy usually takes 2 months. In the interim, it is advisable to prescribe other medications for the pruritus.
Lichen sclerosus and squamous cell hyperplasia sometimes coincide. Fortunately, the therapies are quite similar and both conditions tend to respond.
Vulvodynia
This disorder consists of chronic vulvar discomfort due to itching, burning, and/or pain that causes physical, sexual, and psychological distress.3,4 Once referred to as essential vulvodynia, it now is defined as generalized vulvar dysesthesia.
Signs and symptoms
Women with this condition tend to have difficulty localizing their pain. They often present with a complaint of recurrent yeast infection or constant irritation at the introitus. Dyspareunia may or may not be a presenting symptom, although intercourse often triggers this condition. Tight pants or rough undergarments also may trigger symptoms.
Common symptoms. In a study by Sadownik,5 women with vulvar dysesthesia reported the following symptoms:
Women with vulvar dysesthesia who appear to have urinary tract symptoms should undergo a urine culture, though it will often be negative and antibiotic therapy will have little effect.
A diagnosis of exclusion
The pain of dysesthesia appears to be neuropathic in origin in that it mimics pain of the sensory nervous system. It may be diffuse or focal, unilateral or bilateral, constant or sporadic. Thus, it is a diagnosis of exclusion.
Recommended therapies
Vulvar dysesthesia should be regarded as a chronic pain syndrome and treated accordingly, with emphasis on generalized improvements in health and attitude rather than single-therapy approaches.
Potent topical corticosteroids are usually of no benefit. Nor does topical estrogen produce long-term relief.
Once all possible causes of symptoms are excluded, refer the patient for education, support, and treatment of depression, if present. Occasionally, topical anesthetics will provide short-term relief.
At least 2 vulvar pain societies—the National Vulvodynia Association and the Vulvar Pain Foundation—have newsletters, outreach programs, and Web sites.
Vulvar vestibulitis
A more readily definable condition in the same category as vulvodynia is so-called vulvar vestibulitis, also known as localized vulvodynia (as classified by the new ACOG Committee Opinion on vulvodynia).
Signs and symptoms
The defining presentation is severe pain on vestibular touch (eg, entry at intercourse), with tenderness to pressure localized within the vulvar vestibule in a horseshoe distribution pattern encompassing 3, 6, and 9 o’clock on the vestibule. Erythema is often present, especially at the 5 and 7 o’clock positions (FIGURE 3).
Patients have no symptoms during normal daily activities, but complain of dyspareunia and an inability to use tampons.
FIGURE 3
Vestibular adenitis
Intense erythema at the 5 o’clock position in the vestibule.
Diagnostic strategies
Vulvar vestibulitis can be diagnosed using a moistened cotton-tip applicator. Pressure applied in the area of the urethral meatus will result in minimal discomfort, but pressure in the horseshoe area of the vestibule will cause exquisite discomfort.
Careful inspection at 5 and 7 o’clock in the vestibule usually uncovers intense erythema over an area of 4 or 5 mm. To distinguish vestibulitis from dysesthesia, see the comparison in TABLE 1.
TABLE 1
Distinguishing vulvar vestibulitis and dysesthesia
| VULVAR VESTIBULITIS | ESSENTIAL VULVAR DYSESTHESIA |
|---|---|
| Pain is usually not constant | Pain is a constant burning sensation |
| Erythema in sensitive areas | No erythema or abnormal appearance |
| Lidocaine quells sensitivity | Lidocaine has no effect |
| Cause is dermal inflammation | Cause is allodynia (heightened nerve sensitivity) |
Recommended therapies
Treatment of vulvar vestibulitis is complex. It is important to see the patient often to ensure that this syndrome is truly present rather than vulvar dysesthesia. Xylocaine jelly should be given in an attempt to relieve symptoms; topical steroid ointments are another option.
Women with persistent symptoms are difficult to treat medically. Earlier theories pointing to infection as the cause of vestibulitis have been discounted.
Some experts believe that foods containing oxalates precipitate these symptoms. It may be advisable to have the patient reduce the content of oxalates in her diet in an effort to address all possible remedies.
For refractory cases, consider surgery
Consider surgical removal of the tender vestibule if all other therapies fail to provide adequate relief. Surgery for this indication has a high success rate (TABLE 2).7
Some surgeons have attempted treatment with laser ablation, but most have found excision more satisfactory, with faster recovery and excellent cosmesis.
Schneider and colleagues8 had 69 women complete a questionnaire 6 months after surgery, 54 (78%) of whom replied. Moderate to excellent improvement was reported by 45 women (83%); 7 had repeat surgery, after which 4 improved.
TABLE 2
Impressive track record for surgical treatment of vestibulitis
| % RESPONSE | |||
|---|---|---|---|
| STUDY | COMPLETE | PARTIAL | NONE |
| Bornstein et al7 | 76 | 24 | 0 |
| Bergeron et al12 | 63 | 37 | 0 |
| Kehoe and Luesley13 | 60 | 29 | 11 |
| Mann et al14 | 66 | 21 | 13 |
| Schover et al15 | 47 | 37 | 16 |
| Marinoff and Turner16 | 82 | 15 | 3 |
| Adapted from Bornstein et al7 | |||
Pigmented lesions
Are they cancer precursors?
Precursors of malignant melanoma of the vulva have yet to be clearly defined. The majority of these melanomas appear to arise de novo; however, some are associated with precursor nevi, especially junctional nevi. The 3 most common types of nevi that appear on the vulva are:
Assessing malignant potential
Only a small number of dysplastic nevi progress to malignant melanoma, but the frequency increases when the dysplastic nevus is familial and not acquired.
In general, the more severe the dysplasia, the greater the likelihood it will progress to malignancy. In dysplastic nevi, the pattern and appearance of the melanocytic cells are atypical. Bridging of melanocytic clusters of atypical cells may occur. Often, the atypical melanocytes are varied in size and shape, increasing in cell and nuclear size as severity increases. In the most severe cases, nucleoli are very prominent.
Many pigmented lesions of the vulva are lentigines, similar to freckles. Distinguishing one pigmented lesion from another is difficult even with magnification, and the clinician often must decide whether or not to biopsy. One set of guidelines recommends excisional biopsy of vulvar nevi when there is a change in:
Note that a reddish lesion may be basal cell hyperplasia, which has been associated with the development of basal cell carcinoma (FIGURE 4).
FIGURE 4
Basal cell carcinoma
An uncommon type of vulvar cancer, this tumor rarely metastasizes.
Premalignant lesions of squamous epithelium
The variable appearance of vulvar intraepithelial neoplasia (VIN) necessitates the liberal use of diagnostic biopsies, particularly when lesions persist or recur. VIN can present as a white lesion, or as pseudopigmented, pink, or raised and eroded.
Cigarette smoking is a risk factor.
Clinical appearance
Macroscopically, VIN lesions are often multiple and appear slightly raised and papular. Hyper- or pseudopigmented lesions are seen in about 30% of cases.
A confluence of VIN can create an appearance of diffuse plaques. In VIN, as for CIN, carcinoma in situ involves a full-thickness abnormality.
Terminology
If the abnormal parabasal layer extends to one half to two thirds of the epithelium, moderate dysplasia is present. A lower degree of involvement is called mild dysplasia, and full-thickness involvement is severe dysplasia or carcinoma in situ.
High rate of persistence, recurrence
Herod and colleagues9 reported on a 15-year follow-up of VIN and found that disease persisted or recurred in 48% of women managed surgically, and 7% of patients progressed to frankly invasive carcinoma. These investigators used the following classification system:
Joura et al10 strongly suggested that the incidence of this condition is increasing, especially in women prior to the 7th decade of life. Whether this increase is due to better recognition or a true rise in prevalence has been debated.
Diagnostic strategies
Application of 5% acetic acid to the vulvar skin will, after 3 to 5 minutes, allow areas of involvement to be readily seen with a handheld magnifying glass. Colposcopy can be used, but is slower and not as efficient as a simple magnifying lens. Most clinicians have abandoned the use of toluidine blue to identify multicentric lesions, since acetic acid appears to be less cumbersome and just as efficient.
White or pseudopigmented lesions (FIGURE 5) can be seen anywhere on the vulva and represent 2 of the 3 presentations of VIN. Pink lesions (FIGURE 5) are usually seen on moist surfaces near mucous membranes, whereas the white or pseudopigmented lesions are usually seen on the drier, hair-bearing areas of the vulva. Biopsy reveals similar histology.
The cause of the pseudopigmented lesions is unclear, but is unrelated to a disturbance of the melanin cells. As with other vulvar lesions, biopsy is essential for a correct diagnosis.
FIGURE 5
VIN III lesions: A trio of presentations
White lesion.
Pseudopigmented lesions.
Pink lesion.
Recommended therapies
VIN is treated by destroying or excising the epithelium involved. When the area is limited in size, simple excision or laser vaporization is preferred. A 2- to 3-mm margin is adequate, because these lesions have sharp borders.
Laser therapy warrants extra care because the epithelium is rarely thicker than 0.5 mm. For this reason, vaporization of the vulva should be limited to the following depths:
These limits will speed healing and prevent the unnecessary destruction of dermis.
Also be aware that the depth of hair-follicle involvement rarely exceeds 1 mm. Vaporization of the full thickness of the dermis will lead to alopecia and vulvar dryness.
When disease is multifocal or confluent, treatment is more challenging. Several decades ago, simple vulvectomy was performed, but the patient was left a sexual cripple.
Since then, laser therapy has been attempted in these cases, and has proved to be effective when the area treated does not exceed 25% of the total area of the vulva. Extensive laser therapy leads to considerable postoperative pain and an unhappy result.
Extensive involvement may necessitate laser treatment by quadrant to achieve the best results. Another option is “skinning vulvectomy” using a skin graft. This procedure, first described by Felix Rutledge,11 requires a 7- or 8-day hospitalization, but allows for complete therapy in 1 session.
Paget’s disease of the vulva
This disease is most frequently seen in the breast nipple (FIGURE 6), where it is usually associated with an underlying infiltrating ductal carcinoma. Extramammary sites include the vulvar, perianal, and axillary regions. The disease has also been seen in the ear canal.
Paget’s disease is an intraepithelial adenocarcinoma of eccrine or apocrine origin.
FIGURE 6
Paget disease: Not just a breast complaint
Paget disease of the nipple with underlying ductal adenocarcinoma.
Vulvar Paget disease: lesion (left) and photomicrograph of the lesion.
Clinical appearance
Paget’s disease of the vulva appears as a superficial, red to pink, velvety, eczematoid lesion (FIGURE 6), which is very pruritic and often associated with exfoliation. Margins are difficult to identify grossly.
On rare occasions, a nodular tumor can be found in the middle of the skin involvement, but in most cases no invasive malignancy is found at extramammary sites on the vulva.
Diagnostic strategies
Microscopic appearance of Paget cells (FIGURE 6) are pathognomonic of the disease.
Older textbooks suggest that 10% to 20% of patients have an associated, underlying, invasive carcinoma of a skin appendage, Bartholin’s gland, urinary tract, or bowel or rectal site, but later experience has not confirmed this. Rather, the likelihood of concomitant invasive disease is much lower than 10%.
Excision is the treatment of choice
Any attempt to achieve negative margins must utilize frozen section. Some studies have suggested that negative margins are not associated with a reduced rate of recurrence, but these findings have been inconsistent.
Recurrence is common
Paget’s disease of the vulva often recurs, especially when the initial lesion is large. Close monitoring will detect these recurrences when they’re quite small and easily removed via local excision. Occasionally, the initial disease is so extensive that skin grafting may be necessary to cover the defect.
The author reports no financial relationships relevant to this article.
1. Voet RL. Classification of vulvar dystrophies and premalignant squamous lesions. J Cutan Pathol. 1994;21:86-90.
2. Lorenz B, Kaufman RH, Kutzner SK. Lichen sclerosus. Therapy with clobetasol propionate. J Reprod Med. 1998;43:790-794.
3. Proceedings of the XVth World Congress. International Society for the Study of Vulvovaginal Disease, Santa Fe, NM; September 26-30, 1999. International Society for the Study of Vulvovaginal Disease Newsletter, Summer 2000.
4. Masheb RM, Nash JM, Brondolo E, Kerns RD. Vulvodynia: an introduction and critical review of a chronic pain condition. Pain. 2000;86-93.
5. Sadownik A. Clinical profile of vulvodynia patients. J Reprod Med. 2000;45:679-684.
6. Edwards A, Wojnarowska F. The vulvar pain syndromes. Int J STD AIDS. 1998;9:74-78.
7. Bornstein J, Zarfati D, Goldik Z, Abramovici H. Vulvar vestibulitis: physical or psychosexual problem? Obstet Gynecol. 1999;93(5 Pt 2):876-880.
8. Schneider D, Yaron M, Bukovsky I, Soffer Y, Halpern R. Outcome of surgical treatment for superficial dyspareunia from vulvar vestibulitis. J Reprod Med. 2001;46:227-231.
9. Herod JJ, Shafi MI, Rollason TP, Jordan JA, Luesley DM. Vulvar intraepithelial neoplasia: long-term follow-up of treated and untreated women. Br J Obstet Gynaecol. 1996;103:446-452.
10. Joura EA, Lösch A, Haider-Angeler M-G, Breitenecker G, Leodolter S. Trends in vulvar neoplasia. J Reprod Med. 2000;45:613-615.
11. Rutledge F, Sinclair M. Treatment of intraepithelial carcinoma of the vulva by skin excision and graft. Am J Obstet Gynecol. 1968;102:807-818.
12. Bergeron S, Bouchard C, Fortier M, Binik YM, Khalife S. The surgical treatment of vulvar vestibulitis syndrome: a follow-up study. J Sex Marital Ther. 1997;23:317-325.
13. Kehoe S, Luesley D. An evaluation of modified vestibulectomy in the treatment of vulvar vestibulitis: preliminary results. Acta Obstet Gynecol Scand. 1996;75:676-677.
14. Mann MS, Kaufman RH, Brown D, Jr, Adam E. Vulvar vestibulitis: significant clinical variables and treatment outcome. Obstet Gynecol. 1992;79:122-125.
15. Schover LR, Youngs DD, Cannata R. Psychosexual aspects of the evaluation and management of vulvar vestibulitis. Am J Obstet Gynecol. 1992;167:630-636.
16. Marinoff SC, Turner ML. Vulvar vestibulitis syndrome: an overview. Am J Obstet Gynecol. 1991;165:1228-1233.
17. Haefner HK, Collins ME, Davis GD, et al. The vulvodynia guideline. J Low Genit Tract Dis. 2005;9:45-51.
1. Voet RL. Classification of vulvar dystrophies and premalignant squamous lesions. J Cutan Pathol. 1994;21:86-90.
2. Lorenz B, Kaufman RH, Kutzner SK. Lichen sclerosus. Therapy with clobetasol propionate. J Reprod Med. 1998;43:790-794.
3. Proceedings of the XVth World Congress. International Society for the Study of Vulvovaginal Disease, Santa Fe, NM; September 26-30, 1999. International Society for the Study of Vulvovaginal Disease Newsletter, Summer 2000.
4. Masheb RM, Nash JM, Brondolo E, Kerns RD. Vulvodynia: an introduction and critical review of a chronic pain condition. Pain. 2000;86-93.
5. Sadownik A. Clinical profile of vulvodynia patients. J Reprod Med. 2000;45:679-684.
6. Edwards A, Wojnarowska F. The vulvar pain syndromes. Int J STD AIDS. 1998;9:74-78.
7. Bornstein J, Zarfati D, Goldik Z, Abramovici H. Vulvar vestibulitis: physical or psychosexual problem? Obstet Gynecol. 1999;93(5 Pt 2):876-880.
8. Schneider D, Yaron M, Bukovsky I, Soffer Y, Halpern R. Outcome of surgical treatment for superficial dyspareunia from vulvar vestibulitis. J Reprod Med. 2001;46:227-231.
9. Herod JJ, Shafi MI, Rollason TP, Jordan JA, Luesley DM. Vulvar intraepithelial neoplasia: long-term follow-up of treated and untreated women. Br J Obstet Gynaecol. 1996;103:446-452.
10. Joura EA, Lösch A, Haider-Angeler M-G, Breitenecker G, Leodolter S. Trends in vulvar neoplasia. J Reprod Med. 2000;45:613-615.
11. Rutledge F, Sinclair M. Treatment of intraepithelial carcinoma of the vulva by skin excision and graft. Am J Obstet Gynecol. 1968;102:807-818.
12. Bergeron S, Bouchard C, Fortier M, Binik YM, Khalife S. The surgical treatment of vulvar vestibulitis syndrome: a follow-up study. J Sex Marital Ther. 1997;23:317-325.
13. Kehoe S, Luesley D. An evaluation of modified vestibulectomy in the treatment of vulvar vestibulitis: preliminary results. Acta Obstet Gynecol Scand. 1996;75:676-677.
14. Mann MS, Kaufman RH, Brown D, Jr, Adam E. Vulvar vestibulitis: significant clinical variables and treatment outcome. Obstet Gynecol. 1992;79:122-125.
15. Schover LR, Youngs DD, Cannata R. Psychosexual aspects of the evaluation and management of vulvar vestibulitis. Am J Obstet Gynecol. 1992;167:630-636.
16. Marinoff SC, Turner ML. Vulvar vestibulitis syndrome: an overview. Am J Obstet Gynecol. 1991;165:1228-1233.
17. Haefner HK, Collins ME, Davis GD, et al. The vulvodynia guideline. J Low Genit Tract Dis. 2005;9:45-51.