User login
In 1976, Abbey S. Meyers, a mother from Connecticut, finally got a diagnosis for her son. He had been displaying “very bizarre symptoms,” Ms. Meyers said in an interview with IndoUSRare,1 but, eventually, at 8 years of age, he was given a diagnosis of Tourette syndrome.
“They tried some medicine to try to get him to sit still, but the drugs didn’t work – or if they did, they put him to sleep,” she recounted. “The teachers would be angry that he fell asleep in the classroom.”
Ms. Meyers consulted the late Arthur K. Shapiro, MD, at what was then named the Mount Sinai School of Medicine in New York. Dr. Shapiro was conducting a small clinical trial of pimozide, a drug under investigation for schizophrenia, for its utility in children with Tourette syndrome.
“The drug worked like magic,” Ms. Meyers reported. Her son’s symptoms were substantially reduced, without sedation. He was followed by Dr. Shapiro every 3 months, at which point he would receive a 90-day refill.
However, when her son turned 10 years of age, Dr. Shapiro was no longer able to provide refills: The Food and Drug Administration (FDA) had turned down the drug manufacturer’s application for approval of pimozide for a schizophrenia indication. The company opted not to pursue further development of the drug because it was not deemed profitable.2
Pimozide became unavailable in the United States. The fact that the drug was so promising for Tourette syndrome did not warrant further investment because Tourette syndrome affected a relatively small number of people.
“I was just devastated,” Ms. Meyers reported.
Springing into advocacy
Ms. Meyers, who was working with the Tourette Syndrome Association at the time (now the Tourette Association of America), contacted people from other rare disease organizations, including the National Huntington’s Disease Association (today the Huntington’s Disease Society of America) and the Paget Foundation (today part of the Bone Health and Osteoporosis Foundation). Those organizations were experiencing similar problems with drug companies that wouldn’t engage in research and development of drugs for patients who had a rare disorder.
“We realized we had to work together to get something done to solve this problem,” Ms. Meyers said.
The sense of urgency over this roadblock increased when another patient who was taking pimozide tried to get a supply of the drug from Canada and was blocked from doing so by customs officials at the airport because the drug was not FDA approved. Working with that patient’s mother, Ms. Meyers contacted U.S. Representative Henry A. Waxman (D-Calif.), who was chair of the Subcommittee on Health and the Environment of the House Energy & Commerce Committee.
Ms. Meyers thought that Congress needed Rep. Waxman’s support if it was going to get involved with this problem. “So, we got Henry Waxman and his staff familiar with the orphan drug problem.”
ODA: Breakthrough legislation
The impetus for the Orphan Drug Act (ODA) started in 1979 with an FDA task force report calling for measures to address what was labeled the “orphan drug problem.”3
In 1982, Rep. Waxman convened a hearing and invited several pharmaceutical companies to attend. They declined the invitation. Ms. Meyers testified at the hearing, which was covered by the Los Angeles Times, giving the issue notoriety.
The issue was also addressed in the popular television series Quincy, M.E. Episodes depicted challenges facing a patient with Tourette syndrome and a patient with myoclonus. Series star Jack Klugman testified before Congress about the need for legislation regarding the development of drugs targeting the treatment of rare diseases.4
Rep. Waxman became the bill’s primary House sponsor. The ODA was approved by the House of Representatives on Dec. 14, 1982.
The combined efforts of the advocacy coalition ultimately culminated in the original ODA being signed into law by President Ronald Reagan on Jan. 4, 1983. The ODA incentivized pharmaceutical companies to allot more resources toward research on and development and distribution of therapeutics for people with a rare disease who had, until that point, been “orphaned,” so to speak, by the medical and scientific community.5
What is it to be a ‘rare disorder’ or an ‘orphan drug’?
The ODA defines a rare disorder as either a condition that affects fewer than 200,000 people or a condition that affects more than 200,000 people but for which there is no reasonable expectation that a pharmaceutical company will recoup the cost of developing a drug by selling it.5

In an interview Peter L. Saltonstall, president and CEO of the National Organization for Rare Disorders, commended Ms. Meyers on her tireless work: “She went from being a mom to a powerful advocate who got thousands of people in D.C. moving Congress to a point where they felt passing the law was necessary. In fact, she was there when the bill was signed into law.”
The FDA can grant orphan drug approval for several categories of products. These include new molecular entities, already-approved drugs for which an additional indication has been designated, and new formulations of existing or established drugs.5
Orphan-drug designation includes tax credits for the developer-manufacturer, a waiver of the usual approval fees that the company must pay to the FDA, and 7 years’ market exclusivity, during which time the FDA cannot award approval of similar treatments for the same indication.
“This [designation] ensures that the company that developed the drug can retain the opportunity for profit,” explained Mr. Saltonstall. “Companies thought: ‘We can afford to do this now. And if we market it the right way and have exclusivity, we can recover some of our profits.’”
Before the ODA, 30 drugs had been approved by the FDA for orphan conditions. By the end of 2022, more than 880 drugs were FDA approved to treat hundreds of rare disorders.
“This just shows the motivation and how the process works,” Mr. Saltonstall said. In fact, almost 50% of novel drugs approved in 2022 by the FDA were an orphan product or had an orphan indication.
In addition to the impact on drug development in the United States, enactment of the ODA had a broader ripple effect, inspiring similar changes internationally in Europe, Australia, Singapore, Japan, and other regions.5
NORD is born
The creation of NORD was initiated by the same group of advocates who lobbied tirelessly for passage of the ODA – including Ms. Meyers, who served as president of the organization for many years. Heidi Ross, MPH, NORD’s vice president of policy and regulatory affairs, called these advocates “trailblazers.”
NORD was founded in May 1983. The organization included, at that time, 40-50 disease-specific organizations. Today, NORD membership comprises more than 330 patient advocacy groups.
“The goal was to be a voice for those organizations and help get them mobilized, help them get their 501(c)3 [status], help them develop their relationship with the FDA, and similar tasks,” Mr. Saltonstall said. “We continue this important work today as the patient groups play a central role in driving care, research, and policies for their given disease. Also, there’s strength in numbers. We call upon these groups and members to help advocate in Washington for policies that impact the greater rare disease community.”
The ODA launched 4 decades of innovation and change, with NORD strengthening the rare disorder community, which encompasses more than 30 million Americans.
“The organization exists to support people living with rare disorders and tries to improve their quality of life,” according to Katie Kowalski, MPH, NORD’s associate director of education.
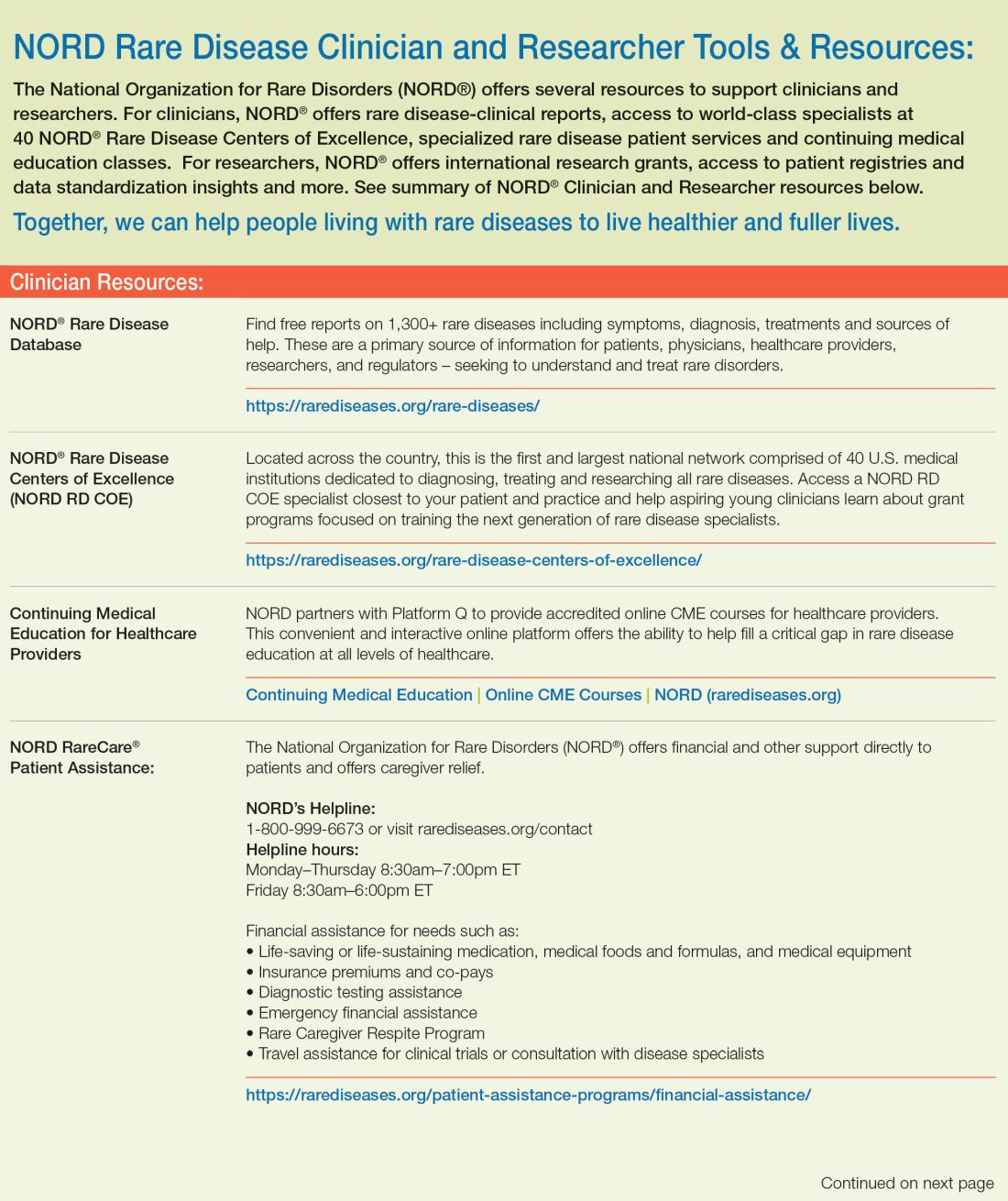
Education. The role of Ms. Kowalski’s department is to “educate patients and caregivers, the general public, health care professionals, and students preparing for health care careers about rare conditions,” Ms. Kowalski said. The education department maintains NORD’s Rare Disease Database,6 which contains more than 1,300 reports about rare conditions. Plus, NORD’s Rare Disease Library archives videos about specific diseases and other topics of interest to the rare disease community, including genetic testing and gene therapy.Continuing medical education programs are available for health care providers.
Events. NORD hosts:
An annual Rare Diseases and Orphan Products Breakthrough Summit for various rare disease stakeholders, including global rare disease medical experts, policy makers, regulatory agencies, industry leaders, and patient community members.
An annual patient and family conference; the 2024 edition is scheduled for June 7-8, 2024, in Los Angeles.
Membership support. NORD’s membership department supports any advocacy organization that represents a rare
disorder. “Some [organizations] are more evolved and sophisticated and can do their own educational programming,” Ms. Kowalski said. “Others are fledgling, nascent organizations that may not have the staff or money for salaries. We try to support them, teach them how to budget and raise funds and form a board of directors.”
Advocacy. NORD has a policy department that works at state and federal levels to advocate for policies affecting patients with a rare disease. Mr. Saltonstall shared that NORD was responsible for setting up and helping put together the rare disease office at the National Institutes of Health and the FDA, and continues to foster a close relationship with those offices.8,9 “In fact,” he said, “nothing happens in Washington regarding rare diseases without our being consulted or at the table.”
Focus on the patient. Mr. Saltonstall assumed his role at NORD in 2008. “By then, many fundamental things had been mastered, and we were ready to take things to the next level,” he said. “There were opportunities to leverage the ODA to help patient organizations.”
“We’re one of the only nonprofit advocacy organizations I know of without industry on the board or as members,” Mr. Saltonstall said. “The organization is completely patient focused. Everything we do comes back to committees with patients who make the decisions and management who helps implement those decisions. This makes us unique. The fact that we’re independent makes Congress trust us to be the true voice of patients.”
Spotlight: Patient care and research
Edward Neilan, MD, PhD, recently joined NORD as chief medical and scientific officer. As a pediatrician, medical geneticist, and molecular biologist, Dr. Neilan became acquainted with NORD as far back as medical school and his residency, when he used a book called the NORD Guide to Rare Disorders to help him explain certain diseases to patients and families.10 “I had a favorable view of NORD because of how useful the book was,” he said.

Dr. Neilan had also received research funding from NORD, almost 20 years ago – a pilot grant for Cockayne syndrome, an extremely rare multisystem genetic disorder characterized by premature aging. “At any given time, there are only about 100 or so identified patients with this condition.”11
Pilot grants are awarded after NORD announces a request for proposals and the proposals received are scored by rare disease medical experts, Dr. Neilan explained. “Because this grant helped me research the condition and get my academic career moving, I always had a warm spot for NORD.”
Excellence in care. Dr. Neilan assumed his position at NORD to become involved with the NORD Rare Disease Centers of Excellence program, which he describes as encouraging “collaboration with, and between, dozens of leading medical centers around the country.”
Dr. Neilan is the first physician to work full time at NORD. “Taking the step of designating and directing collaboration amongst centers of excellence around the country seemed to require having a full-time physician on board,” he said, “so I decided to jump in.”
Ms. Kowalski elaborated: “NORD’s Rare Disease Centers of Excellence includes 11 different working groups to address the big problems that need to be solved in rare diseases: working collaboratively. [This] is sometimes rare in academic medicine, but necessary, especially when there aren’t many patients with a given condition.”
Since Dr. Neilan’s arrival, NORD has designated 40 institutions across the country as a NORD Rare Disease Centers of Excellence.12
Natural history research
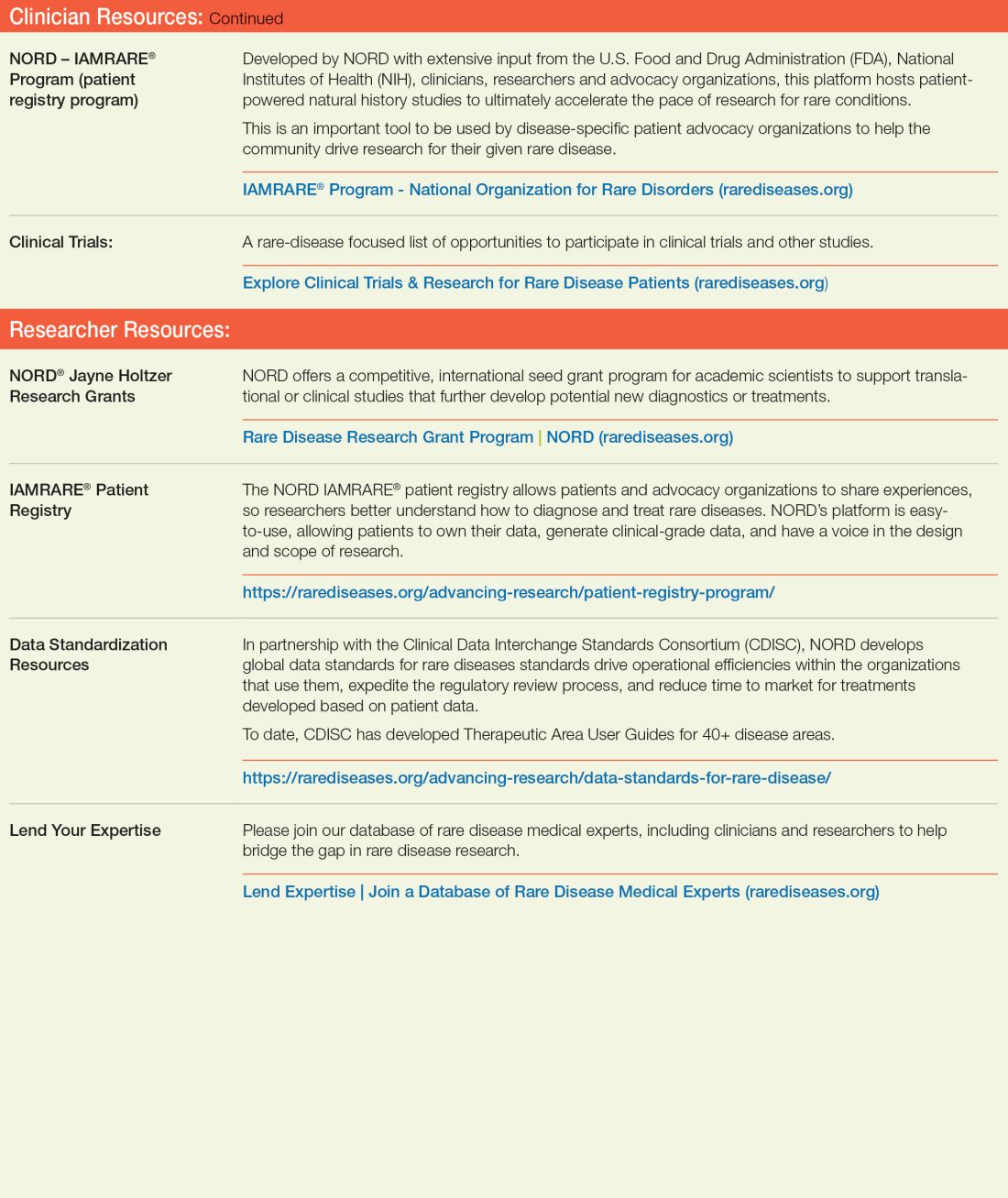
NORD’s research department awards seed grants to academic investigators who are researching rare disorders and has built an online patient registry platform that helps other, disease-specific patient advocacy organizations conduct natural history studies.
Dr. Neilan said that the registry program was motivated by input from the FDA indicating that companies were sometimes trying to develop drugs to treat a rare disease before fully understanding the natural history of that disease.
“There was a perceived lack of enough natural history data,” Dr. Neilan explained, “so how could the effectiveness of the drug be measured? What would be a meaningful improvement?” NORD assists in making these rare disease foundations more “research ready” so that enough will be known about the disease for drug development “to have a greater chance of success.”
“There’s a lot of promise on the horizon with gene therapy, and the new platforms may accelerate the production of these therapies,” Ms. Kowalski said.
Registries are customized to each disease and foundation by experts, patients, and families involved with that particular disease and foundation. For example: An ongoing study on the NORD platform is a study of metachromatic leukodystrophy (MLD), an autosomal-recessive lysosomal disorder that results in a buildup of sulfatides, a major lipid group in serum, which lead to destruction of the myelin sheath and progressive demyelination of the nervous system.13
“[MLD] is a tragic disorder that can first present in late infancy and may progress rapidly over 6 months or so to the point that children lose much of their neurological functioning,” Dr. Neilan said.
The FDA funded NORD to run the HOME study,14,15 in which families can participate without visiting a research site in person. This was particularly valuable during the COVID-19 pandemic, when many studies were “forced to shift gears and see how much data could be collected if patients were afraid to come to the hospital or not allowed to go to a hospital for nonemergency visits,” Dr. Neilan said.
The HOME study was designed before the onset of the COVID-19 pandemic to reduce the burden on patients of participating in research. The trial became a trend-setter in the shift to what are known as decentralized trials, in which research can be conducted through video, using a tablet that NORD mails to the family.
“This is obviously much more convenient for families who no longer have to travel long distances to the few sites in the country – which are often hundreds or even thousands of miles away – that are studying the condition,” Dr. Neilan said. The decentralized trial model is being used with other conditions, as well.
“There are infantile, juvenile, and adult-onset forms of MLD, and the limited therapeutic options may involve bone-marrow transplant, which may be at least partially effective, as donor-derived bone marrow–derived cells can provide enzymes to protect the brain,” said Dr. Neilan. Gene therapy for MLD has also been developed and is approved in Europe, but not in the United States. “MLD is typical of conditions that often start early in childhood and are progressive, so that, sometimes, by the time the parent realizes that there’s a problem, too much damage has been done to the brain for much repair to take place. Prevention of further damage is easier than reversing an ongoing disease process, so early treatment is important.” That’s why the number of movements to expand newborn screening for various conditions, to identify them before symptoms develop, is increasing.
“That’s another area where NORD has historically been active – in encouraging newborn screening,” Dr. Neilan said.
Evolution of the ODA
Since 1983, “a number of amendments ... made the original [ODA] stronger or refined it in various ways,” said Mr. Saltonstall. NORD continues to “very carefully watch any attempts to change it, alter it, move it, take pieces away from it, or – some people say – to make it ‘better.’ To us, it’s a very important law.”
Orphan Drug Credit (ODC). Ms. Ross elaborated: “In recent years, Congress has considered significant changes to the Orphan Drug Credit, which is one of several critical incentives established by the ODA.” When established in 1983, the ODC provided sponsors of a drug with a 50% tax credit for qualified clinical testing expenses associated with developing an orphan drug.
“Unfortunately, despite fierce opposition from NORD and our army of membership organizations and grassroots advocates,” Ms. Ross said, “the Tax Cuts and Jobs Act of 2017 reduced the ODC from 50% to 25%. Given the significant amount of time it takes to conduct research and development into rare diseases, we still don’t have a good sense as to the impact of the ODC being reduced to 25%.”
However, efforts to further limit the availability of the ODC during debate around the Build Back Better framework in 2021 were ultimately defeated. That defeat was, in part, a result of NORD’s rare disease community’s advocacy,16 when no changes to the ODC were included in the Inflation Reduction Act.
Patient Assistance Program. In 1987, NORD’s multifaceted patient assistance program (serving today under the umbrella name RareCare17) was founded to help patients obtain lifesaving or life-sustaining medication that they could not otherwise afford, Ms. Ross said. This was based on an unmet need for patients living and struggling with a rare disease who didn’t have access to the care and treatment they needed. “There was no other foundation equipped to do this at the time. NORD came forward to develop the first program of its kind.”
The program provides medication, financial assistance with insurance premiums and copays, diagnostic testing assistance, and travel assistance for clinical trials or consultation with disease specialists. According to Ms. Ross, “today, NORD’s patient assistance program provides, on average, $30 million to $40 million in patient assistance annually to eligible patients and families.”
Pharmaceutical companies do contribute to the patient assistance program. “However, they’re in the dark as to how the money is allocated,” said Mr. Saltonstall. “For example, a given company might donate money for patients with a particular disease but won’t know if patients who have that disease will necessarily receive funds to use toward that company’s drug. The patient might receive assistance to take a drug made by a different company – a competitor.”
There are approximately 14 foundations around the country that have worked within the constraints of the Department of Health & Human Services Office of Inspector General, which established rules about how foundations must operate. Under the broader umbrella of NORD, these foundations also help pay coinsurance costs or provide drugs at no cost to patients who meet financial criteria.
An enduring movement
Despite the successes brought about by the ODA, the search for new rare disorder treatments is far from over. We know of more than 7,000 rare diseases; scientists discover more every year. Fewer than 5% of rare disorders have an FDA-approved treatment.
Similar to advancements made in other diseases, progress in rare disease care and treatments will continue to require an all-in approach to solve what is a looming and massive public health challenge.
As NORD founder Abbey S. Meyers wrote in her 2016 book, Orphan Drugs: A Global Crusade: “It was all of us working together that built an impregnable movement demanding a solution. In the end, with the help of government and a touch of Hollywood, the forces opposing us could not win.”
References
1. Rare Disease Day 2023 at IndoUSrare – Fireside Chat with Dr. Abbey S. Meyers. 2023 Mar 3. Indo US Organization for Rare Diseases. https://www.youtube.com/watch?v=fGTWUcQJPlU.
2. Mikami K. Soc Hist Med. 2019;32(3):609-30. doi: 10.1093/shm/hkx098.
3. National Organization for Rare Disorders. The Orphan Drug Act Turns 40: NORD Celebrates Its Impact on Rare Diseases. 2023 Jan 4. https://rarediseases.org/the-orphan-drug-act-turns-40-nord-celebrates-its-impact-on-rare-diseases. 4. Swann J. The story behind the Orphan Drug Act. US Food and Drug Administration. 2018 Feb 23. https://www.fda.gov/industry/fdas-rare-disease-day/story-behind-orphan-drug-act.
5. Roberts A-D and Wadhwa R. Orphan drug approval laws, in StatPearls (Internet). StatPearls Publishing. 2023 Jun 5. www.ncbi.nlm.nih.gov/books/NBK572052/#.
6. National Organization for Rare Disorders. Rare disease database. https://rarediseases.org/rare-diseases/.
7. National Organization for Rare Disorders. Rare disease video library. 2023 Jan 19. https://rarediseases.org/video-library/.
8. National Center for Advancing Translational Sciences. Rare disease research and resources. 2023 May 16. Accessed Sep. 17., 2023. https://ncats.nih.gov/rare-diseases.
9. Food and Drug Administration. Rare diseases team. 2023 Aug 29. https://www.fda.gov/about-fda/center-drug-evaluation-and-research-cder/rare-diseases-team.
10. National Organization for Rare Disorders. “NORD Guide to Rare Disorders,” 3rd edition. Philadelphia: Lippincott Williams & Wilkins, 2002.
11. National Organization for Rare Disorders. Cockayne syndrome. 2022 Jun 7. https://rarediseases.org/rare-diseases/cockayne-syndrome/.
12. National Organization for Rare Disorders. NORD Rare Disease Centers of Excellence. 2023 Jun 28. https://rarediseases.org/rare-disease-centers-of-excellence/.
13. National Organization for Rare Disorders. Metachromatic leukodystrophy. 2022 Mar 22. https://rarediseases.org/rare-diseases/metachromatic-leukodystrophy/#complete-report.
14. National Organization for Rare Disorders. The Natural History of Metachromatic Leukodystrophy Study. 2023 Feb 23. https://rarediseases.org/mld-home-study/.
15. The Natural History of Metachromatic Leukodystrophy Study (HOME Study). 2023 Jun 13. https://clinicaltrials.gov/study/NCT04628364?.
16. National Organization for Rare Disorders, Saltonstall PL. Letter to US Congress House Committee on Ways and Means. 2021 Sep 13. https://rarediseases.org/wp-content/uploads/2022/04/NORD_ODTC-Letter_FINAL.pdf.
17. National Organization for Rare Disorders. RareCare®: NORD’s patient assistance programs. 2022 Nov 1. https://rarediseases.org/wp-content/uploads/2022/04/NORD_ODTC-Letter_FINAL.pdf.
In 1976, Abbey S. Meyers, a mother from Connecticut, finally got a diagnosis for her son. He had been displaying “very bizarre symptoms,” Ms. Meyers said in an interview with IndoUSRare,1 but, eventually, at 8 years of age, he was given a diagnosis of Tourette syndrome.
“They tried some medicine to try to get him to sit still, but the drugs didn’t work – or if they did, they put him to sleep,” she recounted. “The teachers would be angry that he fell asleep in the classroom.”
Ms. Meyers consulted the late Arthur K. Shapiro, MD, at what was then named the Mount Sinai School of Medicine in New York. Dr. Shapiro was conducting a small clinical trial of pimozide, a drug under investigation for schizophrenia, for its utility in children with Tourette syndrome.
“The drug worked like magic,” Ms. Meyers reported. Her son’s symptoms were substantially reduced, without sedation. He was followed by Dr. Shapiro every 3 months, at which point he would receive a 90-day refill.
However, when her son turned 10 years of age, Dr. Shapiro was no longer able to provide refills: The Food and Drug Administration (FDA) had turned down the drug manufacturer’s application for approval of pimozide for a schizophrenia indication. The company opted not to pursue further development of the drug because it was not deemed profitable.2
Pimozide became unavailable in the United States. The fact that the drug was so promising for Tourette syndrome did not warrant further investment because Tourette syndrome affected a relatively small number of people.
“I was just devastated,” Ms. Meyers reported.
Springing into advocacy
Ms. Meyers, who was working with the Tourette Syndrome Association at the time (now the Tourette Association of America), contacted people from other rare disease organizations, including the National Huntington’s Disease Association (today the Huntington’s Disease Society of America) and the Paget Foundation (today part of the Bone Health and Osteoporosis Foundation). Those organizations were experiencing similar problems with drug companies that wouldn’t engage in research and development of drugs for patients who had a rare disorder.
“We realized we had to work together to get something done to solve this problem,” Ms. Meyers said.
The sense of urgency over this roadblock increased when another patient who was taking pimozide tried to get a supply of the drug from Canada and was blocked from doing so by customs officials at the airport because the drug was not FDA approved. Working with that patient’s mother, Ms. Meyers contacted U.S. Representative Henry A. Waxman (D-Calif.), who was chair of the Subcommittee on Health and the Environment of the House Energy & Commerce Committee.
Ms. Meyers thought that Congress needed Rep. Waxman’s support if it was going to get involved with this problem. “So, we got Henry Waxman and his staff familiar with the orphan drug problem.”
ODA: Breakthrough legislation
The impetus for the Orphan Drug Act (ODA) started in 1979 with an FDA task force report calling for measures to address what was labeled the “orphan drug problem.”3
In 1982, Rep. Waxman convened a hearing and invited several pharmaceutical companies to attend. They declined the invitation. Ms. Meyers testified at the hearing, which was covered by the Los Angeles Times, giving the issue notoriety.
The issue was also addressed in the popular television series Quincy, M.E. Episodes depicted challenges facing a patient with Tourette syndrome and a patient with myoclonus. Series star Jack Klugman testified before Congress about the need for legislation regarding the development of drugs targeting the treatment of rare diseases.4
Rep. Waxman became the bill’s primary House sponsor. The ODA was approved by the House of Representatives on Dec. 14, 1982.
The combined efforts of the advocacy coalition ultimately culminated in the original ODA being signed into law by President Ronald Reagan on Jan. 4, 1983. The ODA incentivized pharmaceutical companies to allot more resources toward research on and development and distribution of therapeutics for people with a rare disease who had, until that point, been “orphaned,” so to speak, by the medical and scientific community.5
What is it to be a ‘rare disorder’ or an ‘orphan drug’?
The ODA defines a rare disorder as either a condition that affects fewer than 200,000 people or a condition that affects more than 200,000 people but for which there is no reasonable expectation that a pharmaceutical company will recoup the cost of developing a drug by selling it.5
In an interview Peter L. Saltonstall, president and CEO of the National Organization for Rare Disorders, commended Ms. Meyers on her tireless work: “She went from being a mom to a powerful advocate who got thousands of people in D.C. moving Congress to a point where they felt passing the law was necessary. In fact, she was there when the bill was signed into law.”
The FDA can grant orphan drug approval for several categories of products. These include new molecular entities, already-approved drugs for which an additional indication has been designated, and new formulations of existing or established drugs.5
Orphan-drug designation includes tax credits for the developer-manufacturer, a waiver of the usual approval fees that the company must pay to the FDA, and 7 years’ market exclusivity, during which time the FDA cannot award approval of similar treatments for the same indication.
“This [designation] ensures that the company that developed the drug can retain the opportunity for profit,” explained Mr. Saltonstall. “Companies thought: ‘We can afford to do this now. And if we market it the right way and have exclusivity, we can recover some of our profits.’”
Before the ODA, 30 drugs had been approved by the FDA for orphan conditions. By the end of 2022, more than 880 drugs were FDA approved to treat hundreds of rare disorders.
“This just shows the motivation and how the process works,” Mr. Saltonstall said. In fact, almost 50% of novel drugs approved in 2022 by the FDA were an orphan product or had an orphan indication.
In addition to the impact on drug development in the United States, enactment of the ODA had a broader ripple effect, inspiring similar changes internationally in Europe, Australia, Singapore, Japan, and other regions.5
NORD is born
The creation of NORD was initiated by the same group of advocates who lobbied tirelessly for passage of the ODA – including Ms. Meyers, who served as president of the organization for many years. Heidi Ross, MPH, NORD’s vice president of policy and regulatory affairs, called these advocates “trailblazers.”
NORD was founded in May 1983. The organization included, at that time, 40-50 disease-specific organizations. Today, NORD membership comprises more than 330 patient advocacy groups.
“The goal was to be a voice for those organizations and help get them mobilized, help them get their 501(c)3 [status], help them develop their relationship with the FDA, and similar tasks,” Mr. Saltonstall said. “We continue this important work today as the patient groups play a central role in driving care, research, and policies for their given disease. Also, there’s strength in numbers. We call upon these groups and members to help advocate in Washington for policies that impact the greater rare disease community.”
The ODA launched 4 decades of innovation and change, with NORD strengthening the rare disorder community, which encompasses more than 30 million Americans.
“The organization exists to support people living with rare disorders and tries to improve their quality of life,” according to Katie Kowalski, MPH, NORD’s associate director of education.
Education. The role of Ms. Kowalski’s department is to “educate patients and caregivers, the general public, health care professionals, and students preparing for health care careers about rare conditions,” Ms. Kowalski said. The education department maintains NORD’s Rare Disease Database,6 which contains more than 1,300 reports about rare conditions. Plus, NORD’s Rare Disease Library archives videos about specific diseases and other topics of interest to the rare disease community, including genetic testing and gene therapy.Continuing medical education programs are available for health care providers.
Events. NORD hosts:
An annual Rare Diseases and Orphan Products Breakthrough Summit for various rare disease stakeholders, including global rare disease medical experts, policy makers, regulatory agencies, industry leaders, and patient community members.
An annual patient and family conference; the 2024 edition is scheduled for June 7-8, 2024, in Los Angeles.
Membership support. NORD’s membership department supports any advocacy organization that represents a rare
disorder. “Some [organizations] are more evolved and sophisticated and can do their own educational programming,” Ms. Kowalski said. “Others are fledgling, nascent organizations that may not have the staff or money for salaries. We try to support them, teach them how to budget and raise funds and form a board of directors.”
Advocacy. NORD has a policy department that works at state and federal levels to advocate for policies affecting patients with a rare disease. Mr. Saltonstall shared that NORD was responsible for setting up and helping put together the rare disease office at the National Institutes of Health and the FDA, and continues to foster a close relationship with those offices.8,9 “In fact,” he said, “nothing happens in Washington regarding rare diseases without our being consulted or at the table.”
Focus on the patient. Mr. Saltonstall assumed his role at NORD in 2008. “By then, many fundamental things had been mastered, and we were ready to take things to the next level,” he said. “There were opportunities to leverage the ODA to help patient organizations.”
“We’re one of the only nonprofit advocacy organizations I know of without industry on the board or as members,” Mr. Saltonstall said. “The organization is completely patient focused. Everything we do comes back to committees with patients who make the decisions and management who helps implement those decisions. This makes us unique. The fact that we’re independent makes Congress trust us to be the true voice of patients.”
Spotlight: Patient care and research
Edward Neilan, MD, PhD, recently joined NORD as chief medical and scientific officer. As a pediatrician, medical geneticist, and molecular biologist, Dr. Neilan became acquainted with NORD as far back as medical school and his residency, when he used a book called the NORD Guide to Rare Disorders to help him explain certain diseases to patients and families.10 “I had a favorable view of NORD because of how useful the book was,” he said.
Dr. Neilan had also received research funding from NORD, almost 20 years ago – a pilot grant for Cockayne syndrome, an extremely rare multisystem genetic disorder characterized by premature aging. “At any given time, there are only about 100 or so identified patients with this condition.”11
Pilot grants are awarded after NORD announces a request for proposals and the proposals received are scored by rare disease medical experts, Dr. Neilan explained. “Because this grant helped me research the condition and get my academic career moving, I always had a warm spot for NORD.”
Excellence in care. Dr. Neilan assumed his position at NORD to become involved with the NORD Rare Disease Centers of Excellence program, which he describes as encouraging “collaboration with, and between, dozens of leading medical centers around the country.”
Dr. Neilan is the first physician to work full time at NORD. “Taking the step of designating and directing collaboration amongst centers of excellence around the country seemed to require having a full-time physician on board,” he said, “so I decided to jump in.”
Ms. Kowalski elaborated: “NORD’s Rare Disease Centers of Excellence includes 11 different working groups to address the big problems that need to be solved in rare diseases: working collaboratively. [This] is sometimes rare in academic medicine, but necessary, especially when there aren’t many patients with a given condition.”
Since Dr. Neilan’s arrival, NORD has designated 40 institutions across the country as a NORD Rare Disease Centers of Excellence.12
Natural history research
NORD’s research department awards seed grants to academic investigators who are researching rare disorders and has built an online patient registry platform that helps other, disease-specific patient advocacy organizations conduct natural history studies.
Dr. Neilan said that the registry program was motivated by input from the FDA indicating that companies were sometimes trying to develop drugs to treat a rare disease before fully understanding the natural history of that disease.
“There was a perceived lack of enough natural history data,” Dr. Neilan explained, “so how could the effectiveness of the drug be measured? What would be a meaningful improvement?” NORD assists in making these rare disease foundations more “research ready” so that enough will be known about the disease for drug development “to have a greater chance of success.”
“There’s a lot of promise on the horizon with gene therapy, and the new platforms may accelerate the production of these therapies,” Ms. Kowalski said.
Registries are customized to each disease and foundation by experts, patients, and families involved with that particular disease and foundation. For example: An ongoing study on the NORD platform is a study of metachromatic leukodystrophy (MLD), an autosomal-recessive lysosomal disorder that results in a buildup of sulfatides, a major lipid group in serum, which lead to destruction of the myelin sheath and progressive demyelination of the nervous system.13
“[MLD] is a tragic disorder that can first present in late infancy and may progress rapidly over 6 months or so to the point that children lose much of their neurological functioning,” Dr. Neilan said.
The FDA funded NORD to run the HOME study,14,15 in which families can participate without visiting a research site in person. This was particularly valuable during the COVID-19 pandemic, when many studies were “forced to shift gears and see how much data could be collected if patients were afraid to come to the hospital or not allowed to go to a hospital for nonemergency visits,” Dr. Neilan said.
The HOME study was designed before the onset of the COVID-19 pandemic to reduce the burden on patients of participating in research. The trial became a trend-setter in the shift to what are known as decentralized trials, in which research can be conducted through video, using a tablet that NORD mails to the family.
“This is obviously much more convenient for families who no longer have to travel long distances to the few sites in the country – which are often hundreds or even thousands of miles away – that are studying the condition,” Dr. Neilan said. The decentralized trial model is being used with other conditions, as well.
“There are infantile, juvenile, and adult-onset forms of MLD, and the limited therapeutic options may involve bone-marrow transplant, which may be at least partially effective, as donor-derived bone marrow–derived cells can provide enzymes to protect the brain,” said Dr. Neilan. Gene therapy for MLD has also been developed and is approved in Europe, but not in the United States. “MLD is typical of conditions that often start early in childhood and are progressive, so that, sometimes, by the time the parent realizes that there’s a problem, too much damage has been done to the brain for much repair to take place. Prevention of further damage is easier than reversing an ongoing disease process, so early treatment is important.” That’s why the number of movements to expand newborn screening for various conditions, to identify them before symptoms develop, is increasing.
“That’s another area where NORD has historically been active – in encouraging newborn screening,” Dr. Neilan said.
Evolution of the ODA
Since 1983, “a number of amendments ... made the original [ODA] stronger or refined it in various ways,” said Mr. Saltonstall. NORD continues to “very carefully watch any attempts to change it, alter it, move it, take pieces away from it, or – some people say – to make it ‘better.’ To us, it’s a very important law.”
Orphan Drug Credit (ODC). Ms. Ross elaborated: “In recent years, Congress has considered significant changes to the Orphan Drug Credit, which is one of several critical incentives established by the ODA.” When established in 1983, the ODC provided sponsors of a drug with a 50% tax credit for qualified clinical testing expenses associated with developing an orphan drug.
“Unfortunately, despite fierce opposition from NORD and our army of membership organizations and grassroots advocates,” Ms. Ross said, “the Tax Cuts and Jobs Act of 2017 reduced the ODC from 50% to 25%. Given the significant amount of time it takes to conduct research and development into rare diseases, we still don’t have a good sense as to the impact of the ODC being reduced to 25%.”
However, efforts to further limit the availability of the ODC during debate around the Build Back Better framework in 2021 were ultimately defeated. That defeat was, in part, a result of NORD’s rare disease community’s advocacy,16 when no changes to the ODC were included in the Inflation Reduction Act.
Patient Assistance Program. In 1987, NORD’s multifaceted patient assistance program (serving today under the umbrella name RareCare17) was founded to help patients obtain lifesaving or life-sustaining medication that they could not otherwise afford, Ms. Ross said. This was based on an unmet need for patients living and struggling with a rare disease who didn’t have access to the care and treatment they needed. “There was no other foundation equipped to do this at the time. NORD came forward to develop the first program of its kind.”
The program provides medication, financial assistance with insurance premiums and copays, diagnostic testing assistance, and travel assistance for clinical trials or consultation with disease specialists. According to Ms. Ross, “today, NORD’s patient assistance program provides, on average, $30 million to $40 million in patient assistance annually to eligible patients and families.”
Pharmaceutical companies do contribute to the patient assistance program. “However, they’re in the dark as to how the money is allocated,” said Mr. Saltonstall. “For example, a given company might donate money for patients with a particular disease but won’t know if patients who have that disease will necessarily receive funds to use toward that company’s drug. The patient might receive assistance to take a drug made by a different company – a competitor.”
There are approximately 14 foundations around the country that have worked within the constraints of the Department of Health & Human Services Office of Inspector General, which established rules about how foundations must operate. Under the broader umbrella of NORD, these foundations also help pay coinsurance costs or provide drugs at no cost to patients who meet financial criteria.
An enduring movement
Despite the successes brought about by the ODA, the search for new rare disorder treatments is far from over. We know of more than 7,000 rare diseases; scientists discover more every year. Fewer than 5% of rare disorders have an FDA-approved treatment.
Similar to advancements made in other diseases, progress in rare disease care and treatments will continue to require an all-in approach to solve what is a looming and massive public health challenge.
As NORD founder Abbey S. Meyers wrote in her 2016 book, Orphan Drugs: A Global Crusade: “It was all of us working together that built an impregnable movement demanding a solution. In the end, with the help of government and a touch of Hollywood, the forces opposing us could not win.”
References
1. Rare Disease Day 2023 at IndoUSrare – Fireside Chat with Dr. Abbey S. Meyers. 2023 Mar 3. Indo US Organization for Rare Diseases. https://www.youtube.com/watch?v=fGTWUcQJPlU.
2. Mikami K. Soc Hist Med. 2019;32(3):609-30. doi: 10.1093/shm/hkx098.
3. National Organization for Rare Disorders. The Orphan Drug Act Turns 40: NORD Celebrates Its Impact on Rare Diseases. 2023 Jan 4. https://rarediseases.org/the-orphan-drug-act-turns-40-nord-celebrates-its-impact-on-rare-diseases. 4. Swann J. The story behind the Orphan Drug Act. US Food and Drug Administration. 2018 Feb 23. https://www.fda.gov/industry/fdas-rare-disease-day/story-behind-orphan-drug-act.
5. Roberts A-D and Wadhwa R. Orphan drug approval laws, in StatPearls (Internet). StatPearls Publishing. 2023 Jun 5. www.ncbi.nlm.nih.gov/books/NBK572052/#.
6. National Organization for Rare Disorders. Rare disease database. https://rarediseases.org/rare-diseases/.
7. National Organization for Rare Disorders. Rare disease video library. 2023 Jan 19. https://rarediseases.org/video-library/.
8. National Center for Advancing Translational Sciences. Rare disease research and resources. 2023 May 16. Accessed Sep. 17., 2023. https://ncats.nih.gov/rare-diseases.
9. Food and Drug Administration. Rare diseases team. 2023 Aug 29. https://www.fda.gov/about-fda/center-drug-evaluation-and-research-cder/rare-diseases-team.
10. National Organization for Rare Disorders. “NORD Guide to Rare Disorders,” 3rd edition. Philadelphia: Lippincott Williams & Wilkins, 2002.
11. National Organization for Rare Disorders. Cockayne syndrome. 2022 Jun 7. https://rarediseases.org/rare-diseases/cockayne-syndrome/.
12. National Organization for Rare Disorders. NORD Rare Disease Centers of Excellence. 2023 Jun 28. https://rarediseases.org/rare-disease-centers-of-excellence/.
13. National Organization for Rare Disorders. Metachromatic leukodystrophy. 2022 Mar 22. https://rarediseases.org/rare-diseases/metachromatic-leukodystrophy/#complete-report.
14. National Organization for Rare Disorders. The Natural History of Metachromatic Leukodystrophy Study. 2023 Feb 23. https://rarediseases.org/mld-home-study/.
15. The Natural History of Metachromatic Leukodystrophy Study (HOME Study). 2023 Jun 13. https://clinicaltrials.gov/study/NCT04628364?.
16. National Organization for Rare Disorders, Saltonstall PL. Letter to US Congress House Committee on Ways and Means. 2021 Sep 13. https://rarediseases.org/wp-content/uploads/2022/04/NORD_ODTC-Letter_FINAL.pdf.
17. National Organization for Rare Disorders. RareCare®: NORD’s patient assistance programs. 2022 Nov 1. https://rarediseases.org/wp-content/uploads/2022/04/NORD_ODTC-Letter_FINAL.pdf.
In 1976, Abbey S. Meyers, a mother from Connecticut, finally got a diagnosis for her son. He had been displaying “very bizarre symptoms,” Ms. Meyers said in an interview with IndoUSRare,1 but, eventually, at 8 years of age, he was given a diagnosis of Tourette syndrome.
“They tried some medicine to try to get him to sit still, but the drugs didn’t work – or if they did, they put him to sleep,” she recounted. “The teachers would be angry that he fell asleep in the classroom.”
Ms. Meyers consulted the late Arthur K. Shapiro, MD, at what was then named the Mount Sinai School of Medicine in New York. Dr. Shapiro was conducting a small clinical trial of pimozide, a drug under investigation for schizophrenia, for its utility in children with Tourette syndrome.
“The drug worked like magic,” Ms. Meyers reported. Her son’s symptoms were substantially reduced, without sedation. He was followed by Dr. Shapiro every 3 months, at which point he would receive a 90-day refill.
However, when her son turned 10 years of age, Dr. Shapiro was no longer able to provide refills: The Food and Drug Administration (FDA) had turned down the drug manufacturer’s application for approval of pimozide for a schizophrenia indication. The company opted not to pursue further development of the drug because it was not deemed profitable.2
Pimozide became unavailable in the United States. The fact that the drug was so promising for Tourette syndrome did not warrant further investment because Tourette syndrome affected a relatively small number of people.
“I was just devastated,” Ms. Meyers reported.
Springing into advocacy
Ms. Meyers, who was working with the Tourette Syndrome Association at the time (now the Tourette Association of America), contacted people from other rare disease organizations, including the National Huntington’s Disease Association (today the Huntington’s Disease Society of America) and the Paget Foundation (today part of the Bone Health and Osteoporosis Foundation). Those organizations were experiencing similar problems with drug companies that wouldn’t engage in research and development of drugs for patients who had a rare disorder.
“We realized we had to work together to get something done to solve this problem,” Ms. Meyers said.
The sense of urgency over this roadblock increased when another patient who was taking pimozide tried to get a supply of the drug from Canada and was blocked from doing so by customs officials at the airport because the drug was not FDA approved. Working with that patient’s mother, Ms. Meyers contacted U.S. Representative Henry A. Waxman (D-Calif.), who was chair of the Subcommittee on Health and the Environment of the House Energy & Commerce Committee.
Ms. Meyers thought that Congress needed Rep. Waxman’s support if it was going to get involved with this problem. “So, we got Henry Waxman and his staff familiar with the orphan drug problem.”
ODA: Breakthrough legislation
The impetus for the Orphan Drug Act (ODA) started in 1979 with an FDA task force report calling for measures to address what was labeled the “orphan drug problem.”3
In 1982, Rep. Waxman convened a hearing and invited several pharmaceutical companies to attend. They declined the invitation. Ms. Meyers testified at the hearing, which was covered by the Los Angeles Times, giving the issue notoriety.
The issue was also addressed in the popular television series Quincy, M.E. Episodes depicted challenges facing a patient with Tourette syndrome and a patient with myoclonus. Series star Jack Klugman testified before Congress about the need for legislation regarding the development of drugs targeting the treatment of rare diseases.4
Rep. Waxman became the bill’s primary House sponsor. The ODA was approved by the House of Representatives on Dec. 14, 1982.
The combined efforts of the advocacy coalition ultimately culminated in the original ODA being signed into law by President Ronald Reagan on Jan. 4, 1983. The ODA incentivized pharmaceutical companies to allot more resources toward research on and development and distribution of therapeutics for people with a rare disease who had, until that point, been “orphaned,” so to speak, by the medical and scientific community.5
What is it to be a ‘rare disorder’ or an ‘orphan drug’?
The ODA defines a rare disorder as either a condition that affects fewer than 200,000 people or a condition that affects more than 200,000 people but for which there is no reasonable expectation that a pharmaceutical company will recoup the cost of developing a drug by selling it.5
In an interview Peter L. Saltonstall, president and CEO of the National Organization for Rare Disorders, commended Ms. Meyers on her tireless work: “She went from being a mom to a powerful advocate who got thousands of people in D.C. moving Congress to a point where they felt passing the law was necessary. In fact, she was there when the bill was signed into law.”
The FDA can grant orphan drug approval for several categories of products. These include new molecular entities, already-approved drugs for which an additional indication has been designated, and new formulations of existing or established drugs.5
Orphan-drug designation includes tax credits for the developer-manufacturer, a waiver of the usual approval fees that the company must pay to the FDA, and 7 years’ market exclusivity, during which time the FDA cannot award approval of similar treatments for the same indication.
“This [designation] ensures that the company that developed the drug can retain the opportunity for profit,” explained Mr. Saltonstall. “Companies thought: ‘We can afford to do this now. And if we market it the right way and have exclusivity, we can recover some of our profits.’”
Before the ODA, 30 drugs had been approved by the FDA for orphan conditions. By the end of 2022, more than 880 drugs were FDA approved to treat hundreds of rare disorders.
“This just shows the motivation and how the process works,” Mr. Saltonstall said. In fact, almost 50% of novel drugs approved in 2022 by the FDA were an orphan product or had an orphan indication.
In addition to the impact on drug development in the United States, enactment of the ODA had a broader ripple effect, inspiring similar changes internationally in Europe, Australia, Singapore, Japan, and other regions.5
NORD is born
The creation of NORD was initiated by the same group of advocates who lobbied tirelessly for passage of the ODA – including Ms. Meyers, who served as president of the organization for many years. Heidi Ross, MPH, NORD’s vice president of policy and regulatory affairs, called these advocates “trailblazers.”
NORD was founded in May 1983. The organization included, at that time, 40-50 disease-specific organizations. Today, NORD membership comprises more than 330 patient advocacy groups.
“The goal was to be a voice for those organizations and help get them mobilized, help them get their 501(c)3 [status], help them develop their relationship with the FDA, and similar tasks,” Mr. Saltonstall said. “We continue this important work today as the patient groups play a central role in driving care, research, and policies for their given disease. Also, there’s strength in numbers. We call upon these groups and members to help advocate in Washington for policies that impact the greater rare disease community.”
The ODA launched 4 decades of innovation and change, with NORD strengthening the rare disorder community, which encompasses more than 30 million Americans.
“The organization exists to support people living with rare disorders and tries to improve their quality of life,” according to Katie Kowalski, MPH, NORD’s associate director of education.
Education. The role of Ms. Kowalski’s department is to “educate patients and caregivers, the general public, health care professionals, and students preparing for health care careers about rare conditions,” Ms. Kowalski said. The education department maintains NORD’s Rare Disease Database,6 which contains more than 1,300 reports about rare conditions. Plus, NORD’s Rare Disease Library archives videos about specific diseases and other topics of interest to the rare disease community, including genetic testing and gene therapy.Continuing medical education programs are available for health care providers.
Events. NORD hosts:
An annual Rare Diseases and Orphan Products Breakthrough Summit for various rare disease stakeholders, including global rare disease medical experts, policy makers, regulatory agencies, industry leaders, and patient community members.
An annual patient and family conference; the 2024 edition is scheduled for June 7-8, 2024, in Los Angeles.
Membership support. NORD’s membership department supports any advocacy organization that represents a rare
disorder. “Some [organizations] are more evolved and sophisticated and can do their own educational programming,” Ms. Kowalski said. “Others are fledgling, nascent organizations that may not have the staff or money for salaries. We try to support them, teach them how to budget and raise funds and form a board of directors.”
Advocacy. NORD has a policy department that works at state and federal levels to advocate for policies affecting patients with a rare disease. Mr. Saltonstall shared that NORD was responsible for setting up and helping put together the rare disease office at the National Institutes of Health and the FDA, and continues to foster a close relationship with those offices.8,9 “In fact,” he said, “nothing happens in Washington regarding rare diseases without our being consulted or at the table.”
Focus on the patient. Mr. Saltonstall assumed his role at NORD in 2008. “By then, many fundamental things had been mastered, and we were ready to take things to the next level,” he said. “There were opportunities to leverage the ODA to help patient organizations.”
“We’re one of the only nonprofit advocacy organizations I know of without industry on the board or as members,” Mr. Saltonstall said. “The organization is completely patient focused. Everything we do comes back to committees with patients who make the decisions and management who helps implement those decisions. This makes us unique. The fact that we’re independent makes Congress trust us to be the true voice of patients.”
Spotlight: Patient care and research
Edward Neilan, MD, PhD, recently joined NORD as chief medical and scientific officer. As a pediatrician, medical geneticist, and molecular biologist, Dr. Neilan became acquainted with NORD as far back as medical school and his residency, when he used a book called the NORD Guide to Rare Disorders to help him explain certain diseases to patients and families.10 “I had a favorable view of NORD because of how useful the book was,” he said.
Dr. Neilan had also received research funding from NORD, almost 20 years ago – a pilot grant for Cockayne syndrome, an extremely rare multisystem genetic disorder characterized by premature aging. “At any given time, there are only about 100 or so identified patients with this condition.”11
Pilot grants are awarded after NORD announces a request for proposals and the proposals received are scored by rare disease medical experts, Dr. Neilan explained. “Because this grant helped me research the condition and get my academic career moving, I always had a warm spot for NORD.”
Excellence in care. Dr. Neilan assumed his position at NORD to become involved with the NORD Rare Disease Centers of Excellence program, which he describes as encouraging “collaboration with, and between, dozens of leading medical centers around the country.”
Dr. Neilan is the first physician to work full time at NORD. “Taking the step of designating and directing collaboration amongst centers of excellence around the country seemed to require having a full-time physician on board,” he said, “so I decided to jump in.”
Ms. Kowalski elaborated: “NORD’s Rare Disease Centers of Excellence includes 11 different working groups to address the big problems that need to be solved in rare diseases: working collaboratively. [This] is sometimes rare in academic medicine, but necessary, especially when there aren’t many patients with a given condition.”
Since Dr. Neilan’s arrival, NORD has designated 40 institutions across the country as a NORD Rare Disease Centers of Excellence.12
Natural history research
NORD’s research department awards seed grants to academic investigators who are researching rare disorders and has built an online patient registry platform that helps other, disease-specific patient advocacy organizations conduct natural history studies.
Dr. Neilan said that the registry program was motivated by input from the FDA indicating that companies were sometimes trying to develop drugs to treat a rare disease before fully understanding the natural history of that disease.
“There was a perceived lack of enough natural history data,” Dr. Neilan explained, “so how could the effectiveness of the drug be measured? What would be a meaningful improvement?” NORD assists in making these rare disease foundations more “research ready” so that enough will be known about the disease for drug development “to have a greater chance of success.”
“There’s a lot of promise on the horizon with gene therapy, and the new platforms may accelerate the production of these therapies,” Ms. Kowalski said.
Registries are customized to each disease and foundation by experts, patients, and families involved with that particular disease and foundation. For example: An ongoing study on the NORD platform is a study of metachromatic leukodystrophy (MLD), an autosomal-recessive lysosomal disorder that results in a buildup of sulfatides, a major lipid group in serum, which lead to destruction of the myelin sheath and progressive demyelination of the nervous system.13
“[MLD] is a tragic disorder that can first present in late infancy and may progress rapidly over 6 months or so to the point that children lose much of their neurological functioning,” Dr. Neilan said.
The FDA funded NORD to run the HOME study,14,15 in which families can participate without visiting a research site in person. This was particularly valuable during the COVID-19 pandemic, when many studies were “forced to shift gears and see how much data could be collected if patients were afraid to come to the hospital or not allowed to go to a hospital for nonemergency visits,” Dr. Neilan said.
The HOME study was designed before the onset of the COVID-19 pandemic to reduce the burden on patients of participating in research. The trial became a trend-setter in the shift to what are known as decentralized trials, in which research can be conducted through video, using a tablet that NORD mails to the family.
“This is obviously much more convenient for families who no longer have to travel long distances to the few sites in the country – which are often hundreds or even thousands of miles away – that are studying the condition,” Dr. Neilan said. The decentralized trial model is being used with other conditions, as well.
“There are infantile, juvenile, and adult-onset forms of MLD, and the limited therapeutic options may involve bone-marrow transplant, which may be at least partially effective, as donor-derived bone marrow–derived cells can provide enzymes to protect the brain,” said Dr. Neilan. Gene therapy for MLD has also been developed and is approved in Europe, but not in the United States. “MLD is typical of conditions that often start early in childhood and are progressive, so that, sometimes, by the time the parent realizes that there’s a problem, too much damage has been done to the brain for much repair to take place. Prevention of further damage is easier than reversing an ongoing disease process, so early treatment is important.” That’s why the number of movements to expand newborn screening for various conditions, to identify them before symptoms develop, is increasing.
“That’s another area where NORD has historically been active – in encouraging newborn screening,” Dr. Neilan said.
Evolution of the ODA
Since 1983, “a number of amendments ... made the original [ODA] stronger or refined it in various ways,” said Mr. Saltonstall. NORD continues to “very carefully watch any attempts to change it, alter it, move it, take pieces away from it, or – some people say – to make it ‘better.’ To us, it’s a very important law.”
Orphan Drug Credit (ODC). Ms. Ross elaborated: “In recent years, Congress has considered significant changes to the Orphan Drug Credit, which is one of several critical incentives established by the ODA.” When established in 1983, the ODC provided sponsors of a drug with a 50% tax credit for qualified clinical testing expenses associated with developing an orphan drug.
“Unfortunately, despite fierce opposition from NORD and our army of membership organizations and grassroots advocates,” Ms. Ross said, “the Tax Cuts and Jobs Act of 2017 reduced the ODC from 50% to 25%. Given the significant amount of time it takes to conduct research and development into rare diseases, we still don’t have a good sense as to the impact of the ODC being reduced to 25%.”
However, efforts to further limit the availability of the ODC during debate around the Build Back Better framework in 2021 were ultimately defeated. That defeat was, in part, a result of NORD’s rare disease community’s advocacy,16 when no changes to the ODC were included in the Inflation Reduction Act.
Patient Assistance Program. In 1987, NORD’s multifaceted patient assistance program (serving today under the umbrella name RareCare17) was founded to help patients obtain lifesaving or life-sustaining medication that they could not otherwise afford, Ms. Ross said. This was based on an unmet need for patients living and struggling with a rare disease who didn’t have access to the care and treatment they needed. “There was no other foundation equipped to do this at the time. NORD came forward to develop the first program of its kind.”
The program provides medication, financial assistance with insurance premiums and copays, diagnostic testing assistance, and travel assistance for clinical trials or consultation with disease specialists. According to Ms. Ross, “today, NORD’s patient assistance program provides, on average, $30 million to $40 million in patient assistance annually to eligible patients and families.”
Pharmaceutical companies do contribute to the patient assistance program. “However, they’re in the dark as to how the money is allocated,” said Mr. Saltonstall. “For example, a given company might donate money for patients with a particular disease but won’t know if patients who have that disease will necessarily receive funds to use toward that company’s drug. The patient might receive assistance to take a drug made by a different company – a competitor.”
There are approximately 14 foundations around the country that have worked within the constraints of the Department of Health & Human Services Office of Inspector General, which established rules about how foundations must operate. Under the broader umbrella of NORD, these foundations also help pay coinsurance costs or provide drugs at no cost to patients who meet financial criteria.
An enduring movement
Despite the successes brought about by the ODA, the search for new rare disorder treatments is far from over. We know of more than 7,000 rare diseases; scientists discover more every year. Fewer than 5% of rare disorders have an FDA-approved treatment.
Similar to advancements made in other diseases, progress in rare disease care and treatments will continue to require an all-in approach to solve what is a looming and massive public health challenge.
As NORD founder Abbey S. Meyers wrote in her 2016 book, Orphan Drugs: A Global Crusade: “It was all of us working together that built an impregnable movement demanding a solution. In the end, with the help of government and a touch of Hollywood, the forces opposing us could not win.”
References
1. Rare Disease Day 2023 at IndoUSrare – Fireside Chat with Dr. Abbey S. Meyers. 2023 Mar 3. Indo US Organization for Rare Diseases. https://www.youtube.com/watch?v=fGTWUcQJPlU.
2. Mikami K. Soc Hist Med. 2019;32(3):609-30. doi: 10.1093/shm/hkx098.
3. National Organization for Rare Disorders. The Orphan Drug Act Turns 40: NORD Celebrates Its Impact on Rare Diseases. 2023 Jan 4. https://rarediseases.org/the-orphan-drug-act-turns-40-nord-celebrates-its-impact-on-rare-diseases. 4. Swann J. The story behind the Orphan Drug Act. US Food and Drug Administration. 2018 Feb 23. https://www.fda.gov/industry/fdas-rare-disease-day/story-behind-orphan-drug-act.
5. Roberts A-D and Wadhwa R. Orphan drug approval laws, in StatPearls (Internet). StatPearls Publishing. 2023 Jun 5. www.ncbi.nlm.nih.gov/books/NBK572052/#.
6. National Organization for Rare Disorders. Rare disease database. https://rarediseases.org/rare-diseases/.
7. National Organization for Rare Disorders. Rare disease video library. 2023 Jan 19. https://rarediseases.org/video-library/.
8. National Center for Advancing Translational Sciences. Rare disease research and resources. 2023 May 16. Accessed Sep. 17., 2023. https://ncats.nih.gov/rare-diseases.
9. Food and Drug Administration. Rare diseases team. 2023 Aug 29. https://www.fda.gov/about-fda/center-drug-evaluation-and-research-cder/rare-diseases-team.
10. National Organization for Rare Disorders. “NORD Guide to Rare Disorders,” 3rd edition. Philadelphia: Lippincott Williams & Wilkins, 2002.
11. National Organization for Rare Disorders. Cockayne syndrome. 2022 Jun 7. https://rarediseases.org/rare-diseases/cockayne-syndrome/.
12. National Organization for Rare Disorders. NORD Rare Disease Centers of Excellence. 2023 Jun 28. https://rarediseases.org/rare-disease-centers-of-excellence/.
13. National Organization for Rare Disorders. Metachromatic leukodystrophy. 2022 Mar 22. https://rarediseases.org/rare-diseases/metachromatic-leukodystrophy/#complete-report.
14. National Organization for Rare Disorders. The Natural History of Metachromatic Leukodystrophy Study. 2023 Feb 23. https://rarediseases.org/mld-home-study/.
15. The Natural History of Metachromatic Leukodystrophy Study (HOME Study). 2023 Jun 13. https://clinicaltrials.gov/study/NCT04628364?.
16. National Organization for Rare Disorders, Saltonstall PL. Letter to US Congress House Committee on Ways and Means. 2021 Sep 13. https://rarediseases.org/wp-content/uploads/2022/04/NORD_ODTC-Letter_FINAL.pdf.
17. National Organization for Rare Disorders. RareCare®: NORD’s patient assistance programs. 2022 Nov 1. https://rarediseases.org/wp-content/uploads/2022/04/NORD_ODTC-Letter_FINAL.pdf.