Erectile dysfunction (ED) is a multifactorial disease that can lead to treatment nonadherence in men taking medications for chronic health problems. Despite the importance of adhering to medication protocols for disease management, several studies demonstrated that a lack of adherence to medication protocols may be a direct response to the development of ED.
The Health Belief Model (HBM) is a conceptual framework used to better understand the relationship between health behavior and adherence in men diagnosed with hypertension. The HBM consists of 3 components that help explain health care behaviors: (1) individual perceptions; (2) modifying factors; and (3) likelihood of action. These components align with the variables in this study, which include beliefs about medicines, illness perception, and erectile function.1 Thus, the research challenge was to determine the relationship between knowledge of hypertension and sexual satisfaction among men with hypertension by using instruments in the form of 2 questionnaires: (1) the Beliefs about Medicines Questionnaire (BMQ), and (2) the International Index of Erectile Functioning (IIEF).2
Methods
A descriptive correlational design was used to explore the relationship between male patients’ antihypertensive medication beliefs and erectile function.
A convenience sample of 47 eligible men (age range 18-75 years) was recruited for this pilot study. Inclusion criteria were hypertension diagnosed by a medical professional, current use of antihypertensive medication, ability to read and write in English, and a signed informed consent. Study participants were recruited from a nurse-managed center in Detroit, Michigan, and from 6 facilities identified through Project Healthy Living 2012. The mission of the nurse-managed center is to assist low-income and underinsured populations in Wayne County, Michigan. Project Healthy Living 2012 performs free and low-cost health screenings and provides general health information to the public at various locations in the Detroit metropolitan area. Written permission to collect data was obtained from the director of Project Healthy Living 2012. Recruitment began after institutional review board approval was obtained. Participants signed an informed consent form that fully explained the nature of the study and the benefits and potential risks of participation.
Instruments
This study used the BMQ and IIEF health-related questionnaires. In addition, demographic information (eg, age, race, marital status, education, length of time with hypertension diagnosis, and current antihypertensive medications) was collected.
The BMQ was originally developed to understand patients’ commonly held beliefs about medications and the factors influencing their adherence to prescribed medication regimens.3 This questionnaire has 2 scales, BMQ Specific and BMQ General (only BMQ Specific was relevant to this study).
The BMQ Specific scale consists of two 5-item subscales, specific-necessity and specific-concern, that are designed to assess respondents’ beliefs about prescribed medications they are taking for specific conditions, such as hypertension. According to Horne and colleagues, the specific-necessity construct represents the perceived role of medication in protecting against deterioration of present and future health status.4 Statement examples include “My current health depends on my medicines,” and “My medicines protect me from becoming worse.” The specific-concern construct has an emotional component (eg, “Having to take my medicines worries me”) and a cognitive component (eg, “My medicines are a mystery to me”).
Items are scored on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Higher BMQ scores signify stronger beliefs. Studies using the BMQ subscales have shown that respondents with stronger beliefs about the necessity of their medications and fewer concerns about their medications are more likely to be adherent.
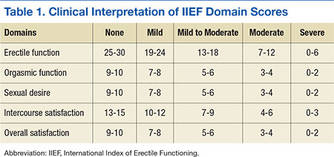
The self-administered IIEF is the instrument most widely used to assess sexual functioning and has been deployed in numerous clinical trials as the primary endpoint in evaluating the efficacy of phosphodiesterase 5-inhibitor therapy in the treatment of ED. The IIEF consists of 15 statements grouped into 5 domains assessing erectile function (6 items), orgasmic function (2 items), sexual desire (2 items), intercourse satisfaction (3 items), and overall satisfaction (2 items). Each domain is scored separately (Table 1).
Data Collection and Analysis
The researcher administered paper-and-pencil versions of the BMQ and the IIEF. Participants were allowed to complete these surveys in a semiprivate setting. No identifying information was collected—only general demographic information. IBM SPSS Version 16 statistical software was used to analyze the data.
Results
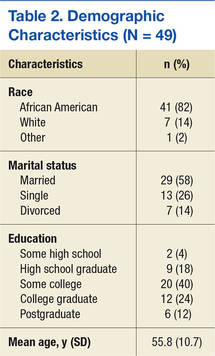
Forty-five men who were taking antihypertensive medication prescribed by a primary care provider agreed to participate. Their mean age was 55.8 years. The majority were African American (82%), married (58%) with some post-high school education (76%) (Table 2). Mean length of time with a hypertension diagnosis was 9.2 years. All respondents reported taking at least 1 antihypertensive medication. The medication most often reported being used was amlodipine, followed by lisinopril and metoprolol.