User login
According to the National Academy of Medicine (NAM), about 100 million people live with chronic pain in the U.S.1 There is evidence for the use of opioids to treat acute pain lasting 12 weeks or less. However, high-quality studies that analyze the benefit and safety of long-term opioid therapy are not yet available.2 In 2013, 249 million opioid prescriptions were written, equivalent to about 1 prescription per adult living in the U.S.3
Between 1999 and 2008, nonmedical use of prescription pain killers in the American Indian and Alaska Native populations was 2 to 3 times the frequency found in the white and black populations, respectively.1 These clinically contradictory practices created an environment conducive to opioid abuse and overdose. According to the Centers for Disease Control and Prevention, 1 in 4 people on chronic opioid therapy struggle with addiction.4 In 2014, more than 14,000 people in the U.S. died from overdoses involving prescription opioids.
The Comprehensive Addiction and Recovery Act of 2016 authorized prescription drug monitoring programs (PMPs) and a task force to create optimal pain treatment practices.5 The American Pharmacists Association (APhA), a major proponent of this law, argued that pharmacists are an underutilized resource despite having valuable clinical knowledge in the initiation, monitoring, and discontinuation of opioids. Additionally, pharmacists are able to refer patients to nonpharmacologic forms of pain management and dispense naloxone for emergent opioid overdose reversal.
Former Surgeon General Vivek Murthy developed the Turn the Tide Rx campaign to curb and reverse the opioid crisis in the U.S.3 The turnthetiderx.org website offers a pledge for clinicians who agree to be educated about pain management. It encourages open communication among prescribers and contains guideline-based resources on assessing pain and addiction risk, appropriate opioid prescribing, and how to manage opioid overdose. As required by law for prescribers in most states, there are instructions on how to access and analyze PMP opioid usage. The website also provides fact sheets about opioid treatments, safe disposal of medications, and helpline information.
Local Opioid Misuse Initiatives
New Mexico (NM) has one of the nation’s highest opioid and heroin overdose death rates.6 In January 2015, the U.S. Attorney’s Office and the University of New Mexico Health and Sciences Center partnered to launch the Heroin and Opioid Prevention and Education Initiative. The partners recognized that joint action between medical sciences and law enforcement was crucial to address the consequences of the opioid epidemic on public health and safety.
In 2017, the IHS established the National Committee on Heroin, Opioids, and Pain Efforts. Comprised of a variety of pharmacy and other subject-matter experts, this committee has a multipronged strategy to address the opioid epidemic from training to expanding medication-assisted treatment.7
Pharmacists provide clinical services in a variety of interdisciplinary ambulatory care clinics at Gallup Indian Medical Center (GIMC) in NM. The GIMC is located outside reservation boundaries but is centrally located to serve Navajo, Zuni, and a variety of other native populations. Pharmacist-run clinics include diabetes mellitus, anticoagulation, asthma, anemia, infectious diseases, and chronic pain. At GIMC, pain management pharmacists use a collective approach to curb opioid misuse. This article describes the establishment and impact of a pharmacist-led pain management clinic (PMC) at GIMC.
Pain Management Clinic
The understaffed urgent care clinic (UCC), emergency department (ED), primary care, and specialty practices plus a growing burden of complicated pain patients incentivized the development of the GIMC PMC. Under a collaborative practice agreement, pain management pharmacists were tasked with assessing, treating, and controlling noncancer chronic pain while improving quality of care and patient satisfaction (eAppendix 1, available at www.fedprac.com). The PMC goal was to improve functionality and pain scores and to reduce patient visits to the UCC and ED.
Originally, the PMC only performed medication titration for patients. In 2012, a former pharmacy resident became the PMC coordinator and has since helped to transform and expand its services. Currently, the coordinator dedicates about 20 hours per week managing pain patients in various capacities. Over time, other pain management pharmacists joined the PMC and support activities for 5 to 10 hours per week. There are now 4 pain management pharmacists who rotate through the PMC.
Pain management clinic visits generally are held once weekly for 3 hours and are occasionally expanded to full days based on patient schedule load. The initial 2 PMC appointments for each patient are 1 hour and are held within a 2-week period. Subsequent visits are each 30 minutes at 1 to 2 month intervals, depending on patient pain level and medication titration requirements. This standardized follow-up ensures new patients receive the close monitoring of slow dosage titrations necessary to achieve maximum therapeutic benefit.
Referrals
Patients only are admitted into the PMC via consults from primary care providers (PCPs). The consultations generally involve patients with complicated medical histories or who require complex therapies. The patients are contacted by telephone prior to scheduling. If a patient is not interested in PMC services, the consult is amended and the PCP is notified. This policy has been newly implemented to reduce the no-show rates. Pain management pharmacists then conduct PMC visits. The PMC activities are reported to the Pharmacy and Therapeutics committee annually. The PMC pharmacists also are available for telephone consultations from any internal hospital system department during weekday business hours.
The PMC patient population is fluid. New patients are accepted and clinically stable patients are discharged from PMC on a regular basis. The stable patients are released back to the PCP for further follow-up. Patients are considered stable if they have reached pain-related goals, are on maintenance doses of opioids, and/or are regularly participating in applicable interventional and referred therapies. If a patient requires reentry into PMC care, a new referral can be placed.
Interventional Programs
Since its inception, PMC has been a referral service to interventional programs. Physicians in the family medicine clinic provide twice weekly pain/palliative care clinic visits. These PCPs typically perform trigger point injections with lidocaine to relax muscles, which may disrupt nerve fibers. Ideally, this treatment reduces the use of opioids, non-steroidal anti-inflammatory drugs (NSAIDs), steroids, and epidural medications. Three acupuncturists were hired, which has reduced scheduling bottlenecks and wait times for patients to return for follow-up, especially in a treatment modality requiring frequent visits for effectiveness.
Pain Committee
As a part of an expansion of pain management services, GIMC established a pain committee (PC). The PC includes the GIMC medical director, PMC coordinator, pain management pharmacists, palliative care providers, PCPs, and specialty care providers. The PC created a detailed policy and procedures on management of chronic non-cancer pain for the Gallup Service Unit (eAppendix 2, available at www.fedprac.com). The PC offers guidance and completes consultations, performs internal review of prescribing patterns, and provides an appeals process for patients who have broken pain agreements. Physician and administrative champions have been instrumental to ensure proper pain management at GIMC.
Many VA facilities have deployed pain management clinics. At the VA Boston Healthcare System (VABHS), a pain management center is staffed by a multidisciplinary team that consists of anesthesiologists, neurologists, psychiatrists, nurses, and pharmacists.8 This pain clinic operates multiple days per week to accommodate demand, and patients are followed at least once a month. The VABHS often synchronized clinic visit dates with medication refill dates. Pharmacists offer an e-consult pain service to provide immediate recommendations to PCPs to bridge those patients awaiting appointments with pain clinic specialists at some VA facilities in Florida.9 Insufficient funding has prevented GIMC from increased PMC clinic hours.
Clinic Scope
Currently, the PMC sees the majority of PC cases. Pain management pharmacists are selected to conduct pain management visits based on interest and competency. Qualifications to work as a PMC pharmacist include on-the-job training, at least 6 annual pain management continuing medical education (CME) credits, participation in the NM naloxone training webinar, and completion of the physical assessment portion of the NM pharmacist clinician training course. It is highly recommended that pharmacists attend the PAINWeek conference in Las Vegas, Nevada, to obtain the necessary CME credits. In addition, pharmacists are requested to obtain the IHS National Clinical Pharmacy Specialist (NCPS) qualification within a year of practice.
Pain management pharmacists in the PMC review the indications for pain management, monitor medication therapy and adherence, adjust doses, manage adverse effects, study trends in pain and mood screening tools, and assess changes in functionality. These pharmacists are able to prescribe, discontinue, or titrate noncontrolled substance adjunctive therapies without a PCP cosignature. Adjunctive medication therapies can be NSAIDs, anticonvulsants, neuropathic pain relievers, muscle relaxers, and topical analgesics.
If adjustments to controlled substances are warranted, pain management pharmacists present the case to the PCP via electronic health record (EHR) notification or telephone conversation. These pharmacists ensure hard copies of controlled substance prescriptions are retrieved and provide refill coordination if assistance is requested by the patient. Pharmacists provide 28-day (not 30-day) prescriptions for opioid and controlled substance prescriptions to reduce weekend refill requests. Pain management pharmacists also order a variety of laboratory tests (eg, liver and renal function tests, and complete blood counts) related to the safe use of medications. If a patient is deemed unfit for PMC management, such as due to pain agreement violations, the PMC coordinator formally presents the case during PC meetings.
The PMC often recommends a multitude of nonpharmacologic treatments, including ice, hot rice socks, an anti-inflammatory diet, massage therapy, tennis ball massage for muscle tension and pinched nerves, chair exercises, transcutaneous electrical nerve stimulation therapy, aquatic therapy, and distraction therapy. Pain management pharmacists also can coordinate referrals to specialists and interventional therapies (eg, physical therapy; occupational therapy; acupuncture; trigger point injections; podiatry; orthopedics; ear, nose and throat; and diabetes mellitus).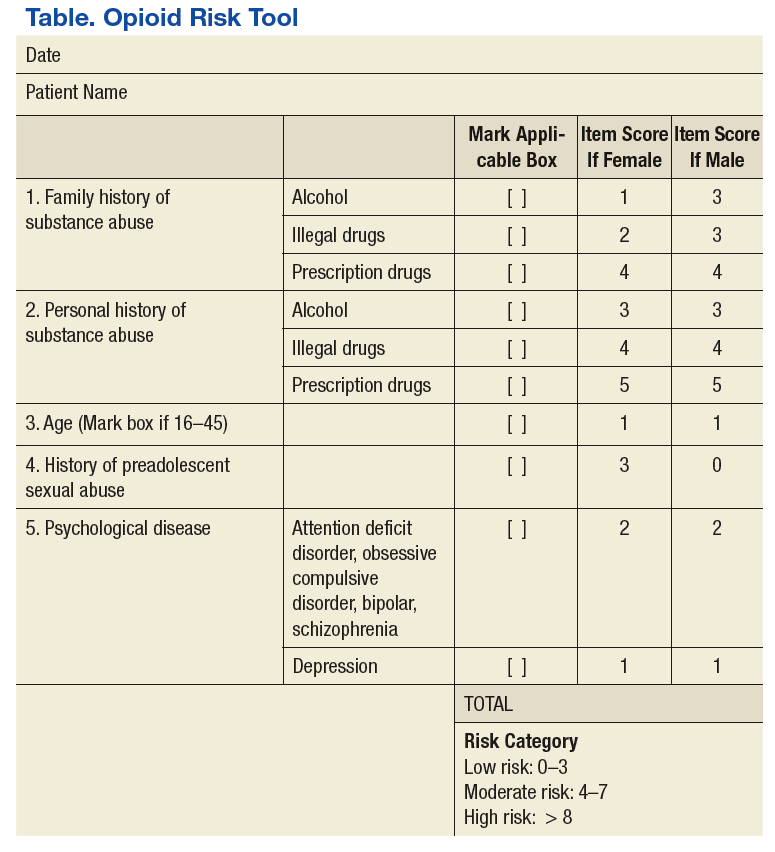
Pain management pharmacists use a variety of established tools in the pain management clinic. The PMC EHR template and interview process are consistent with the universal precautions approach to unified pain management.10 Many of the questionnaires, tools, and laboratory tests are repeated periodically based on PMC policy and patient-specific need. These tools include a controlled substance pain agreement, consent for chronic opioid therapy, Opioid Risk Tool (ORT), Current Opioid Misuse Measure (COMM) for opioid abuse risk assessment, and the Patient Health Questionnaire (PHQ-9) for concurrent depression (Table and eAppendices 1, 3, and 4, available at www.fedprac.com). The ORT recently was added to the patient assessment packet to provide a stronger assessment of opioid misuse and abuse risk. Patient goals also are discussed with an emphasis on realistic changes, the level of control that would satisfy the patient and is feasible, what activities of daily living or hobbies the patient would like to regain, and what relationships the patient would like to improve.
PMC Patients
New patients are required to complete urine drug tests (UDTs), which can be performed in house or sent out if specific drug levels are required. Federally, marijuana is an illicit substance and is not prescribed or dispensed. Unpredictable effects of traditional medicine on the UDT have been observed. If a UDT shows positive for illicit substances, a discussion with the patient on toxicity and risks is initiated allowing them to choose to continue to use other substances for pain or use only the pain medication(s) appropriately prescribed by GIMC providers. Patients can be deemed ineligible for PMC management if they do not discontinue the use of illicit substances.
Health care providers and pharmacists involved in the prescribing or dispensing of controlled substances also complete a review of the patient’s PMP profile. It is mandatory in NM to complete PMP surveillance prior to prescribing controlled substances in quantities greater than 12 units within a 72-hour period and every 3 months for refills of chronic opioids.11 The PMP Interconnect service allows registered providers in NM to search for controlled substance usage in 25 states. All but 1 state in the U.S. has a PMP in development or in place. Federal providers who do not have a NM professional license also may apply for a NM PMP login to take advantage of the PMP Interconnect service. If the patient’s PMP is negative for prescribed opioids or positive for nonprescribed substances, the providers will conduct more research to reassess the risks and benefits of ongoing opioid therapy.
Random pill counts for tracked patients also have been incorporated into the PMC policy. These pill counts can be requested regardless of clinic appointment dates and can show whether patients are taking too many pills or diverting pills. Pill counts also may show that the patient may not need as many tablets per prescription if they consistently have more than expected based on dosing frequency. If a patient has adhered to prescribing recommendations, he or she may be allowed an early refill of the chronic opioid to cover them during a vacation or other unexpected event. However, if the pill counts are not consistent with instructions, then prescribing may be restricted to a 5-day, 7-day, or 14-day supply only. If patients do not present for pill count within 24 hours of the request, they can have their opioid use privileges at GIMC revoked as consented in the pain agreement. Patients are educated on proper storage and security of opioids medication at home and funding for lock boxes is expected in the near future. Patients may be referred to other services if opioid-use disorders are identified and confirmed.
Other administrative components of the pain management pharmacist responsibilities include clinical chart reviews before appointments or telephone consultations, sending appointment letters, contacting patients about and conducting random pill counts, and documenting PMC visit notes and updating flowsheets (eAppendices 4 and 5, available at www.fedprac.com). Currently under development is an EHR function that can quickly provide a summary of a patient’s pain management without a tedious search through the chart. Pain management pharmacists regularly instruct pharmacists and providers on changes in regulatory requirements of pain management as it pertains to prescription fills or clinical indications.
Ancillary Pharmacy Services
All pain patients on opioids therapies receive an annual pain evaluation. This evaluation provides a holistic description of the patient’s pain, a second opinion, and a collective review of the safety and efficacy of treatment. Components of the pain evaluation include review of medication toxicities and adverse effects, reconciliation of the treatment with current pain diagnosis and intensity, and coordination of opioid tapering schedules. Physical assessments and pill counts also are performed. Issues that have been uncovered include incidences of opioid-induced hyperalgesia and patients filling opioids prescriptions without taking the medications because they did not want to tell the provider the medication did not work.
Naloxone overdose prevention training and dispensing has been critical for ensuring maximum safety and life-saving methods in the realm of opioid therapy. Providers, patients, and rescue buddies are trained in the indication for, the administration of, and directions after naloxone use. Patients then are provided with naloxone nasal spray after the conclusion of the training and with instruction on refill procedures. Naloxone can be administered without legal penalty by anyone in NM. When refills for naloxone are requested, a naloxone-specific refill note is filed in the EHR to collect data on naloxone usage. In collaboration with a local suicide and substance abuse prevention network, 2 pain management pharmacists have created a Pills Can Kill booklet for dispersion to patients in waiting rooms, offices, schools, and throughout the county.
MedSafe receptacles (Houston, Texas) for collection of unused or unwanted medications, including controlled substances, are available in the pharmacy. These receptacles give patients a convenient and free outlet to remove circulating opioids from general access in the community.
Clinic Impact
Previously at GIMC, clinical pain conditions were managed by providers with minimal pain management expertise. Providers in the UCC and ED treated both acute and chronic pain with minimally enforced opioid prescribing limits. Often, patients were prescribed the dangerous drug trio of opioids, benzodiazepines, and muscle relaxers. In addition, there were inconsistent PMP checks, scheduled or random UDTs, or pill counts.
Currently, providers adhere more strongly to their scope of practice, which has resulted in less erratic opioid prescribing, from initiating therapy to prescribing large quantities. Providers in the UCC and ED more often triage chronic opioid pain patients to the PCP rather than obliging patients’ requests for chronic pain medication refills. Since UCC and ED providers now focus on the treatment of acute pain, there have been fewer drug seekers frequenting those departments, which has reduced the drug-seeking burden on PCPs and the outpatient pharmacy.
Increased utilization and study of the PMP profiles at GIMC has helped uncover important information, including incidences of theft and diversion. For example, a patient or caregiver who claimed stolen opioids was discovered to be diverting opioids from patients under her care and acutely drugging her patients in order for their UDTs to appear positive for opioids. Patients have been found drug and doctor shopping under maiden and married names, under multiple birthdays, in other states, or under a different gender altogether. Some patients have been selling immense amounts of opioids and others consuming immense amounts.
Statewide statistics from the NM Board of Pharmacy from 2016 describes a 20.1% increase in PMP usage over the previous year.12 Data from 3 million prescriptions are uploaded to the PMP annually, and more than 100,000 search requests are processed monthly.11 There was a 16% decrease in opioid prescriptions per patient from multiple providers, a 14.2% decline in concurrent opioid and benzodiazepine prescriptions, and a 7.2% reduction in total opioid prescriptions.12 Fortunately, opioid overdose death rates are down 7% from the previous year.
There is an assumption of mutual trust between patient and provider. However, patients are given more responsibility for pain management through the use of a variety of objective tools and labs. Only a few people have requested refills on the naloxone kits other than for replacement of expired product. Based on experience, many patients and rescue buddies have inquired why they did not know of opioid-related risks earlier and stated that if they had naloxone available at home earlier, they could have saved a life. Further research is needed on the true impact of naloxone and its expanding access in the community.
The PMC has shown clinical success beyond simply helping to curb inappropriate opioid prescribing and overdose deaths. Investigative work such as initiating the right drug for the pain level or defining twice daily dosing as every 12 hours and not any 2 times per day has improved pain and function greatly. Many cases of hyperalgesia have been reduced by careful reductions in daily opioid doses.
Conclusion
The PMC and partners will continue to sustain efforts and transform now that the opioid crisis is exposed in the media, the IHS, and the PHS. The ongoing goals of the pain committee are to lift the dependence on opioids as long-term treatment, identify alternative solutions to pain conditions, and execute appropriate coordination of treatment. Optimization of pain management will depend on a variety of administrative and supportive service changes. Expansion of more PMC days is being considered to reduce no-show rates and the delay to first scheduled appointment. Recruitment and maintenance of specialists in behavioral health are crucial.
Securing avenues for medication-assisted therapies with buprenorphine and methadone also will help to reverse the prevalence of the opioid use disorders. The public hospital in Gallup, NM, has begun to mirror GIMC policies for consistent community actions toward improved pain management. Additionally, the GIMC experiences have been shared with area IHS facility pharmacists who are becoming increasingly involved in the national efforts to improve pain care. The pharmacy pain management clinic services at GIMC have emphasized judicious opioid prescribing, reduced overdose risk in the community, and improved patient functionality and quality of care through close pharmacotherapy monitoring.
1. The American Academy of Pain Medicine. AAPM Facts and Figures in Pain. http://www.painmed.org/patientcenter/facts_on_pain.aspx. Accessed September 18, 2017.
2. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain---United States, 2016. JAMA. 2016;315(15):1624-1645.
3. U.S. Department of Health and Human Services. The surgeon general’s call to end the opioid crisis. https://turnthetiderx.org/. Accessed September 18, 2017.
4. Centers for Disease Control and Prevention. Prescription opioid overdose data. http://www.cdc.gov/drugoverdose/data/overdose.html. Updated August 1, 2017. Accessed September 18, 2017.
5. American Pharmacists Association. United States House of Representatives approves opioid bill package. http://www.pharmacist.com/united-states-house-representatives-approves-opioid-bill-package. Published May 13, 2016. Accessed September 18, 2017.
6. U.S. Attorney’s Office, District of New MexicoHeroin and opioid prevention and education (HOPE) initiative. http://www.hopeinitiativenm.org/. Ac cessed May 6, 2017.
7. U.S. Department of Health and Human Services,National Committee on Heroin, Opioids, and Pain Efforts (HOPE). Indian Health Service Circular No. 17-04. https://www.ihs.gov/ihm/index.cfm?module=dsp_ihm_circ_main&circ=ihm_circ_1704. Published March 24, 2017. Accessed May 6, 2017.
8. Rapoport A, Akbik H. Pharmacist-managed pain clinic at a Veterans Affairs Medical Center. Am J Health Syst Pharm. 2004;61(13):1341-1343.
9. Miller DM, Harvey TL. Pharmacist pain e-consults that result in a therapy change. Fed Pract. 2015 July;32(7):14-19.
10. Zacharoff, KL, Menefee Pujol, L, Corsini, E. PainEDU.org Manual. A Pocket Guide to Pain Management. 4th ed. Newton, MA : Inflexxion, Inc; 2010.
11. New Mexico Board of Pharmacy. Prescription monitoring program. http://nmpmp.org/. Accessed May 6, 2017.
12. New Mexico Department of Health Reports on Improved Opioid Prescribing Practices, Reduced Drug Overdose Death Rates. NABP e-News. http://nabp.bmetrack.com/c/v?e=A90B1D&c=8AB9&t= 0&l=193A4F8E. Accessed January 16, 2017.
LT Patel is a clinical staff pharmacist at Gallup Indian Medical Center in New Mexico.
Acknowledgments
The author expresses her gratitude for the time, effort, and clinical expertise of Aimee Reinhard, PharmD, NCPS, the Pharmacy pain management clinic coordinator, for spearheading an excellent and growing collaborative pain management program at GIMC and for providing the majority of the insight and details seen in this publication.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
 Disclaimer
Disclaimer
The opinions expressed herein are those of the author and does not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies.
LT Patel is a clinical staff pharmacist at Gallup Indian Medical Center in New Mexico.
Acknowledgments
The author expresses her gratitude for the time, effort, and clinical expertise of Aimee Reinhard, PharmD, NCPS, the Pharmacy pain management clinic coordinator, for spearheading an excellent and growing collaborative pain management program at GIMC and for providing the majority of the insight and details seen in this publication.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and does not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies.
LT Patel is a clinical staff pharmacist at Gallup Indian Medical Center in New Mexico.
Acknowledgments
The author expresses her gratitude for the time, effort, and clinical expertise of Aimee Reinhard, PharmD, NCPS, the Pharmacy pain management clinic coordinator, for spearheading an excellent and growing collaborative pain management program at GIMC and for providing the majority of the insight and details seen in this publication.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and does not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies.
According to the National Academy of Medicine (NAM), about 100 million people live with chronic pain in the U.S.1 There is evidence for the use of opioids to treat acute pain lasting 12 weeks or less. However, high-quality studies that analyze the benefit and safety of long-term opioid therapy are not yet available.2 In 2013, 249 million opioid prescriptions were written, equivalent to about 1 prescription per adult living in the U.S.3
Between 1999 and 2008, nonmedical use of prescription pain killers in the American Indian and Alaska Native populations was 2 to 3 times the frequency found in the white and black populations, respectively.1 These clinically contradictory practices created an environment conducive to opioid abuse and overdose. According to the Centers for Disease Control and Prevention, 1 in 4 people on chronic opioid therapy struggle with addiction.4 In 2014, more than 14,000 people in the U.S. died from overdoses involving prescription opioids.
The Comprehensive Addiction and Recovery Act of 2016 authorized prescription drug monitoring programs (PMPs) and a task force to create optimal pain treatment practices.5 The American Pharmacists Association (APhA), a major proponent of this law, argued that pharmacists are an underutilized resource despite having valuable clinical knowledge in the initiation, monitoring, and discontinuation of opioids. Additionally, pharmacists are able to refer patients to nonpharmacologic forms of pain management and dispense naloxone for emergent opioid overdose reversal.
Former Surgeon General Vivek Murthy developed the Turn the Tide Rx campaign to curb and reverse the opioid crisis in the U.S.3 The turnthetiderx.org website offers a pledge for clinicians who agree to be educated about pain management. It encourages open communication among prescribers and contains guideline-based resources on assessing pain and addiction risk, appropriate opioid prescribing, and how to manage opioid overdose. As required by law for prescribers in most states, there are instructions on how to access and analyze PMP opioid usage. The website also provides fact sheets about opioid treatments, safe disposal of medications, and helpline information.
Local Opioid Misuse Initiatives
New Mexico (NM) has one of the nation’s highest opioid and heroin overdose death rates.6 In January 2015, the U.S. Attorney’s Office and the University of New Mexico Health and Sciences Center partnered to launch the Heroin and Opioid Prevention and Education Initiative. The partners recognized that joint action between medical sciences and law enforcement was crucial to address the consequences of the opioid epidemic on public health and safety.
In 2017, the IHS established the National Committee on Heroin, Opioids, and Pain Efforts. Comprised of a variety of pharmacy and other subject-matter experts, this committee has a multipronged strategy to address the opioid epidemic from training to expanding medication-assisted treatment.7
Pharmacists provide clinical services in a variety of interdisciplinary ambulatory care clinics at Gallup Indian Medical Center (GIMC) in NM. The GIMC is located outside reservation boundaries but is centrally located to serve Navajo, Zuni, and a variety of other native populations. Pharmacist-run clinics include diabetes mellitus, anticoagulation, asthma, anemia, infectious diseases, and chronic pain. At GIMC, pain management pharmacists use a collective approach to curb opioid misuse. This article describes the establishment and impact of a pharmacist-led pain management clinic (PMC) at GIMC.
Pain Management Clinic
The understaffed urgent care clinic (UCC), emergency department (ED), primary care, and specialty practices plus a growing burden of complicated pain patients incentivized the development of the GIMC PMC. Under a collaborative practice agreement, pain management pharmacists were tasked with assessing, treating, and controlling noncancer chronic pain while improving quality of care and patient satisfaction (eAppendix 1, available at www.fedprac.com). The PMC goal was to improve functionality and pain scores and to reduce patient visits to the UCC and ED.
Originally, the PMC only performed medication titration for patients. In 2012, a former pharmacy resident became the PMC coordinator and has since helped to transform and expand its services. Currently, the coordinator dedicates about 20 hours per week managing pain patients in various capacities. Over time, other pain management pharmacists joined the PMC and support activities for 5 to 10 hours per week. There are now 4 pain management pharmacists who rotate through the PMC.
Pain management clinic visits generally are held once weekly for 3 hours and are occasionally expanded to full days based on patient schedule load. The initial 2 PMC appointments for each patient are 1 hour and are held within a 2-week period. Subsequent visits are each 30 minutes at 1 to 2 month intervals, depending on patient pain level and medication titration requirements. This standardized follow-up ensures new patients receive the close monitoring of slow dosage titrations necessary to achieve maximum therapeutic benefit.
Referrals
Patients only are admitted into the PMC via consults from primary care providers (PCPs). The consultations generally involve patients with complicated medical histories or who require complex therapies. The patients are contacted by telephone prior to scheduling. If a patient is not interested in PMC services, the consult is amended and the PCP is notified. This policy has been newly implemented to reduce the no-show rates. Pain management pharmacists then conduct PMC visits. The PMC activities are reported to the Pharmacy and Therapeutics committee annually. The PMC pharmacists also are available for telephone consultations from any internal hospital system department during weekday business hours.
The PMC patient population is fluid. New patients are accepted and clinically stable patients are discharged from PMC on a regular basis. The stable patients are released back to the PCP for further follow-up. Patients are considered stable if they have reached pain-related goals, are on maintenance doses of opioids, and/or are regularly participating in applicable interventional and referred therapies. If a patient requires reentry into PMC care, a new referral can be placed.
Interventional Programs
Since its inception, PMC has been a referral service to interventional programs. Physicians in the family medicine clinic provide twice weekly pain/palliative care clinic visits. These PCPs typically perform trigger point injections with lidocaine to relax muscles, which may disrupt nerve fibers. Ideally, this treatment reduces the use of opioids, non-steroidal anti-inflammatory drugs (NSAIDs), steroids, and epidural medications. Three acupuncturists were hired, which has reduced scheduling bottlenecks and wait times for patients to return for follow-up, especially in a treatment modality requiring frequent visits for effectiveness.
Pain Committee
As a part of an expansion of pain management services, GIMC established a pain committee (PC). The PC includes the GIMC medical director, PMC coordinator, pain management pharmacists, palliative care providers, PCPs, and specialty care providers. The PC created a detailed policy and procedures on management of chronic non-cancer pain for the Gallup Service Unit (eAppendix 2, available at www.fedprac.com). The PC offers guidance and completes consultations, performs internal review of prescribing patterns, and provides an appeals process for patients who have broken pain agreements. Physician and administrative champions have been instrumental to ensure proper pain management at GIMC.
Many VA facilities have deployed pain management clinics. At the VA Boston Healthcare System (VABHS), a pain management center is staffed by a multidisciplinary team that consists of anesthesiologists, neurologists, psychiatrists, nurses, and pharmacists.8 This pain clinic operates multiple days per week to accommodate demand, and patients are followed at least once a month. The VABHS often synchronized clinic visit dates with medication refill dates. Pharmacists offer an e-consult pain service to provide immediate recommendations to PCPs to bridge those patients awaiting appointments with pain clinic specialists at some VA facilities in Florida.9 Insufficient funding has prevented GIMC from increased PMC clinic hours.
Clinic Scope
Currently, the PMC sees the majority of PC cases. Pain management pharmacists are selected to conduct pain management visits based on interest and competency. Qualifications to work as a PMC pharmacist include on-the-job training, at least 6 annual pain management continuing medical education (CME) credits, participation in the NM naloxone training webinar, and completion of the physical assessment portion of the NM pharmacist clinician training course. It is highly recommended that pharmacists attend the PAINWeek conference in Las Vegas, Nevada, to obtain the necessary CME credits. In addition, pharmacists are requested to obtain the IHS National Clinical Pharmacy Specialist (NCPS) qualification within a year of practice.
Pain management pharmacists in the PMC review the indications for pain management, monitor medication therapy and adherence, adjust doses, manage adverse effects, study trends in pain and mood screening tools, and assess changes in functionality. These pharmacists are able to prescribe, discontinue, or titrate noncontrolled substance adjunctive therapies without a PCP cosignature. Adjunctive medication therapies can be NSAIDs, anticonvulsants, neuropathic pain relievers, muscle relaxers, and topical analgesics.
If adjustments to controlled substances are warranted, pain management pharmacists present the case to the PCP via electronic health record (EHR) notification or telephone conversation. These pharmacists ensure hard copies of controlled substance prescriptions are retrieved and provide refill coordination if assistance is requested by the patient. Pharmacists provide 28-day (not 30-day) prescriptions for opioid and controlled substance prescriptions to reduce weekend refill requests. Pain management pharmacists also order a variety of laboratory tests (eg, liver and renal function tests, and complete blood counts) related to the safe use of medications. If a patient is deemed unfit for PMC management, such as due to pain agreement violations, the PMC coordinator formally presents the case during PC meetings.
The PMC often recommends a multitude of nonpharmacologic treatments, including ice, hot rice socks, an anti-inflammatory diet, massage therapy, tennis ball massage for muscle tension and pinched nerves, chair exercises, transcutaneous electrical nerve stimulation therapy, aquatic therapy, and distraction therapy. Pain management pharmacists also can coordinate referrals to specialists and interventional therapies (eg, physical therapy; occupational therapy; acupuncture; trigger point injections; podiatry; orthopedics; ear, nose and throat; and diabetes mellitus).
Pain management pharmacists use a variety of established tools in the pain management clinic. The PMC EHR template and interview process are consistent with the universal precautions approach to unified pain management.10 Many of the questionnaires, tools, and laboratory tests are repeated periodically based on PMC policy and patient-specific need. These tools include a controlled substance pain agreement, consent for chronic opioid therapy, Opioid Risk Tool (ORT), Current Opioid Misuse Measure (COMM) for opioid abuse risk assessment, and the Patient Health Questionnaire (PHQ-9) for concurrent depression (Table and eAppendices 1, 3, and 4, available at www.fedprac.com). The ORT recently was added to the patient assessment packet to provide a stronger assessment of opioid misuse and abuse risk. Patient goals also are discussed with an emphasis on realistic changes, the level of control that would satisfy the patient and is feasible, what activities of daily living or hobbies the patient would like to regain, and what relationships the patient would like to improve.
PMC Patients
New patients are required to complete urine drug tests (UDTs), which can be performed in house or sent out if specific drug levels are required. Federally, marijuana is an illicit substance and is not prescribed or dispensed. Unpredictable effects of traditional medicine on the UDT have been observed. If a UDT shows positive for illicit substances, a discussion with the patient on toxicity and risks is initiated allowing them to choose to continue to use other substances for pain or use only the pain medication(s) appropriately prescribed by GIMC providers. Patients can be deemed ineligible for PMC management if they do not discontinue the use of illicit substances.
Health care providers and pharmacists involved in the prescribing or dispensing of controlled substances also complete a review of the patient’s PMP profile. It is mandatory in NM to complete PMP surveillance prior to prescribing controlled substances in quantities greater than 12 units within a 72-hour period and every 3 months for refills of chronic opioids.11 The PMP Interconnect service allows registered providers in NM to search for controlled substance usage in 25 states. All but 1 state in the U.S. has a PMP in development or in place. Federal providers who do not have a NM professional license also may apply for a NM PMP login to take advantage of the PMP Interconnect service. If the patient’s PMP is negative for prescribed opioids or positive for nonprescribed substances, the providers will conduct more research to reassess the risks and benefits of ongoing opioid therapy.
Random pill counts for tracked patients also have been incorporated into the PMC policy. These pill counts can be requested regardless of clinic appointment dates and can show whether patients are taking too many pills or diverting pills. Pill counts also may show that the patient may not need as many tablets per prescription if they consistently have more than expected based on dosing frequency. If a patient has adhered to prescribing recommendations, he or she may be allowed an early refill of the chronic opioid to cover them during a vacation or other unexpected event. However, if the pill counts are not consistent with instructions, then prescribing may be restricted to a 5-day, 7-day, or 14-day supply only. If patients do not present for pill count within 24 hours of the request, they can have their opioid use privileges at GIMC revoked as consented in the pain agreement. Patients are educated on proper storage and security of opioids medication at home and funding for lock boxes is expected in the near future. Patients may be referred to other services if opioid-use disorders are identified and confirmed.
Other administrative components of the pain management pharmacist responsibilities include clinical chart reviews before appointments or telephone consultations, sending appointment letters, contacting patients about and conducting random pill counts, and documenting PMC visit notes and updating flowsheets (eAppendices 4 and 5, available at www.fedprac.com). Currently under development is an EHR function that can quickly provide a summary of a patient’s pain management without a tedious search through the chart. Pain management pharmacists regularly instruct pharmacists and providers on changes in regulatory requirements of pain management as it pertains to prescription fills or clinical indications.
Ancillary Pharmacy Services
All pain patients on opioids therapies receive an annual pain evaluation. This evaluation provides a holistic description of the patient’s pain, a second opinion, and a collective review of the safety and efficacy of treatment. Components of the pain evaluation include review of medication toxicities and adverse effects, reconciliation of the treatment with current pain diagnosis and intensity, and coordination of opioid tapering schedules. Physical assessments and pill counts also are performed. Issues that have been uncovered include incidences of opioid-induced hyperalgesia and patients filling opioids prescriptions without taking the medications because they did not want to tell the provider the medication did not work.
Naloxone overdose prevention training and dispensing has been critical for ensuring maximum safety and life-saving methods in the realm of opioid therapy. Providers, patients, and rescue buddies are trained in the indication for, the administration of, and directions after naloxone use. Patients then are provided with naloxone nasal spray after the conclusion of the training and with instruction on refill procedures. Naloxone can be administered without legal penalty by anyone in NM. When refills for naloxone are requested, a naloxone-specific refill note is filed in the EHR to collect data on naloxone usage. In collaboration with a local suicide and substance abuse prevention network, 2 pain management pharmacists have created a Pills Can Kill booklet for dispersion to patients in waiting rooms, offices, schools, and throughout the county.
MedSafe receptacles (Houston, Texas) for collection of unused or unwanted medications, including controlled substances, are available in the pharmacy. These receptacles give patients a convenient and free outlet to remove circulating opioids from general access in the community.
Clinic Impact
Previously at GIMC, clinical pain conditions were managed by providers with minimal pain management expertise. Providers in the UCC and ED treated both acute and chronic pain with minimally enforced opioid prescribing limits. Often, patients were prescribed the dangerous drug trio of opioids, benzodiazepines, and muscle relaxers. In addition, there were inconsistent PMP checks, scheduled or random UDTs, or pill counts.
Currently, providers adhere more strongly to their scope of practice, which has resulted in less erratic opioid prescribing, from initiating therapy to prescribing large quantities. Providers in the UCC and ED more often triage chronic opioid pain patients to the PCP rather than obliging patients’ requests for chronic pain medication refills. Since UCC and ED providers now focus on the treatment of acute pain, there have been fewer drug seekers frequenting those departments, which has reduced the drug-seeking burden on PCPs and the outpatient pharmacy.
Increased utilization and study of the PMP profiles at GIMC has helped uncover important information, including incidences of theft and diversion. For example, a patient or caregiver who claimed stolen opioids was discovered to be diverting opioids from patients under her care and acutely drugging her patients in order for their UDTs to appear positive for opioids. Patients have been found drug and doctor shopping under maiden and married names, under multiple birthdays, in other states, or under a different gender altogether. Some patients have been selling immense amounts of opioids and others consuming immense amounts.
Statewide statistics from the NM Board of Pharmacy from 2016 describes a 20.1% increase in PMP usage over the previous year.12 Data from 3 million prescriptions are uploaded to the PMP annually, and more than 100,000 search requests are processed monthly.11 There was a 16% decrease in opioid prescriptions per patient from multiple providers, a 14.2% decline in concurrent opioid and benzodiazepine prescriptions, and a 7.2% reduction in total opioid prescriptions.12 Fortunately, opioid overdose death rates are down 7% from the previous year.
There is an assumption of mutual trust between patient and provider. However, patients are given more responsibility for pain management through the use of a variety of objective tools and labs. Only a few people have requested refills on the naloxone kits other than for replacement of expired product. Based on experience, many patients and rescue buddies have inquired why they did not know of opioid-related risks earlier and stated that if they had naloxone available at home earlier, they could have saved a life. Further research is needed on the true impact of naloxone and its expanding access in the community.
The PMC has shown clinical success beyond simply helping to curb inappropriate opioid prescribing and overdose deaths. Investigative work such as initiating the right drug for the pain level or defining twice daily dosing as every 12 hours and not any 2 times per day has improved pain and function greatly. Many cases of hyperalgesia have been reduced by careful reductions in daily opioid doses.
Conclusion
The PMC and partners will continue to sustain efforts and transform now that the opioid crisis is exposed in the media, the IHS, and the PHS. The ongoing goals of the pain committee are to lift the dependence on opioids as long-term treatment, identify alternative solutions to pain conditions, and execute appropriate coordination of treatment. Optimization of pain management will depend on a variety of administrative and supportive service changes. Expansion of more PMC days is being considered to reduce no-show rates and the delay to first scheduled appointment. Recruitment and maintenance of specialists in behavioral health are crucial.
Securing avenues for medication-assisted therapies with buprenorphine and methadone also will help to reverse the prevalence of the opioid use disorders. The public hospital in Gallup, NM, has begun to mirror GIMC policies for consistent community actions toward improved pain management. Additionally, the GIMC experiences have been shared with area IHS facility pharmacists who are becoming increasingly involved in the national efforts to improve pain care. The pharmacy pain management clinic services at GIMC have emphasized judicious opioid prescribing, reduced overdose risk in the community, and improved patient functionality and quality of care through close pharmacotherapy monitoring.
According to the National Academy of Medicine (NAM), about 100 million people live with chronic pain in the U.S.1 There is evidence for the use of opioids to treat acute pain lasting 12 weeks or less. However, high-quality studies that analyze the benefit and safety of long-term opioid therapy are not yet available.2 In 2013, 249 million opioid prescriptions were written, equivalent to about 1 prescription per adult living in the U.S.3
Between 1999 and 2008, nonmedical use of prescription pain killers in the American Indian and Alaska Native populations was 2 to 3 times the frequency found in the white and black populations, respectively.1 These clinically contradictory practices created an environment conducive to opioid abuse and overdose. According to the Centers for Disease Control and Prevention, 1 in 4 people on chronic opioid therapy struggle with addiction.4 In 2014, more than 14,000 people in the U.S. died from overdoses involving prescription opioids.
The Comprehensive Addiction and Recovery Act of 2016 authorized prescription drug monitoring programs (PMPs) and a task force to create optimal pain treatment practices.5 The American Pharmacists Association (APhA), a major proponent of this law, argued that pharmacists are an underutilized resource despite having valuable clinical knowledge in the initiation, monitoring, and discontinuation of opioids. Additionally, pharmacists are able to refer patients to nonpharmacologic forms of pain management and dispense naloxone for emergent opioid overdose reversal.
Former Surgeon General Vivek Murthy developed the Turn the Tide Rx campaign to curb and reverse the opioid crisis in the U.S.3 The turnthetiderx.org website offers a pledge for clinicians who agree to be educated about pain management. It encourages open communication among prescribers and contains guideline-based resources on assessing pain and addiction risk, appropriate opioid prescribing, and how to manage opioid overdose. As required by law for prescribers in most states, there are instructions on how to access and analyze PMP opioid usage. The website also provides fact sheets about opioid treatments, safe disposal of medications, and helpline information.
Local Opioid Misuse Initiatives
New Mexico (NM) has one of the nation’s highest opioid and heroin overdose death rates.6 In January 2015, the U.S. Attorney’s Office and the University of New Mexico Health and Sciences Center partnered to launch the Heroin and Opioid Prevention and Education Initiative. The partners recognized that joint action between medical sciences and law enforcement was crucial to address the consequences of the opioid epidemic on public health and safety.
In 2017, the IHS established the National Committee on Heroin, Opioids, and Pain Efforts. Comprised of a variety of pharmacy and other subject-matter experts, this committee has a multipronged strategy to address the opioid epidemic from training to expanding medication-assisted treatment.7
Pharmacists provide clinical services in a variety of interdisciplinary ambulatory care clinics at Gallup Indian Medical Center (GIMC) in NM. The GIMC is located outside reservation boundaries but is centrally located to serve Navajo, Zuni, and a variety of other native populations. Pharmacist-run clinics include diabetes mellitus, anticoagulation, asthma, anemia, infectious diseases, and chronic pain. At GIMC, pain management pharmacists use a collective approach to curb opioid misuse. This article describes the establishment and impact of a pharmacist-led pain management clinic (PMC) at GIMC.
Pain Management Clinic
The understaffed urgent care clinic (UCC), emergency department (ED), primary care, and specialty practices plus a growing burden of complicated pain patients incentivized the development of the GIMC PMC. Under a collaborative practice agreement, pain management pharmacists were tasked with assessing, treating, and controlling noncancer chronic pain while improving quality of care and patient satisfaction (eAppendix 1, available at www.fedprac.com). The PMC goal was to improve functionality and pain scores and to reduce patient visits to the UCC and ED.
Originally, the PMC only performed medication titration for patients. In 2012, a former pharmacy resident became the PMC coordinator and has since helped to transform and expand its services. Currently, the coordinator dedicates about 20 hours per week managing pain patients in various capacities. Over time, other pain management pharmacists joined the PMC and support activities for 5 to 10 hours per week. There are now 4 pain management pharmacists who rotate through the PMC.
Pain management clinic visits generally are held once weekly for 3 hours and are occasionally expanded to full days based on patient schedule load. The initial 2 PMC appointments for each patient are 1 hour and are held within a 2-week period. Subsequent visits are each 30 minutes at 1 to 2 month intervals, depending on patient pain level and medication titration requirements. This standardized follow-up ensures new patients receive the close monitoring of slow dosage titrations necessary to achieve maximum therapeutic benefit.
Referrals
Patients only are admitted into the PMC via consults from primary care providers (PCPs). The consultations generally involve patients with complicated medical histories or who require complex therapies. The patients are contacted by telephone prior to scheduling. If a patient is not interested in PMC services, the consult is amended and the PCP is notified. This policy has been newly implemented to reduce the no-show rates. Pain management pharmacists then conduct PMC visits. The PMC activities are reported to the Pharmacy and Therapeutics committee annually. The PMC pharmacists also are available for telephone consultations from any internal hospital system department during weekday business hours.
The PMC patient population is fluid. New patients are accepted and clinically stable patients are discharged from PMC on a regular basis. The stable patients are released back to the PCP for further follow-up. Patients are considered stable if they have reached pain-related goals, are on maintenance doses of opioids, and/or are regularly participating in applicable interventional and referred therapies. If a patient requires reentry into PMC care, a new referral can be placed.
Interventional Programs
Since its inception, PMC has been a referral service to interventional programs. Physicians in the family medicine clinic provide twice weekly pain/palliative care clinic visits. These PCPs typically perform trigger point injections with lidocaine to relax muscles, which may disrupt nerve fibers. Ideally, this treatment reduces the use of opioids, non-steroidal anti-inflammatory drugs (NSAIDs), steroids, and epidural medications. Three acupuncturists were hired, which has reduced scheduling bottlenecks and wait times for patients to return for follow-up, especially in a treatment modality requiring frequent visits for effectiveness.
Pain Committee
As a part of an expansion of pain management services, GIMC established a pain committee (PC). The PC includes the GIMC medical director, PMC coordinator, pain management pharmacists, palliative care providers, PCPs, and specialty care providers. The PC created a detailed policy and procedures on management of chronic non-cancer pain for the Gallup Service Unit (eAppendix 2, available at www.fedprac.com). The PC offers guidance and completes consultations, performs internal review of prescribing patterns, and provides an appeals process for patients who have broken pain agreements. Physician and administrative champions have been instrumental to ensure proper pain management at GIMC.
Many VA facilities have deployed pain management clinics. At the VA Boston Healthcare System (VABHS), a pain management center is staffed by a multidisciplinary team that consists of anesthesiologists, neurologists, psychiatrists, nurses, and pharmacists.8 This pain clinic operates multiple days per week to accommodate demand, and patients are followed at least once a month. The VABHS often synchronized clinic visit dates with medication refill dates. Pharmacists offer an e-consult pain service to provide immediate recommendations to PCPs to bridge those patients awaiting appointments with pain clinic specialists at some VA facilities in Florida.9 Insufficient funding has prevented GIMC from increased PMC clinic hours.
Clinic Scope
Currently, the PMC sees the majority of PC cases. Pain management pharmacists are selected to conduct pain management visits based on interest and competency. Qualifications to work as a PMC pharmacist include on-the-job training, at least 6 annual pain management continuing medical education (CME) credits, participation in the NM naloxone training webinar, and completion of the physical assessment portion of the NM pharmacist clinician training course. It is highly recommended that pharmacists attend the PAINWeek conference in Las Vegas, Nevada, to obtain the necessary CME credits. In addition, pharmacists are requested to obtain the IHS National Clinical Pharmacy Specialist (NCPS) qualification within a year of practice.
Pain management pharmacists in the PMC review the indications for pain management, monitor medication therapy and adherence, adjust doses, manage adverse effects, study trends in pain and mood screening tools, and assess changes in functionality. These pharmacists are able to prescribe, discontinue, or titrate noncontrolled substance adjunctive therapies without a PCP cosignature. Adjunctive medication therapies can be NSAIDs, anticonvulsants, neuropathic pain relievers, muscle relaxers, and topical analgesics.
If adjustments to controlled substances are warranted, pain management pharmacists present the case to the PCP via electronic health record (EHR) notification or telephone conversation. These pharmacists ensure hard copies of controlled substance prescriptions are retrieved and provide refill coordination if assistance is requested by the patient. Pharmacists provide 28-day (not 30-day) prescriptions for opioid and controlled substance prescriptions to reduce weekend refill requests. Pain management pharmacists also order a variety of laboratory tests (eg, liver and renal function tests, and complete blood counts) related to the safe use of medications. If a patient is deemed unfit for PMC management, such as due to pain agreement violations, the PMC coordinator formally presents the case during PC meetings.
The PMC often recommends a multitude of nonpharmacologic treatments, including ice, hot rice socks, an anti-inflammatory diet, massage therapy, tennis ball massage for muscle tension and pinched nerves, chair exercises, transcutaneous electrical nerve stimulation therapy, aquatic therapy, and distraction therapy. Pain management pharmacists also can coordinate referrals to specialists and interventional therapies (eg, physical therapy; occupational therapy; acupuncture; trigger point injections; podiatry; orthopedics; ear, nose and throat; and diabetes mellitus).
Pain management pharmacists use a variety of established tools in the pain management clinic. The PMC EHR template and interview process are consistent with the universal precautions approach to unified pain management.10 Many of the questionnaires, tools, and laboratory tests are repeated periodically based on PMC policy and patient-specific need. These tools include a controlled substance pain agreement, consent for chronic opioid therapy, Opioid Risk Tool (ORT), Current Opioid Misuse Measure (COMM) for opioid abuse risk assessment, and the Patient Health Questionnaire (PHQ-9) for concurrent depression (Table and eAppendices 1, 3, and 4, available at www.fedprac.com). The ORT recently was added to the patient assessment packet to provide a stronger assessment of opioid misuse and abuse risk. Patient goals also are discussed with an emphasis on realistic changes, the level of control that would satisfy the patient and is feasible, what activities of daily living or hobbies the patient would like to regain, and what relationships the patient would like to improve.
PMC Patients
New patients are required to complete urine drug tests (UDTs), which can be performed in house or sent out if specific drug levels are required. Federally, marijuana is an illicit substance and is not prescribed or dispensed. Unpredictable effects of traditional medicine on the UDT have been observed. If a UDT shows positive for illicit substances, a discussion with the patient on toxicity and risks is initiated allowing them to choose to continue to use other substances for pain or use only the pain medication(s) appropriately prescribed by GIMC providers. Patients can be deemed ineligible for PMC management if they do not discontinue the use of illicit substances.
Health care providers and pharmacists involved in the prescribing or dispensing of controlled substances also complete a review of the patient’s PMP profile. It is mandatory in NM to complete PMP surveillance prior to prescribing controlled substances in quantities greater than 12 units within a 72-hour period and every 3 months for refills of chronic opioids.11 The PMP Interconnect service allows registered providers in NM to search for controlled substance usage in 25 states. All but 1 state in the U.S. has a PMP in development or in place. Federal providers who do not have a NM professional license also may apply for a NM PMP login to take advantage of the PMP Interconnect service. If the patient’s PMP is negative for prescribed opioids or positive for nonprescribed substances, the providers will conduct more research to reassess the risks and benefits of ongoing opioid therapy.
Random pill counts for tracked patients also have been incorporated into the PMC policy. These pill counts can be requested regardless of clinic appointment dates and can show whether patients are taking too many pills or diverting pills. Pill counts also may show that the patient may not need as many tablets per prescription if they consistently have more than expected based on dosing frequency. If a patient has adhered to prescribing recommendations, he or she may be allowed an early refill of the chronic opioid to cover them during a vacation or other unexpected event. However, if the pill counts are not consistent with instructions, then prescribing may be restricted to a 5-day, 7-day, or 14-day supply only. If patients do not present for pill count within 24 hours of the request, they can have their opioid use privileges at GIMC revoked as consented in the pain agreement. Patients are educated on proper storage and security of opioids medication at home and funding for lock boxes is expected in the near future. Patients may be referred to other services if opioid-use disorders are identified and confirmed.
Other administrative components of the pain management pharmacist responsibilities include clinical chart reviews before appointments or telephone consultations, sending appointment letters, contacting patients about and conducting random pill counts, and documenting PMC visit notes and updating flowsheets (eAppendices 4 and 5, available at www.fedprac.com). Currently under development is an EHR function that can quickly provide a summary of a patient’s pain management without a tedious search through the chart. Pain management pharmacists regularly instruct pharmacists and providers on changes in regulatory requirements of pain management as it pertains to prescription fills or clinical indications.
Ancillary Pharmacy Services
All pain patients on opioids therapies receive an annual pain evaluation. This evaluation provides a holistic description of the patient’s pain, a second opinion, and a collective review of the safety and efficacy of treatment. Components of the pain evaluation include review of medication toxicities and adverse effects, reconciliation of the treatment with current pain diagnosis and intensity, and coordination of opioid tapering schedules. Physical assessments and pill counts also are performed. Issues that have been uncovered include incidences of opioid-induced hyperalgesia and patients filling opioids prescriptions without taking the medications because they did not want to tell the provider the medication did not work.
Naloxone overdose prevention training and dispensing has been critical for ensuring maximum safety and life-saving methods in the realm of opioid therapy. Providers, patients, and rescue buddies are trained in the indication for, the administration of, and directions after naloxone use. Patients then are provided with naloxone nasal spray after the conclusion of the training and with instruction on refill procedures. Naloxone can be administered without legal penalty by anyone in NM. When refills for naloxone are requested, a naloxone-specific refill note is filed in the EHR to collect data on naloxone usage. In collaboration with a local suicide and substance abuse prevention network, 2 pain management pharmacists have created a Pills Can Kill booklet for dispersion to patients in waiting rooms, offices, schools, and throughout the county.
MedSafe receptacles (Houston, Texas) for collection of unused or unwanted medications, including controlled substances, are available in the pharmacy. These receptacles give patients a convenient and free outlet to remove circulating opioids from general access in the community.
Clinic Impact
Previously at GIMC, clinical pain conditions were managed by providers with minimal pain management expertise. Providers in the UCC and ED treated both acute and chronic pain with minimally enforced opioid prescribing limits. Often, patients were prescribed the dangerous drug trio of opioids, benzodiazepines, and muscle relaxers. In addition, there were inconsistent PMP checks, scheduled or random UDTs, or pill counts.
Currently, providers adhere more strongly to their scope of practice, which has resulted in less erratic opioid prescribing, from initiating therapy to prescribing large quantities. Providers in the UCC and ED more often triage chronic opioid pain patients to the PCP rather than obliging patients’ requests for chronic pain medication refills. Since UCC and ED providers now focus on the treatment of acute pain, there have been fewer drug seekers frequenting those departments, which has reduced the drug-seeking burden on PCPs and the outpatient pharmacy.
Increased utilization and study of the PMP profiles at GIMC has helped uncover important information, including incidences of theft and diversion. For example, a patient or caregiver who claimed stolen opioids was discovered to be diverting opioids from patients under her care and acutely drugging her patients in order for their UDTs to appear positive for opioids. Patients have been found drug and doctor shopping under maiden and married names, under multiple birthdays, in other states, or under a different gender altogether. Some patients have been selling immense amounts of opioids and others consuming immense amounts.
Statewide statistics from the NM Board of Pharmacy from 2016 describes a 20.1% increase in PMP usage over the previous year.12 Data from 3 million prescriptions are uploaded to the PMP annually, and more than 100,000 search requests are processed monthly.11 There was a 16% decrease in opioid prescriptions per patient from multiple providers, a 14.2% decline in concurrent opioid and benzodiazepine prescriptions, and a 7.2% reduction in total opioid prescriptions.12 Fortunately, opioid overdose death rates are down 7% from the previous year.
There is an assumption of mutual trust between patient and provider. However, patients are given more responsibility for pain management through the use of a variety of objective tools and labs. Only a few people have requested refills on the naloxone kits other than for replacement of expired product. Based on experience, many patients and rescue buddies have inquired why they did not know of opioid-related risks earlier and stated that if they had naloxone available at home earlier, they could have saved a life. Further research is needed on the true impact of naloxone and its expanding access in the community.
The PMC has shown clinical success beyond simply helping to curb inappropriate opioid prescribing and overdose deaths. Investigative work such as initiating the right drug for the pain level or defining twice daily dosing as every 12 hours and not any 2 times per day has improved pain and function greatly. Many cases of hyperalgesia have been reduced by careful reductions in daily opioid doses.
Conclusion
The PMC and partners will continue to sustain efforts and transform now that the opioid crisis is exposed in the media, the IHS, and the PHS. The ongoing goals of the pain committee are to lift the dependence on opioids as long-term treatment, identify alternative solutions to pain conditions, and execute appropriate coordination of treatment. Optimization of pain management will depend on a variety of administrative and supportive service changes. Expansion of more PMC days is being considered to reduce no-show rates and the delay to first scheduled appointment. Recruitment and maintenance of specialists in behavioral health are crucial.
Securing avenues for medication-assisted therapies with buprenorphine and methadone also will help to reverse the prevalence of the opioid use disorders. The public hospital in Gallup, NM, has begun to mirror GIMC policies for consistent community actions toward improved pain management. Additionally, the GIMC experiences have been shared with area IHS facility pharmacists who are becoming increasingly involved in the national efforts to improve pain care. The pharmacy pain management clinic services at GIMC have emphasized judicious opioid prescribing, reduced overdose risk in the community, and improved patient functionality and quality of care through close pharmacotherapy monitoring.
1. The American Academy of Pain Medicine. AAPM Facts and Figures in Pain. http://www.painmed.org/patientcenter/facts_on_pain.aspx. Accessed September 18, 2017.
2. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain---United States, 2016. JAMA. 2016;315(15):1624-1645.
3. U.S. Department of Health and Human Services. The surgeon general’s call to end the opioid crisis. https://turnthetiderx.org/. Accessed September 18, 2017.
4. Centers for Disease Control and Prevention. Prescription opioid overdose data. http://www.cdc.gov/drugoverdose/data/overdose.html. Updated August 1, 2017. Accessed September 18, 2017.
5. American Pharmacists Association. United States House of Representatives approves opioid bill package. http://www.pharmacist.com/united-states-house-representatives-approves-opioid-bill-package. Published May 13, 2016. Accessed September 18, 2017.
6. U.S. Attorney’s Office, District of New MexicoHeroin and opioid prevention and education (HOPE) initiative. http://www.hopeinitiativenm.org/. Ac cessed May 6, 2017.
7. U.S. Department of Health and Human Services,National Committee on Heroin, Opioids, and Pain Efforts (HOPE). Indian Health Service Circular No. 17-04. https://www.ihs.gov/ihm/index.cfm?module=dsp_ihm_circ_main&circ=ihm_circ_1704. Published March 24, 2017. Accessed May 6, 2017.
8. Rapoport A, Akbik H. Pharmacist-managed pain clinic at a Veterans Affairs Medical Center. Am J Health Syst Pharm. 2004;61(13):1341-1343.
9. Miller DM, Harvey TL. Pharmacist pain e-consults that result in a therapy change. Fed Pract. 2015 July;32(7):14-19.
10. Zacharoff, KL, Menefee Pujol, L, Corsini, E. PainEDU.org Manual. A Pocket Guide to Pain Management. 4th ed. Newton, MA : Inflexxion, Inc; 2010.
11. New Mexico Board of Pharmacy. Prescription monitoring program. http://nmpmp.org/. Accessed May 6, 2017.
12. New Mexico Department of Health Reports on Improved Opioid Prescribing Practices, Reduced Drug Overdose Death Rates. NABP e-News. http://nabp.bmetrack.com/c/v?e=A90B1D&c=8AB9&t= 0&l=193A4F8E. Accessed January 16, 2017.
1. The American Academy of Pain Medicine. AAPM Facts and Figures in Pain. http://www.painmed.org/patientcenter/facts_on_pain.aspx. Accessed September 18, 2017.
2. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain---United States, 2016. JAMA. 2016;315(15):1624-1645.
3. U.S. Department of Health and Human Services. The surgeon general’s call to end the opioid crisis. https://turnthetiderx.org/. Accessed September 18, 2017.
4. Centers for Disease Control and Prevention. Prescription opioid overdose data. http://www.cdc.gov/drugoverdose/data/overdose.html. Updated August 1, 2017. Accessed September 18, 2017.
5. American Pharmacists Association. United States House of Representatives approves opioid bill package. http://www.pharmacist.com/united-states-house-representatives-approves-opioid-bill-package. Published May 13, 2016. Accessed September 18, 2017.
6. U.S. Attorney’s Office, District of New MexicoHeroin and opioid prevention and education (HOPE) initiative. http://www.hopeinitiativenm.org/. Ac cessed May 6, 2017.
7. U.S. Department of Health and Human Services,National Committee on Heroin, Opioids, and Pain Efforts (HOPE). Indian Health Service Circular No. 17-04. https://www.ihs.gov/ihm/index.cfm?module=dsp_ihm_circ_main&circ=ihm_circ_1704. Published March 24, 2017. Accessed May 6, 2017.
8. Rapoport A, Akbik H. Pharmacist-managed pain clinic at a Veterans Affairs Medical Center. Am J Health Syst Pharm. 2004;61(13):1341-1343.
9. Miller DM, Harvey TL. Pharmacist pain e-consults that result in a therapy change. Fed Pract. 2015 July;32(7):14-19.
10. Zacharoff, KL, Menefee Pujol, L, Corsini, E. PainEDU.org Manual. A Pocket Guide to Pain Management. 4th ed. Newton, MA : Inflexxion, Inc; 2010.
11. New Mexico Board of Pharmacy. Prescription monitoring program. http://nmpmp.org/. Accessed May 6, 2017.
12. New Mexico Department of Health Reports on Improved Opioid Prescribing Practices, Reduced Drug Overdose Death Rates. NABP e-News. http://nabp.bmetrack.com/c/v?e=A90B1D&c=8AB9&t= 0&l=193A4F8E. Accessed January 16, 2017.