User login
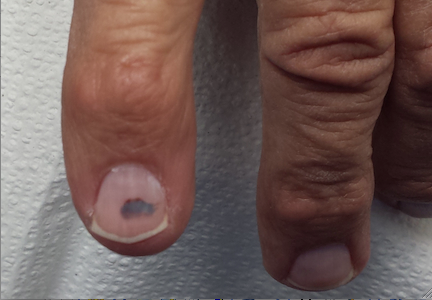
Eight months ago, this 67-year-old man first noticed a dark lesion under his second fingernail. Since then, it has not changed. It is completely asymptomatic, but it hasn’t grown out, either, which concerns the patient and his primary care provider. The latter recommends a visit to dermatology.

The patient denies any history of trauma to either the finger or the nail and says he hasn’t had any similar problems with his other fingernails. His history does include excessive sun exposure, particularly during his young adulthood. He has had several basal cell carcinomas removed over the years, mostly from his face.
EXAMINATION
The lesion in question is 4 mm, dark brown to black, and macular. It is located under the mid portion of his right index fingernail. No abnormality of the nail plate itself is felt, and all his other fingernails appear normal.
A presumptive diagnosis of subungual hematoma is challenged by the given history of at least eight months without any change or movement to the lesion. This fact is at odds with the nature of a hematoma.
Continue for the procedure and discussion >>
PROCEDURE
Since the lesion cannot simply be ignored, given the real (albeit remote) possibility of melanoma, how to proceed is thoroughly discussed with the patient. As a result, the finger is anesthetized by digital block technique, using 2% plain lidocaine. A tourniquet is then created from a small exam glove with the tip of the index finger removed. This portion of the glove is then rolled up to the base of the finger, and when the patient holds his hand above his heart, it provides a relatively bloodless field.
Then, under clean conditions, the portion of the nail plate covering the lesion is removed with iris scissors, revealing the expected subungual hematoma (characterized by clotted blood adhering to the underside of the nail plate). The nail bed now appears totally normal. After the tourniquet is released, the site is cleaned and dressed and the patient reassured as to the benignancy of the lesion.

DISCUSSION
Subungual melanoma is unusual but greatly feared because of its generally poor prognosis. This is not due to any inherent virulence but rather to delayed diagnosis. Such a delay may be caused by disbelief or denial on the part of the patient. A notable case is that of musician Bob Marley, who died in 1981 from metastatic melanoma that had started under a toenail. (Legend continues to maintain that the trauma of kicking a soccer ball caused the cancer, though this is totally anecdotal.)
Marley, who was born in Jamaica and was of mixed African and European ancestry, embodies the fact that while persons with darker skin develop melanoma far less frequently than do fair-skinned individuals, they tend to get it in locations with the least amount of pigment (eg, palms, soles, mouth, under nails). Most patients, and many unwary providers, have simply never been exposed to this very real phenomenon.
Melanoma that develops in these peripheral locations is called acral lentiginous melanoma. Hands, feet, thumbs, and halluces are the most common locations. Nearly all these melanomas begin as tan to brown macules and tend to enlarge and darken over time. They eventually transition to a vertical growth phase that allows penetration of superficial vasculature by tumor cells, leading to metastasis.
The presentation of this patient’s lesion is inconsistent with that of subungual melanoma, which usually involves the periungual margins (especially the cuticle, which eventually darkens focally, a phenomenon termed Hutchinson’s sign). In any case, whenever a subungual melanoma is suspected, a biopsy must be performed.
In all likelihood, this patient sustained trauma to this nail but forgot about it. In another two months or so, his subungual hematoma would have grown out, proving its benignancy. But in the circumstances, we had no choice but to take his given history seriously and properly evaluate the lesion.
Continue for Joe Monroe's learning points >>
TAKE-HOME LEARNING POINTS
• Acral lentiginous melanoma is associated with a generally poor prognosis, primarily due to delayed diagnosis.
• This type of melanoma is typically found on the scalp, palms, or soles, under nails, and even in the mouth. The thumb and big toe are the most common locations when hands or feet are involved.
• Patients with darker skin are far less likely to develop melanoma than their fair-skinned counterparts—but when they do, the aforementioned locations are the most common.
• For nondermatology providers, affected patients should probably be referred to dermatology for evaluation and possible biopsy.
• For any subungual or periungual lesion noted on physical examination, a history should be sought.
Eight months ago, this 67-year-old man first noticed a dark lesion under his second fingernail. Since then, it has not changed. It is completely asymptomatic, but it hasn’t grown out, either, which concerns the patient and his primary care provider. The latter recommends a visit to dermatology.
The patient denies any history of trauma to either the finger or the nail and says he hasn’t had any similar problems with his other fingernails. His history does include excessive sun exposure, particularly during his young adulthood. He has had several basal cell carcinomas removed over the years, mostly from his face.
EXAMINATION
The lesion in question is 4 mm, dark brown to black, and macular. It is located under the mid portion of his right index fingernail. No abnormality of the nail plate itself is felt, and all his other fingernails appear normal.
A presumptive diagnosis of subungual hematoma is challenged by the given history of at least eight months without any change or movement to the lesion. This fact is at odds with the nature of a hematoma.
Continue for the procedure and discussion >>
PROCEDURE
Since the lesion cannot simply be ignored, given the real (albeit remote) possibility of melanoma, how to proceed is thoroughly discussed with the patient. As a result, the finger is anesthetized by digital block technique, using 2% plain lidocaine. A tourniquet is then created from a small exam glove with the tip of the index finger removed. This portion of the glove is then rolled up to the base of the finger, and when the patient holds his hand above his heart, it provides a relatively bloodless field.
Then, under clean conditions, the portion of the nail plate covering the lesion is removed with iris scissors, revealing the expected subungual hematoma (characterized by clotted blood adhering to the underside of the nail plate). The nail bed now appears totally normal. After the tourniquet is released, the site is cleaned and dressed and the patient reassured as to the benignancy of the lesion.
DISCUSSION
Subungual melanoma is unusual but greatly feared because of its generally poor prognosis. This is not due to any inherent virulence but rather to delayed diagnosis. Such a delay may be caused by disbelief or denial on the part of the patient. A notable case is that of musician Bob Marley, who died in 1981 from metastatic melanoma that had started under a toenail. (Legend continues to maintain that the trauma of kicking a soccer ball caused the cancer, though this is totally anecdotal.)
Marley, who was born in Jamaica and was of mixed African and European ancestry, embodies the fact that while persons with darker skin develop melanoma far less frequently than do fair-skinned individuals, they tend to get it in locations with the least amount of pigment (eg, palms, soles, mouth, under nails). Most patients, and many unwary providers, have simply never been exposed to this very real phenomenon.
Melanoma that develops in these peripheral locations is called acral lentiginous melanoma. Hands, feet, thumbs, and halluces are the most common locations. Nearly all these melanomas begin as tan to brown macules and tend to enlarge and darken over time. They eventually transition to a vertical growth phase that allows penetration of superficial vasculature by tumor cells, leading to metastasis.
The presentation of this patient’s lesion is inconsistent with that of subungual melanoma, which usually involves the periungual margins (especially the cuticle, which eventually darkens focally, a phenomenon termed Hutchinson’s sign). In any case, whenever a subungual melanoma is suspected, a biopsy must be performed.
In all likelihood, this patient sustained trauma to this nail but forgot about it. In another two months or so, his subungual hematoma would have grown out, proving its benignancy. But in the circumstances, we had no choice but to take his given history seriously and properly evaluate the lesion.
Continue for Joe Monroe's learning points >>
TAKE-HOME LEARNING POINTS
• Acral lentiginous melanoma is associated with a generally poor prognosis, primarily due to delayed diagnosis.
• This type of melanoma is typically found on the scalp, palms, or soles, under nails, and even in the mouth. The thumb and big toe are the most common locations when hands or feet are involved.
• Patients with darker skin are far less likely to develop melanoma than their fair-skinned counterparts—but when they do, the aforementioned locations are the most common.
• For nondermatology providers, affected patients should probably be referred to dermatology for evaluation and possible biopsy.
• For any subungual or periungual lesion noted on physical examination, a history should be sought.
Eight months ago, this 67-year-old man first noticed a dark lesion under his second fingernail. Since then, it has not changed. It is completely asymptomatic, but it hasn’t grown out, either, which concerns the patient and his primary care provider. The latter recommends a visit to dermatology.
The patient denies any history of trauma to either the finger or the nail and says he hasn’t had any similar problems with his other fingernails. His history does include excessive sun exposure, particularly during his young adulthood. He has had several basal cell carcinomas removed over the years, mostly from his face.
EXAMINATION
The lesion in question is 4 mm, dark brown to black, and macular. It is located under the mid portion of his right index fingernail. No abnormality of the nail plate itself is felt, and all his other fingernails appear normal.
A presumptive diagnosis of subungual hematoma is challenged by the given history of at least eight months without any change or movement to the lesion. This fact is at odds with the nature of a hematoma.
Continue for the procedure and discussion >>
PROCEDURE
Since the lesion cannot simply be ignored, given the real (albeit remote) possibility of melanoma, how to proceed is thoroughly discussed with the patient. As a result, the finger is anesthetized by digital block technique, using 2% plain lidocaine. A tourniquet is then created from a small exam glove with the tip of the index finger removed. This portion of the glove is then rolled up to the base of the finger, and when the patient holds his hand above his heart, it provides a relatively bloodless field.
Then, under clean conditions, the portion of the nail plate covering the lesion is removed with iris scissors, revealing the expected subungual hematoma (characterized by clotted blood adhering to the underside of the nail plate). The nail bed now appears totally normal. After the tourniquet is released, the site is cleaned and dressed and the patient reassured as to the benignancy of the lesion.
DISCUSSION
Subungual melanoma is unusual but greatly feared because of its generally poor prognosis. This is not due to any inherent virulence but rather to delayed diagnosis. Such a delay may be caused by disbelief or denial on the part of the patient. A notable case is that of musician Bob Marley, who died in 1981 from metastatic melanoma that had started under a toenail. (Legend continues to maintain that the trauma of kicking a soccer ball caused the cancer, though this is totally anecdotal.)
Marley, who was born in Jamaica and was of mixed African and European ancestry, embodies the fact that while persons with darker skin develop melanoma far less frequently than do fair-skinned individuals, they tend to get it in locations with the least amount of pigment (eg, palms, soles, mouth, under nails). Most patients, and many unwary providers, have simply never been exposed to this very real phenomenon.
Melanoma that develops in these peripheral locations is called acral lentiginous melanoma. Hands, feet, thumbs, and halluces are the most common locations. Nearly all these melanomas begin as tan to brown macules and tend to enlarge and darken over time. They eventually transition to a vertical growth phase that allows penetration of superficial vasculature by tumor cells, leading to metastasis.
The presentation of this patient’s lesion is inconsistent with that of subungual melanoma, which usually involves the periungual margins (especially the cuticle, which eventually darkens focally, a phenomenon termed Hutchinson’s sign). In any case, whenever a subungual melanoma is suspected, a biopsy must be performed.
In all likelihood, this patient sustained trauma to this nail but forgot about it. In another two months or so, his subungual hematoma would have grown out, proving its benignancy. But in the circumstances, we had no choice but to take his given history seriously and properly evaluate the lesion.
Continue for Joe Monroe's learning points >>
TAKE-HOME LEARNING POINTS
• Acral lentiginous melanoma is associated with a generally poor prognosis, primarily due to delayed diagnosis.
• This type of melanoma is typically found on the scalp, palms, or soles, under nails, and even in the mouth. The thumb and big toe are the most common locations when hands or feet are involved.
• Patients with darker skin are far less likely to develop melanoma than their fair-skinned counterparts—but when they do, the aforementioned locations are the most common.
• For nondermatology providers, affected patients should probably be referred to dermatology for evaluation and possible biopsy.
• For any subungual or periungual lesion noted on physical examination, a history should be sought.