Imaging
Clinically significant macular edema (CSME) was first defined by the Early Treatment Diabetic Retinopathy Study (ETDRS) as macular edema that involves the center of vision, called the fovea, and can be visualized with clinical examination of the retina. The criteria for CSME are used to identify edema that is mostly likely to cause vision loss and to guide laser treatment. 20 Today, adjunctive testing, such as optical coherence tomography (OCT) and fluorescein angiography (FA), aid in the earlier detection and diagnosis of DME. These imaging techniques are capable of detecting small amounts of macular edema that are vision-threatening but are not visible on exam. Center-involving DME is edema that involves the fovea; noncenter-involving DME is edema that does not involve the fovea but is found within the macula. Color and redfree fundus photographs, OCT, and FA are also used to guide treatment in patients with DME.
Color fundus photographs are helpful as a screening tool that identifies those patients who need to be seen by an eye care provider for a dilated fundus exam. Photographs are also helpful in documenting the changes in DME after treatment. Optical coherence tomography allows for high-resolution imaging of the retinal layers and objective measurement of the amount and location of DME. This information can be used to detect any change in DME between visits and evaluate the response to treatment. Further treatment decisions are frequently made based in part on the findings seen on OCT (Figure 2).
Fluorescein angiography is an imaging test that uses an IV dye called fluorescein to detect areas of retinal nonperfusion, edema, and neovascularization. Fluorescein is injected into a peripheral vein (frequently in the antecubital area or in the hand). Photographs are then taken
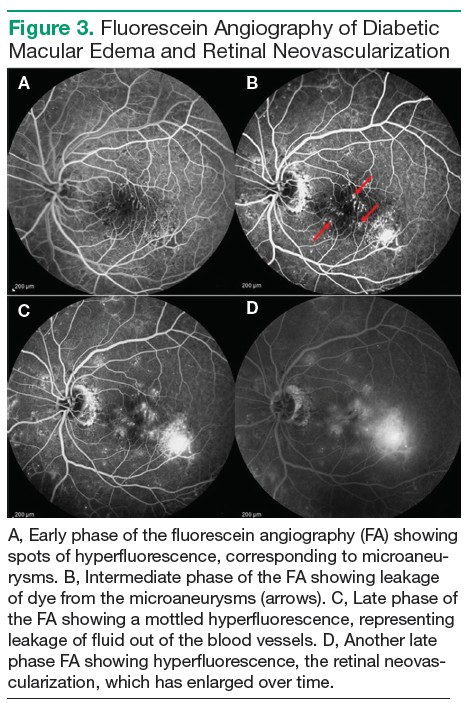
using special filters that allow only the wavelength corresponding to the fluorescein dye to be visible. The fluorescein can be seen filling the retinal arteries within 20 seconds of the peripheral injection. Photographs are usually taken intermittently for 15 minutes. As time passes, the dye will leak out of any blood vessels that have increased vascular permeability and highlight any microaneurysms, because the dye pools in the outpouching of the blood vessel. Leakage of the dye out of the vessels can be seen as an increase in fluorescence, or whitening, outside of the blood vessels in the photograph. This leakage leads to the accumulation of fluid in the retina, causing DME. Neovascularization is also very permeable, and areas of neovascularization, an indicator of proliferative diabetic retinopathy, are apparent on FA as spots of intense hyperfluorescence (Figure 3).
Treatment
In 1985, results from ETDRS revolutionized the treatment of DME. The study showed that by applying laser burns to leaking microaneurysms or in a grid pattern over an area of diffuse edema, severe vision loss could be reduced by 50%. In the past few years, the role of laser treatment has shifted so that it is now indicated for the treatment of noncenter-involving DME. The impetus for this change was the development of anti-VEGF therapy, which is now the first-line therapy for centerinvolving DME.