Dr. Dyson is a behavioral medicine postdoctoral fellow, and Dr. Cordova and Dr. Johnson-Wright are clinical psychologists, all at the VA Northern California Health Care System. Dr. Cordova is also an associate professor, and co-director of the Early Intervention Clinic, at Palo Alto University in Palo Alto, California.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those ofFederal Practitioner,Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
According to Sime, exercise therapy is the “practice of combining a program of exercise with traditional psychotherapy.”62 Sime outlined a 10-session approach to exercise therapy and suggested that walking with patients while engaging in psychotherapy can reduce barriers to change. This approach may be effective for several reasons. First, it models the recommendation to engage in activity despite not feeling well and often improves mood. Second, the experiential nature of the intervention gives the patient an immediate opportunity to physically feel the benefits of activity. Third, the experiential component is similar to experiential exercise interventions, which have been shown to improve chronic health problems, such as obesity, and it parallels in vivo exposure, which is highly effective in treating anxiety.10,63
Exposure to exercise also has been effective in treating chronic pain in patients who fear physical activity because they anticipate pain or reinjury. In patients with chronic low back pain, in vivo exposure reduced anxiety more than an education-only session did, and the result was improved participation in relevant daily activities.64 Results were sustained at the 6-month follow-up but only for patients who received in vivo exposure.65 Similarly, in vivo exposure to feared movements increased physical activity and reduced pain-related fear, catastrophizing, and disability in patients with chronic low back pain.65 These findings have implications for other chronic health problems. Particularly for patients who fear and avoid exercise, psychoeducation about exercise and opportunities to experience exercise in session may increase physical activity outside of therapy.10
Obstacles to Exercise Promotion
Mental health care providers may be reluctant to use experiential exercise interventions for a variety of reasons. Some fear that they or their patients might sustain an injury or an exacerbation of physical symptoms. In addition, some MHCPs have liability and safety concerns surrounding meetings with patients outside the office. And obtaining medical clearance requires extra time and energy.
Some MHCPs think that this type of experiential activity might cross a professional boundary. Others may wonder whether providing experiential exercise as part of mental health services is sufficiently evidence based or is a breach of standards of practice. Similarly, some MHCPs who use manual-based interventions are hesitant to stray from an evidence-based protocol and include experiential exercise in psychotherapy. Further, some MHCPs do not feel competent to provide such an intervention, given that it is not typically covered in their mental health care training, and they think that providing opportunities for experiential exercise falls outside their MHCP role. Last, some MHCPs are uncomfortable exercising on their own and thus may be particularly uncomfortable exercising in front of patients.
Promoting Physical Activity
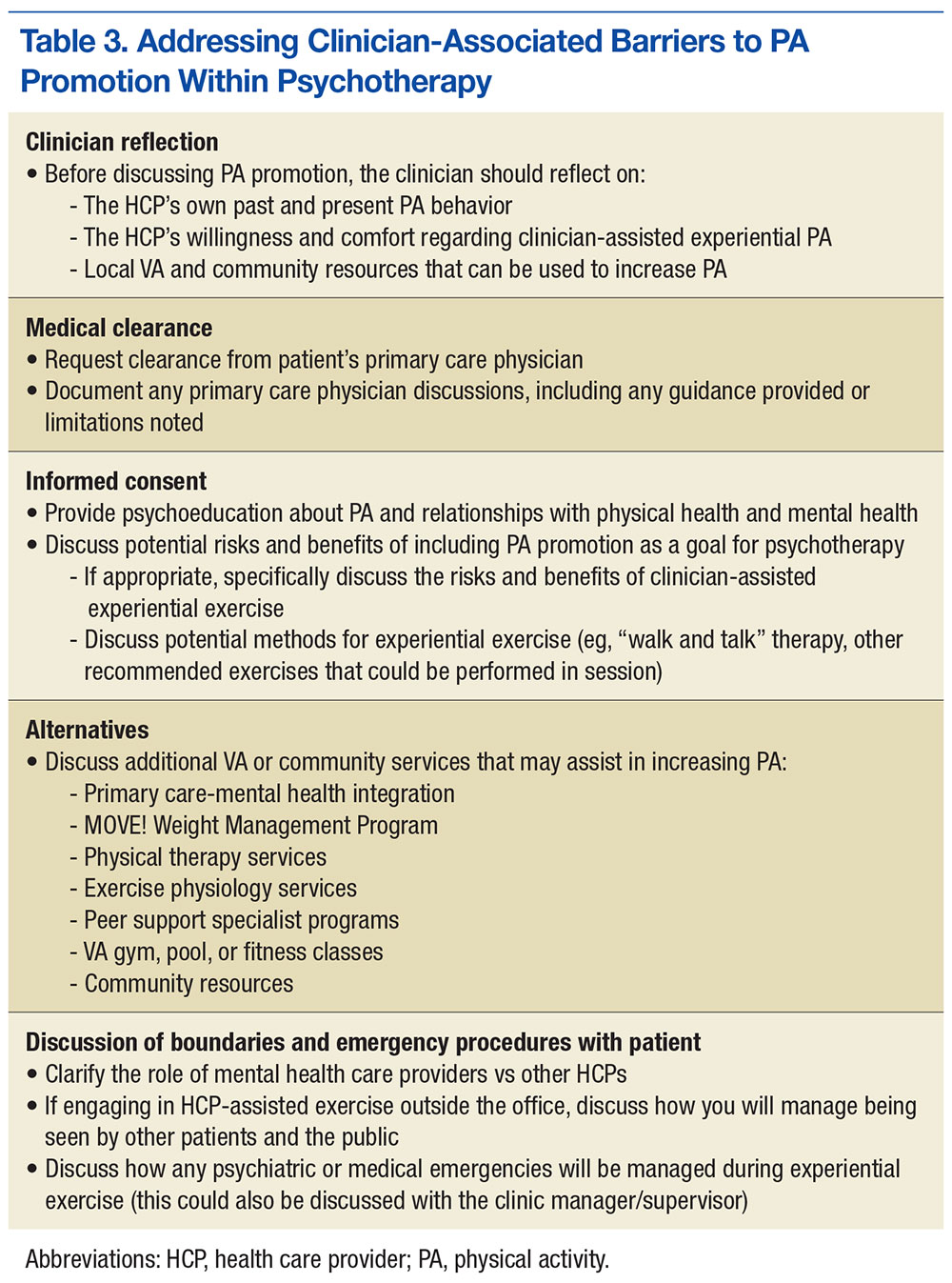
Although significant, barriers to promotion of physical activity can be effectively reduced by taking the steps outlined in Table 3. First, MHCPs must reflect on their own past and present physical activity and on their readiness to provide clinician-assisted experiential exercise. In addition, MHCPs should explore nearby alternative resources for physical activity, share their findings with patients, and encourage patients to use these resources. Next, medical clearance for increased physical activity can be obtained from patients’ primary care physicians, and any physical activity recommendations or limitations can be reviewed and documented. Mental health care providers should then obtain patients’ informed consent, which involves discussing the potential risks and benefits of increased exercise and, if appropriate, collaborate with patients to reach an agreement to focus on physical activity as an important aspect of their work together. Any additional risks and benefits of clinician-assisted experiential exercise can be discussed, and the ways in which physical activity can be used in session (eg, “walk and talk therapy”; other exercises recommended by the medical team) can be reviewed. Further, MHCPs can clarify their role and discuss how clear boundaries will be maintained within the therapeutic relationship. Alternative VA and community services that can help increase physical activity should also be discussed.
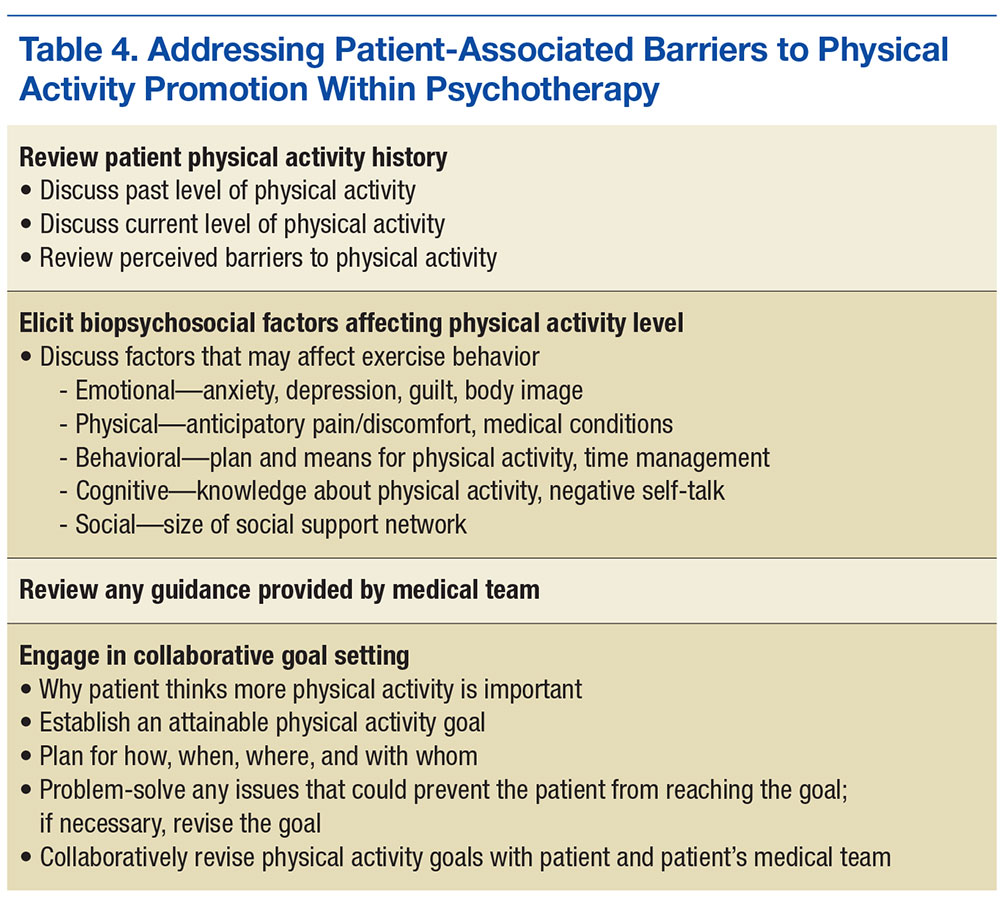
Once these steps are complete, MHCPs can address patient’s barriers to physical activity (Table 4). A discussion of the patient’s physical activity history is a good starting point. Biopsychosocial factors that can affect the ability to engage in and follow through with physical activity can then be explored, and HCPs and patients can set specific attainable physical activity goals. For instance, MHCPs can specify whether in-session clinic-assisted experiential exercise will be used and, if so, in what capacity. Last, physical activity goals can be revised periodically and revisited with the medical team.
Alternate Promotions
Mental health care providers also should consider involving other HCPs. Physical therapists and exercise physiologists are in a unique position to provide experiential exercise training. Some VA facilities include experiential exercise in their MOVE! program—veterans exercise together in the VA’s physical therapy gym while being monitored by a physical therapist.