Dr. Reed is an acute medicine clinical pharmacy specialist at the Captain James A. Lovell Federal Health Care Center in North Chicago, Illinois. Dr. Mok is a clinical pharmacy specialist at the Cheyenne VA Medical Center in Wyoming.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Patients who met the inclusion criteria were enrolled in the study. Patient’s Computerized Patient Record System charts were reviewed for demographics (sex, age, race); magnesium level; active order for PPI during same period magnesium level was drawn; PPI name, dose, and therapy duration; and concomitant use of a diuretic (yes or no) and, if yes, type of diuretic.
To assess a significance criterion (α) of 0.05 and a power of 80% 1,375 patients in a 1:4 ratio (275 cases, 1,100 controls) were required in order to detect a difference in rates of hypomagnesemia between patients who received a PPI and those who did not. Primary outcome data are reported as percentages and calculated odds ratios (ORs). Significance of ORs was determined with 95% confidence intervals (CIs). Secondary outcomes were PPI dose and therapy duration and concomitant use of a diuretic. Descriptive statistics were used for secondary outcomes.
Results
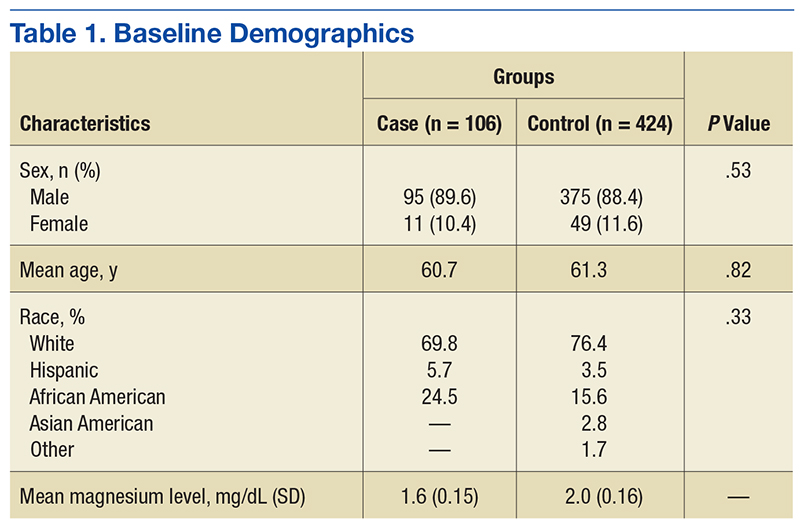
Five hundred thirty charts (106 cases, 424 controls) were included and reviewed. Table 1 lists the baseline demographics. There were no statistically significant differences in age, sex, or race between the case and control groups. Mean (SD) magnesium level was 1.6 (0.15)
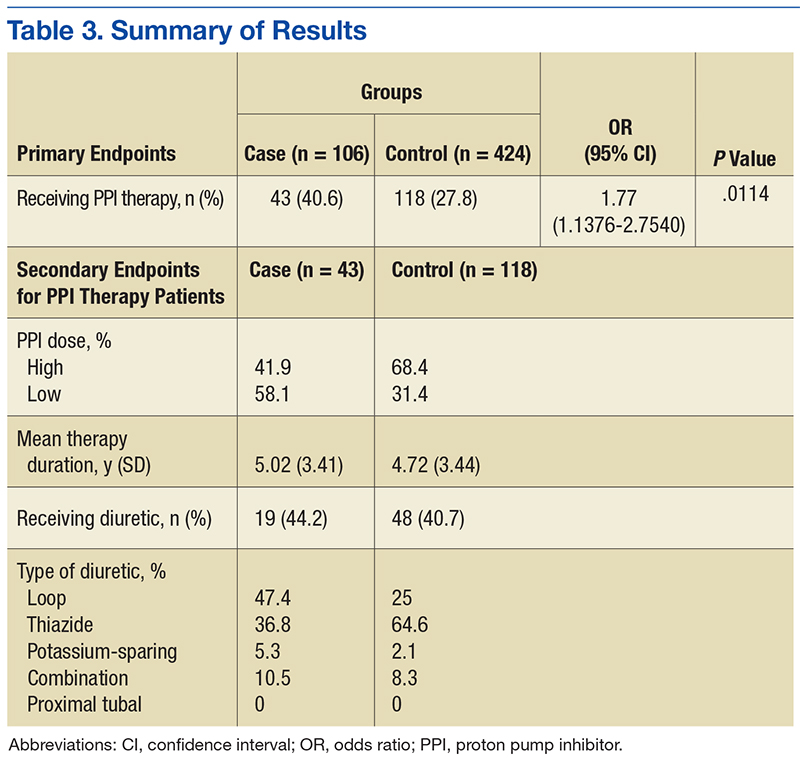
mg/dL for the case group and 2.0 (0.16) mg/dL for the control group. Forty-three (40.6%) of the 106 patients in the case group and 118 (27.8%) of the patients in the control group were concomitantly using a PPI when their magnesium level was checked (OR, 1.77; 95% CI, 1.14-2.75; P = .01). The number of patients needed to harm (NNH) was 10 (calculation based on OR).
The authors assessed for other clinical factors that might concurrently or
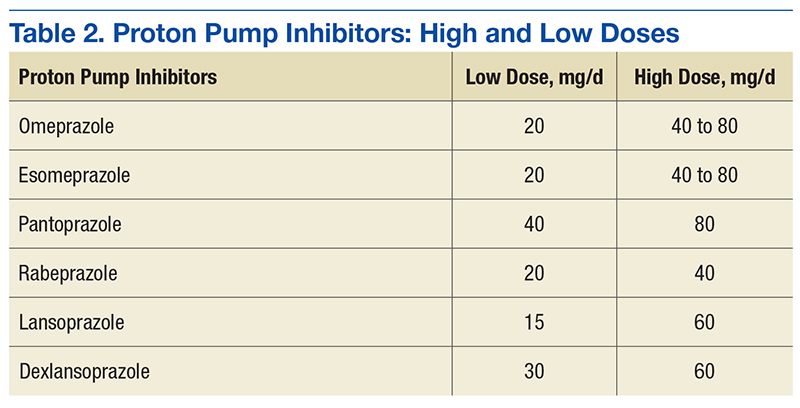
independently increase the risk for PPI-associated hypomagnesemia. High-dose PPIs were used by 41.9% of patients in the case group and 68.4% of patients in the control group. Table 2 lists the high and low therapeutic doses of specific PPI agents. Mean (SD) duration of PPI therapy was 5.02 (3.41) years for the
case group and 4.72 (3.44) years for the control group. Nineteen (44.2%) of the 43 patients in the case group and 48 (40.7%) of the 118 patients in the control group concomitantly used a diuretic. In each group, the majority of patients used loop and thiazide diuretics. Table 3 summarizes the study results.