Best Practices
The Multiple Sclerosis Centers of Excellence: A Model of Excellence in the VA
The MS Centers of Excellence at the VA improves the consistency and quality of care for veterans with MS.
The VA MS Surveillance Registry combines a traditional MS registry with individual clinical and utilization data within the largest integrated health system in the US.
Objective: To demonstrate the infrastructure and utility of an interactive health system database for multiple sclerosis (MS), we present the MS Surveillance Registry (MSSR) within the US Department of Veterans Affairs (VA).
Background: Disease specific databases can be helpful in the management of neurologic conditions but few are fully integrated into the electronic health record and linked to health system data. Creating a consistent information technology (IT) architecture and with ongoing support within disease specific registries has been a challenge.
Methods: Building the MSSR was initiated by an iterative process with an IT team and MS health care providers. A common registry platform shared by other VA disease specific registries (eg, traumatic brain injury and cancer) was used to develop the IT infrastructure. MS cases were entered online into the MS Assessment Tool at selected MS Centers of Excellence (MSCoE) clinics in the US. Other large VA databases linked to MSSR are reviewed. Patient demographic and clinical characteristics were compared and contrasted with the broader VA population and other US registry populations.
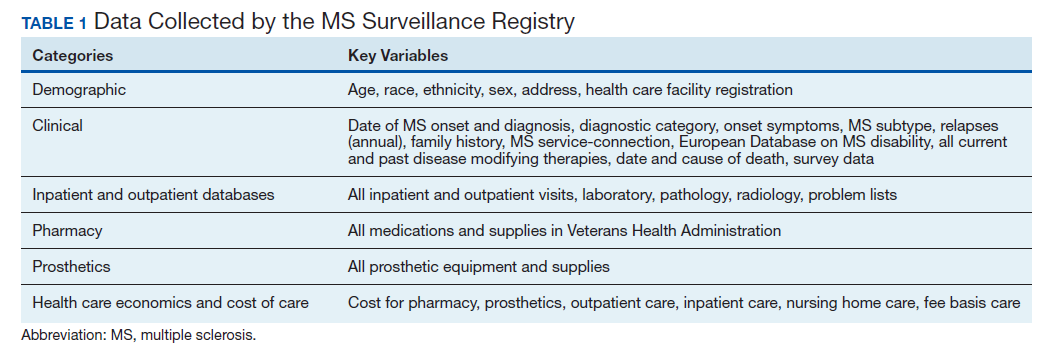
Results: We have enrolled 1,743 patients with MS in the MSSR through fiscal year 2019 from selected MS regional programs in the VA MSCoE network. The mean age of patients was 56.0 years, with a 2.7 male:female ratio. Among those with definite MS, the mean European Database for MS Disability Score was 4.7 and 75% had ever used an MS disease modifying therapy. A summary electronic dashboard was developed for health care providers to easily access demographic and clinical data for individuals and groups of patients. Data on comorbid conditions, pharmacy and prosthetics utilization, outpatient clinic visits, and inpatient admission were documented for each patient.
Conclusions: The MSSR is a unique electronic database that has enhanced clinical management of MS and serves as a national source for clinical outcomes.