Michael Buys is an Anesthesiologist, Kimberlee Bayless is a Nurse Practitioner, Jennifer Romesser is a Psychologist, Zachary Anderson and Shardool Patel are Pharmacists, all at the Salt Lake City VA Medical Center in Utah. Julie Beckstrom is a Research Nurse and Benjamin Brook is an Associate Professor, both in the Department of Surgery; Michael Buysis an Associate Professor in the Department of Anesthesiology; Chong Zhang is a Statistician, and Angela Presson is a Research Associate Professor, both in the Department of Internal Medicine and Epidemiology; all at the University of Utah in Salt Lake City. Correspondence: Michael Buys (michael.buys@hsc.utah.edu)
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
Background: For patients with existing chronic opioid use or a history of substance use disorder, often little presurgical planning or postsurgical coordination of care among surgeons, primary care providers, or addiction care providers occurs.
Methods: In 2018, we developed the Transitional Pain Service (TPS) to identify at-risk patients as soon as they were indicated for surgery, to allow time for evaluation, education, and developing an individualized pain plan, and opioid taper prior to surgery if indicated. An electronic dashboard registry of surgical episodes provided data to TPS providers and included baseline history, morphine equivalent daily dose, and patient-reported pain outcomes, using measures from the Patient-Reported Outcome Measurement System for pain intensity, pain interference, and physical function, and a pain-catastrophizing scale score.
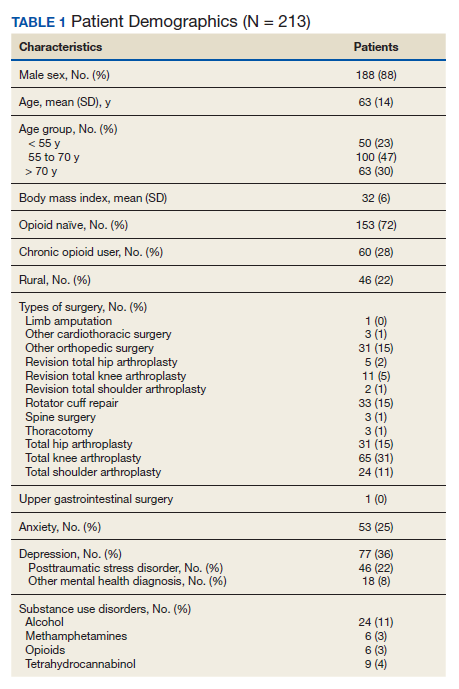
Results: Two-hundred thirteen patients were enrolled between January and December 2018. Nearly all (99%) patients had ≥ 1 successful follow-up within 14 days after discharge; 96% had ≥ 1 follow-up between 14 and 30 days after surgery; and 72% had completed personal follow-up 90 days after discharge.
Conclusions: In 2018 the overall use of opioids after orthopedic surgery decreased by > 40% from the previous year. Despite this more restricted use of opioids, pain interference and physical function scores indicated that surgical patients do not seem to experience increased pain or reduced physical function.
Despite advancements in techniques, postsurgical pain continues to be a prominent part of the patient experience. Often this experience can lead to developing chronic postsurgical pain that interferes with quality of life after the expected time to recovery.1-3 As many as 14% of patients who undergo surgery without any history of opioid use develop chronic opioid use that persists after recovery from their operation.4-8 For patients with existing chronic opioid use or a history of substance use disorder (SUD), surgeons, primary care providers, or addiction providers often do not provide sufficient presurgical planning or postsurgical coordination of care. This lack of pain care coordination can increase the risk of inadequate pain control, opioid use escalation, or SUD relapse after surgery.
Convincing arguments have been made that a perioperative surgical home can improve significantly the quality of perioperative care.9-14 This report describes our experience implementing a perioperative surgical home at the US Department of Veterans Affairs (VA) Salt Lake City VA Medical Center (SLCVAMC), focusing on pain management extending from the preoperative period until 6 months or more after surgery. This type of Transitional Pain Service (TPS) has been described previously.15-17 Our service differs from those described previously by enrolling all patients before surgery rather than select postsurgical enrollment of only patients with a history of opioid use or SUD or patients who struggle with persistent postsurgical pain.
Methods
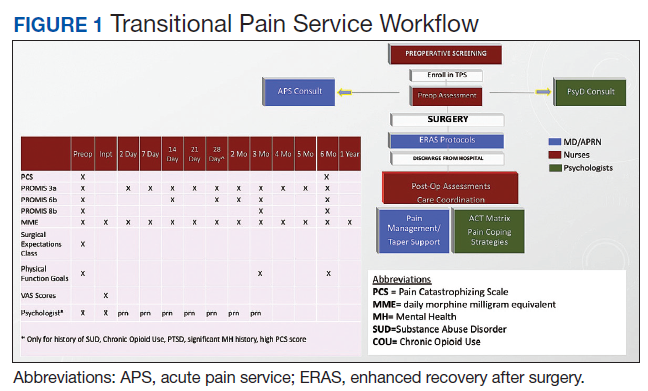
In January 2018, we developed and implemented a new TPS at the SLCVAMC. The transitional pain team consisted of an anesthesiologist with specialization in acute pain management, a nurse practitioner (NP) with experience in both acute and chronic pain management, 2 nurse care coordinators, and a psychologist (Figure 1). Before implementation, a needs assessment took place with these key stakeholders and others at SLCVAMC to identify the following specific goals of the TPS: (1) reduce pain through pharmacologic and nonpharmacologic interventions; (2) eliminate new chronic opioid use in previously nonopioid user (NOU) patients; (3) address chronic opioid use in previous chronic opioid users (COUs) by providing support for opioid taper and alternative analgesic therapies for their chronic pain conditions; and (4) improve continuity of care by close coordination with the surgical team, primary care providers (PCPs), and mental health or chronic pain providers as needed.
Once these TPS goals were defined, the Consolidated Framework for Implementation Research (CFIR) guided the implementation. CFIR is a theory-based implementation framework consisting of 5 domains: intervention characteristics, inner setting, outer setting, characteristics of individuals, and process. These domains were used to identify barriers and facilitators during the early implementation process and helped refine TPS as it was put into clinical practice.
Patient Selection
During the initial implementation of TPS, enrollment was limited to patients scheduled for elective primary or revision knee, hip, or shoulder replacement as well as rotator cuff repair surgery. But as the TPS workflow became established after iterative refinement, we expanded the program to enroll patients with established risk factors for OUD having other types of surgery (Table 1). The diagnosis of risk factors, such as history of SUD, chronic opioid use, or significant mental health disorders (ie, history of suicidal ideation or attempt, posttraumatic stress disorder, and inpatient psychiatric care) were confirmed through both in-person interviews and electronic health record (EHR) documentation. The overall goal was to identify all at-risk patients as soon as they were indicated for surgery, to allow time for evaluation, education, developing an individualized pain plan, and opioid taper prior to surgery if indicated.
Preoperative Procedures
Once identified, patients were contacted by a TPS team member and invited to attend a onetime 90-minute presurgical expectations class held at SLCVAMC. The education curriculum was developed by the whole team, and classes were taught primarily by the TPS psychologist. The class included education about expectations for postoperative pain, available analgesic therapies, opioid education, appropriate use of opioids, and the effect of psychological factors on pain. Pain coping strategies were introduced using a mindfulness-based intervention (MBI) and the Acceptance and Commitment Therapy (ACT) matrix. Classes were offered multiple times a week to help maximize convenience for patients and were separate from the anesthesia preoperative evaluation. Patients attended class only once. High-risk patients (patients with chronic opioid therapy, recent history of or current SUDs, significant comorbid mental health issues) were encouraged to attend this class one-on-one with the TPS psychologist rather than in the group setting, so individual attention to mental health and SUD issues could be addressed directly. For patients who were unable to or who chose not to attend the class, the basic education component of the class without the MBI and ACT matrix was provided by nurse care coordinators and/or the anesthesiologist/NP individually before surgery either during the anesthesia preoperative visit or in the same-day surgery unit on the day of surgery.