Linda Resnik is a Research Career Scientist at the US Department of Veterans Affairs (VA) Providence VA Medical Center (VAMC), and Professor of Health Services, Policy and Practice at Brown University in Rhode island, Matthew Borgia is a Biostatistician; and Sarah Ekerholm is a Program Manager in the Research Department, Providence VAMC. Melissa Clark is an Adjunct Professor at University of Massachusetts Medical school in Worcester and Professor of Health Services Policy and Practice, Brown University. Jason Highsmith is a National Program Director at the VA Rehabilitation and Prosthetics Services, Orthotic & Prosthetic Clinical Services in Washington, DC and is Professor at the University of South Florida, Morsani College of Medicine, School of Physical Therapy & Rehabilitation Sciences in Tampa. Billie Randolph is Deputy Director of the Extremity Trauma and Amputation Center of Excellence. Joseph Webster is a Professor in the Department of Physical Medicine and Rehabilitation, School of Medicine at Virginia Commonwealth University and aStaff Physician, Physical Medicine and Rehabilitation Hunter Holmes McGuire VAMC in Richmond. Correspondence: Linda Resnik (linda.resnik@va.gov)
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article. This work was funded by the Office of the Assistant Secretary of Defense for Health Affairs, through the Orthotics and Prosthetics Outcomes Research Program Prosthetics Outcomes Research Award (W81XWH-16- 675 2-0065) and the U.S Department of Veterans Affairs (VA RR&D, A2707-I and VA RR&D A9264A-S).
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
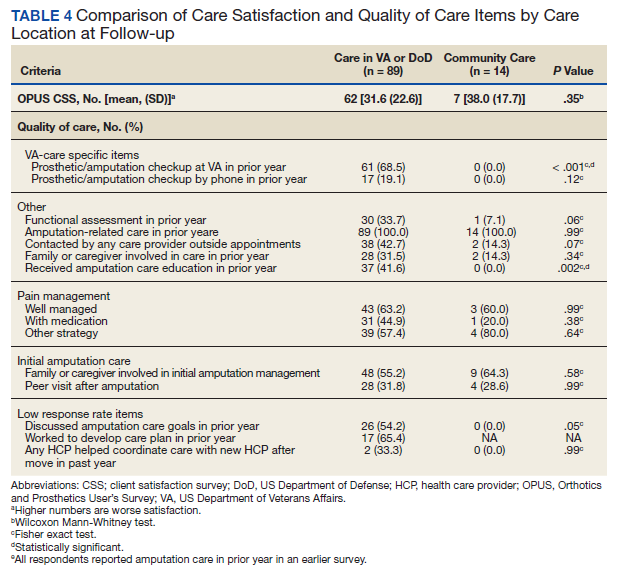
For participants who indicated that they received amputation care between baseline and follow-up, CSS mean (SD) scores were better, but not statistically different, for those who reported care in the VA or DoD vs private care, 31.6 (22.6) vs 38.0 (17.7) (Table 4). When compared with community-based care, more participants who received care in the VA or DoD in the prior year had a functional assessment in that time period (33.7% vs 7.1%, P = .06), were contacted by HCPs outside of appointments (42.7% vs 18.8%, P = .07), and received information about amputation care in the prior year (41.6% vs 0%, P =.002). There was no difference in the proportion whose family/caregivers were involved in care in the prior year.
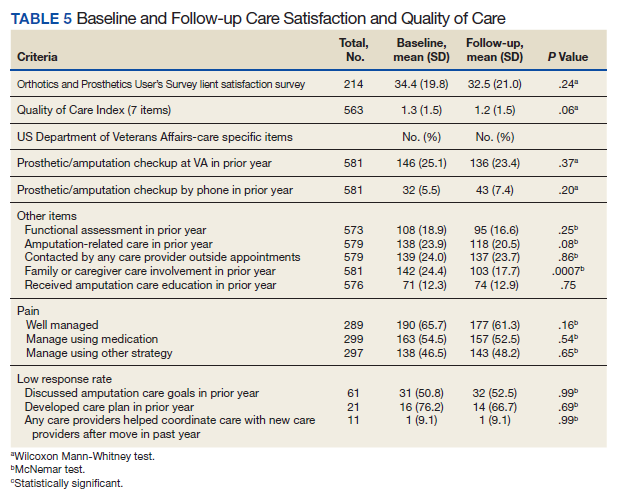
No statistically significant differences were observed in paired comparisons of the CSS and Quality of Care Index at baseline or follow-up for all participants with data at both time points (Table 5; eAppendix 3 available at doi:10.12788/fp.0096). Individual pain measures did not differ significantly between timepoints. Quality Index mean (SD) scores were 1.3 (1.5) and 1.2 (1.5) at baseline and follow-up, respectively (P = .07). For the 214 prosthesis users with longitudinal data, baseline CSS mean (SD) scores were generally worse at baseline than at follow-up: 34.4 (19.8) vs 32.5 (21.0) (P = .23). Family/caregiver involvement in amputation care was significantly higher in the year before baseline when compared with the year prior to follow-up (24.4% vs 17.7%, P = .001). There were no other statistically significant differences in Quality of Care items between baseline and follow-up.
Discussion
Our longitudinal study provides insights into the experiences of veterans with major ULA related to satisfaction with prosthetic limb care services and receipt of amputation-related care. We reported on the development and use of a new summary measure of amputation care quality, which we designed to capture some of the key elements of care quality as provided in the VA/DoD CPG.2