New Oral Anticoagulants
The new oral anticoagulants that have completed phase 3 trials for VTE prophylaxis following total joint replacement surgery include the selective Factor Xa inhibitors rivaroxaban and apixaban and the direct thrombin inhibitor dabigatran etexilate. Unlike warfarin, these agents do not require routine monitoring, a result of their predictable pharmacokinetic/pharmacodynamic (PK/PD) relationship, and they have few clinically significant drug interactions.17 Dabigatran and apixaban are not currently FDA approved for VTE prophylaxis following total joint replacement surgery; however, rivaroxaban was approved by the FDA in July 2011 for this indication.6
Apixaban
The Apixaban or Enoxaparin for Thromboprophylaxis After Knee Replacement (ADVANCE)-1 and ADVANCE-2 trials evaluated the use of Apixaban for thromboprophylaxis in patients undergoing TKR.18,19 In the ADVANCE-1 trial, patients undergoing TKR were randomized to receive either apixaban 2.5 mg orally twice daily or the North American preferred dosing of enoxaparin, 30 mg subcutaneously (SC) twice daily, with both agents started 12 to 24 hours after surgery and then taken for 10 to 14 days.18
Apixaban did not meet the prespecified statistical criteria for noninferiority compared with enoxaparin, although the rates of the primary efficacy endpoint (composite of VTE and all-cause mortality) were similar: 9.0% and 8.8% of patients, respectively. However, apixaban showed lower rates of clinically relevant bleeding and a similar adverse event (AE) profile compared with enoxaparin.
In the ADVANCE-2 trial, patients undergoing TKR received either apixaban 2.5 mg orally twice daily or enoxaparin 40 mg SC once daily for 10 to 14 days.19 The primary efficacy outcome (composite of total VTE and all-cause mortality) occurred at significantly lower rates in patients receiving apixaban (15% and 24%, respectively; relative risk [RR] 0.62; 95% confidence interval [CI] 0.51-0.74; P < .0001). Rates of major or clinically relevant nonmajor bleeding events occurred at similar rates between the 2 groups.
In the ADVANCE-3 trial, patients undergoing THR received either apixaban 2.5 orally twice daily or enoxaparin 40 mg SC once daily for 35 days.20 The primary efficacy outcome (composite of total VTE and all-cause mortality) occurred at significantly lower rates in patients receiving apixaban (1.4% and 3.9%, respectively; RR 0.36; 95% CI 0.22-0.54; P < .001). Rates of major or clinically relevant nonmajor bleeding events occurred at similar rates between both groups.
Dabigatran etexilate
Dabigatran etexilate has been evaluated in patients undergoing TKR in the Oral Dabigatran Etexilate vs Subcutaneous Enoxaparin for the Prevention of Venous Thromboembolism After Total Knee Replacement (RE-MODEL) and Oral Thrombin Inhibitor Dabigatran Etexilate vs North American Enoxaparin Regimen for Prevention of Venous Thromboembolism After Total Knee Replacement (RE-MOBILIZE) studies and in patients undergoing THR in the Oral Dabigatran vs Enoxaparin for Thromboprophylaxis After Primary Total Hip Arthroplasty (RE-NOVATE)-1 and RE-NOVATE‑2 trials.21-24
In RE-MODEL, patients undergoing TKR received either 150 mg or 220 mg of dabigatran etexilate once daily (starting with a half dose 1 to 4 hours after surgery) or enoxaparin 40 mg once daily (started the evening before surgery) for 6 to 10 days.23 Both doses of dabigatran had a similar incidence of the composite of total VTE and mortality and major bleeding. In RE-MOBILIZE, patients undergoing TKR received either 150 mg or 220 mg of dabigatran etexilate once daily or the North American regimen of enoxaparin, 30 mg SC twice daily for 12 to 15 days.24 Both dabigatran regimens had a significantly higher incidence of the composite of total VTE, failing to establish noninferiority to enoxaparin. The incidence of major bleeding was not significantly different among the 3 groups.
In RE-NOVATE I, patients undergoing THR received either dabigatran 150 mg or 220 mg twice daily, or enoxaparin 40 mg SC once daily for 28 to 35 days.21 Both doses of dabigatran had a similar incidence of the composite of total VTE and mortality and major bleeding. Because RE-NOVATE I did not include any study sites in North America, a second phase 3 trial, RE-NOVATE II, was conducted to include North American sites. RE-NOVATE II had an identical trial design to RE-NOVATE I and similar results (noninferior efficacy and comparable safety).22
Rivaroxaban
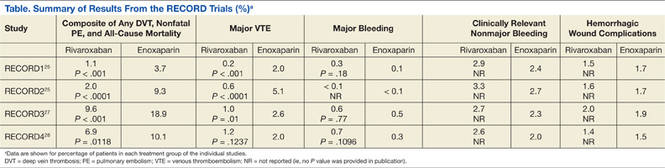
The phase 3 Rivaroxaban vs Enoxaparin for Thromboprophylaxis After Hip Arthroplasty (RECORD) program consisted of 4 double-blind randomized trials that compared the efficacy and safety of oral rivaroxaban to SC enoxaparin in THR (RECORD1 and 2) and TKR (RECORD3 and 4). The RECORD1 and 2 trials compared rivaroxaban 10 mg orally once daily for 31 to 39 days with enoxaparin 40 mg SC once daily (for 31-39 days in RECORD1 and for 10-14 days followed by placebo in RECORD2). The RECORD3 and 4 trials compared 10- to 14-day regimens of rivaroxaban 10 mg orally once daily with enoxaparin 40 mg SC once daily (RECORD3) and 30 mg twice daily (RECORD4). The 4 trials used the same efficacy and safety outcomes (Table).