Mary J. Aigner, PhD, RN, FNP-BC; and Pawan Sikka, MD
Dr. Sikka is the chief of Pulmonary, Critical Care, and Sleep Medicine, at the Central Texas Veterans Health Care System in Temple, Texas. Dr. Aigner was an advanced practice registered nurse practitioner in Pulmonary and Sleep Medicine at the Central Texas Veterans Health Care System at the time the article was written and is now retired.
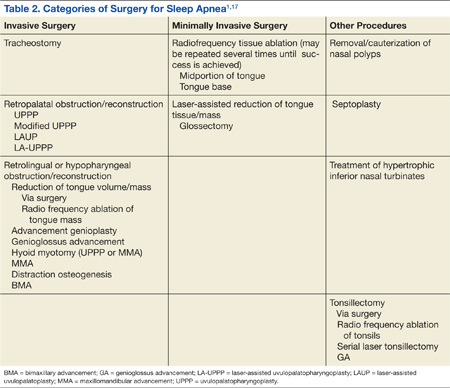
Surgery for OSA can be divided into 2 categories, invasive surgery and minimally invasive surgery (Table 2). Invasive surgeries for OSA have a higher risk of complications and postoperative pain.9
Invasive Surgery The UPPP surgery is perhaps the best-known invasive procedure for treating OSA. A meta-analysis of 15 studies on UPPP outcomes found overall improvement in AHI of 33% but with postoperative AHI remaining elevated at an average of 29.8 events per hour.13
Adverse effects for the procedure include changes in taste, dysphagia, nasal regurgitation, and voice alterations. Seven of the 15 studies reported at least 1 death following the UPPP procedure. The effects of UPPP surgery on systemic and cardiovascular sequelae of OSA are not fully known and need to be further researched. 13
Another invasive procedure that is similar to the UPPP is the laser-assisted uvulopalatoplasty (LAUP) procedure. First reported in 1990, LAUP was developed as a procedure to eliminate snoring and was found to be effective. Other studies have been conducted since then, but there are inconsistencies in the specific types of procedures performed and a lack of detailed data analysis.
Adverse effects of the LAUP procedure include minor bleeding, globus sensation, local infection, minor dysphagia and dysphonia, and transient velopharyngeal insufficiency.14 However, studies have also shown that about one-quarter of the participants developed persistent dysphagia or mild to moderate scar fibrosis. Postoperative swelling can reduce an already narrow airway, and the use of sedatives or narcotics can make this problem worse. Some studies have noted structural changes following this procedure that lower airway resistance, resulting in the collapse of the upper airway and the narrowing of the airway during inhalation with worsening OSA.13,14
Practice parameters for the LAUP procedure were developed by the AASM in 1994. The AASM recommended against using LAUP to treat OSA (and other sleep-related breathing disorders) and against substituting LAUP for UPPP surgery. The AASM also suggested criteria for choosing candidates for LAUP and urged that patients be given full information about the procedure and a preoperative evaluation from their provider.5,14
Minimally Invasive Surgery Radiofrequency surgery and soft palate implants are considered minimally invasive procedures, according to the criteria established in a study by Maurer.11 Various nasal surgeries (eg, septoplasty, adenoidectomy, and polyp removal) could also be considered minimally invasive and are often performed in patients with OSA to improve tolerance of CPAP by improving the ability to breathe nasally. However, nasal surgery with improvement of nasal breathing has not been found to have a significant impact on adults who have OSA. An advantage of nasal surgery is that some studies have shown longer use of CPAP therapy, up to 2 hours longer per night.5
With radiofrequency of the tongue base, high-frequency radio waves, either monopolar or bipolar, are used to coagulate the interstitial tissue at the base of the tongue. This, in turn, leads to necrosis and scarring, which then leads to stiffening of the tissue and in some cases, volume reduction. The surgeon controls the temperature to avoid overdosing and tissue carbonization. A number of lesions are produced during a session and the number of sessions necessary for full treatment varies per surgeon and the technical system used in procedures.
Although radiofrequency ablation (RFA) has been used on the tonsils and soft palate, RFA is currently available only to patients with OSA on the tongue base. A reduction in AHI of 33% on average was achieved in a review of 6 studies, and the reduction was stable over a 2-year period.11 The average presurgery AHI was 39.5, and the average postsurgery AHI was 28.7. In this same review, the average Epworth Sleepiness Scale (ESS) (a commonly used subjective tool to measure levels of daytime sleepiness) score was 10.4 presurgery and 4.5 postsurgery.11
A Chinese study looked at complications from RFA of the tongue base. According to the abstract (the article was written in Chinese), 1 patient (n = 193) developed a fatal arrhythmia. The authors’ recommendation was for close monitoring after surgery until the swelling subsided.15
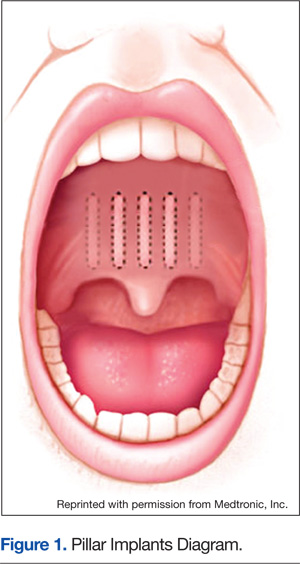
With soft palate implants, small cylinders of woven polyester (“polyethylene terephthalate, commonly marketed as Dacron polyester”) yarn, 18 mm long by 2 mm diameter, are inserted at the junction of the hard palate and soft palate. Placed into the proximal soft palate tissue, these implants are designed to stiffen the soft palate “through fibrotic tissue encapsulation and tissue ingrowth over time.” Many patients with only snoring or mild to moderate OSA have found improvement with this procedure. Improved reduction of snoring was found in 1 study (n = 79), which looked at the use of Pillar implants to reduce snoring (Figure 1). This reduction of snoring occurred in patients with lower AHI levels before the procedure.16 Mauer reviewed 3 studies of the palatal implants and found a pooled reduction of 26% in AHI after placement.11