Dr. Skolarus, Dr. Hofer, Dr. Hawley, and Dr. Sales are all investigators at the HSR&D Center for Clinical Management Research in the VA Ann Arbor Health Care System in Michigan. Dr. Montgomery, Dr. Hafez, and Dr. Skolarus are all staff urologists in the Urology Section, VA Ann Arbor Health Care System and along with Dr. Hollenbeck are members of the Department of Urology, University of Michigan. Dr. Hofer and Dr. Hawley are in the Department of Internal Medicine, University of Michigan. Dr. Shelton and Ms. Antonio are both at the VA Greater Los Angeles Healthcare System and University of California, Los Angeles. Dr. Sales is also in the Department of Systems Leadership and Effectiveness Science at the School of Nursing, University of Michigan.
Multilevel regression modeling, an extension of linear regression modeling suitable for partitioning the variation in an outcome variable attributable to different levels (ie, facility and VISN), was used to examine whether variation in the urologist workforce was primarily based at the facility or regional VISN level.6 This approach accounted for the potentially correlated nature of the data (ie, multiple facilities within each VISN) by incorporating a VISN-level random effect in the model. A random intercept model with no explanatory variables, known as an empty model, was used as the primary model.6 The intraclass correlation coefficient (ICC) corresponding to the estimated variance components from the empty model was calculated to determine the portion of the total variation in unadjusted urologist workforce that occurs between VISNs.7 Prostate cancer caseload was then included to test whether allocation seemed to be driven by clinical need or other regional factors.
All analyses were performed using STATA, Version 12 (StataCorp LP, College Station, TX), and all testing was 2-sided. The probability of a type I error was set at .05. This study protocol was approved by the VA Ann Arbor Health Care System Research and Development Committee and Institutional Review Board.
Results
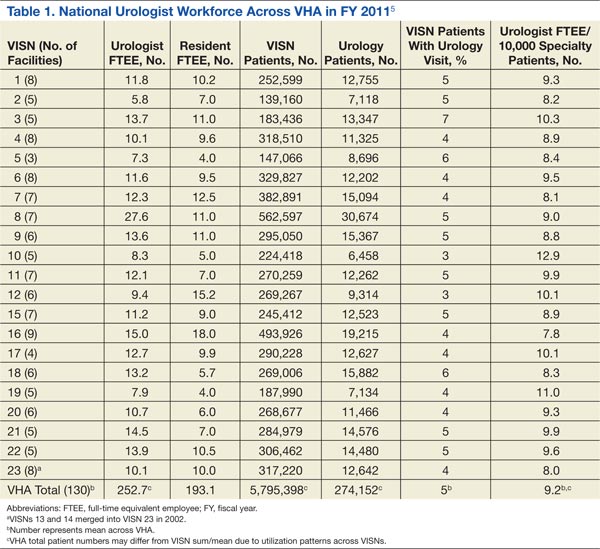
Nearly 1 in 20 VHA patients (n = 274,152) were evaluated in a urology clinic at least once in FY 2011. It was found that 252.7 FTEE and 193.1 residents comprised the VHA urologist workforce (Table 1). Marked regional variation was found in unadjusted urologist staffing at both the facility and VISN levels. The urologist workforce ranged from 0.17 to 5.91 FTEEs across the 130 VHA facilities. At the VISN level, staffing varied over 5-fold (5.8 FTEEs in VISN 2 to 27.6 FTEEs in VISN 8).
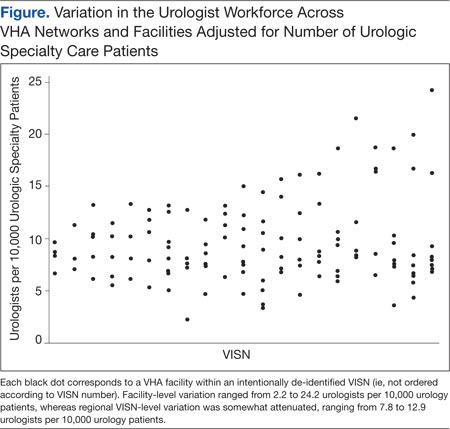
Variation in the VHA urologist workforce distribution persisted even after standardizing by patient volume. The urologist workforce continued to vary from 0.94 to 9.95 FTEEs per 100,000 facility patients. This was even more dramatic when adjusted for volume of unique urology patients, ranging from 2.2 to 24.2 FTEE urologists per 10,000 urology patients (Figure).5 From the specialist perspective, each might serve 18 to 64 newly diagnosed patients with prostate cancer annually, depending on the VISN.
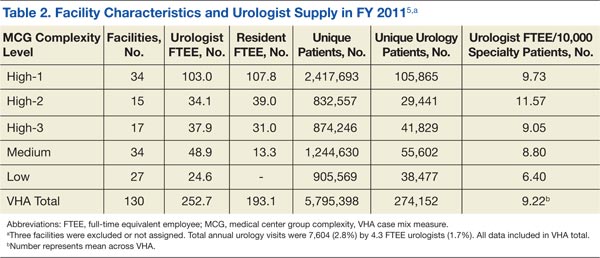
Forty percent of urologists were located in 34 of the most complex facilities (Table 2). Urology patient caseload was associated with facility complexity in univariate analysis (P < .001). In the adjusted multivariable model, increasing facility complexity was associated with increasing urologist workforce (P < .001) as well as resident staffing (P < .001), but not with urology patient caseload (P = .27). The empty multilevel model indicated that 27.3% of variation in unadjusted urologist workforce (ICC = 0.273, 95% confidence interval [CI], 0.098-0.448) was attributable to differences at the regional network level. After adjustment for VISN prostate cancer caseload, this decreased to 24.8% (ICC = 0.248; 95% CI, 0.076-0.419).
Discussion
The VHA urologist workforce served over 250,000 patients in FY 2011, and a substantial variation in workforce distribution at the facility and VISN levels was identified in this study. After adjusting for prostate cancer caseload as a proxy for clinical demand, there was some imbalance of urology specialists across regional networks, though most workforce variation occurred within networks in this integrated delivery system. Based on these findings, VHA specialty care initiatives should likely focus within regional networks rather than pursue electronic efforts nationally to improve specialty care access for patients and PCPs.
Regional variation in the VHA urologist workforce was expected, given a limited national supply of urologists and specialist preferences toward metropolitan areas.2-4 Overcoming this maldistribution has important implications for outcomes in many urologic disease processes.8-10 For example, counties with ≥ 1 urologist have up to a 20% reduction in bladder and prostate cancer-related mortality compared with those without a urologist.4 Moreover, the number of veterans with known urologic needs or currently receiving urologic specialty care likely significantly undercounts the total number who could benefit from this care. This is particularly true for facilities with fewer urology resources where patients may be less likely to get a referral, or if they are referred, it is likely outside VHA, creating fragmented care and potentially higher cost.
Understanding the urology workforce distribution, coupled with its sophisticated nationwide EMR, VHA has a unique opportunity to transform how urologic specialty care is delivered without moving around the current workforce. Based on these findings, the system could redistribute resources within each region to meet growing specialty care needs through telemedicine.
At least 2 innovative approaches are underway that might serve the system’s urology care needs: e-consults and the Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) video teleconsulting and education project.11,12 The first allows PCPs to request specialist review of the EMR, interpretation of the specific problem, and recommendation for a plan of care, which may or may not include a specialist visit.1,13 The second involves video conferences, which allow multiple PCPs from less complex facilities or rural areas to present cases to specialists from tertiary medical centers for real-time consultation and case-based learning. These initiatives could take advantage of the facility-based variation in urologist workforce by linking facilities with relatively generous urology resources with those with fewer resources to meet the needs of each region’s population and their PCPs while minimizing travel and wait times.