Yeun-Hee Anna Park is Chief of Hematology/Oncology; Alison Keller is a Research Coordinator; and Ta-Chueh Melody Hsu is a Research Nurse Practitioner, all at James J. Peters Veterans Affairs Medical Center, Bronx, New York. Balmatee Bidassie is an Industrial Engineer VA Center for Applied Systems Engineering (VA-CASE), VISN11 - Veterans Engineering Resource Center (VERC) at Richard L. Roudebush Veterans Affairs Medical Center, Indianapolis, Indiana. Vickie Venne was a Senior Genetic Counselor for the US Department of Veterans Affairs (VA) Genomic Medicine Services, and Sarah Colonna is a Hematologist/Oncologist; both at George E. Wahlen Veterans Affairs Medical Center, Salt Lake City, Utah. Douglas Hawley is a Hematologist/Oncologist at Cincinnati Veterans Affairs Medical Center, Cincinnati, Ohio. Lori Hoffman-Högg is a ONS Clinical Nurse Advisor for the Oncology Field Advisory Committee and VHA National Program Manager for Prevention Policy at Veterans Health Administration (VHA) National Center for Health Promotion and Disease Prevention, Durham, North Carolina and VHA Office of Nursing Services, Washington, DC. Bernadette Heron is a Program Manager at Veterans Health Administration, Pharmacy Benefits Management Services in Hines, Illinois. Anita Aggarwal is a Hematologist/Oncologist Washington Veterans Affairs Medical Center, Washington, DC.
Breast cancer is the most common cancer in women.52 The number of women with breast cancer in the VHA has more than tripled from 1995 to 2012.1 The lifetime risk of developing breast cancer in the general population is about 13%.50 This rate can be affected by risk factors including age, hormone exposure, family history, radiation exposure, and lifestyle factors, such as weight and alcohol use.6,52-56 In the United States, invasive breast cancer affects 1 in 8 women.50,52,57
Our screened population showed nearly 3 times as many women veterans were at an increased risk for breast cancer when compared with historical averages in US women. This difference may be based on a high rate of prior breast biopsies or positive family history, although a provocative study using the Surveillance, Epidemiology, and End Results database showed military women to have higher rates of breast cancer as well.9 Historically, Blacks are vastly understudied in clinical research with only 5% representation on a national level.5,58 The urban locations of both pilot sites (Washington, DC and Bronx, NY) allowed for the inclusion of minority patients in our study. We found that the rates of breast cancer in Black women veterans to be higher than seen nationally, possibly prompting further screening initiatives for this understudied population.
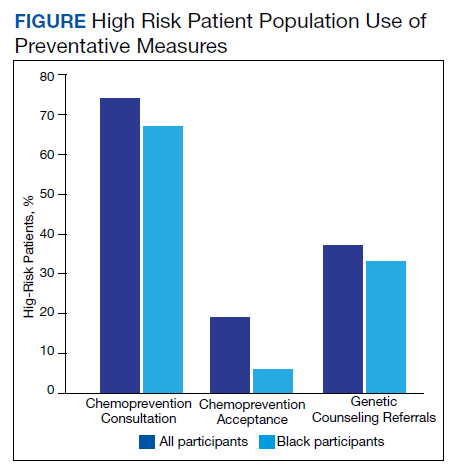
Our pilot study’s chemoprevention utilization (19%) was double the < 10% seen in the national population.33-35 The presence of a knowledgeable breast health practitioner to recruit study participants and offer personalized counseling to women veterans is a likely factor in overcoming barriers to chemopreventive acceptance. These participants may have been motivated to seek care for their high-risk status given a strong family history and prior breast biopsies.
Interestingly, a 3-fold higher PTSD rate was seen in this pilot population (29%) when compared with PTSD rates in the general female population (7-10%) and still one-third higher than the general population of women veterans (20%).45-47 Mental health, anxiety, and PTSD have been barriers to patients who sought treatment and have been implicated in poor adherence to medical advice.48,49 Cancer screening can induce anxiety in patients, and it may be amplified in patients with PTSD. It was remarkable that although adherence with screening recommendations is decreased when PTSD is present, our patient population demonstrated a higher rate of screening adherence.
Women who are seen at the VA often use multiple clinical specialties, and their EMR can be accessed across VA medical centers nationwide. Therefore, identifying women veterans who meet screening criteria is easily attainable within the VA.
When comparing high-risk with average risk women, the lifestyle results (BMI, smoking history, exercise and consumption of fruits, vegetables and alcohol) were essentially the same. Lifestyle factors were similar to national population rates and were unlikely to impact risk levels.
Limitations
Study limitations included a high number of self-referrals and the large percentage of patients with a family history of breast cancer, making them more likely to seek screening. The higher-than-average risk of breast cancer may be driven by a high rate of breast biopsies and a strong family history. Lifestyle metrics could not be accurately compared to other national assessments of lifestyle factors due to the difference in data points that we used or the format of our questions.