Apar Kishor Ganti, MD, MS Doctor and Mrs. D. Leon UNMC Research Fund Chair in Internal Medicine Staff Physician, VA Nebraska-Western Iowa Health Care System Professor of Medicine, Division of Oncology-Hematology Professor (Courtesy) of Biochemistry and Molecular Biology Associate Director of Clinical Research, Fred & Pamela Buffett Cancer Center University of Nebraska Medical Center Omaha, NE
Slideshow below.
In the United States and among veterans, lung cancer has the highest rate of cancer-related mortality. Earlier detection and increased screening of high-risk individuals can improve the overall survival rate.1 With the broadening of the USPSTF lung cancer screening guidelines, in 2020 an estimated 15 million people in the United States—including at least 900,000 veterans—were eligible for lung cancer screening by CT.2,3 However, only 5% of those eligible were screened.4,5 One reason for this vast discrepancy is uneven access. Estimates in 2021 were that <20% of eligible veterans have undergone lung cancer screening because of problems accessing it in rural areas.6
Implementing the expanded USPSTF guidelines is key to maximizing screening among underserved populations, such as those in rural areas who may lack access to nearby health care, as well as racial and ethnic minorities.1 A study of one VAMCs standardization of screening practices found that radiologists were more likely to adapt to these changes than primary care clinicians, suggesting a need to better understand differences in health care professional practices and priorities to universally improve screening rates across the VA.1
An important question will always be how many high-risk veterans are being screened for lung cancer?1 To ensure proper care, it is important to understand the characteristics of clinicians who provide screening based on setting and clinical areas of expertise. Where are they, who are they, and how do our most vulnerable populations gain access? Access is critical, particularly among clinicians who typically provide screening to those underserved populations.
Although lung cancer screening rates have increased over the years, overall, utilization remains low, even though data show a 20% reduction in lung cancer mortality with adherence to yearly CT screening.7 Looking at these rates helps us understand the need to intervene to increase lung cancer screening rates.8 Guidelines have been an essential component when it comes to outcomes related to screenings. Through programs implemented by the VHA, the goal is to improve the uptake and quality of lung cancer screening and optimize the practice and access for all veterans.9 For clinicians, future work should evaluate lung cancer screening programs with high vs low rates of adherence to identify and publicize best practices for timely, appropriate follow-up.9 Although adherence rates remain low regardless of race, further research, particularly among Black veterans, is encouraged to address delayed follow-up and to create culturally competent and inclusive lung cancer screening programs.10
1
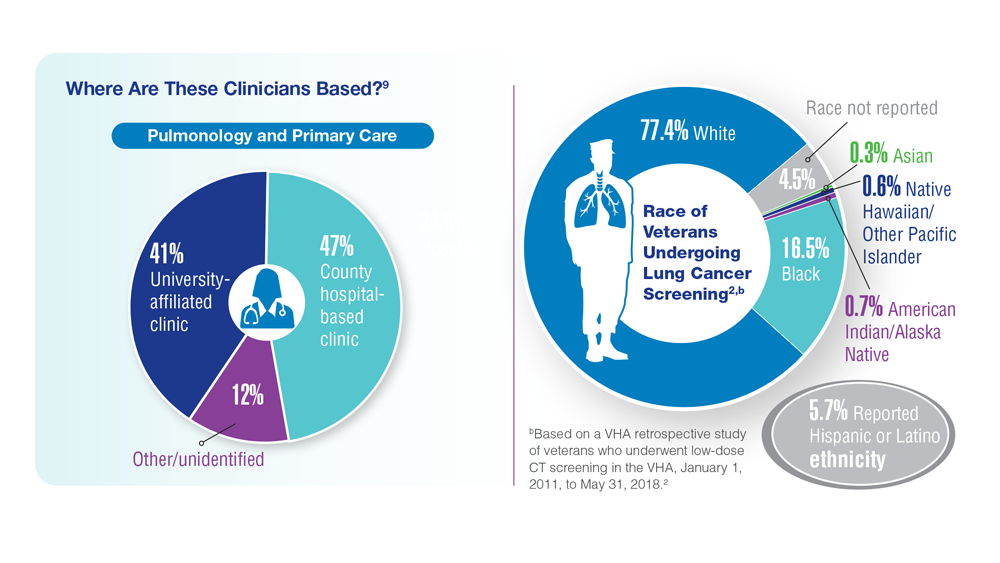
Who is getting screened for lung cancer in the VHA?9,c
75 of 130 VAMCs across all 4 regions performed initial lung cancer screenings between 2011 and 2018.2
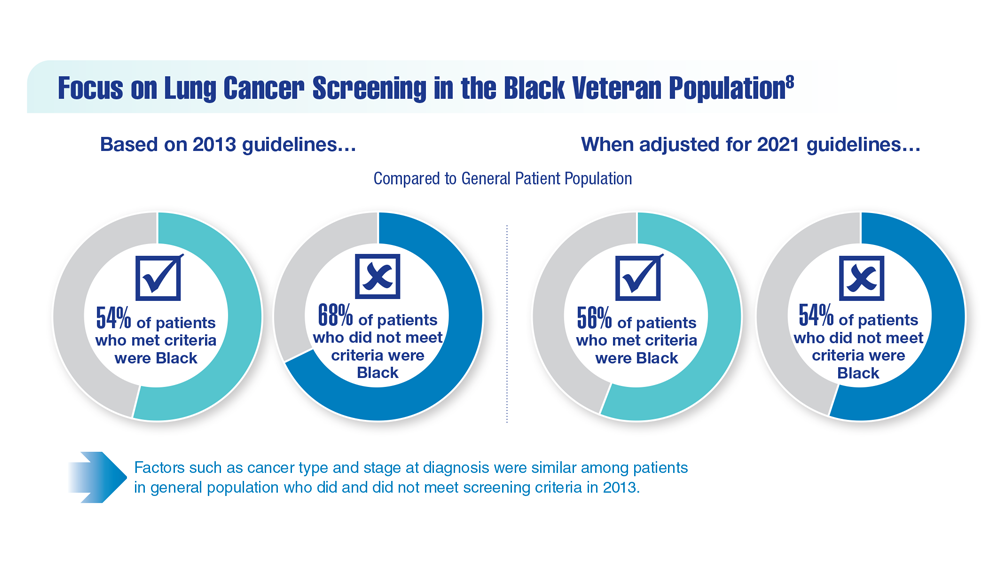
Following the 2021 USPSTF guideline updates, a retrospective review looked at the applicability of the screening guidelines within the Southeast Louisiana VHCS, which serves a predominantly Black population. It was determined that the prior (2013) criteria may have not included enough Black individuals at risk for lung cancer. These findings underscored the need for screening models to take race and ethnicity into account for more effective early-stage diagnosing, along with standardized VA lung cancer screening programs.
Differences in the presence of COPD and smoking history were more significant and may have contributed to some patients not meeting the criteria for lung cancer screening.8 COPD diagnosis and smoking history data were based on the full population of patients diagnosed with stage 1 or 2 lung cancer in the Southeast Louisiana VHCS.