Chronic esophageal symptoms attributed to gastroesophageal reflux disease (GERD) are common presenting symptoms in gastroenterology, leading to high healthcare costs and adverse quality of life globally.1,2 The clinical diagnosis of GERD hinges on the presence of “troublesome” compatible typical symptoms (heartburn, acid regurgitation) or evidence of mucosal injury on endoscopy (esophagitis, Barrett’s esophagus, peptic stricture).3 With the growing availability of proton pump inhibitors (PPIs), patients and clinicians often utilize an empiric therapeutic trial of PPI as an initial test, with symptom improvement in the absence of alarm symptoms indicating a high likelihood of GERD.4 A meta-analysis of studies that used objective measures of GERD (in this case, 24-hour pH monitoring) showed that the “PPI test” has a sensitivity of 78%, but a specificity of only 54%, as a diagnostic approach to GERD symptoms.5 Apart from noncardiac chest pain, the diagnostic yield is even lower for atypical and extra-esophageal symptoms such as cough or laryngeal symptoms.6
Dr. Amit Patel
Therefore, when symptoms persist despite seemingly adequate PPI therapy, esophageal investigation may start with endoscopy but continues with ambulatory reflux and motility testing.7 At endoscopy, exclusion of eosinophilic esophagitis with esophageal biopsies represents an important component of initial evaluation when symptoms are refractory to PPIs.8 Further, the more atypical the presentation, the greater the need for esophageal testing prior to long-term PPI therapy. Esophageal function testing is also indicated when confirmation of GERD is needed prior to surgical or endoscopic reflux procedures.
The “nuts and bolts” of reflux testing
Ambulatory reflux testing assesses esophageal reflux burden and symptom-reflux association (SRA). Individual reflux events are identified as either a drop in esophageal pH to less than 4 (acid reflux events), or a sharp decrease in esophageal impedance measurements in a retrograde fashion (impedance-detected reflux events), with subsequent recovery to the baseline in each instance. Ambulatory reflux testing affords insight into three areas: 1) measurement of esophageal acid exposure time (AET); the cumulative time duration when distal esophageal pH is less than 4 at the recording site, reported as a percentage of the recording period; 2) measurement of the number of reflux events both acidic (from pH monitoring) and weakly acidic/alkaline (from impedance monitoring); and 3) quantitative evaluation of the association between reported symptom episodes and reflux events.
Dr. C. Prakash Gyawali
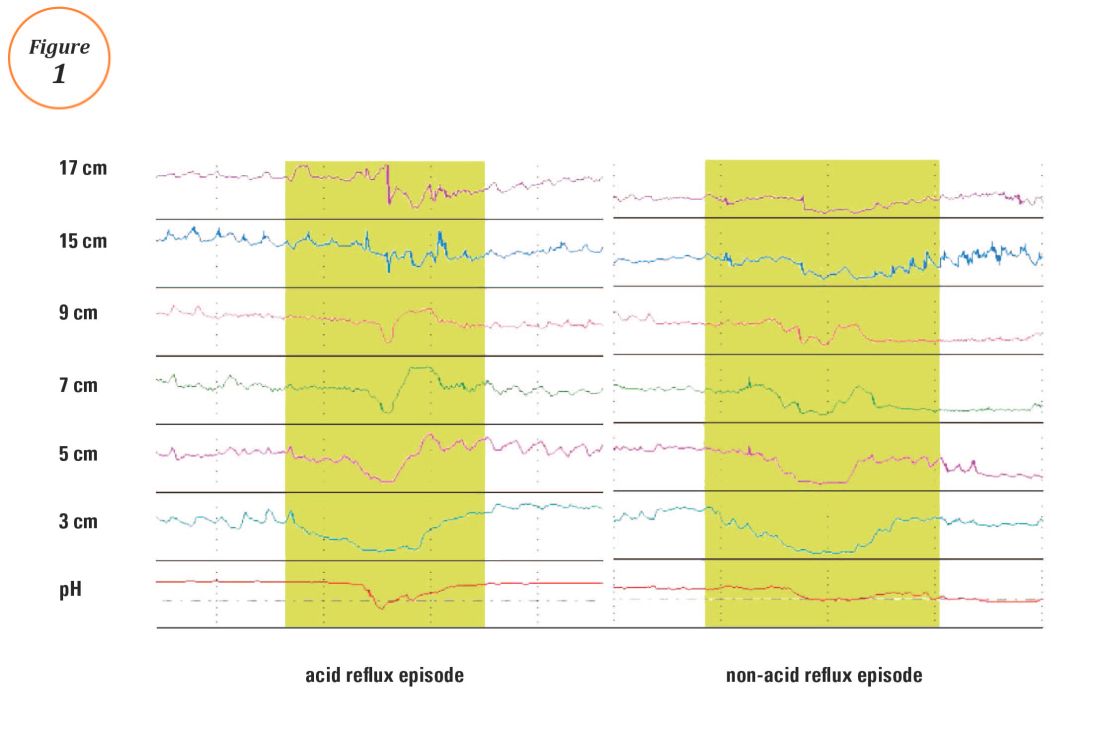
The three available modalities of ambulatory reflux monitoring consist of catheter-based pH, wireless pH, and combined catheter-based pH-impedance monitoring. Catheter-based pH monitoring, introduced in the 1970s, requires transnasal catheter placement and typically records for 24 hours before catheter removal. The catheter is positioned with the distal pH sensor 5 cm proximal to the upper margin of the manometrically identified lower esophageal sphincter (LES). New guidelines suggest AET less than 4% is reliably normal, while AET greater than 6% is pathologic; values in between are considered borderline and require alternate evidence for GERD, such as endoscopic findings.7 Wireless pH probes are placed 6 cm proximal to the squamocolumnar junction at endoscopy and communicate with a pager-sized receiver worn by the patient.9 Patient comfort is not compromised, with less restriction of typical patient activities compared to catheter-based testing, facilitating longer recording periods of 48-96 hours, which can overcome day-to-day variations in esophageal reflux burden.7 With catheter-based pH-impedance monitoring, multiple pairs of impedance sensors measure the resistance to flow of a tiny electrical current between sensors. Since resistance to flow (that is, impedance) is low in the presence of a bolus or refluxate in the esophageal lumen, the impedance tracing drops during reflux events in a retrograde fashion across the esophageal impedance sensor pairs, regardless of the acidity of the reflux (Figure 1).10 Combined pH-impedance testing thus detects refluxate in the esophagus regardless of pH, improving the sensitivity of detection of reflux events over pH testing alone, thereby promoting greater yield of SRA. However, there remains wide inter-observer variation on the designation of impedance reflux events.11
Representative Esophageal pH-Impedance Tracings of Reflux Episodes (examples of acid and non-acid reflux episodes)
The two most commonly utilized SRA metrics are the symptom index (SI) and symptom-association probability (SAP). Individual symptom episodes are designated as related to preceding reflux events if they occur within 2 minutes of the reflux events. The SI represents the simple ratio of the number of reflux-related symptoms to the total number of symptom episodes reported during the ambulatory reflux study, with values above 50% designated as positive.12 For calculation of the SAP, the ambulatory reflux study is divided into 2-minute intervals. For each interval, the presence or absence of a reflux event and a symptom episode is assessed; the final counts are tabulated on a 2 x 2 table, and a Fisher exact test is applied to generate a “P” value. The SAP is positive if P is less than 0.05, corresponding to an SAP of greater than 95%, or a less than 5% chance that the observed association between symptoms and reflux events occurred by chance.13 The SAP can also be calculated post-hoc with data typically extracted during a pH study, using statistical modeling; termed the Ghillebert Probability Estimate,14 this corresponds well with the former method of SAP calculation.15
The SI and SAP can be calculated individually for acid-detected reflux events and for impedance-detected reflux events. Since reflux events are better detected with impedance, combined pH-impedance testing increases the yield of detecting positive SRA, especially when performed off PPI therapy.16,17 Because these indices are heavily reliant on patient reporting of symptom episodes, SRA can be overinterpreted;18 positive associations are more clinically useful than negative results in the evaluation of symptoms attributed to GERD.19 Despite these concerns, the two most consistent predictors of symptomatic outcome with antireflux therapy on pH-impedance testing are abnormal AET and positive SAP with impedance-detected reflux events.17
Copyright Elsevier/AGA
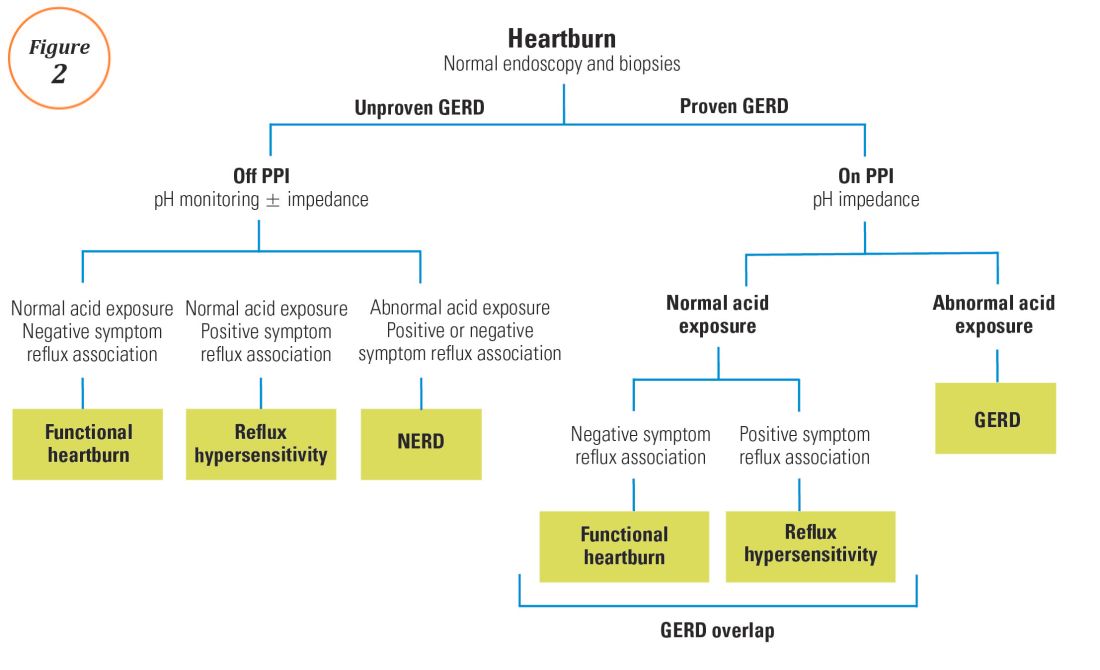
Rome IV Algorithm for the Evaluation of Heartburn. This figure was published in Aziz A, Fass R, Gyawali CP, Miwa H, Pandolfino J, Zerbib F. Esophageal Disorders. Gastroenterology 2016;150:1368-1379.
Along with reflux testing, an esophageal high-resolution manometry (HRM) study is typically performed to establish the location of the LES for placement of reflux catheters. Beyond this primary indication, HRM serves the important role of excluding significant esophageal motor disorders in these patients, particularly achalasia spectrum disorders.20 Despite a diametrically opposite pathophysiology compared to GERD, achalasia can present with retrosternal discomfort (often interpreted as heartburn) and esophageal regurgitation (potentially interpreted as acid regurgitation).21 Therefore, achalasia spectrum disorders can be mistaken for GERD and managed with acid suppression, thereby contributing to the pool of symptomatic patients refractory to PPI therapy. HRM has high accuracy and specificity for the diagnosis of achalasia and other major esophageal motor disorders.22 Other foregut disorders diagnosed using HRM (typically combined HRM and impedance, or HRiM) include rumination and supragastric belching. The exclusion of a major esophageal motor disorder is also a requirement for the diagnosis of a functional esophageal disorder, where esophageal reflux testing is normal.23

 Copyright Elsevier/AGA
Copyright Elsevier/AGA
