User login
45 researchers awarded millions in research funding
The Foundation introduced new awards in the 2021 awards cycle addressing diversity of GI investigators and the need for GI-specific COVID-19 research.
The American Gastroenterological Association is excited to announce the 45 researchers inducted into the 2021 class of AGA Research Foundation Awards Program recipients.
In the 2021 awards cycle, the AGA Research Foundation will provide more than $2.5 million in research funding to investigators working on projects that will further enhance our understanding of gastrointestinal and liver conditions and ultimately lead to the development of better treatment options for digestive diseases patients.
“This year, we made several enhancements to our awards portfolio to address current priorities for AGA and the field – we launched a new COVID-19 research award and established a summer undergraduate research fellowship to introduce talented underrepresented minority students into GI research,” said Robert S. Sandler, MD, MPH, AGAF, chair of the AGA Research Foundation. “We continue to change our funding program to meet the needs of GI research. What does not change is our long-standing commitment to support the research careers of talented early career investigators.”
The AGA Research Foundation Awards Program recruits, retains, and supports the most promising researchers in gastroenterology and hepatology. With funding from the foundation, recipients have protected time to take their research to the next level.
View the full list of recipients online.
The AGA Research Awards Program is made possible thanks to generous donors and funders. Learn more about the AGA Research Foundation at http://foundation.gastro.org.
The Foundation introduced new awards in the 2021 awards cycle addressing diversity of GI investigators and the need for GI-specific COVID-19 research.
The American Gastroenterological Association is excited to announce the 45 researchers inducted into the 2021 class of AGA Research Foundation Awards Program recipients.
In the 2021 awards cycle, the AGA Research Foundation will provide more than $2.5 million in research funding to investigators working on projects that will further enhance our understanding of gastrointestinal and liver conditions and ultimately lead to the development of better treatment options for digestive diseases patients.
“This year, we made several enhancements to our awards portfolio to address current priorities for AGA and the field – we launched a new COVID-19 research award and established a summer undergraduate research fellowship to introduce talented underrepresented minority students into GI research,” said Robert S. Sandler, MD, MPH, AGAF, chair of the AGA Research Foundation. “We continue to change our funding program to meet the needs of GI research. What does not change is our long-standing commitment to support the research careers of talented early career investigators.”
The AGA Research Foundation Awards Program recruits, retains, and supports the most promising researchers in gastroenterology and hepatology. With funding from the foundation, recipients have protected time to take their research to the next level.
View the full list of recipients online.
The AGA Research Awards Program is made possible thanks to generous donors and funders. Learn more about the AGA Research Foundation at http://foundation.gastro.org.
The Foundation introduced new awards in the 2021 awards cycle addressing diversity of GI investigators and the need for GI-specific COVID-19 research.
The American Gastroenterological Association is excited to announce the 45 researchers inducted into the 2021 class of AGA Research Foundation Awards Program recipients.
In the 2021 awards cycle, the AGA Research Foundation will provide more than $2.5 million in research funding to investigators working on projects that will further enhance our understanding of gastrointestinal and liver conditions and ultimately lead to the development of better treatment options for digestive diseases patients.
“This year, we made several enhancements to our awards portfolio to address current priorities for AGA and the field – we launched a new COVID-19 research award and established a summer undergraduate research fellowship to introduce talented underrepresented minority students into GI research,” said Robert S. Sandler, MD, MPH, AGAF, chair of the AGA Research Foundation. “We continue to change our funding program to meet the needs of GI research. What does not change is our long-standing commitment to support the research careers of talented early career investigators.”
The AGA Research Foundation Awards Program recruits, retains, and supports the most promising researchers in gastroenterology and hepatology. With funding from the foundation, recipients have protected time to take their research to the next level.
View the full list of recipients online.
The AGA Research Awards Program is made possible thanks to generous donors and funders. Learn more about the AGA Research Foundation at http://foundation.gastro.org.
Digital GI Corner: Digital navigation to automate patient engagement and reduce procedure no-shows
Patient navigation as a best practice for GI procedures
Colonoscopy is the preferred method for colorectal cancer (CRC) screening. Among scheduled outpatient colonoscopies, key metrics like no-show rates and poor bowel preparation can be as high as 25% in some facilities. These missed appointments and repeated calls with patients have been an important source of wasted resources, poor patient outcomes, and revenue loss for endoscopy facilities (estimated to be up to $1 million dollars for 10-member GI practice).
Studies have shown that patient navigation (PN), a patient-centered approach, overcomes barriers in health care delivery, thus improving adherence to CRC screening. Typically, navigators are specialized health practitioners who fill a variety of functions, including providing updates and instructions to patients, as well as assisting with test-related fears. Despite the overall cost-effectiveness, PN programs require significant resources from hospitals or medical groups. The continued focus in the United States on value-based medicine has provided an urgent need for cost-effective treatments that are also readily available to most physicians.
Digital navigation to automate navigation for colonoscopy and other GI procedures
(see Figure below). Given the widespread use of mobile phones, DN has the ability to change the way doctors and health care providers work. This led to Mount Sinai Health System, New York, conducting a quality improvement program to automate and evaluate the effectiveness of an automated text messaging and web-based “digital navigation” platform for decreasing colonoscopy appointment no-show rates.
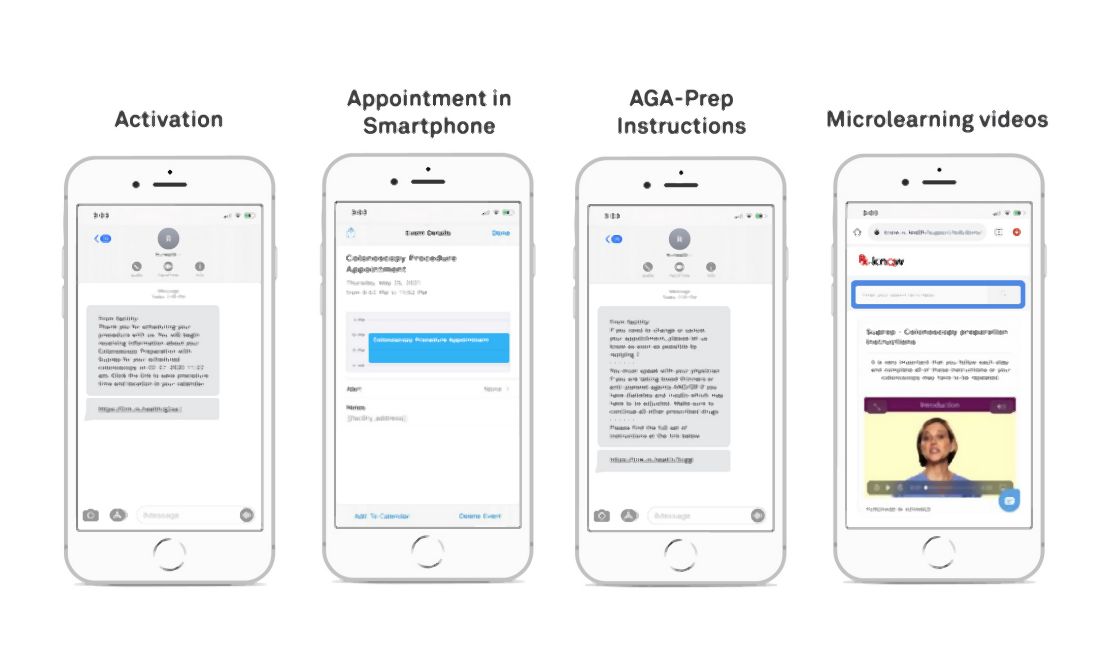
If a valid phone number was available in the patient’s electronic medical record chart and they did not opt out of receiving text message communications from the Mount Sinai Health System, patients over the age of 18 years who were scheduled for a colonoscopy at either of Mount Sinai Hospital, Mount Sinai Morningside, or Mount Sinai West were automatically sent DN SMS messages. The RxUniverse software platform (Rx.Health, New York) was used to send DN content through SMS to all eligible patients. The software platform interfaces with the EMR and endoscopy system (Provation) to automatically extract patient phone number and appointment details.
Impact of digital navigation and patient engagement
This study at Mount Sinai Health System demonstrated that patient engagement with SMS-based navigation is strongly predictive of colonoscopy completion. Patients with high engagement with digital navigation are about four times more likely to complete colonoscopy. Of all covariates included in the model, high DN engagement level had the largest effect size (odds ratio, 3.97), compared with no engagement. For health systems with patient navigators, targeting patients who are unlikely to engage DN or are low-engagers may be a more efficient use of person-to-person navigation.
Value-based reimbursement and cost-effectiveness have emerged as core principles in American health care reform, possibly requiring the creation of affordable, cost-effective approaches. Our research at Mount Sinai Health System suggested that SMS-based navigation can be a potential cost-effective strategy for reducing no-show rates. Beyond appointment no-shows, adequate bowel preparation is another important component of the preprocedure navigation process. Insufficient bowel preparation requires a repeat procedure, as poor visualization of the colon results in reduced therapeutic benefit from screening colonoscopy. We’ve shown in previous studies that our DN platform can increase bowel preparation efficiency, which results in lower rates of aborted procedures.
Missed colonoscopies not only cause longer wait times for patients, but they also cost the average facility $725 a day in lost revenue. It has been found through studies that traditional PN is cost-effective, with additional revenue generated from increased colonoscopy completion rates exceeding the costs of program implementation. While formal cost analyses have not been conducted on DN, estimates have shown around $1 million in annual savings for an average ambulatory surgery center or 10-member GI practice.
Looking ahead: AGA digital transformation network
After positive results for the Rx.Health’s platform were seen at Mount Sinai Health System, the American Gastroenterological Association partnered with Rx.Health to provide the GI community with a GI endoscopy transformation network. The core purpose of this endoscopy transformation network is to take an evidence-based approach and use digital medicine to positively affect key metrics and safety around periprocedural care and support “procedure bundles.” To illustrate the specific case of colonoscopy, these included the following: enhancing colorectal cancer surveillance rates though a comprehensive screening test strategy, decreasing no-show rates through shared decision-making and better preprocedure engagement, improving rates of adequate bowel preparation, benchmarking safety of procedures nationwide, and ensuring patient satisfaction and adequate recall for repeat procedures. These metrics represent key sources of revenue loss for provider organizations and, more importantly, have negative implications on patient care.
This collaboration is now supporting the implementation and expansion of the digital navigation program to all GI procedures at more than 15 different sites across the country.
Dr. Atreja is an adjunct associate professor at the Icahn School of Medicine at Mount Sinai, New York, and chief information officer and chief digital health officer at UC Davis Medical Center, Sacramento. The Icahn School of Medicine has licensed technology to Rx.Health. Dr. Atreja has no other conflicts to disclose
Patient navigation as a best practice for GI procedures
Colonoscopy is the preferred method for colorectal cancer (CRC) screening. Among scheduled outpatient colonoscopies, key metrics like no-show rates and poor bowel preparation can be as high as 25% in some facilities. These missed appointments and repeated calls with patients have been an important source of wasted resources, poor patient outcomes, and revenue loss for endoscopy facilities (estimated to be up to $1 million dollars for 10-member GI practice).
Studies have shown that patient navigation (PN), a patient-centered approach, overcomes barriers in health care delivery, thus improving adherence to CRC screening. Typically, navigators are specialized health practitioners who fill a variety of functions, including providing updates and instructions to patients, as well as assisting with test-related fears. Despite the overall cost-effectiveness, PN programs require significant resources from hospitals or medical groups. The continued focus in the United States on value-based medicine has provided an urgent need for cost-effective treatments that are also readily available to most physicians.
Digital navigation to automate navigation for colonoscopy and other GI procedures
(see Figure below). Given the widespread use of mobile phones, DN has the ability to change the way doctors and health care providers work. This led to Mount Sinai Health System, New York, conducting a quality improvement program to automate and evaluate the effectiveness of an automated text messaging and web-based “digital navigation” platform for decreasing colonoscopy appointment no-show rates.
If a valid phone number was available in the patient’s electronic medical record chart and they did not opt out of receiving text message communications from the Mount Sinai Health System, patients over the age of 18 years who were scheduled for a colonoscopy at either of Mount Sinai Hospital, Mount Sinai Morningside, or Mount Sinai West were automatically sent DN SMS messages. The RxUniverse software platform (Rx.Health, New York) was used to send DN content through SMS to all eligible patients. The software platform interfaces with the EMR and endoscopy system (Provation) to automatically extract patient phone number and appointment details.
Impact of digital navigation and patient engagement
This study at Mount Sinai Health System demonstrated that patient engagement with SMS-based navigation is strongly predictive of colonoscopy completion. Patients with high engagement with digital navigation are about four times more likely to complete colonoscopy. Of all covariates included in the model, high DN engagement level had the largest effect size (odds ratio, 3.97), compared with no engagement. For health systems with patient navigators, targeting patients who are unlikely to engage DN or are low-engagers may be a more efficient use of person-to-person navigation.
Value-based reimbursement and cost-effectiveness have emerged as core principles in American health care reform, possibly requiring the creation of affordable, cost-effective approaches. Our research at Mount Sinai Health System suggested that SMS-based navigation can be a potential cost-effective strategy for reducing no-show rates. Beyond appointment no-shows, adequate bowel preparation is another important component of the preprocedure navigation process. Insufficient bowel preparation requires a repeat procedure, as poor visualization of the colon results in reduced therapeutic benefit from screening colonoscopy. We’ve shown in previous studies that our DN platform can increase bowel preparation efficiency, which results in lower rates of aborted procedures.
Missed colonoscopies not only cause longer wait times for patients, but they also cost the average facility $725 a day in lost revenue. It has been found through studies that traditional PN is cost-effective, with additional revenue generated from increased colonoscopy completion rates exceeding the costs of program implementation. While formal cost analyses have not been conducted on DN, estimates have shown around $1 million in annual savings for an average ambulatory surgery center or 10-member GI practice.
Looking ahead: AGA digital transformation network
After positive results for the Rx.Health’s platform were seen at Mount Sinai Health System, the American Gastroenterological Association partnered with Rx.Health to provide the GI community with a GI endoscopy transformation network. The core purpose of this endoscopy transformation network is to take an evidence-based approach and use digital medicine to positively affect key metrics and safety around periprocedural care and support “procedure bundles.” To illustrate the specific case of colonoscopy, these included the following: enhancing colorectal cancer surveillance rates though a comprehensive screening test strategy, decreasing no-show rates through shared decision-making and better preprocedure engagement, improving rates of adequate bowel preparation, benchmarking safety of procedures nationwide, and ensuring patient satisfaction and adequate recall for repeat procedures. These metrics represent key sources of revenue loss for provider organizations and, more importantly, have negative implications on patient care.
This collaboration is now supporting the implementation and expansion of the digital navigation program to all GI procedures at more than 15 different sites across the country.
Dr. Atreja is an adjunct associate professor at the Icahn School of Medicine at Mount Sinai, New York, and chief information officer and chief digital health officer at UC Davis Medical Center, Sacramento. The Icahn School of Medicine has licensed technology to Rx.Health. Dr. Atreja has no other conflicts to disclose
Patient navigation as a best practice for GI procedures
Colonoscopy is the preferred method for colorectal cancer (CRC) screening. Among scheduled outpatient colonoscopies, key metrics like no-show rates and poor bowel preparation can be as high as 25% in some facilities. These missed appointments and repeated calls with patients have been an important source of wasted resources, poor patient outcomes, and revenue loss for endoscopy facilities (estimated to be up to $1 million dollars for 10-member GI practice).
Studies have shown that patient navigation (PN), a patient-centered approach, overcomes barriers in health care delivery, thus improving adherence to CRC screening. Typically, navigators are specialized health practitioners who fill a variety of functions, including providing updates and instructions to patients, as well as assisting with test-related fears. Despite the overall cost-effectiveness, PN programs require significant resources from hospitals or medical groups. The continued focus in the United States on value-based medicine has provided an urgent need for cost-effective treatments that are also readily available to most physicians.
Digital navigation to automate navigation for colonoscopy and other GI procedures
(see Figure below). Given the widespread use of mobile phones, DN has the ability to change the way doctors and health care providers work. This led to Mount Sinai Health System, New York, conducting a quality improvement program to automate and evaluate the effectiveness of an automated text messaging and web-based “digital navigation” platform for decreasing colonoscopy appointment no-show rates.
If a valid phone number was available in the patient’s electronic medical record chart and they did not opt out of receiving text message communications from the Mount Sinai Health System, patients over the age of 18 years who were scheduled for a colonoscopy at either of Mount Sinai Hospital, Mount Sinai Morningside, or Mount Sinai West were automatically sent DN SMS messages. The RxUniverse software platform (Rx.Health, New York) was used to send DN content through SMS to all eligible patients. The software platform interfaces with the EMR and endoscopy system (Provation) to automatically extract patient phone number and appointment details.
Impact of digital navigation and patient engagement
This study at Mount Sinai Health System demonstrated that patient engagement with SMS-based navigation is strongly predictive of colonoscopy completion. Patients with high engagement with digital navigation are about four times more likely to complete colonoscopy. Of all covariates included in the model, high DN engagement level had the largest effect size (odds ratio, 3.97), compared with no engagement. For health systems with patient navigators, targeting patients who are unlikely to engage DN or are low-engagers may be a more efficient use of person-to-person navigation.
Value-based reimbursement and cost-effectiveness have emerged as core principles in American health care reform, possibly requiring the creation of affordable, cost-effective approaches. Our research at Mount Sinai Health System suggested that SMS-based navigation can be a potential cost-effective strategy for reducing no-show rates. Beyond appointment no-shows, adequate bowel preparation is another important component of the preprocedure navigation process. Insufficient bowel preparation requires a repeat procedure, as poor visualization of the colon results in reduced therapeutic benefit from screening colonoscopy. We’ve shown in previous studies that our DN platform can increase bowel preparation efficiency, which results in lower rates of aborted procedures.
Missed colonoscopies not only cause longer wait times for patients, but they also cost the average facility $725 a day in lost revenue. It has been found through studies that traditional PN is cost-effective, with additional revenue generated from increased colonoscopy completion rates exceeding the costs of program implementation. While formal cost analyses have not been conducted on DN, estimates have shown around $1 million in annual savings for an average ambulatory surgery center or 10-member GI practice.
Looking ahead: AGA digital transformation network
After positive results for the Rx.Health’s platform were seen at Mount Sinai Health System, the American Gastroenterological Association partnered with Rx.Health to provide the GI community with a GI endoscopy transformation network. The core purpose of this endoscopy transformation network is to take an evidence-based approach and use digital medicine to positively affect key metrics and safety around periprocedural care and support “procedure bundles.” To illustrate the specific case of colonoscopy, these included the following: enhancing colorectal cancer surveillance rates though a comprehensive screening test strategy, decreasing no-show rates through shared decision-making and better preprocedure engagement, improving rates of adequate bowel preparation, benchmarking safety of procedures nationwide, and ensuring patient satisfaction and adequate recall for repeat procedures. These metrics represent key sources of revenue loss for provider organizations and, more importantly, have negative implications on patient care.
This collaboration is now supporting the implementation and expansion of the digital navigation program to all GI procedures at more than 15 different sites across the country.
Dr. Atreja is an adjunct associate professor at the Icahn School of Medicine at Mount Sinai, New York, and chief information officer and chief digital health officer at UC Davis Medical Center, Sacramento. The Icahn School of Medicine has licensed technology to Rx.Health. Dr. Atreja has no other conflicts to disclose
Top cases
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community (https://community.gastro.org) to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. The following is a preview of a recent popular clinical discussion.

In the post “Cessation of surveillance colonoscopy,” Gyanprakash A. Ketwaroo, MD, asked the following:Wanted to get your thoughts on how you approach stopping surveillance colonoscopy for older adults. Do you use decision support tools, assessing life-expectancy, prior polyp history, etc? Or is it more practical to defer to PCP for goals of care discussion prior to surveillance colonoscopy at certain age (eg 75 or 80)?See how AGA members responded and join the discussion: https://community.gastro.org/posts/24089.
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community (https://community.gastro.org) to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. The following is a preview of a recent popular clinical discussion.
In the post “Cessation of surveillance colonoscopy,” Gyanprakash A. Ketwaroo, MD, asked the following:Wanted to get your thoughts on how you approach stopping surveillance colonoscopy for older adults. Do you use decision support tools, assessing life-expectancy, prior polyp history, etc? Or is it more practical to defer to PCP for goals of care discussion prior to surveillance colonoscopy at certain age (eg 75 or 80)?See how AGA members responded and join the discussion: https://community.gastro.org/posts/24089.
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community (https://community.gastro.org) to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. The following is a preview of a recent popular clinical discussion.
In the post “Cessation of surveillance colonoscopy,” Gyanprakash A. Ketwaroo, MD, asked the following:Wanted to get your thoughts on how you approach stopping surveillance colonoscopy for older adults. Do you use decision support tools, assessing life-expectancy, prior polyp history, etc? Or is it more practical to defer to PCP for goals of care discussion prior to surveillance colonoscopy at certain age (eg 75 or 80)?See how AGA members responded and join the discussion: https://community.gastro.org/posts/24089.
Memorial and honorary gifts: A special tribute
Make a tribute gift to honor someone whose life has been touched by GI research or celebrate a special occasion such as a birthday while supporting the AGA Research Awards Program through the AGA Research Foundation. A tribute gift will make your loved one feel special because it honors their passion, and also help us fund research grants to talented investigators whose work will shape the future of clinical care.
- A gift in memory of a loved one. A memorial gift is a meaningful way to celebrate the legacy of a family member, friend, or colleague.
- A gift today. An outright gift will help fund the AGA Research Awards Program. Your gift will assist in furthering basic digestive disease research which can ultimately advance research into all digestive diseases. The financial benefits include an income tax deduction and possible elimination of capital gains tax.
Learn more about ways to recognize and acknowledge someone by visit our website at https://foundation.gastro.org/ways-to-contribute/.
Make a tribute gift to honor someone whose life has been touched by GI research or celebrate a special occasion such as a birthday while supporting the AGA Research Awards Program through the AGA Research Foundation. A tribute gift will make your loved one feel special because it honors their passion, and also help us fund research grants to talented investigators whose work will shape the future of clinical care.
- A gift in memory of a loved one. A memorial gift is a meaningful way to celebrate the legacy of a family member, friend, or colleague.
- A gift today. An outright gift will help fund the AGA Research Awards Program. Your gift will assist in furthering basic digestive disease research which can ultimately advance research into all digestive diseases. The financial benefits include an income tax deduction and possible elimination of capital gains tax.
Learn more about ways to recognize and acknowledge someone by visit our website at https://foundation.gastro.org/ways-to-contribute/.
Make a tribute gift to honor someone whose life has been touched by GI research or celebrate a special occasion such as a birthday while supporting the AGA Research Awards Program through the AGA Research Foundation. A tribute gift will make your loved one feel special because it honors their passion, and also help us fund research grants to talented investigators whose work will shape the future of clinical care.
- A gift in memory of a loved one. A memorial gift is a meaningful way to celebrate the legacy of a family member, friend, or colleague.
- A gift today. An outright gift will help fund the AGA Research Awards Program. Your gift will assist in furthering basic digestive disease research which can ultimately advance research into all digestive diseases. The financial benefits include an income tax deduction and possible elimination of capital gains tax.
Learn more about ways to recognize and acknowledge someone by visit our website at https://foundation.gastro.org/ways-to-contribute/.
Get to know DDW® 2021 Virtual
The world’s premier meeting for gastroenterology, hepatology, endoscopy, and gastrointestinal surgery professionals will be a fully virtual event, May 21-23, 2021. We invite you to take advantage of this unique opportunity to exchange knowledge with colleagues from all over the world and explore the latest advances in the field – all from the convenience of your home. Plus, your registration grants you access to everything offered at Digestive Disease Week® (DDW) this year (no additional ticketed sessions). Learn more and register at ddw.org.
The world’s premier meeting for gastroenterology, hepatology, endoscopy, and gastrointestinal surgery professionals will be a fully virtual event, May 21-23, 2021. We invite you to take advantage of this unique opportunity to exchange knowledge with colleagues from all over the world and explore the latest advances in the field – all from the convenience of your home. Plus, your registration grants you access to everything offered at Digestive Disease Week® (DDW) this year (no additional ticketed sessions). Learn more and register at ddw.org.
The world’s premier meeting for gastroenterology, hepatology, endoscopy, and gastrointestinal surgery professionals will be a fully virtual event, May 21-23, 2021. We invite you to take advantage of this unique opportunity to exchange knowledge with colleagues from all over the world and explore the latest advances in the field – all from the convenience of your home. Plus, your registration grants you access to everything offered at Digestive Disease Week® (DDW) this year (no additional ticketed sessions). Learn more and register at ddw.org.
Call for new AGA guideline topics
The AGA Institute Clinical Guidelines Committee wants your input on the next set of guidelines to be developed. By completing an online form, you can submit recommendations for guideline topics that will be developed within the next two years. The deadline to submit your ideas is Monday, May 3.
It’s as easy as three steps to submit a guideline idea
- Check out the guidelines that AGA has already developed or are in progress.
- Complete the survey below. You can submit more than one guideline topic by filling out the form multiple times.
- Stay tuned for follow up questions in case the committee needs more information on your recommendations.
The AGA Institute Clinical Guidelines Committee will review guideline topics in May, prioritizing and ranking topics based on the following criteria: prevalence of disease, resource utilization, variation in care, other existing guidelines, new data/changes in diagnosis or treatment, and potential for measure/quality development. Once vetted, four or more new guidelines will be recommended for development throughout the year. Complete the online survey at www.surveymonkey.com/r/AGAtopicsubmission
The AGA Institute Clinical Guidelines Committee wants your input on the next set of guidelines to be developed. By completing an online form, you can submit recommendations for guideline topics that will be developed within the next two years. The deadline to submit your ideas is Monday, May 3.
It’s as easy as three steps to submit a guideline idea
- Check out the guidelines that AGA has already developed or are in progress.
- Complete the survey below. You can submit more than one guideline topic by filling out the form multiple times.
- Stay tuned for follow up questions in case the committee needs more information on your recommendations.
The AGA Institute Clinical Guidelines Committee will review guideline topics in May, prioritizing and ranking topics based on the following criteria: prevalence of disease, resource utilization, variation in care, other existing guidelines, new data/changes in diagnosis or treatment, and potential for measure/quality development. Once vetted, four or more new guidelines will be recommended for development throughout the year. Complete the online survey at www.surveymonkey.com/r/AGAtopicsubmission
The AGA Institute Clinical Guidelines Committee wants your input on the next set of guidelines to be developed. By completing an online form, you can submit recommendations for guideline topics that will be developed within the next two years. The deadline to submit your ideas is Monday, May 3.
It’s as easy as three steps to submit a guideline idea
- Check out the guidelines that AGA has already developed or are in progress.
- Complete the survey below. You can submit more than one guideline topic by filling out the form multiple times.
- Stay tuned for follow up questions in case the committee needs more information on your recommendations.
The AGA Institute Clinical Guidelines Committee will review guideline topics in May, prioritizing and ranking topics based on the following criteria: prevalence of disease, resource utilization, variation in care, other existing guidelines, new data/changes in diagnosis or treatment, and potential for measure/quality development. Once vetted, four or more new guidelines will be recommended for development throughout the year. Complete the online survey at www.surveymonkey.com/r/AGAtopicsubmission
AGAF applications now open
Applications are now open for the 2022 AGA Fellowship cohort. AGA is proud to formally recognize its exemplary members whose accomplishments and contributions demonstrate a deep commitment to gastroenterology through the AGA Fellows Program. Those in clinical practice, education or research (basic or clinical) are encouraged to apply today.
Longstanding members who apply and meet the program criteria are granted the distinguished honor of AGA Fellowship and receive the following:
- The privilege of using the designation “AGAF” in professional activities.
- An official certificate and pin denoting your status.
- International acknowledgment at Digestive Disease Week® (DDW).
- A listing on the AGA website alongside esteemed peers.
- A pre-written, fill-in press release and a digital badge to inform others of your accomplishment.
Apply for consideration and gain recognition worldwide for your commitment to the field. The deadline is Aug. 24.
Applications are now open for the 2022 AGA Fellowship cohort. AGA is proud to formally recognize its exemplary members whose accomplishments and contributions demonstrate a deep commitment to gastroenterology through the AGA Fellows Program. Those in clinical practice, education or research (basic or clinical) are encouraged to apply today.
Longstanding members who apply and meet the program criteria are granted the distinguished honor of AGA Fellowship and receive the following:
- The privilege of using the designation “AGAF” in professional activities.
- An official certificate and pin denoting your status.
- International acknowledgment at Digestive Disease Week® (DDW).
- A listing on the AGA website alongside esteemed peers.
- A pre-written, fill-in press release and a digital badge to inform others of your accomplishment.
Apply for consideration and gain recognition worldwide for your commitment to the field. The deadline is Aug. 24.
Applications are now open for the 2022 AGA Fellowship cohort. AGA is proud to formally recognize its exemplary members whose accomplishments and contributions demonstrate a deep commitment to gastroenterology through the AGA Fellows Program. Those in clinical practice, education or research (basic or clinical) are encouraged to apply today.
Longstanding members who apply and meet the program criteria are granted the distinguished honor of AGA Fellowship and receive the following:
- The privilege of using the designation “AGAF” in professional activities.
- An official certificate and pin denoting your status.
- International acknowledgment at Digestive Disease Week® (DDW).
- A listing on the AGA website alongside esteemed peers.
- A pre-written, fill-in press release and a digital badge to inform others of your accomplishment.
Apply for consideration and gain recognition worldwide for your commitment to the field. The deadline is Aug. 24.
Top cases
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community (https://community.gastro.org) to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. Here’s a preview of a recent popular clinical discussion:
From Jennifer Weiss, MD, MS, AGAF: Implementing CRC screening at 45:
The ACS recommended lowering the CRC screening age to 45, ACG has recently followed suit, and the USPSTF draft revisions also support a lower CRC screening age. In this month of colorectal cancer awareness, I was wondering how many people have started implementing this change in their practice and if they have received any pushback from insurance companies?
See how AGA members responded and join the discussion: https://community.gastro.org/posts/23923
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community (https://community.gastro.org) to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. Here’s a preview of a recent popular clinical discussion:
From Jennifer Weiss, MD, MS, AGAF: Implementing CRC screening at 45:
The ACS recommended lowering the CRC screening age to 45, ACG has recently followed suit, and the USPSTF draft revisions also support a lower CRC screening age. In this month of colorectal cancer awareness, I was wondering how many people have started implementing this change in their practice and if they have received any pushback from insurance companies?
See how AGA members responded and join the discussion: https://community.gastro.org/posts/23923
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community (https://community.gastro.org) to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. Here’s a preview of a recent popular clinical discussion:
From Jennifer Weiss, MD, MS, AGAF: Implementing CRC screening at 45:
The ACS recommended lowering the CRC screening age to 45, ACG has recently followed suit, and the USPSTF draft revisions also support a lower CRC screening age. In this month of colorectal cancer awareness, I was wondering how many people have started implementing this change in their practice and if they have received any pushback from insurance companies?
See how AGA members responded and join the discussion: https://community.gastro.org/posts/23923
Top cases
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. The following is a preview of a recent popular clinical discussion:
From John Fang, MD: Update on feeding tubes: Indications and troubleshooting complications.
Gastroenterologists are uniquely positioned to manage individuals with feeding tubes as their training underscores principles in digestion, nutrition support, and enteral tube placement. Adequate management of individuals with feeding tubes and, importantly, the complications that arise from feeding tube use and placement require both right education and experience. Therefore, gastroenterologists are well suited to both place and manage individuals with feeding tubes in the long term.
Questions:
1. Are gastroenterologist best suited for placement and management of feeding tubes (vs. interventional radiology or surgery)?
2. Are gastroenterologists adequately trained place and manage feeding tubes?
3. What are the most difficult complication(s) of feeding tubes to manage?
The conversation stems from the February In Focus article from The New Gastroenterologist, “Update on feeding tubes: Indications and troubleshooting complications.”
See how AGA members responded and join the discussion: https://community.gastro.org/posts/23639.
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. The following is a preview of a recent popular clinical discussion:
From John Fang, MD: Update on feeding tubes: Indications and troubleshooting complications.
Gastroenterologists are uniquely positioned to manage individuals with feeding tubes as their training underscores principles in digestion, nutrition support, and enteral tube placement. Adequate management of individuals with feeding tubes and, importantly, the complications that arise from feeding tube use and placement require both right education and experience. Therefore, gastroenterologists are well suited to both place and manage individuals with feeding tubes in the long term.
Questions:
1. Are gastroenterologist best suited for placement and management of feeding tubes (vs. interventional radiology or surgery)?
2. Are gastroenterologists adequately trained place and manage feeding tubes?
3. What are the most difficult complication(s) of feeding tubes to manage?
The conversation stems from the February In Focus article from The New Gastroenterologist, “Update on feeding tubes: Indications and troubleshooting complications.”
See how AGA members responded and join the discussion: https://community.gastro.org/posts/23639.
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. The following is a preview of a recent popular clinical discussion:
From John Fang, MD: Update on feeding tubes: Indications and troubleshooting complications.
Gastroenterologists are uniquely positioned to manage individuals with feeding tubes as their training underscores principles in digestion, nutrition support, and enteral tube placement. Adequate management of individuals with feeding tubes and, importantly, the complications that arise from feeding tube use and placement require both right education and experience. Therefore, gastroenterologists are well suited to both place and manage individuals with feeding tubes in the long term.
Questions:
1. Are gastroenterologist best suited for placement and management of feeding tubes (vs. interventional radiology or surgery)?
2. Are gastroenterologists adequately trained place and manage feeding tubes?
3. What are the most difficult complication(s) of feeding tubes to manage?
The conversation stems from the February In Focus article from The New Gastroenterologist, “Update on feeding tubes: Indications and troubleshooting complications.”
See how AGA members responded and join the discussion: https://community.gastro.org/posts/23639.
Introducing this year’s Recognition Prize recipients
“AGA Recognition Prizes allow members to honor their contemporaries for their exceptional contributions to the field of gastroenterology and hepatology,” said Hashem B. El-Serag, MD, MPH, AGAF, chair of AGA. “The 2021 AGA Recognition Prize winners represent only a small group of our widely distinguished and exceptional members who help make AGA such an accomplished organization. We are honored that such esteemed individuals are representatives of AGA.”
This year the AGA Recognition Prizes will be presented virtually in May 2021.
- Michael Camilleri, MD, AGAF, Julius Friedenwald Medal
- Byron Cryer, MD, Distinguished Service Award in Diversity, Equity and Inclusion
- Sandra Quezada, MD, MS, Distinguished Service Award in Diversity, Equity and Inclusion
- Kim Barrett, Distinguished Achievement Award in Basic Science
- David Y. Graham, William Beaumont Prize
- Griffin Rodgers, MD, MACP, Research Service Award
- Lin Chang, Distinguished Educator Award
- Nimish Vakil, MD, AGAF, FASGE, Distinguished Clinician Award in Private Practice
- Peter H.R. Green, Distinguished Clinician Award in Academic Practice
- Vay Liang “Bill” Go, MD, AGAF, Distinguished Mentor Award
- Shahnaz Sultan, MD, MHSc, AGAF, Outstanding Service Award
- Osama Altayar, MD, Outstanding Service Award
- Perica Davitkov, MD, Outstanding Service Award
- Joseph D. Feuerstein, MD, Outstanding Service Award
- Shazia M. Siddique, MD, MSHP, Outstanding Service Award
- Yngve T. Falck-Ytter, MD, AGAF, Outstanding Service Award
- Joseph K. Lim, MD, AGAF, Outstanding Service Award
To learn more about our 2021 AGA recognition prize recipients, visit https://gastro.org/2021awards.
“AGA Recognition Prizes allow members to honor their contemporaries for their exceptional contributions to the field of gastroenterology and hepatology,” said Hashem B. El-Serag, MD, MPH, AGAF, chair of AGA. “The 2021 AGA Recognition Prize winners represent only a small group of our widely distinguished and exceptional members who help make AGA such an accomplished organization. We are honored that such esteemed individuals are representatives of AGA.”
This year the AGA Recognition Prizes will be presented virtually in May 2021.
- Michael Camilleri, MD, AGAF, Julius Friedenwald Medal
- Byron Cryer, MD, Distinguished Service Award in Diversity, Equity and Inclusion
- Sandra Quezada, MD, MS, Distinguished Service Award in Diversity, Equity and Inclusion
- Kim Barrett, Distinguished Achievement Award in Basic Science
- David Y. Graham, William Beaumont Prize
- Griffin Rodgers, MD, MACP, Research Service Award
- Lin Chang, Distinguished Educator Award
- Nimish Vakil, MD, AGAF, FASGE, Distinguished Clinician Award in Private Practice
- Peter H.R. Green, Distinguished Clinician Award in Academic Practice
- Vay Liang “Bill” Go, MD, AGAF, Distinguished Mentor Award
- Shahnaz Sultan, MD, MHSc, AGAF, Outstanding Service Award
- Osama Altayar, MD, Outstanding Service Award
- Perica Davitkov, MD, Outstanding Service Award
- Joseph D. Feuerstein, MD, Outstanding Service Award
- Shazia M. Siddique, MD, MSHP, Outstanding Service Award
- Yngve T. Falck-Ytter, MD, AGAF, Outstanding Service Award
- Joseph K. Lim, MD, AGAF, Outstanding Service Award
To learn more about our 2021 AGA recognition prize recipients, visit https://gastro.org/2021awards.
“AGA Recognition Prizes allow members to honor their contemporaries for their exceptional contributions to the field of gastroenterology and hepatology,” said Hashem B. El-Serag, MD, MPH, AGAF, chair of AGA. “The 2021 AGA Recognition Prize winners represent only a small group of our widely distinguished and exceptional members who help make AGA such an accomplished organization. We are honored that such esteemed individuals are representatives of AGA.”
This year the AGA Recognition Prizes will be presented virtually in May 2021.
- Michael Camilleri, MD, AGAF, Julius Friedenwald Medal
- Byron Cryer, MD, Distinguished Service Award in Diversity, Equity and Inclusion
- Sandra Quezada, MD, MS, Distinguished Service Award in Diversity, Equity and Inclusion
- Kim Barrett, Distinguished Achievement Award in Basic Science
- David Y. Graham, William Beaumont Prize
- Griffin Rodgers, MD, MACP, Research Service Award
- Lin Chang, Distinguished Educator Award
- Nimish Vakil, MD, AGAF, FASGE, Distinguished Clinician Award in Private Practice
- Peter H.R. Green, Distinguished Clinician Award in Academic Practice
- Vay Liang “Bill” Go, MD, AGAF, Distinguished Mentor Award
- Shahnaz Sultan, MD, MHSc, AGAF, Outstanding Service Award
- Osama Altayar, MD, Outstanding Service Award
- Perica Davitkov, MD, Outstanding Service Award
- Joseph D. Feuerstein, MD, Outstanding Service Award
- Shazia M. Siddique, MD, MSHP, Outstanding Service Award
- Yngve T. Falck-Ytter, MD, AGAF, Outstanding Service Award
- Joseph K. Lim, MD, AGAF, Outstanding Service Award
To learn more about our 2021 AGA recognition prize recipients, visit https://gastro.org/2021awards.