User login
Restless Legs Syndrome Among Veterans With Spinal Cord Lesions (FULL)
Spinal cord injuries (SCI) are common in veteran populations.1 Veterans with spinal cord injuries and disorders (SCI/D) also may have concurrent sleep disturbances. Spinal cord injury typically causes spasticity.2,3 Hypersensitivity of the flexor reflex pathways is believed to cause painful muscle spasms in patients with SCI.4 Neuropathic pain at or below the level of the lesion also is common.
Restless legs syndrome (RLS) is a common sleep disorder that affects sleep quality and can occur concomitantly with spinal cord lesions.5 In about 80% of RLS cases, involuntary movements of legs across hip, knee, and ankle joints during sleep, known as periodic limb movement during sleep (PLMS), occurs.6 Several studies showed increased prevalence of PLMS in patients with SCI, and some case reports suggest an increased prevalence of RLS in this population.7,8 One small study showed that 100% of patients with SCI had symptoms of RLS.6 Another study found that SCI could trigger PLMS.8
The pathophysiology of RLS and PLMS in patients with SCI is not fully understood, but case reports describing PLM in SCI patients points to a possible role of central pattern generators and the flexor reflex afferents in the pathophysiology of PLMS.9,10 Changes of the tissue microstructure in the midbrain and upper cervical spinal cord have been described in patients with RLS.11The objective of this study was to assess the prevalence of RLS in a veteran population with SCI/D and
Methods
The institutional review and ethical approval boards of the Minneapolis VA Health Care System approved the study. Within the VA system, 666 patients with SCI/D were identified using a national database. Of the 666 people, 316 were excluded, 199 were included, and 151 were deceased.
Patients aged between 18 and 65 years were included in the study. Charts of patients who had been discharged with the diagnosis of SCI from 2002 to 2008 were studied. All patients met the inclusion criteria of the International Restless Legs Syndrome Study Group diagnosis.
Exclusion criteria were as follows: Patients with evidence of brain pathology (eg, stroke), concurrent neurologic condition associated with RLS (Parkinson disease, spinocerebellar ataxia, peripheral neuropathy), concurrent psychiatric condition within the setting of treatment with dopamine antagonists, secondary causes of RLS (renal failure/uremia, iron deficiency, rheumatoid arthritis, and pregnancy) and a recent history of alcohol or drug misuse or current evidence of substance use of < 1 year.
A patient list was compiled that included the etiology of the SCI (vascular injury, multiple sclerosis [MS], trauma, unknown, and other), the level(s) and completeness of the SCI per radiology report, RLS pharmacotherapies, and pertinent medical history.
Axial T2-weighted images on magnetic resonance imaging (MRI) scans were retrospectively reviewed. Sagittal T1/T2-weighted and axial T2-weighted sequences were performed routinely on all patients with spinal cord lesions. The analysis included the extension of the lesion on both sagittal and axial distributions. The anatomic location of the cord lesion was categorized by the following: (1) pure gray matter (central cord); (2) white matter (dorsal [D], dorsolateral [DL], ventral [V], ventrolateral areas [VL]).
A questionnaire using standard diagnostic criteria for RLS was mailed to the 199 patients who met the inclusion criteria (Appendix A). 

All analyses were carried out using StataCorp STATA 13 (College Station, TX). Descriptive statistics were used. The analyses were carried out using chi-square and Fisher exact tests. Differences between the groups were considered statistically significant at P < .05. The data were analyzed to obtain point prevalence among patients with SCI, and comparisons were made among the different subgroups.
Results
Of the 162 patients who chose to participate in the study, the sleep specialists confirmed 31 (19%) to have RLS, 112 (69%) were confirmed negative for RLS, and an additional 19 (12%) screened positive for RLS but were not confirmed to have RLS by the sleep specialists (Figure 1). 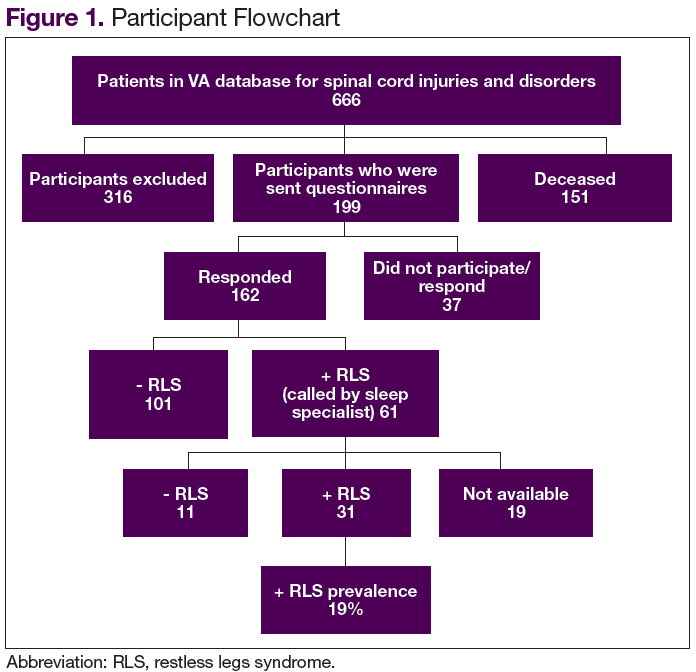
The etiology of SCI was subdivided into 4 groups: MS, trauma, vascular, and other/unknown. Within each group (– RLS vs + RLS), MS and trauma were the most common etiologies with 55% MS and 36% trauma in the + RLS group.
When comparing RLS among the spinal cord levels (cervical, thoracic, lumbar and cervical + thoracic), only the cervical + thoracic subgroup (18% + RLS vs 5% – RLS) showed a significant difference (Figure 2). 
There was no significant difference found with the prevalence of RLS in the axial plane of the spinal cord lesions (ventral/ventro-lateral/central cord vs dorsal/dorsolateral) or by the completeness of spinal cord lesions, P = .76. There was a higher prevalence of incomplete cord injury, however, within each subgroup of RLS.
The Mann-Whitney test was used to analyze the burden of disease in both groups (+ RLS vs – RLS). Moderate level of burden was most frequently reported with a higher prevalence within the + RLS group. Of those receiving treatment for RLS, 71% were + RLS vs 46% – RLS with a P value of .01. Symptoms of RLS after cord injury were 89% + RLS vs 55% – RLS with a P value of .03.
Discussion
This study represents one of the first studies to determine the prevalence of RLS in veterans with spinal cord disease. Research in this area is important to raise awareness of RLS among the veteran population with and without SCI and disorders. Restless legs syndrome often escapes diagnosis because of difficulty understanding the patient’s descriptions of their sensations. In addition, RLS may cause debilitating symptoms of sleep deprivation, daytime sleepiness, discomfort, and fatigue, which often results in decreased quality of life (QOL). Proper screening and treatment may improve QOL.
A study by Kumru and colleagues showed a similar rate of RLS in patients with SCI and RLS symptoms presented in the first year after SCI as did this study (18% vs 19%, respectively).4 In that study, RLS was more common in patients with lesions in lumbosacral area. Kumru and colleagues also showed that a dopaminergic medication improved symptoms of RLS in this population, whereas this study did not explore treatment outcomes.4
The pathogenesis of RLS is not fully known, but hereditary factors, iron metabolism, and the brain dopaminergic system are thought to be involved.11 It is hypothesized that spinal cord lesions allow the appearance of RLS symptoms and spinal leg movement generator by blocking descending inhibitory spinal pathways.12 One hypothesis is that damage to A11 nuclei (the main source of dopamine in the spinal cord or its diencephalospinal tract in animals) causes hyperexcitability of the spinal cord and leads to PLM and RLS symptoms.13 As the axons of A11 nuclei are present along the whole span of the spinal cord, SCI/D in patients with RLS might interrupt this dopaminergic tract and produce the RLS symptoms.
Limitations
This study included only veterans, so the prevalence may not apply to the nonveteran SCI population. Also, the population mainly was male, and there was no accurate information on race. Ferritin levels of the patients were not checked and is a major factor in RLS. The reported onset of RLS after the SCI could be due to recall bias.
Conclusion
The prevalence of RLS in veterans with SCI is above that reported in the general population (19% vs 10%, respectively). Furthermore, those with RLS have symptoms that often started after the SCI (suggesting causality) and required therapy due to their level of RLS symptom burden. A spectrum of severity of symptoms is present among those with RLS, with 83% having moderate-to-severe RLS affecting their QOL.
Although there was not a statistically significant relationship between RLS and spinal cord lesion level, there was a slightly higher prevalence of RLS at the cervical and thoracic levels, which may be relevant for future studies. There was no difference found between the RLS subgroups with respect to the location of the lesion within the spinal cord; however, a larger sample size may be needed to determine whether this would reach statistical significance. Prompt search for symptoms of RLS in veterans with SCI is warranted to provide adequate treatment to improve sleep health and QOL in this population.
1. Lasfargues JE, Custis D, Morrone F, Carswell J, Nguyen T. A model for estimating spinal cord injury prevalence in the United States. Paraplegia. 1995;33(2):62-68.
2. Sjölund BH. Pain and rehabilitation after spinal cord injury: the case of sensory spasticity? Brain Res Brain Res Rev. 2002;40(1-3):250-256.
3. Adams MM, Hicks AL. Spasticity after spinal cord injury. Spinal Cord. 2005;43(10):577-586.
4. Kumru H, Vidal J, Benito J, et al. Restless leg syndrome in patients with spinal cord injury. Parkinsonism Relat Disord. 2015;21(12):1461-1464.
5. Wilt TJ, MacDonald R, Ouellette J, et al. Pharmacologic therapy for primary restless legs syndrome: a systematic review and meta-analysis. JAMA Intern Med. 2013;173(7):496-505.
6. American Academy of Sleep Medicine. The International Classification of Sleep Disorders: Diagnostic and Coding Manual. (AASM ICSD-3). 3rd ed. Westchester, IL: American Academy of Sleep Medicine; 2014.
7. Telles SC, Alves RC, Chadi G. Periodic limb movements during sleep and restless legs syndrome in patients with ASIA A spinal cord injury. J Neurol Sci. 2011;303(1-2):119-123.
8. Telles SC, Alves RS, Chadi G. Spinal cord injury as a trigger to develop periodic leg movements during sleep: an evolutionary perspective. Arq Neuropsiquiatr. 2012;70(11):880-884.
9. Tings T, Baier PC, Paulus W, Trenkwalder C. Restless legs syndrome induced by impairment of sensory spinal pathways. J Neurol. 2003;250(4):499-500.
10. Paulus W, Trenkwalder C. Less is more: pathophysiology of dopaminergic-therapy-related augmentation in restless legs syndrome. Lancet Neurol. 2006;5(10):878-886.
11. Silber MH, Ehrenberg BL, Allen RP, et al; Medical Advisory Board of the Restless Legs Syndrome Foundation. An algorithm for the management of restless legs syndrome. Mayo Clin Proc. 2004;79(7):916-922.
12. Hartmann M, Pfister R, Pfadenhauer K. Restless legs syndrome associated with spinal cord lesions. J Neurol Neurosurg Psychiatry. 1999;66(5):688-689.
13. Clemens S, Rye D, Hochman S. Restless legs syndrome: revisiting the dopamine hypothesis from the spinal cord perspective. Neurology. 2006;67(1):125-130.
Spinal cord injuries (SCI) are common in veteran populations.1 Veterans with spinal cord injuries and disorders (SCI/D) also may have concurrent sleep disturbances. Spinal cord injury typically causes spasticity.2,3 Hypersensitivity of the flexor reflex pathways is believed to cause painful muscle spasms in patients with SCI.4 Neuropathic pain at or below the level of the lesion also is common.
Restless legs syndrome (RLS) is a common sleep disorder that affects sleep quality and can occur concomitantly with spinal cord lesions.5 In about 80% of RLS cases, involuntary movements of legs across hip, knee, and ankle joints during sleep, known as periodic limb movement during sleep (PLMS), occurs.6 Several studies showed increased prevalence of PLMS in patients with SCI, and some case reports suggest an increased prevalence of RLS in this population.7,8 One small study showed that 100% of patients with SCI had symptoms of RLS.6 Another study found that SCI could trigger PLMS.8
The pathophysiology of RLS and PLMS in patients with SCI is not fully understood, but case reports describing PLM in SCI patients points to a possible role of central pattern generators and the flexor reflex afferents in the pathophysiology of PLMS.9,10 Changes of the tissue microstructure in the midbrain and upper cervical spinal cord have been described in patients with RLS.11The objective of this study was to assess the prevalence of RLS in a veteran population with SCI/D and
Methods
The institutional review and ethical approval boards of the Minneapolis VA Health Care System approved the study. Within the VA system, 666 patients with SCI/D were identified using a national database. Of the 666 people, 316 were excluded, 199 were included, and 151 were deceased.
Patients aged between 18 and 65 years were included in the study. Charts of patients who had been discharged with the diagnosis of SCI from 2002 to 2008 were studied. All patients met the inclusion criteria of the International Restless Legs Syndrome Study Group diagnosis.
Exclusion criteria were as follows: Patients with evidence of brain pathology (eg, stroke), concurrent neurologic condition associated with RLS (Parkinson disease, spinocerebellar ataxia, peripheral neuropathy), concurrent psychiatric condition within the setting of treatment with dopamine antagonists, secondary causes of RLS (renal failure/uremia, iron deficiency, rheumatoid arthritis, and pregnancy) and a recent history of alcohol or drug misuse or current evidence of substance use of < 1 year.
A patient list was compiled that included the etiology of the SCI (vascular injury, multiple sclerosis [MS], trauma, unknown, and other), the level(s) and completeness of the SCI per radiology report, RLS pharmacotherapies, and pertinent medical history.
Axial T2-weighted images on magnetic resonance imaging (MRI) scans were retrospectively reviewed. Sagittal T1/T2-weighted and axial T2-weighted sequences were performed routinely on all patients with spinal cord lesions. The analysis included the extension of the lesion on both sagittal and axial distributions. The anatomic location of the cord lesion was categorized by the following: (1) pure gray matter (central cord); (2) white matter (dorsal [D], dorsolateral [DL], ventral [V], ventrolateral areas [VL]).
A questionnaire using standard diagnostic criteria for RLS was mailed to the 199 patients who met the inclusion criteria (Appendix A).
All analyses were carried out using StataCorp STATA 13 (College Station, TX). Descriptive statistics were used. The analyses were carried out using chi-square and Fisher exact tests. Differences between the groups were considered statistically significant at P < .05. The data were analyzed to obtain point prevalence among patients with SCI, and comparisons were made among the different subgroups.
Results
Of the 162 patients who chose to participate in the study, the sleep specialists confirmed 31 (19%) to have RLS, 112 (69%) were confirmed negative for RLS, and an additional 19 (12%) screened positive for RLS but were not confirmed to have RLS by the sleep specialists (Figure 1).
The etiology of SCI was subdivided into 4 groups: MS, trauma, vascular, and other/unknown. Within each group (– RLS vs + RLS), MS and trauma were the most common etiologies with 55% MS and 36% trauma in the + RLS group.
When comparing RLS among the spinal cord levels (cervical, thoracic, lumbar and cervical + thoracic), only the cervical + thoracic subgroup (18% + RLS vs 5% – RLS) showed a significant difference (Figure 2).
There was no significant difference found with the prevalence of RLS in the axial plane of the spinal cord lesions (ventral/ventro-lateral/central cord vs dorsal/dorsolateral) or by the completeness of spinal cord lesions, P = .76. There was a higher prevalence of incomplete cord injury, however, within each subgroup of RLS.
The Mann-Whitney test was used to analyze the burden of disease in both groups (+ RLS vs – RLS). Moderate level of burden was most frequently reported with a higher prevalence within the + RLS group. Of those receiving treatment for RLS, 71% were + RLS vs 46% – RLS with a P value of .01. Symptoms of RLS after cord injury were 89% + RLS vs 55% – RLS with a P value of .03.
Discussion
This study represents one of the first studies to determine the prevalence of RLS in veterans with spinal cord disease. Research in this area is important to raise awareness of RLS among the veteran population with and without SCI and disorders. Restless legs syndrome often escapes diagnosis because of difficulty understanding the patient’s descriptions of their sensations. In addition, RLS may cause debilitating symptoms of sleep deprivation, daytime sleepiness, discomfort, and fatigue, which often results in decreased quality of life (QOL). Proper screening and treatment may improve QOL.
A study by Kumru and colleagues showed a similar rate of RLS in patients with SCI and RLS symptoms presented in the first year after SCI as did this study (18% vs 19%, respectively).4 In that study, RLS was more common in patients with lesions in lumbosacral area. Kumru and colleagues also showed that a dopaminergic medication improved symptoms of RLS in this population, whereas this study did not explore treatment outcomes.4
The pathogenesis of RLS is not fully known, but hereditary factors, iron metabolism, and the brain dopaminergic system are thought to be involved.11 It is hypothesized that spinal cord lesions allow the appearance of RLS symptoms and spinal leg movement generator by blocking descending inhibitory spinal pathways.12 One hypothesis is that damage to A11 nuclei (the main source of dopamine in the spinal cord or its diencephalospinal tract in animals) causes hyperexcitability of the spinal cord and leads to PLM and RLS symptoms.13 As the axons of A11 nuclei are present along the whole span of the spinal cord, SCI/D in patients with RLS might interrupt this dopaminergic tract and produce the RLS symptoms.
Limitations
This study included only veterans, so the prevalence may not apply to the nonveteran SCI population. Also, the population mainly was male, and there was no accurate information on race. Ferritin levels of the patients were not checked and is a major factor in RLS. The reported onset of RLS after the SCI could be due to recall bias.
Conclusion
The prevalence of RLS in veterans with SCI is above that reported in the general population (19% vs 10%, respectively). Furthermore, those with RLS have symptoms that often started after the SCI (suggesting causality) and required therapy due to their level of RLS symptom burden. A spectrum of severity of symptoms is present among those with RLS, with 83% having moderate-to-severe RLS affecting their QOL.
Although there was not a statistically significant relationship between RLS and spinal cord lesion level, there was a slightly higher prevalence of RLS at the cervical and thoracic levels, which may be relevant for future studies. There was no difference found between the RLS subgroups with respect to the location of the lesion within the spinal cord; however, a larger sample size may be needed to determine whether this would reach statistical significance. Prompt search for symptoms of RLS in veterans with SCI is warranted to provide adequate treatment to improve sleep health and QOL in this population.
Spinal cord injuries (SCI) are common in veteran populations.1 Veterans with spinal cord injuries and disorders (SCI/D) also may have concurrent sleep disturbances. Spinal cord injury typically causes spasticity.2,3 Hypersensitivity of the flexor reflex pathways is believed to cause painful muscle spasms in patients with SCI.4 Neuropathic pain at or below the level of the lesion also is common.
Restless legs syndrome (RLS) is a common sleep disorder that affects sleep quality and can occur concomitantly with spinal cord lesions.5 In about 80% of RLS cases, involuntary movements of legs across hip, knee, and ankle joints during sleep, known as periodic limb movement during sleep (PLMS), occurs.6 Several studies showed increased prevalence of PLMS in patients with SCI, and some case reports suggest an increased prevalence of RLS in this population.7,8 One small study showed that 100% of patients with SCI had symptoms of RLS.6 Another study found that SCI could trigger PLMS.8
The pathophysiology of RLS and PLMS in patients with SCI is not fully understood, but case reports describing PLM in SCI patients points to a possible role of central pattern generators and the flexor reflex afferents in the pathophysiology of PLMS.9,10 Changes of the tissue microstructure in the midbrain and upper cervical spinal cord have been described in patients with RLS.11The objective of this study was to assess the prevalence of RLS in a veteran population with SCI/D and
Methods
The institutional review and ethical approval boards of the Minneapolis VA Health Care System approved the study. Within the VA system, 666 patients with SCI/D were identified using a national database. Of the 666 people, 316 were excluded, 199 were included, and 151 were deceased.
Patients aged between 18 and 65 years were included in the study. Charts of patients who had been discharged with the diagnosis of SCI from 2002 to 2008 were studied. All patients met the inclusion criteria of the International Restless Legs Syndrome Study Group diagnosis.
Exclusion criteria were as follows: Patients with evidence of brain pathology (eg, stroke), concurrent neurologic condition associated with RLS (Parkinson disease, spinocerebellar ataxia, peripheral neuropathy), concurrent psychiatric condition within the setting of treatment with dopamine antagonists, secondary causes of RLS (renal failure/uremia, iron deficiency, rheumatoid arthritis, and pregnancy) and a recent history of alcohol or drug misuse or current evidence of substance use of < 1 year.
A patient list was compiled that included the etiology of the SCI (vascular injury, multiple sclerosis [MS], trauma, unknown, and other), the level(s) and completeness of the SCI per radiology report, RLS pharmacotherapies, and pertinent medical history.
Axial T2-weighted images on magnetic resonance imaging (MRI) scans were retrospectively reviewed. Sagittal T1/T2-weighted and axial T2-weighted sequences were performed routinely on all patients with spinal cord lesions. The analysis included the extension of the lesion on both sagittal and axial distributions. The anatomic location of the cord lesion was categorized by the following: (1) pure gray matter (central cord); (2) white matter (dorsal [D], dorsolateral [DL], ventral [V], ventrolateral areas [VL]).
A questionnaire using standard diagnostic criteria for RLS was mailed to the 199 patients who met the inclusion criteria (Appendix A).
All analyses were carried out using StataCorp STATA 13 (College Station, TX). Descriptive statistics were used. The analyses were carried out using chi-square and Fisher exact tests. Differences between the groups were considered statistically significant at P < .05. The data were analyzed to obtain point prevalence among patients with SCI, and comparisons were made among the different subgroups.
Results
Of the 162 patients who chose to participate in the study, the sleep specialists confirmed 31 (19%) to have RLS, 112 (69%) were confirmed negative for RLS, and an additional 19 (12%) screened positive for RLS but were not confirmed to have RLS by the sleep specialists (Figure 1).
The etiology of SCI was subdivided into 4 groups: MS, trauma, vascular, and other/unknown. Within each group (– RLS vs + RLS), MS and trauma were the most common etiologies with 55% MS and 36% trauma in the + RLS group.
When comparing RLS among the spinal cord levels (cervical, thoracic, lumbar and cervical + thoracic), only the cervical + thoracic subgroup (18% + RLS vs 5% – RLS) showed a significant difference (Figure 2).
There was no significant difference found with the prevalence of RLS in the axial plane of the spinal cord lesions (ventral/ventro-lateral/central cord vs dorsal/dorsolateral) or by the completeness of spinal cord lesions, P = .76. There was a higher prevalence of incomplete cord injury, however, within each subgroup of RLS.
The Mann-Whitney test was used to analyze the burden of disease in both groups (+ RLS vs – RLS). Moderate level of burden was most frequently reported with a higher prevalence within the + RLS group. Of those receiving treatment for RLS, 71% were + RLS vs 46% – RLS with a P value of .01. Symptoms of RLS after cord injury were 89% + RLS vs 55% – RLS with a P value of .03.
Discussion
This study represents one of the first studies to determine the prevalence of RLS in veterans with spinal cord disease. Research in this area is important to raise awareness of RLS among the veteran population with and without SCI and disorders. Restless legs syndrome often escapes diagnosis because of difficulty understanding the patient’s descriptions of their sensations. In addition, RLS may cause debilitating symptoms of sleep deprivation, daytime sleepiness, discomfort, and fatigue, which often results in decreased quality of life (QOL). Proper screening and treatment may improve QOL.
A study by Kumru and colleagues showed a similar rate of RLS in patients with SCI and RLS symptoms presented in the first year after SCI as did this study (18% vs 19%, respectively).4 In that study, RLS was more common in patients with lesions in lumbosacral area. Kumru and colleagues also showed that a dopaminergic medication improved symptoms of RLS in this population, whereas this study did not explore treatment outcomes.4
The pathogenesis of RLS is not fully known, but hereditary factors, iron metabolism, and the brain dopaminergic system are thought to be involved.11 It is hypothesized that spinal cord lesions allow the appearance of RLS symptoms and spinal leg movement generator by blocking descending inhibitory spinal pathways.12 One hypothesis is that damage to A11 nuclei (the main source of dopamine in the spinal cord or its diencephalospinal tract in animals) causes hyperexcitability of the spinal cord and leads to PLM and RLS symptoms.13 As the axons of A11 nuclei are present along the whole span of the spinal cord, SCI/D in patients with RLS might interrupt this dopaminergic tract and produce the RLS symptoms.
Limitations
This study included only veterans, so the prevalence may not apply to the nonveteran SCI population. Also, the population mainly was male, and there was no accurate information on race. Ferritin levels of the patients were not checked and is a major factor in RLS. The reported onset of RLS after the SCI could be due to recall bias.
Conclusion
The prevalence of RLS in veterans with SCI is above that reported in the general population (19% vs 10%, respectively). Furthermore, those with RLS have symptoms that often started after the SCI (suggesting causality) and required therapy due to their level of RLS symptom burden. A spectrum of severity of symptoms is present among those with RLS, with 83% having moderate-to-severe RLS affecting their QOL.
Although there was not a statistically significant relationship between RLS and spinal cord lesion level, there was a slightly higher prevalence of RLS at the cervical and thoracic levels, which may be relevant for future studies. There was no difference found between the RLS subgroups with respect to the location of the lesion within the spinal cord; however, a larger sample size may be needed to determine whether this would reach statistical significance. Prompt search for symptoms of RLS in veterans with SCI is warranted to provide adequate treatment to improve sleep health and QOL in this population.
1. Lasfargues JE, Custis D, Morrone F, Carswell J, Nguyen T. A model for estimating spinal cord injury prevalence in the United States. Paraplegia. 1995;33(2):62-68.
2. Sjölund BH. Pain and rehabilitation after spinal cord injury: the case of sensory spasticity? Brain Res Brain Res Rev. 2002;40(1-3):250-256.
3. Adams MM, Hicks AL. Spasticity after spinal cord injury. Spinal Cord. 2005;43(10):577-586.
4. Kumru H, Vidal J, Benito J, et al. Restless leg syndrome in patients with spinal cord injury. Parkinsonism Relat Disord. 2015;21(12):1461-1464.
5. Wilt TJ, MacDonald R, Ouellette J, et al. Pharmacologic therapy for primary restless legs syndrome: a systematic review and meta-analysis. JAMA Intern Med. 2013;173(7):496-505.
6. American Academy of Sleep Medicine. The International Classification of Sleep Disorders: Diagnostic and Coding Manual. (AASM ICSD-3). 3rd ed. Westchester, IL: American Academy of Sleep Medicine; 2014.
7. Telles SC, Alves RC, Chadi G. Periodic limb movements during sleep and restless legs syndrome in patients with ASIA A spinal cord injury. J Neurol Sci. 2011;303(1-2):119-123.
8. Telles SC, Alves RS, Chadi G. Spinal cord injury as a trigger to develop periodic leg movements during sleep: an evolutionary perspective. Arq Neuropsiquiatr. 2012;70(11):880-884.
9. Tings T, Baier PC, Paulus W, Trenkwalder C. Restless legs syndrome induced by impairment of sensory spinal pathways. J Neurol. 2003;250(4):499-500.
10. Paulus W, Trenkwalder C. Less is more: pathophysiology of dopaminergic-therapy-related augmentation in restless legs syndrome. Lancet Neurol. 2006;5(10):878-886.
11. Silber MH, Ehrenberg BL, Allen RP, et al; Medical Advisory Board of the Restless Legs Syndrome Foundation. An algorithm for the management of restless legs syndrome. Mayo Clin Proc. 2004;79(7):916-922.
12. Hartmann M, Pfister R, Pfadenhauer K. Restless legs syndrome associated with spinal cord lesions. J Neurol Neurosurg Psychiatry. 1999;66(5):688-689.
13. Clemens S, Rye D, Hochman S. Restless legs syndrome: revisiting the dopamine hypothesis from the spinal cord perspective. Neurology. 2006;67(1):125-130.
1. Lasfargues JE, Custis D, Morrone F, Carswell J, Nguyen T. A model for estimating spinal cord injury prevalence in the United States. Paraplegia. 1995;33(2):62-68.
2. Sjölund BH. Pain and rehabilitation after spinal cord injury: the case of sensory spasticity? Brain Res Brain Res Rev. 2002;40(1-3):250-256.
3. Adams MM, Hicks AL. Spasticity after spinal cord injury. Spinal Cord. 2005;43(10):577-586.
4. Kumru H, Vidal J, Benito J, et al. Restless leg syndrome in patients with spinal cord injury. Parkinsonism Relat Disord. 2015;21(12):1461-1464.
5. Wilt TJ, MacDonald R, Ouellette J, et al. Pharmacologic therapy for primary restless legs syndrome: a systematic review and meta-analysis. JAMA Intern Med. 2013;173(7):496-505.
6. American Academy of Sleep Medicine. The International Classification of Sleep Disorders: Diagnostic and Coding Manual. (AASM ICSD-3). 3rd ed. Westchester, IL: American Academy of Sleep Medicine; 2014.
7. Telles SC, Alves RC, Chadi G. Periodic limb movements during sleep and restless legs syndrome in patients with ASIA A spinal cord injury. J Neurol Sci. 2011;303(1-2):119-123.
8. Telles SC, Alves RS, Chadi G. Spinal cord injury as a trigger to develop periodic leg movements during sleep: an evolutionary perspective. Arq Neuropsiquiatr. 2012;70(11):880-884.
9. Tings T, Baier PC, Paulus W, Trenkwalder C. Restless legs syndrome induced by impairment of sensory spinal pathways. J Neurol. 2003;250(4):499-500.
10. Paulus W, Trenkwalder C. Less is more: pathophysiology of dopaminergic-therapy-related augmentation in restless legs syndrome. Lancet Neurol. 2006;5(10):878-886.
11. Silber MH, Ehrenberg BL, Allen RP, et al; Medical Advisory Board of the Restless Legs Syndrome Foundation. An algorithm for the management of restless legs syndrome. Mayo Clin Proc. 2004;79(7):916-922.
12. Hartmann M, Pfister R, Pfadenhauer K. Restless legs syndrome associated with spinal cord lesions. J Neurol Neurosurg Psychiatry. 1999;66(5):688-689.
13. Clemens S, Rye D, Hochman S. Restless legs syndrome: revisiting the dopamine hypothesis from the spinal cord perspective. Neurology. 2006;67(1):125-130.
The manipulative self-harmer
CASE: Self-destructive behaviors
After being acquitted of 4 counts of second-degree forgery for writing checks from her mother’s bank account, Ms. L, age 52, is sent to the state hospital for a forensic examination to determine competency. Two years later she is granted conditional release from the hospital, transferred to our not-for-profit community mental health center, and enrolled in an intensive inpatient treatment program to monitor forensic patients. She is legally required to comply with treatment recommendations.
At admission, Ms. L is diagnosed with major depression, recurrent, and borderline personality disorder (BPD). She has no history of antisocial behavior or criminal acts other than forging checks and has never spent time in prison, which makes it unlikely she has co morbid antisocial personality disorder (Table 1).1
Over the next 5 years Ms. L tests limits with the treatment team and acts out by engaging in self-harming behaviors. In 1 instance, she cuts her forearm deeply, stuffs the wound with mayonnaise and paper towels, and wraps her arm with a bandage. She wears a long-sleeved shirt to hide her wound, which is not discovered until a severe infection develops.
Ms. L has difficulty with coping skills and interpersonal relationships. She approaches others with ambivalence and mistrust and consistently expects them to demean or take advantage of her. Ms. L is manipulative, at times injuring herself after perceived wrongdoings by staff. For example, after her therapist reschedules a meeting because of an emergency, Ms. L pours scalding water on her foot.
Table 1
Cluster B personality disorders: Differential diagnosis
| Diagnosis | Features |
|---|---|
| Borderline personality disorder | Self-destructiveness, angry disruptions in close relationships, and chronic feelings of deep emptiness and loneliness |
| Histrionic personality disorder | Attention seeking, manipulative behavior, and rapidly shifting emotions |
| Antisocial personality disorder | Manipulative to gain profit, power, or other material gratification |
| Source: Reference 1 | |
The authors’ observations
Ms. L consistently displays 3 common constructs of BPD:
- primitive defense mechanisms
- identity diffusion
- generally intact reality testing.2
Defense mechanisms are psychological attempts to deal with intrapsychic stress. Splitting—vacillating between extremes of idealization and devaluation—is a fundamental primitive defense mechanism that is the root of BPD.2 Identity diffusion causes confusion about life goals and values and feelings of boredom and emptiness. This internal world leads a patient to have the same perception of the external world, which explains many symptoms of BPD, such as rapidly shifting moods, intense anger, lack of clear sense of self, fear of abandonment, and unstable and intense interpersonal relationships.2
Early in treatment, Ms. L had difficulty breaking a cycle of self-defeating behavior, such as destroying personal items, trying to hang herself, and gluing an ear plug in her ear. During an argument with a staff member, Ms. L punched a wall and fractured her left hand. BPD patients sometimes will “up the ante” when acting out. For example, one of our patients claimed to have planted a bomb in an elementary school and another swallowed inedible objects, including spoons, forks, and butter knives. In Ms. L’s case, we addressed her self-harm behavior by helping her:
- develop less destructive coping skills such as drawing or painting
- identify irrational thoughts that contribute to self harm.
HISTORY: Troubled past
Raised by her biologic parents, Ms. L met all developmental milestones. She denies a history of childhood abuse but reports experiencing “depression and memory loss” and relationship problems with her parents during adolescence. As a child she often missed school because she “did not want anyone to know what a disgusting person I was” and “I should have my head cut open and cut into little pieces for thinking such mean thoughts.” Ms. L dropped out of school in the twelfth grade but obtained her general educational development certificate.
Notes and letters Ms. L wrote while in treatment consistently refer to her negative self-image. Ms. L writes that she feels she does not deserve to “be a part of this world,” is “never good enough for anyone,” and “should be thrown away with the garbage.”
Ms. L vacillates between desiring a closer relationship with her parents, especially her mother, and wanting to “cut them out of my life for good.” She has minimal contact with her older sister. Ms. L is divorced and has 2 adult sons. She was involved sporadically in her sons’ lives when they were children, but now has no contact with them.
BPD and crime
Ms. L is enrolled in the “911 program,” which monitors individuals who have been found not guilty by reason of mental defect. Individuals with BPD often are convicted of serious and violent crimes, which may be because of BPD features such as interpersonal hostility and self-harm. Impulsivity, substance abuse, and parental neglect—all of which are associated with BPD—can increase risk of criminality.3 There is no evidence to suggest a direct link between BPD and criminality; however, over-representation of BPD in prison populations suggest that in severe cases it may increase criminogenic risk.1,3
TREATMENT: Worsened depression
When Ms. L arrives at our facility, her medication regimen includes fluoxetine, 80 mg/d, risperidone, 2 mg/d, and buspirone, 20 mg/d. Risperidone and buspirone are discontinued because of perceived lack of efficacy. Venlafaxine XR is added and titrated to 300 mg/d, and Ms. L receives lorazepam, 1 and 2 mg as needed. However, lorazepam carries risks because impulsivity and impaired judgment—which are common in BPD—can lead to dependence and abuse. We feel that in a supervised setting the risks can be managed.
Recently, staff witnessed Ms. L experiencing an episode that appeared to be a grand mal seizure. After Ms. L is evaluated at the local emergency room, her EEG is normal, but a neurologic consult recommends discontinuing fluoxetine or venlafaxine XR because they may have contributed to the seizure. We taper and discontinue venlafaxine XR but Ms. L complains bitterly that she is getting increasingly depressed. On several occasions she attempts to pit team members against each other.
Ms. L falls, injures her back, and begins to abuse opiates. After her prescription runs out, she obtains more from an intellectually limited patient in her treatment program. Ms. L says she is getting more depressed, threatens suicide, and is placed in a more restrictive in-patient setting. We consider adding pregabalin to address her pain and help with anxiety and impulse control but the consulting neurologist prescribes carbamazepine, 400 mg/d, and her pain improves.5,6
The authors’ observations
BPD treatment primarily is psychotherapeutic and emphasizes skill building (Table 2) with focused, symptom-targeted pharmacotherapy as indicated.4 Pharmacotherapy typically targets 3 domains:
- affective dysregulation
- impulsive-behavioral dyscontrol symptoms
- cognitive-perceptual symptoms.
Patients with prominent anxiety may benefit from benzodiazepines, although research on these agents for BPD is limited. Recent studies show efficacy with fluoxetine, olanzapine, or a combination of both,7 and divalproex.8 Preliminary data supports the use of topiramate, quetiapine, risperidone, ziprasidone, lamotrigine, and clonidine (Table 3).9-14 A recent review and meta-analysis showed efficacy with topira-mate, lamotrigine, valproate, aripiprazole, and olanzapine.15
For Ms. L, we restart venlafaxine at a lower dose of 50 mg/d and titrate it to 150 mg/d, which is still lower than her previous dose of 300 mg/d. She has no recurrence of seizures and her depression improves.
Table 2
Features of psychotherapeutic modalities for BPD
| Description | Mode of treatment | Skills taught | |
|---|---|---|---|
| Dialectical behavior therapy | Manualized, time-limited, cognitive-behavioral approach based on the biosocial theory of BPD | Individual therapy, group skills training, telephone contact, and therapist consultation | Core mindfulness skills, interpersonal effectiveness skills, emotion modulation skills, and distress tolerance skills |
| Systems Training for Emotional Predictability and Problem Solving | Manual-based, group treatment that includes a systems component to train family members, friends, and significant others | 20-week basic skills group and a 1-year, twice-monthly advanced group program; utilizes a classroom ‘seminar’ format | Awareness of illness, emotion management skills, and behavior management skills |
| BPD: borderline personality disorder | |||
Table 3
Pharmacotherapy for BPD: What the evidence says
| Study | Design | Results |
|---|---|---|
| Hollander et al, 20039 | 96 patients with Cluster B personality disorders randomized to divalproex or placebo for 12 weeks | Divalproex was superior to placebo in treating impulsive aggression, irritability, and global severity |
| Hilger et al, 200310 | Case report of 2 women with BPD and severe self-mutilation receiving quetiapine monotherapy | Quetiapine resulted in a marked improvement of impulsive behavior and overall level of function |
| Rizvi, 200211 | Case report of a 14-year-old female with borderline personality traits admitted to an inpatient facility for suicide attempt, impulsive behavior, and mood lability. Lamotrigine was started at 25 mg/d and titrated to 200 mg/d. At admission, she was receiving clonazepam, valproic acid, quetiapine, and fluoxetine, which were tapered and discontinued | Over 6 months of inpatient treatment, suicidal behavior and ideation diminished and impulse control and mood lability improved; continued improvement at 1-year follow up |
| Rocca et al, 200212 | 15 BPD outpatients with aggressive behavior given risperidone (mean dose 3.27 mg/d) in an 8-week open-label study | Risperidone produced a significant reduction in aggression based on AQ scores, reduction in depressive symptoms, and an increase in energy and global functioning |
| Philipsen et al, 200413 | 14 women with BPD given oral clonidine, 75 and 150 µg, while experiencing strong aversive inner tension and urge to commit self-injury | Clonidine significantly decreased aversive inner tension, dissociative symptoms, and urge to commit self-injury as measured by self rated scales |
| Pascual et al, 200414 | A 2-week open-label study of 10 females and 2 males presenting to psychiatric emergency service for self-injurious behavior, aggression/hostility, loss of impulse control, and severe anxiety/depressive symptoms received IM ziprasidone, 20 mg, followed by flexible oral dosing between 40 mg/d and 160 mg/d | 9 patients who completed the study showed statistically significant improvements on CGI-S, HAM-D-17, HAM-A, BPRS, and BIS |
| AQ: Aggression Questionnaire; BIS: Barratt Impulsiveness Scale; BPD: borderline personality disorder; BPRS: Brief Psychiatric Rating Scale; CGI-S: Clinical Global Impressions-Severity of Illness; HAM-A: Hamilton Anxiety Rating scale; HAM-D-17: 17-item Hamilton Depression Rating scale | ||
OUTCOME: Some improvement
Ms. L has no dramatic suicidal gestures for 3 years. Although she continues to engage in self-injurious behaviors, the intensity and frequency are reduced and she does not inflict any serious injury for 18 months. Her mood and behavior continue to oscillate; she is relatively calm and satisfied 1 week, angry and assaultive the next. This stormy course is expected given her BPD diagnosis.
Initially, Ms. L resided in a locked residential unit and was minimally compliant with treatment recommendations and unit policies. As treatment progressed she moved to a different locked unit and eventually to an apartment. Recently, she was placed in a more restrictive setting because her hostile and self-destructive behavior escalated.
The authors’ observations
Ms. L is no different from most Axis II Cluster B disordered patients. During treatment she shows improvement by refraining from self-destructive behaviors for up to 18 months, but she then briefly reverts back to maladaptive behaviors. Ms. L resides in a very structured treatment setting. It is not clear if the gains she made in treatment would have been possible if she was living on her own in the community.
One year after finishing the court-mandated “911 program,” Ms. L lives in the community, draws and paints quite well, attends weekly individual and group therapy, and refrains from self-mutilation. She still experiences volatile moods, but can handle them without inflicting self injury.
Related resources
- Oldham JM. Guideline watch: practice guideline for the treatment of patients with borderline personality disorder. Arlington, VA: American Psychiatric Association; 2005. www.psychiatryonline.com/content.aspx?aID=148722.
- Koenigsberg HW, Kernberg OF, Stone MH, et al. Borderline patients: extending the limits of treatability. New York, NY: Basic Books; 2000.
Drug brand names
- Aripiprazole • Abilify
- Buspirone • Buspar
- Carbamazepine • Tegretol
- Clonidine • Catapres
- Divalproex • Depakote
- Fluoxetine • Prozac
- Fluoxetine-olanzapine • Symbyax
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Pregabalin • Lyrica
- Risperidone • Risperdal
- Topiramate • Topamax
- Valproic acid • Depakene
- Venlafaxine XR • Effexor XR
- Ziprasidone • Geodon
Disclosures
Dr. Hashmi is on the speakers bureau for AstraZeneca, Eli Lilly and Company, and Janssen.
Dr. Vowell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Diagnostic and statistical manual of mental disorders, 4th ed, text revision. Washington, DC: American Psychiatric Association; 2000.
2. Koenigsberg HW, Kernberg OF, Stone MH, et al. Borderline patients: extending the limits of treatability. New York, NY: Basic Books; 2000.
3. Nee C, Farman S. Female prisoners with borderline personality disorder: some promising treatment developments. Crim Behav Ment Health. 2005;15:2-16.
4. Oldham JM, Bender DS, Skodol AE, et al. Testing an APA practice guideline: symptom-targeted medication utilization for patients with borderline personality disorder. J Psychiatr Pract. 2004;10:156-161.
5. American Psychiatric Association Practice Guidelines. Practice guideline for the treatment of patients with borderline personality disorder. Am J Psychiatry. 2001;158(suppl 10):1-52.
6. Yatham LN. Newer anticonvulsants in the treatment of bipolar disorder. J Clin Psychiatry. 2004;65(suppl 10):28-35.
7. Rinne T, van den Brink W, Wouters L, et al. SSRI treatment of borderline personality disorder: a randomized, placebo-controlled clinical trial for female patients with borderline personality disorder. Am J Psychiatry. 2002;159(12):2048-2054.
8. Zanarini MC, Frankenburg FR, Parachini EA. A preliminary, randomized trial of fluoxetine, olanzapine, and the olanzapine-fluoxetine combination in women with borderline personality disorder. J Clin Psychiatry. 2004;65(7):903-907.
9. Hollander E, Tracy KA, Swann AC, et al. Divalproex in the treatment of impulsive aggression: efficacy in cluster B personality disorders. Neuropsychopharmacology. 2003;28(6):1186-1197.
10. Hilger E, Barnas C, Kasper S. Quetiapine in the treatment of borderline personality disorder. World J Biol Psychiatry. 2003;4(1):42-44.
11. Rizvi ST. Lamotrigine and borderline personality disorder. J Child Adolesc Psychopharmacol. 2002;12(4):365-366.
12. Rocca P, Marchiaro L, Cocuzza E, et al. Treatment of borderline personality disorder with risperidone. J Clin Psychiatry. 2002;63(3):241-244.
13. Philipsen A, Richter H, Schmahl C, et al. Clonidine in acute aversive inner tension and self-injurious behavior in female patients with borderline personality disorder. J Clin Psychiatry. 2004;65(10):1414-1419.
14. Pascual JC, Oller S, Soler J, et al. Ziprasidone in the acute treatment of borderline personality disorder in psychiatric emergency services. J Clin Psychiatry. 2004;65(9):1281-1282.
15. Lieb K, Völlm B, Rücker G, et al. Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials. Br J Psychiatry. 2010;196(1):4-12.
CASE: Self-destructive behaviors
After being acquitted of 4 counts of second-degree forgery for writing checks from her mother’s bank account, Ms. L, age 52, is sent to the state hospital for a forensic examination to determine competency. Two years later she is granted conditional release from the hospital, transferred to our not-for-profit community mental health center, and enrolled in an intensive inpatient treatment program to monitor forensic patients. She is legally required to comply with treatment recommendations.
At admission, Ms. L is diagnosed with major depression, recurrent, and borderline personality disorder (BPD). She has no history of antisocial behavior or criminal acts other than forging checks and has never spent time in prison, which makes it unlikely she has co morbid antisocial personality disorder (Table 1).1
Over the next 5 years Ms. L tests limits with the treatment team and acts out by engaging in self-harming behaviors. In 1 instance, she cuts her forearm deeply, stuffs the wound with mayonnaise and paper towels, and wraps her arm with a bandage. She wears a long-sleeved shirt to hide her wound, which is not discovered until a severe infection develops.
Ms. L has difficulty with coping skills and interpersonal relationships. She approaches others with ambivalence and mistrust and consistently expects them to demean or take advantage of her. Ms. L is manipulative, at times injuring herself after perceived wrongdoings by staff. For example, after her therapist reschedules a meeting because of an emergency, Ms. L pours scalding water on her foot.
Table 1
Cluster B personality disorders: Differential diagnosis
| Diagnosis | Features |
|---|---|
| Borderline personality disorder | Self-destructiveness, angry disruptions in close relationships, and chronic feelings of deep emptiness and loneliness |
| Histrionic personality disorder | Attention seeking, manipulative behavior, and rapidly shifting emotions |
| Antisocial personality disorder | Manipulative to gain profit, power, or other material gratification |
| Source: Reference 1 | |
The authors’ observations
Ms. L consistently displays 3 common constructs of BPD:
- primitive defense mechanisms
- identity diffusion
- generally intact reality testing.2
Defense mechanisms are psychological attempts to deal with intrapsychic stress. Splitting—vacillating between extremes of idealization and devaluation—is a fundamental primitive defense mechanism that is the root of BPD.2 Identity diffusion causes confusion about life goals and values and feelings of boredom and emptiness. This internal world leads a patient to have the same perception of the external world, which explains many symptoms of BPD, such as rapidly shifting moods, intense anger, lack of clear sense of self, fear of abandonment, and unstable and intense interpersonal relationships.2
Early in treatment, Ms. L had difficulty breaking a cycle of self-defeating behavior, such as destroying personal items, trying to hang herself, and gluing an ear plug in her ear. During an argument with a staff member, Ms. L punched a wall and fractured her left hand. BPD patients sometimes will “up the ante” when acting out. For example, one of our patients claimed to have planted a bomb in an elementary school and another swallowed inedible objects, including spoons, forks, and butter knives. In Ms. L’s case, we addressed her self-harm behavior by helping her:
- develop less destructive coping skills such as drawing or painting
- identify irrational thoughts that contribute to self harm.
HISTORY: Troubled past
Raised by her biologic parents, Ms. L met all developmental milestones. She denies a history of childhood abuse but reports experiencing “depression and memory loss” and relationship problems with her parents during adolescence. As a child she often missed school because she “did not want anyone to know what a disgusting person I was” and “I should have my head cut open and cut into little pieces for thinking such mean thoughts.” Ms. L dropped out of school in the twelfth grade but obtained her general educational development certificate.
Notes and letters Ms. L wrote while in treatment consistently refer to her negative self-image. Ms. L writes that she feels she does not deserve to “be a part of this world,” is “never good enough for anyone,” and “should be thrown away with the garbage.”
Ms. L vacillates between desiring a closer relationship with her parents, especially her mother, and wanting to “cut them out of my life for good.” She has minimal contact with her older sister. Ms. L is divorced and has 2 adult sons. She was involved sporadically in her sons’ lives when they were children, but now has no contact with them.
BPD and crime
Ms. L is enrolled in the “911 program,” which monitors individuals who have been found not guilty by reason of mental defect. Individuals with BPD often are convicted of serious and violent crimes, which may be because of BPD features such as interpersonal hostility and self-harm. Impulsivity, substance abuse, and parental neglect—all of which are associated with BPD—can increase risk of criminality.3 There is no evidence to suggest a direct link between BPD and criminality; however, over-representation of BPD in prison populations suggest that in severe cases it may increase criminogenic risk.1,3
TREATMENT: Worsened depression
When Ms. L arrives at our facility, her medication regimen includes fluoxetine, 80 mg/d, risperidone, 2 mg/d, and buspirone, 20 mg/d. Risperidone and buspirone are discontinued because of perceived lack of efficacy. Venlafaxine XR is added and titrated to 300 mg/d, and Ms. L receives lorazepam, 1 and 2 mg as needed. However, lorazepam carries risks because impulsivity and impaired judgment—which are common in BPD—can lead to dependence and abuse. We feel that in a supervised setting the risks can be managed.
Recently, staff witnessed Ms. L experiencing an episode that appeared to be a grand mal seizure. After Ms. L is evaluated at the local emergency room, her EEG is normal, but a neurologic consult recommends discontinuing fluoxetine or venlafaxine XR because they may have contributed to the seizure. We taper and discontinue venlafaxine XR but Ms. L complains bitterly that she is getting increasingly depressed. On several occasions she attempts to pit team members against each other.
Ms. L falls, injures her back, and begins to abuse opiates. After her prescription runs out, she obtains more from an intellectually limited patient in her treatment program. Ms. L says she is getting more depressed, threatens suicide, and is placed in a more restrictive in-patient setting. We consider adding pregabalin to address her pain and help with anxiety and impulse control but the consulting neurologist prescribes carbamazepine, 400 mg/d, and her pain improves.5,6
The authors’ observations
BPD treatment primarily is psychotherapeutic and emphasizes skill building (Table 2) with focused, symptom-targeted pharmacotherapy as indicated.4 Pharmacotherapy typically targets 3 domains:
- affective dysregulation
- impulsive-behavioral dyscontrol symptoms
- cognitive-perceptual symptoms.
Patients with prominent anxiety may benefit from benzodiazepines, although research on these agents for BPD is limited. Recent studies show efficacy with fluoxetine, olanzapine, or a combination of both,7 and divalproex.8 Preliminary data supports the use of topiramate, quetiapine, risperidone, ziprasidone, lamotrigine, and clonidine (Table 3).9-14 A recent review and meta-analysis showed efficacy with topira-mate, lamotrigine, valproate, aripiprazole, and olanzapine.15
For Ms. L, we restart venlafaxine at a lower dose of 50 mg/d and titrate it to 150 mg/d, which is still lower than her previous dose of 300 mg/d. She has no recurrence of seizures and her depression improves.
Table 2
Features of psychotherapeutic modalities for BPD
| Description | Mode of treatment | Skills taught | |
|---|---|---|---|
| Dialectical behavior therapy | Manualized, time-limited, cognitive-behavioral approach based on the biosocial theory of BPD | Individual therapy, group skills training, telephone contact, and therapist consultation | Core mindfulness skills, interpersonal effectiveness skills, emotion modulation skills, and distress tolerance skills |
| Systems Training for Emotional Predictability and Problem Solving | Manual-based, group treatment that includes a systems component to train family members, friends, and significant others | 20-week basic skills group and a 1-year, twice-monthly advanced group program; utilizes a classroom ‘seminar’ format | Awareness of illness, emotion management skills, and behavior management skills |
| BPD: borderline personality disorder | |||
Table 3
Pharmacotherapy for BPD: What the evidence says
| Study | Design | Results |
|---|---|---|
| Hollander et al, 20039 | 96 patients with Cluster B personality disorders randomized to divalproex or placebo for 12 weeks | Divalproex was superior to placebo in treating impulsive aggression, irritability, and global severity |
| Hilger et al, 200310 | Case report of 2 women with BPD and severe self-mutilation receiving quetiapine monotherapy | Quetiapine resulted in a marked improvement of impulsive behavior and overall level of function |
| Rizvi, 200211 | Case report of a 14-year-old female with borderline personality traits admitted to an inpatient facility for suicide attempt, impulsive behavior, and mood lability. Lamotrigine was started at 25 mg/d and titrated to 200 mg/d. At admission, she was receiving clonazepam, valproic acid, quetiapine, and fluoxetine, which were tapered and discontinued | Over 6 months of inpatient treatment, suicidal behavior and ideation diminished and impulse control and mood lability improved; continued improvement at 1-year follow up |
| Rocca et al, 200212 | 15 BPD outpatients with aggressive behavior given risperidone (mean dose 3.27 mg/d) in an 8-week open-label study | Risperidone produced a significant reduction in aggression based on AQ scores, reduction in depressive symptoms, and an increase in energy and global functioning |
| Philipsen et al, 200413 | 14 women with BPD given oral clonidine, 75 and 150 µg, while experiencing strong aversive inner tension and urge to commit self-injury | Clonidine significantly decreased aversive inner tension, dissociative symptoms, and urge to commit self-injury as measured by self rated scales |
| Pascual et al, 200414 | A 2-week open-label study of 10 females and 2 males presenting to psychiatric emergency service for self-injurious behavior, aggression/hostility, loss of impulse control, and severe anxiety/depressive symptoms received IM ziprasidone, 20 mg, followed by flexible oral dosing between 40 mg/d and 160 mg/d | 9 patients who completed the study showed statistically significant improvements on CGI-S, HAM-D-17, HAM-A, BPRS, and BIS |
| AQ: Aggression Questionnaire; BIS: Barratt Impulsiveness Scale; BPD: borderline personality disorder; BPRS: Brief Psychiatric Rating Scale; CGI-S: Clinical Global Impressions-Severity of Illness; HAM-A: Hamilton Anxiety Rating scale; HAM-D-17: 17-item Hamilton Depression Rating scale | ||
OUTCOME: Some improvement
Ms. L has no dramatic suicidal gestures for 3 years. Although she continues to engage in self-injurious behaviors, the intensity and frequency are reduced and she does not inflict any serious injury for 18 months. Her mood and behavior continue to oscillate; she is relatively calm and satisfied 1 week, angry and assaultive the next. This stormy course is expected given her BPD diagnosis.
Initially, Ms. L resided in a locked residential unit and was minimally compliant with treatment recommendations and unit policies. As treatment progressed she moved to a different locked unit and eventually to an apartment. Recently, she was placed in a more restrictive setting because her hostile and self-destructive behavior escalated.
The authors’ observations
Ms. L is no different from most Axis II Cluster B disordered patients. During treatment she shows improvement by refraining from self-destructive behaviors for up to 18 months, but she then briefly reverts back to maladaptive behaviors. Ms. L resides in a very structured treatment setting. It is not clear if the gains she made in treatment would have been possible if she was living on her own in the community.
One year after finishing the court-mandated “911 program,” Ms. L lives in the community, draws and paints quite well, attends weekly individual and group therapy, and refrains from self-mutilation. She still experiences volatile moods, but can handle them without inflicting self injury.
Related resources
- Oldham JM. Guideline watch: practice guideline for the treatment of patients with borderline personality disorder. Arlington, VA: American Psychiatric Association; 2005. www.psychiatryonline.com/content.aspx?aID=148722.
- Koenigsberg HW, Kernberg OF, Stone MH, et al. Borderline patients: extending the limits of treatability. New York, NY: Basic Books; 2000.
Drug brand names
- Aripiprazole • Abilify
- Buspirone • Buspar
- Carbamazepine • Tegretol
- Clonidine • Catapres
- Divalproex • Depakote
- Fluoxetine • Prozac
- Fluoxetine-olanzapine • Symbyax
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Pregabalin • Lyrica
- Risperidone • Risperdal
- Topiramate • Topamax
- Valproic acid • Depakene
- Venlafaxine XR • Effexor XR
- Ziprasidone • Geodon
Disclosures
Dr. Hashmi is on the speakers bureau for AstraZeneca, Eli Lilly and Company, and Janssen.
Dr. Vowell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Self-destructive behaviors
After being acquitted of 4 counts of second-degree forgery for writing checks from her mother’s bank account, Ms. L, age 52, is sent to the state hospital for a forensic examination to determine competency. Two years later she is granted conditional release from the hospital, transferred to our not-for-profit community mental health center, and enrolled in an intensive inpatient treatment program to monitor forensic patients. She is legally required to comply with treatment recommendations.
At admission, Ms. L is diagnosed with major depression, recurrent, and borderline personality disorder (BPD). She has no history of antisocial behavior or criminal acts other than forging checks and has never spent time in prison, which makes it unlikely she has co morbid antisocial personality disorder (Table 1).1
Over the next 5 years Ms. L tests limits with the treatment team and acts out by engaging in self-harming behaviors. In 1 instance, she cuts her forearm deeply, stuffs the wound with mayonnaise and paper towels, and wraps her arm with a bandage. She wears a long-sleeved shirt to hide her wound, which is not discovered until a severe infection develops.
Ms. L has difficulty with coping skills and interpersonal relationships. She approaches others with ambivalence and mistrust and consistently expects them to demean or take advantage of her. Ms. L is manipulative, at times injuring herself after perceived wrongdoings by staff. For example, after her therapist reschedules a meeting because of an emergency, Ms. L pours scalding water on her foot.
Table 1
Cluster B personality disorders: Differential diagnosis
| Diagnosis | Features |
|---|---|
| Borderline personality disorder | Self-destructiveness, angry disruptions in close relationships, and chronic feelings of deep emptiness and loneliness |
| Histrionic personality disorder | Attention seeking, manipulative behavior, and rapidly shifting emotions |
| Antisocial personality disorder | Manipulative to gain profit, power, or other material gratification |
| Source: Reference 1 | |
The authors’ observations
Ms. L consistently displays 3 common constructs of BPD:
- primitive defense mechanisms
- identity diffusion
- generally intact reality testing.2
Defense mechanisms are psychological attempts to deal with intrapsychic stress. Splitting—vacillating between extremes of idealization and devaluation—is a fundamental primitive defense mechanism that is the root of BPD.2 Identity diffusion causes confusion about life goals and values and feelings of boredom and emptiness. This internal world leads a patient to have the same perception of the external world, which explains many symptoms of BPD, such as rapidly shifting moods, intense anger, lack of clear sense of self, fear of abandonment, and unstable and intense interpersonal relationships.2
Early in treatment, Ms. L had difficulty breaking a cycle of self-defeating behavior, such as destroying personal items, trying to hang herself, and gluing an ear plug in her ear. During an argument with a staff member, Ms. L punched a wall and fractured her left hand. BPD patients sometimes will “up the ante” when acting out. For example, one of our patients claimed to have planted a bomb in an elementary school and another swallowed inedible objects, including spoons, forks, and butter knives. In Ms. L’s case, we addressed her self-harm behavior by helping her:
- develop less destructive coping skills such as drawing or painting
- identify irrational thoughts that contribute to self harm.
HISTORY: Troubled past
Raised by her biologic parents, Ms. L met all developmental milestones. She denies a history of childhood abuse but reports experiencing “depression and memory loss” and relationship problems with her parents during adolescence. As a child she often missed school because she “did not want anyone to know what a disgusting person I was” and “I should have my head cut open and cut into little pieces for thinking such mean thoughts.” Ms. L dropped out of school in the twelfth grade but obtained her general educational development certificate.
Notes and letters Ms. L wrote while in treatment consistently refer to her negative self-image. Ms. L writes that she feels she does not deserve to “be a part of this world,” is “never good enough for anyone,” and “should be thrown away with the garbage.”
Ms. L vacillates between desiring a closer relationship with her parents, especially her mother, and wanting to “cut them out of my life for good.” She has minimal contact with her older sister. Ms. L is divorced and has 2 adult sons. She was involved sporadically in her sons’ lives when they were children, but now has no contact with them.
BPD and crime
Ms. L is enrolled in the “911 program,” which monitors individuals who have been found not guilty by reason of mental defect. Individuals with BPD often are convicted of serious and violent crimes, which may be because of BPD features such as interpersonal hostility and self-harm. Impulsivity, substance abuse, and parental neglect—all of which are associated with BPD—can increase risk of criminality.3 There is no evidence to suggest a direct link between BPD and criminality; however, over-representation of BPD in prison populations suggest that in severe cases it may increase criminogenic risk.1,3
TREATMENT: Worsened depression
When Ms. L arrives at our facility, her medication regimen includes fluoxetine, 80 mg/d, risperidone, 2 mg/d, and buspirone, 20 mg/d. Risperidone and buspirone are discontinued because of perceived lack of efficacy. Venlafaxine XR is added and titrated to 300 mg/d, and Ms. L receives lorazepam, 1 and 2 mg as needed. However, lorazepam carries risks because impulsivity and impaired judgment—which are common in BPD—can lead to dependence and abuse. We feel that in a supervised setting the risks can be managed.
Recently, staff witnessed Ms. L experiencing an episode that appeared to be a grand mal seizure. After Ms. L is evaluated at the local emergency room, her EEG is normal, but a neurologic consult recommends discontinuing fluoxetine or venlafaxine XR because they may have contributed to the seizure. We taper and discontinue venlafaxine XR but Ms. L complains bitterly that she is getting increasingly depressed. On several occasions she attempts to pit team members against each other.
Ms. L falls, injures her back, and begins to abuse opiates. After her prescription runs out, she obtains more from an intellectually limited patient in her treatment program. Ms. L says she is getting more depressed, threatens suicide, and is placed in a more restrictive in-patient setting. We consider adding pregabalin to address her pain and help with anxiety and impulse control but the consulting neurologist prescribes carbamazepine, 400 mg/d, and her pain improves.5,6
The authors’ observations
BPD treatment primarily is psychotherapeutic and emphasizes skill building (Table 2) with focused, symptom-targeted pharmacotherapy as indicated.4 Pharmacotherapy typically targets 3 domains:
- affective dysregulation
- impulsive-behavioral dyscontrol symptoms
- cognitive-perceptual symptoms.
Patients with prominent anxiety may benefit from benzodiazepines, although research on these agents for BPD is limited. Recent studies show efficacy with fluoxetine, olanzapine, or a combination of both,7 and divalproex.8 Preliminary data supports the use of topiramate, quetiapine, risperidone, ziprasidone, lamotrigine, and clonidine (Table 3).9-14 A recent review and meta-analysis showed efficacy with topira-mate, lamotrigine, valproate, aripiprazole, and olanzapine.15
For Ms. L, we restart venlafaxine at a lower dose of 50 mg/d and titrate it to 150 mg/d, which is still lower than her previous dose of 300 mg/d. She has no recurrence of seizures and her depression improves.
Table 2
Features of psychotherapeutic modalities for BPD
| Description | Mode of treatment | Skills taught | |
|---|---|---|---|
| Dialectical behavior therapy | Manualized, time-limited, cognitive-behavioral approach based on the biosocial theory of BPD | Individual therapy, group skills training, telephone contact, and therapist consultation | Core mindfulness skills, interpersonal effectiveness skills, emotion modulation skills, and distress tolerance skills |
| Systems Training for Emotional Predictability and Problem Solving | Manual-based, group treatment that includes a systems component to train family members, friends, and significant others | 20-week basic skills group and a 1-year, twice-monthly advanced group program; utilizes a classroom ‘seminar’ format | Awareness of illness, emotion management skills, and behavior management skills |
| BPD: borderline personality disorder | |||
Table 3
Pharmacotherapy for BPD: What the evidence says
| Study | Design | Results |
|---|---|---|
| Hollander et al, 20039 | 96 patients with Cluster B personality disorders randomized to divalproex or placebo for 12 weeks | Divalproex was superior to placebo in treating impulsive aggression, irritability, and global severity |
| Hilger et al, 200310 | Case report of 2 women with BPD and severe self-mutilation receiving quetiapine monotherapy | Quetiapine resulted in a marked improvement of impulsive behavior and overall level of function |
| Rizvi, 200211 | Case report of a 14-year-old female with borderline personality traits admitted to an inpatient facility for suicide attempt, impulsive behavior, and mood lability. Lamotrigine was started at 25 mg/d and titrated to 200 mg/d. At admission, she was receiving clonazepam, valproic acid, quetiapine, and fluoxetine, which were tapered and discontinued | Over 6 months of inpatient treatment, suicidal behavior and ideation diminished and impulse control and mood lability improved; continued improvement at 1-year follow up |
| Rocca et al, 200212 | 15 BPD outpatients with aggressive behavior given risperidone (mean dose 3.27 mg/d) in an 8-week open-label study | Risperidone produced a significant reduction in aggression based on AQ scores, reduction in depressive symptoms, and an increase in energy and global functioning |
| Philipsen et al, 200413 | 14 women with BPD given oral clonidine, 75 and 150 µg, while experiencing strong aversive inner tension and urge to commit self-injury | Clonidine significantly decreased aversive inner tension, dissociative symptoms, and urge to commit self-injury as measured by self rated scales |
| Pascual et al, 200414 | A 2-week open-label study of 10 females and 2 males presenting to psychiatric emergency service for self-injurious behavior, aggression/hostility, loss of impulse control, and severe anxiety/depressive symptoms received IM ziprasidone, 20 mg, followed by flexible oral dosing between 40 mg/d and 160 mg/d | 9 patients who completed the study showed statistically significant improvements on CGI-S, HAM-D-17, HAM-A, BPRS, and BIS |
| AQ: Aggression Questionnaire; BIS: Barratt Impulsiveness Scale; BPD: borderline personality disorder; BPRS: Brief Psychiatric Rating Scale; CGI-S: Clinical Global Impressions-Severity of Illness; HAM-A: Hamilton Anxiety Rating scale; HAM-D-17: 17-item Hamilton Depression Rating scale | ||
OUTCOME: Some improvement
Ms. L has no dramatic suicidal gestures for 3 years. Although she continues to engage in self-injurious behaviors, the intensity and frequency are reduced and she does not inflict any serious injury for 18 months. Her mood and behavior continue to oscillate; she is relatively calm and satisfied 1 week, angry and assaultive the next. This stormy course is expected given her BPD diagnosis.
Initially, Ms. L resided in a locked residential unit and was minimally compliant with treatment recommendations and unit policies. As treatment progressed she moved to a different locked unit and eventually to an apartment. Recently, she was placed in a more restrictive setting because her hostile and self-destructive behavior escalated.
The authors’ observations
Ms. L is no different from most Axis II Cluster B disordered patients. During treatment she shows improvement by refraining from self-destructive behaviors for up to 18 months, but she then briefly reverts back to maladaptive behaviors. Ms. L resides in a very structured treatment setting. It is not clear if the gains she made in treatment would have been possible if she was living on her own in the community.
One year after finishing the court-mandated “911 program,” Ms. L lives in the community, draws and paints quite well, attends weekly individual and group therapy, and refrains from self-mutilation. She still experiences volatile moods, but can handle them without inflicting self injury.
Related resources
- Oldham JM. Guideline watch: practice guideline for the treatment of patients with borderline personality disorder. Arlington, VA: American Psychiatric Association; 2005. www.psychiatryonline.com/content.aspx?aID=148722.
- Koenigsberg HW, Kernberg OF, Stone MH, et al. Borderline patients: extending the limits of treatability. New York, NY: Basic Books; 2000.
Drug brand names
- Aripiprazole • Abilify
- Buspirone • Buspar
- Carbamazepine • Tegretol
- Clonidine • Catapres
- Divalproex • Depakote
- Fluoxetine • Prozac
- Fluoxetine-olanzapine • Symbyax
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Pregabalin • Lyrica
- Risperidone • Risperdal
- Topiramate • Topamax
- Valproic acid • Depakene
- Venlafaxine XR • Effexor XR
- Ziprasidone • Geodon
Disclosures
Dr. Hashmi is on the speakers bureau for AstraZeneca, Eli Lilly and Company, and Janssen.
Dr. Vowell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Diagnostic and statistical manual of mental disorders, 4th ed, text revision. Washington, DC: American Psychiatric Association; 2000.
2. Koenigsberg HW, Kernberg OF, Stone MH, et al. Borderline patients: extending the limits of treatability. New York, NY: Basic Books; 2000.
3. Nee C, Farman S. Female prisoners with borderline personality disorder: some promising treatment developments. Crim Behav Ment Health. 2005;15:2-16.
4. Oldham JM, Bender DS, Skodol AE, et al. Testing an APA practice guideline: symptom-targeted medication utilization for patients with borderline personality disorder. J Psychiatr Pract. 2004;10:156-161.
5. American Psychiatric Association Practice Guidelines. Practice guideline for the treatment of patients with borderline personality disorder. Am J Psychiatry. 2001;158(suppl 10):1-52.
6. Yatham LN. Newer anticonvulsants in the treatment of bipolar disorder. J Clin Psychiatry. 2004;65(suppl 10):28-35.
7. Rinne T, van den Brink W, Wouters L, et al. SSRI treatment of borderline personality disorder: a randomized, placebo-controlled clinical trial for female patients with borderline personality disorder. Am J Psychiatry. 2002;159(12):2048-2054.
8. Zanarini MC, Frankenburg FR, Parachini EA. A preliminary, randomized trial of fluoxetine, olanzapine, and the olanzapine-fluoxetine combination in women with borderline personality disorder. J Clin Psychiatry. 2004;65(7):903-907.
9. Hollander E, Tracy KA, Swann AC, et al. Divalproex in the treatment of impulsive aggression: efficacy in cluster B personality disorders. Neuropsychopharmacology. 2003;28(6):1186-1197.
10. Hilger E, Barnas C, Kasper S. Quetiapine in the treatment of borderline personality disorder. World J Biol Psychiatry. 2003;4(1):42-44.
11. Rizvi ST. Lamotrigine and borderline personality disorder. J Child Adolesc Psychopharmacol. 2002;12(4):365-366.
12. Rocca P, Marchiaro L, Cocuzza E, et al. Treatment of borderline personality disorder with risperidone. J Clin Psychiatry. 2002;63(3):241-244.
13. Philipsen A, Richter H, Schmahl C, et al. Clonidine in acute aversive inner tension and self-injurious behavior in female patients with borderline personality disorder. J Clin Psychiatry. 2004;65(10):1414-1419.
14. Pascual JC, Oller S, Soler J, et al. Ziprasidone in the acute treatment of borderline personality disorder in psychiatric emergency services. J Clin Psychiatry. 2004;65(9):1281-1282.
15. Lieb K, Völlm B, Rücker G, et al. Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials. Br J Psychiatry. 2010;196(1):4-12.
1. Diagnostic and statistical manual of mental disorders, 4th ed, text revision. Washington, DC: American Psychiatric Association; 2000.
2. Koenigsberg HW, Kernberg OF, Stone MH, et al. Borderline patients: extending the limits of treatability. New York, NY: Basic Books; 2000.
3. Nee C, Farman S. Female prisoners with borderline personality disorder: some promising treatment developments. Crim Behav Ment Health. 2005;15:2-16.
4. Oldham JM, Bender DS, Skodol AE, et al. Testing an APA practice guideline: symptom-targeted medication utilization for patients with borderline personality disorder. J Psychiatr Pract. 2004;10:156-161.
5. American Psychiatric Association Practice Guidelines. Practice guideline for the treatment of patients with borderline personality disorder. Am J Psychiatry. 2001;158(suppl 10):1-52.
6. Yatham LN. Newer anticonvulsants in the treatment of bipolar disorder. J Clin Psychiatry. 2004;65(suppl 10):28-35.
7. Rinne T, van den Brink W, Wouters L, et al. SSRI treatment of borderline personality disorder: a randomized, placebo-controlled clinical trial for female patients with borderline personality disorder. Am J Psychiatry. 2002;159(12):2048-2054.
8. Zanarini MC, Frankenburg FR, Parachini EA. A preliminary, randomized trial of fluoxetine, olanzapine, and the olanzapine-fluoxetine combination in women with borderline personality disorder. J Clin Psychiatry. 2004;65(7):903-907.
9. Hollander E, Tracy KA, Swann AC, et al. Divalproex in the treatment of impulsive aggression: efficacy in cluster B personality disorders. Neuropsychopharmacology. 2003;28(6):1186-1197.
10. Hilger E, Barnas C, Kasper S. Quetiapine in the treatment of borderline personality disorder. World J Biol Psychiatry. 2003;4(1):42-44.
11. Rizvi ST. Lamotrigine and borderline personality disorder. J Child Adolesc Psychopharmacol. 2002;12(4):365-366.
12. Rocca P, Marchiaro L, Cocuzza E, et al. Treatment of borderline personality disorder with risperidone. J Clin Psychiatry. 2002;63(3):241-244.
13. Philipsen A, Richter H, Schmahl C, et al. Clonidine in acute aversive inner tension and self-injurious behavior in female patients with borderline personality disorder. J Clin Psychiatry. 2004;65(10):1414-1419.
14. Pascual JC, Oller S, Soler J, et al. Ziprasidone in the acute treatment of borderline personality disorder in psychiatric emergency services. J Clin Psychiatry. 2004;65(9):1281-1282.
15. Lieb K, Völlm B, Rücker G, et al. Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials. Br J Psychiatry. 2010;196(1):4-12.