User login
The Clinicians’ Role in Building a System of Care: Army Behavioral Health Since 2001
The Military Health System has changed in countless ways during the era of the Global War on Terror, but no clinical area has been challenged as thoroughly and transformed as extensively as U.S. Army behavioral health care. Through 2011, the wars in Iraq and Afghanistan required soldiers to spend more than 1.5 million years in theater and contributed to significant increases in the incidence of posttraumatic stress disorder (PTSD), depression, and other behavioral health conditions in soldiers and family members.1,2
Unfortunately, the Army’s behavioral health treatment system, which had sufficiently met Army beneficiaries’ needs during peacetime, w
as not adequately resourced or structured to provide care on the scale that was required, and major problems in access, quality, continuity, and safety emerged.3 Army behavioral health and primary care providers experienced these challenges within their own practices, and many developed local solutions. Realizing that a near-complete system transformation was necessary, medical leaders turned to clinicians drawn from the field to develop a strategy to identify the best clinical practices and to build a standardized, cohesive system of care around them.
Although many challenges remain, the Army’s system of behavioral health care has substantially improved and now better supports clinicians in the field as they care for soldiers and their family members. Clinicians at the headquarters and local hospital levels played key roles in this transformation; however, very little literature on the topic exists. Clinicians engaging in current or planning for future health care system changes would benefit from a description of the process.
Unprecedented Challenges
As the wars in Iraq and Afghanistan intensified in the mid-2000s and the demand for behavioral health care grew, the full picture of the shortfalls in the Army’s system of behavioral health care came to the forefront. Provider shortages contributed to long waits for initial appointments, disrupted continuity, and reduced effectiveness of care.4 Even after an infusion of more than $1 billion in congressionally directed funding increased the number of staff and multiplied the clinical and nonclinical programs across the force, significant problems remained.5,6
Army hospitals divided behavioral health care between psychiatry, psychology, and social work fiefdoms, whose stovepipes often fractured communication between providers treating the same patient and prevented effective care coordination. Behavioral health clinics on each post offered different clinical services. Confused soldiers, leaders, and family members were forced to navigate various versions of behavioral health care each time they moved. Inaccurate, locally developed information systems produced little data on the effectiveness of local programs and hindered clinicians and leaders seeking to improve care. Without sufficient clinical capacity on the outpatient side, outpatient providers frequently admitted their patients to inpatient settings because it presented the only option to deliver needed services in a safe setting.
The turning point for improving care occurred in 2012 when senior medical leaders designated a behavioral health leadership team of clinicians, administrators, and analysts at the Army’s Office of the Surgeon General (OTSG) as its first service line. The move consolidated authority over behavioral health-related policy, programs, and funding and clearly communicated that Army Medicine was committed to improving behavioral health care. While behavioral health leaders had operated at OTSG for several years prior, they did not have the authority or resources to make widespread changes. Fortunately, the Army Surgeon General also adopted a command philosophy that emphasized the Operating Company Model, which sought to reduce variance by replicating successful practices across the enterprise. The Operating Company Model also limited each hospital commander’s authority to design their own unique clinical structure and shifted that responsibility to the clinicians in each service line at the headquarters level.
Forming a System of Care
The Behavioral Health Service Line partnered with the U.S. Army Public Health Command and systems engineers at the Massachusetts Institute of Technology to map the existing system of care and identify innovative clinical programs that represented best practices. In addition to 2 programs mandated by the DoD (Behavioral Health in Primary Care Medical Homes7 and Family Advocacy Programs),8 other programs (Embedded Behavioral Health, Multi-Disciplinary Behavioral Health clinics, Intensive Outpatient Program, inpatient care, residential care for substance use disorders, Connect Care, Tele-Behavioral Health, and the Child and Family Behavioral Health System) were selected for replication throughout the Army because they successfully demonstrated promising outcomes and filled a critical need.
To run the emerging standardized clinical programs, the Behavioral Health Service Line streamlined the leadership structure by eliminating all departments organized around provider discipline (ie, psychiatry, psychology, and social work) and created a single department of Behavioral Health at each Army hospital. For the first time, staff were organized into clinical teams based on the needs of the patients, not professional background. This change created new leadership opportunities across disciplines, reduced infighting, and eliminated a major source of confusion for patients and line leaders. The group of standard clinical programs, managed through integrated behavioral health departments in each Army hospital, was dubbed the Behavioral Health System of Care.
Change to department organizations and clinical programs created the need to reconfigure administrative data systems to provide accurate and timely information about system performance. Administrative teams revised Medical Expense Reporting and Performance System codes to provide visibility on important data, such as patient encounters and Revenue Value Units, down to the clinic and provider levels. To improve the reliability of existing data, OTSG staff led a multiyear effort to “clean” several data sources, such as those specifying provider type and work center.
Analysts used the refined workload information to build new tools, such as one to display individual provider productivity and one to predict the number and type of clinical staff required to meet the needs of the population at each Army installation. The administrative reorganization better informed clinical leaders at all levels by supplying meaningful data that enabled comparisons of performance within one or more Army hospitals.8
Translating System Changes Into Better Care
Despite transformative changes to Army behavioral health care, clinicians and leaders still had little insight into what mattered most: measuirng patient response to the treatment. To solve this issue, a team of Army clinical and information technology innovators developed the Behavioral Health Data Portal (BHDP), which used validated scales to collect input from patients at each outpatient visit about their current and recent symptoms. Clinicians use the information to complement their assessment, refine diagnoses, individualize treatment plans, and follow their patients’ progress.9
The BHDP also aggregates information on each patient’s progress into clinical outcome metrics that inform leaders about the effectiveness of the care their clinics provide. For the first time, analysts can establish correlations between specific actions at the clinic level and positive clinical outcomes. For example, the relationship between the use of evidence-based psychotherapies, regular follow-up, a strong therapeutic alliance, and provider use of BHDP have been clearly linked to more rapid resolution of PTSD symptoms. These insights provide opportunities to act on specific processes at the clinic level with high confidence that by doing so, clinicians are improving the effectiveness of the care delivered in their clinics.
Conclusion
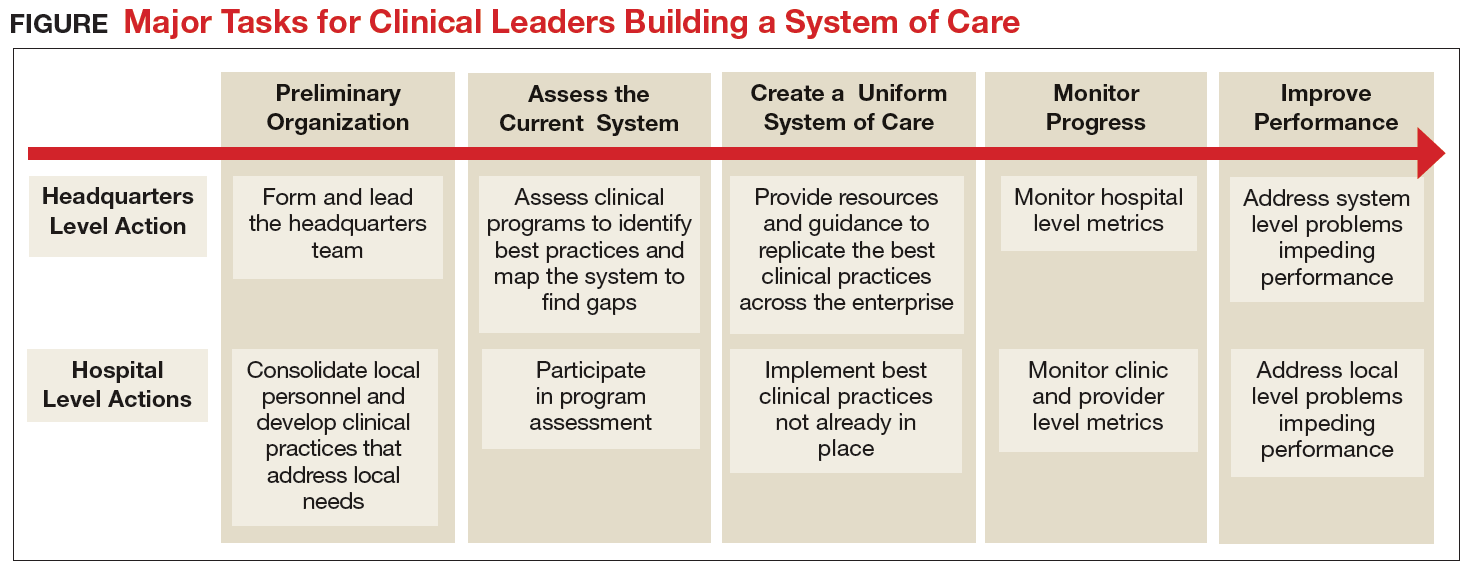
The transformation of Army behavioral health care has encompassed all aspects of the treatment system, but it has been led by clinicians working at the local and headquarters levels (Figure). Although many challenges remain, today’s outpatient system is more efficient and effective. For example, Army medical facilities are now able to meet more of the total demand for outpatient behavioral health care of its beneficiaries; 77% in September 2017 compared with a low of 59% in January 2013, based on Army Strategic Management System data as of December 1, 2017. With
The Army continues to improve its system of care to better inform and enable clinicians to deliver evidence-based care. The clinician-led process that advanced this area of military medicine is applicable to others. A core group of dedicated clinical professionals committed to multiyear processes can implement large-scale changes if they are empowered and resourced by senior medical leaders. A standardized system of care built on clinical best practices and guided by clinicians using accurate data, including clinical outcomes, would benefit any component of the MHS.
1. Baiocchi D. Measuring Army deployments to Iraq and Afghanistan. https://www.rand.org/pubs/research_reports/RR145.html. Published 2013. Accessed December 1, 2017.
2. Hoge C, Castro C, Messer S, McGurk D, Cotting D, Koffman D. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N Engl J Med. 2004;351(1):13-22.
3. Tanielian T, Jaycox LH (eds). Invisible wounds of war. RAND Corporation. https://www.rand.org/pubs/monographs/MG720.html. Published 2008. Accessed December 1, 2017.
4. Prine C. Army’s mental health programs swamped, understaffed. Pittsburgh Tribune-Review. http://triblive .com/x/pittsburghtrib/news/s_721604.html. Published February 7, 2011. Accessed December 1, 2017.
5. Weinick R, Beckjord E, Farmer C, et al. Programs addressing psychological health and traumatic brain injury among U.S. military servicemembers and their families. https://www.rand.org/pubs/technical_reports/TR950 .html. Published 2011. Accessed December 1, 2017.
6. Hoge CW, Ivany CG, Brusher EA, et al. Transformation of mental health care for U.S. soldiers and families during the Iraq and Afghanistan wars: where science and politics intersect. Am J Psychiatry. 2016;173(4):334-343.
7. Hunter CL, Goodie JL. Operational and clinical components for integrated-collaborative behavioral healthcare in the patient-centered medical home. Fam Syst Health. 2010;28(4):308-321.
8. Srinivasan J, Ivany CG, Sarmiento D, Woodson J. How the U.S. Army redesigned its mental health system. Harvard Business Review. https://hbr.org/2017/10/how-the-u-s-army-redesigned-its-mental-health-system. Published October 16, 2017. Accessed December 1, 2017.
9. Srinivasan J, Brown MD, Ivany CG, Woodson J. How the U.S. Army personalized its mental health care. Harvard Business Review. https://hbr.org/2016/12/how-the-u-s-army-personalized-its-mental-health-care. Published December 7, 2016. Accessed December 1, 2017.
The Military Health System has changed in countless ways during the era of the Global War on Terror, but no clinical area has been challenged as thoroughly and transformed as extensively as U.S. Army behavioral health care. Through 2011, the wars in Iraq and Afghanistan required soldiers to spend more than 1.5 million years in theater and contributed to significant increases in the incidence of posttraumatic stress disorder (PTSD), depression, and other behavioral health conditions in soldiers and family members.1,2
Unfortunately, the Army’s behavioral health treatment system, which had sufficiently met Army beneficiaries’ needs during peacetime, w
as not adequately resourced or structured to provide care on the scale that was required, and major problems in access, quality, continuity, and safety emerged.3 Army behavioral health and primary care providers experienced these challenges within their own practices, and many developed local solutions. Realizing that a near-complete system transformation was necessary, medical leaders turned to clinicians drawn from the field to develop a strategy to identify the best clinical practices and to build a standardized, cohesive system of care around them.
Although many challenges remain, the Army’s system of behavioral health care has substantially improved and now better supports clinicians in the field as they care for soldiers and their family members. Clinicians at the headquarters and local hospital levels played key roles in this transformation; however, very little literature on the topic exists. Clinicians engaging in current or planning for future health care system changes would benefit from a description of the process.
Unprecedented Challenges
As the wars in Iraq and Afghanistan intensified in the mid-2000s and the demand for behavioral health care grew, the full picture of the shortfalls in the Army’s system of behavioral health care came to the forefront. Provider shortages contributed to long waits for initial appointments, disrupted continuity, and reduced effectiveness of care.4 Even after an infusion of more than $1 billion in congressionally directed funding increased the number of staff and multiplied the clinical and nonclinical programs across the force, significant problems remained.5,6
Army hospitals divided behavioral health care between psychiatry, psychology, and social work fiefdoms, whose stovepipes often fractured communication between providers treating the same patient and prevented effective care coordination. Behavioral health clinics on each post offered different clinical services. Confused soldiers, leaders, and family members were forced to navigate various versions of behavioral health care each time they moved. Inaccurate, locally developed information systems produced little data on the effectiveness of local programs and hindered clinicians and leaders seeking to improve care. Without sufficient clinical capacity on the outpatient side, outpatient providers frequently admitted their patients to inpatient settings because it presented the only option to deliver needed services in a safe setting.
The turning point for improving care occurred in 2012 when senior medical leaders designated a behavioral health leadership team of clinicians, administrators, and analysts at the Army’s Office of the Surgeon General (OTSG) as its first service line. The move consolidated authority over behavioral health-related policy, programs, and funding and clearly communicated that Army Medicine was committed to improving behavioral health care. While behavioral health leaders had operated at OTSG for several years prior, they did not have the authority or resources to make widespread changes. Fortunately, the Army Surgeon General also adopted a command philosophy that emphasized the Operating Company Model, which sought to reduce variance by replicating successful practices across the enterprise. The Operating Company Model also limited each hospital commander’s authority to design their own unique clinical structure and shifted that responsibility to the clinicians in each service line at the headquarters level.
Forming a System of Care
The Behavioral Health Service Line partnered with the U.S. Army Public Health Command and systems engineers at the Massachusetts Institute of Technology to map the existing system of care and identify innovative clinical programs that represented best practices. In addition to 2 programs mandated by the DoD (Behavioral Health in Primary Care Medical Homes7 and Family Advocacy Programs),8 other programs (Embedded Behavioral Health, Multi-Disciplinary Behavioral Health clinics, Intensive Outpatient Program, inpatient care, residential care for substance use disorders, Connect Care, Tele-Behavioral Health, and the Child and Family Behavioral Health System) were selected for replication throughout the Army because they successfully demonstrated promising outcomes and filled a critical need.
To run the emerging standardized clinical programs, the Behavioral Health Service Line streamlined the leadership structure by eliminating all departments organized around provider discipline (ie, psychiatry, psychology, and social work) and created a single department of Behavioral Health at each Army hospital. For the first time, staff were organized into clinical teams based on the needs of the patients, not professional background. This change created new leadership opportunities across disciplines, reduced infighting, and eliminated a major source of confusion for patients and line leaders. The group of standard clinical programs, managed through integrated behavioral health departments in each Army hospital, was dubbed the Behavioral Health System of Care.
Change to department organizations and clinical programs created the need to reconfigure administrative data systems to provide accurate and timely information about system performance. Administrative teams revised Medical Expense Reporting and Performance System codes to provide visibility on important data, such as patient encounters and Revenue Value Units, down to the clinic and provider levels. To improve the reliability of existing data, OTSG staff led a multiyear effort to “clean” several data sources, such as those specifying provider type and work center.
Analysts used the refined workload information to build new tools, such as one to display individual provider productivity and one to predict the number and type of clinical staff required to meet the needs of the population at each Army installation. The administrative reorganization better informed clinical leaders at all levels by supplying meaningful data that enabled comparisons of performance within one or more Army hospitals.8
Translating System Changes Into Better Care
Despite transformative changes to Army behavioral health care, clinicians and leaders still had little insight into what mattered most: measuirng patient response to the treatment. To solve this issue, a team of Army clinical and information technology innovators developed the Behavioral Health Data Portal (BHDP), which used validated scales to collect input from patients at each outpatient visit about their current and recent symptoms. Clinicians use the information to complement their assessment, refine diagnoses, individualize treatment plans, and follow their patients’ progress.9
The BHDP also aggregates information on each patient’s progress into clinical outcome metrics that inform leaders about the effectiveness of the care their clinics provide. For the first time, analysts can establish correlations between specific actions at the clinic level and positive clinical outcomes. For example, the relationship between the use of evidence-based psychotherapies, regular follow-up, a strong therapeutic alliance, and provider use of BHDP have been clearly linked to more rapid resolution of PTSD symptoms. These insights provide opportunities to act on specific processes at the clinic level with high confidence that by doing so, clinicians are improving the effectiveness of the care delivered in their clinics.
Conclusion
The transformation of Army behavioral health care has encompassed all aspects of the treatment system, but it has been led by clinicians working at the local and headquarters levels (Figure). Although many challenges remain, today’s outpatient system is more efficient and effective. For example, Army medical facilities are now able to meet more of the total demand for outpatient behavioral health care of its beneficiaries; 77% in September 2017 compared with a low of 59% in January 2013, based on Army Strategic Management System data as of December 1, 2017. With
The Army continues to improve its system of care to better inform and enable clinicians to deliver evidence-based care. The clinician-led process that advanced this area of military medicine is applicable to others. A core group of dedicated clinical professionals committed to multiyear processes can implement large-scale changes if they are empowered and resourced by senior medical leaders. A standardized system of care built on clinical best practices and guided by clinicians using accurate data, including clinical outcomes, would benefit any component of the MHS.
The Military Health System has changed in countless ways during the era of the Global War on Terror, but no clinical area has been challenged as thoroughly and transformed as extensively as U.S. Army behavioral health care. Through 2011, the wars in Iraq and Afghanistan required soldiers to spend more than 1.5 million years in theater and contributed to significant increases in the incidence of posttraumatic stress disorder (PTSD), depression, and other behavioral health conditions in soldiers and family members.1,2
Unfortunately, the Army’s behavioral health treatment system, which had sufficiently met Army beneficiaries’ needs during peacetime, w
as not adequately resourced or structured to provide care on the scale that was required, and major problems in access, quality, continuity, and safety emerged.3 Army behavioral health and primary care providers experienced these challenges within their own practices, and many developed local solutions. Realizing that a near-complete system transformation was necessary, medical leaders turned to clinicians drawn from the field to develop a strategy to identify the best clinical practices and to build a standardized, cohesive system of care around them.
Although many challenges remain, the Army’s system of behavioral health care has substantially improved and now better supports clinicians in the field as they care for soldiers and their family members. Clinicians at the headquarters and local hospital levels played key roles in this transformation; however, very little literature on the topic exists. Clinicians engaging in current or planning for future health care system changes would benefit from a description of the process.
Unprecedented Challenges
As the wars in Iraq and Afghanistan intensified in the mid-2000s and the demand for behavioral health care grew, the full picture of the shortfalls in the Army’s system of behavioral health care came to the forefront. Provider shortages contributed to long waits for initial appointments, disrupted continuity, and reduced effectiveness of care.4 Even after an infusion of more than $1 billion in congressionally directed funding increased the number of staff and multiplied the clinical and nonclinical programs across the force, significant problems remained.5,6
Army hospitals divided behavioral health care between psychiatry, psychology, and social work fiefdoms, whose stovepipes often fractured communication between providers treating the same patient and prevented effective care coordination. Behavioral health clinics on each post offered different clinical services. Confused soldiers, leaders, and family members were forced to navigate various versions of behavioral health care each time they moved. Inaccurate, locally developed information systems produced little data on the effectiveness of local programs and hindered clinicians and leaders seeking to improve care. Without sufficient clinical capacity on the outpatient side, outpatient providers frequently admitted their patients to inpatient settings because it presented the only option to deliver needed services in a safe setting.
The turning point for improving care occurred in 2012 when senior medical leaders designated a behavioral health leadership team of clinicians, administrators, and analysts at the Army’s Office of the Surgeon General (OTSG) as its first service line. The move consolidated authority over behavioral health-related policy, programs, and funding and clearly communicated that Army Medicine was committed to improving behavioral health care. While behavioral health leaders had operated at OTSG for several years prior, they did not have the authority or resources to make widespread changes. Fortunately, the Army Surgeon General also adopted a command philosophy that emphasized the Operating Company Model, which sought to reduce variance by replicating successful practices across the enterprise. The Operating Company Model also limited each hospital commander’s authority to design their own unique clinical structure and shifted that responsibility to the clinicians in each service line at the headquarters level.
Forming a System of Care
The Behavioral Health Service Line partnered with the U.S. Army Public Health Command and systems engineers at the Massachusetts Institute of Technology to map the existing system of care and identify innovative clinical programs that represented best practices. In addition to 2 programs mandated by the DoD (Behavioral Health in Primary Care Medical Homes7 and Family Advocacy Programs),8 other programs (Embedded Behavioral Health, Multi-Disciplinary Behavioral Health clinics, Intensive Outpatient Program, inpatient care, residential care for substance use disorders, Connect Care, Tele-Behavioral Health, and the Child and Family Behavioral Health System) were selected for replication throughout the Army because they successfully demonstrated promising outcomes and filled a critical need.
To run the emerging standardized clinical programs, the Behavioral Health Service Line streamlined the leadership structure by eliminating all departments organized around provider discipline (ie, psychiatry, psychology, and social work) and created a single department of Behavioral Health at each Army hospital. For the first time, staff were organized into clinical teams based on the needs of the patients, not professional background. This change created new leadership opportunities across disciplines, reduced infighting, and eliminated a major source of confusion for patients and line leaders. The group of standard clinical programs, managed through integrated behavioral health departments in each Army hospital, was dubbed the Behavioral Health System of Care.
Change to department organizations and clinical programs created the need to reconfigure administrative data systems to provide accurate and timely information about system performance. Administrative teams revised Medical Expense Reporting and Performance System codes to provide visibility on important data, such as patient encounters and Revenue Value Units, down to the clinic and provider levels. To improve the reliability of existing data, OTSG staff led a multiyear effort to “clean” several data sources, such as those specifying provider type and work center.
Analysts used the refined workload information to build new tools, such as one to display individual provider productivity and one to predict the number and type of clinical staff required to meet the needs of the population at each Army installation. The administrative reorganization better informed clinical leaders at all levels by supplying meaningful data that enabled comparisons of performance within one or more Army hospitals.8
Translating System Changes Into Better Care
Despite transformative changes to Army behavioral health care, clinicians and leaders still had little insight into what mattered most: measuirng patient response to the treatment. To solve this issue, a team of Army clinical and information technology innovators developed the Behavioral Health Data Portal (BHDP), which used validated scales to collect input from patients at each outpatient visit about their current and recent symptoms. Clinicians use the information to complement their assessment, refine diagnoses, individualize treatment plans, and follow their patients’ progress.9
The BHDP also aggregates information on each patient’s progress into clinical outcome metrics that inform leaders about the effectiveness of the care their clinics provide. For the first time, analysts can establish correlations between specific actions at the clinic level and positive clinical outcomes. For example, the relationship between the use of evidence-based psychotherapies, regular follow-up, a strong therapeutic alliance, and provider use of BHDP have been clearly linked to more rapid resolution of PTSD symptoms. These insights provide opportunities to act on specific processes at the clinic level with high confidence that by doing so, clinicians are improving the effectiveness of the care delivered in their clinics.
Conclusion
The transformation of Army behavioral health care has encompassed all aspects of the treatment system, but it has been led by clinicians working at the local and headquarters levels (Figure). Although many challenges remain, today’s outpatient system is more efficient and effective. For example, Army medical facilities are now able to meet more of the total demand for outpatient behavioral health care of its beneficiaries; 77% in September 2017 compared with a low of 59% in January 2013, based on Army Strategic Management System data as of December 1, 2017. With
The Army continues to improve its system of care to better inform and enable clinicians to deliver evidence-based care. The clinician-led process that advanced this area of military medicine is applicable to others. A core group of dedicated clinical professionals committed to multiyear processes can implement large-scale changes if they are empowered and resourced by senior medical leaders. A standardized system of care built on clinical best practices and guided by clinicians using accurate data, including clinical outcomes, would benefit any component of the MHS.
1. Baiocchi D. Measuring Army deployments to Iraq and Afghanistan. https://www.rand.org/pubs/research_reports/RR145.html. Published 2013. Accessed December 1, 2017.
2. Hoge C, Castro C, Messer S, McGurk D, Cotting D, Koffman D. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N Engl J Med. 2004;351(1):13-22.
3. Tanielian T, Jaycox LH (eds). Invisible wounds of war. RAND Corporation. https://www.rand.org/pubs/monographs/MG720.html. Published 2008. Accessed December 1, 2017.
4. Prine C. Army’s mental health programs swamped, understaffed. Pittsburgh Tribune-Review. http://triblive .com/x/pittsburghtrib/news/s_721604.html. Published February 7, 2011. Accessed December 1, 2017.
5. Weinick R, Beckjord E, Farmer C, et al. Programs addressing psychological health and traumatic brain injury among U.S. military servicemembers and their families. https://www.rand.org/pubs/technical_reports/TR950 .html. Published 2011. Accessed December 1, 2017.
6. Hoge CW, Ivany CG, Brusher EA, et al. Transformation of mental health care for U.S. soldiers and families during the Iraq and Afghanistan wars: where science and politics intersect. Am J Psychiatry. 2016;173(4):334-343.
7. Hunter CL, Goodie JL. Operational and clinical components for integrated-collaborative behavioral healthcare in the patient-centered medical home. Fam Syst Health. 2010;28(4):308-321.
8. Srinivasan J, Ivany CG, Sarmiento D, Woodson J. How the U.S. Army redesigned its mental health system. Harvard Business Review. https://hbr.org/2017/10/how-the-u-s-army-redesigned-its-mental-health-system. Published October 16, 2017. Accessed December 1, 2017.
9. Srinivasan J, Brown MD, Ivany CG, Woodson J. How the U.S. Army personalized its mental health care. Harvard Business Review. https://hbr.org/2016/12/how-the-u-s-army-personalized-its-mental-health-care. Published December 7, 2016. Accessed December 1, 2017.
1. Baiocchi D. Measuring Army deployments to Iraq and Afghanistan. https://www.rand.org/pubs/research_reports/RR145.html. Published 2013. Accessed December 1, 2017.
2. Hoge C, Castro C, Messer S, McGurk D, Cotting D, Koffman D. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N Engl J Med. 2004;351(1):13-22.
3. Tanielian T, Jaycox LH (eds). Invisible wounds of war. RAND Corporation. https://www.rand.org/pubs/monographs/MG720.html. Published 2008. Accessed December 1, 2017.
4. Prine C. Army’s mental health programs swamped, understaffed. Pittsburgh Tribune-Review. http://triblive .com/x/pittsburghtrib/news/s_721604.html. Published February 7, 2011. Accessed December 1, 2017.
5. Weinick R, Beckjord E, Farmer C, et al. Programs addressing psychological health and traumatic brain injury among U.S. military servicemembers and their families. https://www.rand.org/pubs/technical_reports/TR950 .html. Published 2011. Accessed December 1, 2017.
6. Hoge CW, Ivany CG, Brusher EA, et al. Transformation of mental health care for U.S. soldiers and families during the Iraq and Afghanistan wars: where science and politics intersect. Am J Psychiatry. 2016;173(4):334-343.
7. Hunter CL, Goodie JL. Operational and clinical components for integrated-collaborative behavioral healthcare in the patient-centered medical home. Fam Syst Health. 2010;28(4):308-321.
8. Srinivasan J, Ivany CG, Sarmiento D, Woodson J. How the U.S. Army redesigned its mental health system. Harvard Business Review. https://hbr.org/2017/10/how-the-u-s-army-redesigned-its-mental-health-system. Published October 16, 2017. Accessed December 1, 2017.
9. Srinivasan J, Brown MD, Ivany CG, Woodson J. How the U.S. Army personalized its mental health care. Harvard Business Review. https://hbr.org/2016/12/how-the-u-s-army-personalized-its-mental-health-care. Published December 7, 2016. Accessed December 1, 2017.