User login
#payattention
Social media consumes the attention of the majority of teens. It is a place to express yourself, flirt, intimidate, and keep them up to date with the latest happenings in the social circles. But, teens are using social media for much more.

Instagram, a social media site comprising photographs followed by comments, is one of the most common sites used by teens. They post everything from the meal they are eating to the new love in their life and everything in between.
A hashtag is a type of label or metadata tag used on social networks and microblogging services, which makes it easier for users to find messages with a specific theme or content. Users create hashtags by placing the hash character # (the number sign) in front of a word or unspaced phrase, either in the main text of a message or at the end. Searching for that hashtag will then present each message that has been tagged with it.1 Although teens seem to prefer simple phrases, these hashtags are used to link users to what many refer to as “Secret Society.”
For example, if a teen girl was “cutting” or interested in connecting with other teens that cut, putting #cat would link her to several social communities with the related topic. Similarly, #selfharm was the initial term used to connect to this secret society. When that was shut down by the social media site, it resurfaced as #selfharmmm2.
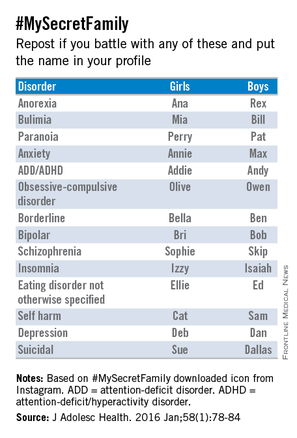
#MySecretFamily is a very popular hashtag that connects teens struggling with a variety of mental illnesses. Teens are instructed to put various names in their profile to identify which mental illness they are battling. For example, depression would be identified as “DEB” for a girl and “DAN” for a boy. The chart below lists various disorders.2
Nonsuicidal self-injury (NSSI) or deliberate destruction of one’s body in the absence of suicidal intent3 is most common in the middle school ages, and exposure to peer NSSI may increase the risk of engaging these behaviors.2,4 Although distinct from suicidal behaviors, there is a comorbidity between them. The normalization of these behaviors through social media and acceptance into the this “Secret Society” can only augment the risk of NSSI.
Parents not only need to be educated about the importance of monitoring their children’s social media but also about what to look for that may be a sign that something more serious is going on with them.
Although we hear so much of the negative impact of social media, it also can be a tool for early intervention.
References
1. Oxford English Dictionary, definition of “hashtag.”
2. J Adolesc Health. 2016 Jan;58(1):78-84.
4. Dev Psychol. 2006 May;42(3):407-17.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
Social media consumes the attention of the majority of teens. It is a place to express yourself, flirt, intimidate, and keep them up to date with the latest happenings in the social circles. But, teens are using social media for much more.
Instagram, a social media site comprising photographs followed by comments, is one of the most common sites used by teens. They post everything from the meal they are eating to the new love in their life and everything in between.
A hashtag is a type of label or metadata tag used on social networks and microblogging services, which makes it easier for users to find messages with a specific theme or content. Users create hashtags by placing the hash character # (the number sign) in front of a word or unspaced phrase, either in the main text of a message or at the end. Searching for that hashtag will then present each message that has been tagged with it.1 Although teens seem to prefer simple phrases, these hashtags are used to link users to what many refer to as “Secret Society.”
For example, if a teen girl was “cutting” or interested in connecting with other teens that cut, putting #cat would link her to several social communities with the related topic. Similarly, #selfharm was the initial term used to connect to this secret society. When that was shut down by the social media site, it resurfaced as #selfharmmm2.
#MySecretFamily is a very popular hashtag that connects teens struggling with a variety of mental illnesses. Teens are instructed to put various names in their profile to identify which mental illness they are battling. For example, depression would be identified as “DEB” for a girl and “DAN” for a boy. The chart below lists various disorders.2
Nonsuicidal self-injury (NSSI) or deliberate destruction of one’s body in the absence of suicidal intent3 is most common in the middle school ages, and exposure to peer NSSI may increase the risk of engaging these behaviors.2,4 Although distinct from suicidal behaviors, there is a comorbidity between them. The normalization of these behaviors through social media and acceptance into the this “Secret Society” can only augment the risk of NSSI.
Parents not only need to be educated about the importance of monitoring their children’s social media but also about what to look for that may be a sign that something more serious is going on with them.
Although we hear so much of the negative impact of social media, it also can be a tool for early intervention.
References
1. Oxford English Dictionary, definition of “hashtag.”
2. J Adolesc Health. 2016 Jan;58(1):78-84.
4. Dev Psychol. 2006 May;42(3):407-17.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
Social media consumes the attention of the majority of teens. It is a place to express yourself, flirt, intimidate, and keep them up to date with the latest happenings in the social circles. But, teens are using social media for much more.
Instagram, a social media site comprising photographs followed by comments, is one of the most common sites used by teens. They post everything from the meal they are eating to the new love in their life and everything in between.
A hashtag is a type of label or metadata tag used on social networks and microblogging services, which makes it easier for users to find messages with a specific theme or content. Users create hashtags by placing the hash character # (the number sign) in front of a word or unspaced phrase, either in the main text of a message or at the end. Searching for that hashtag will then present each message that has been tagged with it.1 Although teens seem to prefer simple phrases, these hashtags are used to link users to what many refer to as “Secret Society.”
For example, if a teen girl was “cutting” or interested in connecting with other teens that cut, putting #cat would link her to several social communities with the related topic. Similarly, #selfharm was the initial term used to connect to this secret society. When that was shut down by the social media site, it resurfaced as #selfharmmm2.
#MySecretFamily is a very popular hashtag that connects teens struggling with a variety of mental illnesses. Teens are instructed to put various names in their profile to identify which mental illness they are battling. For example, depression would be identified as “DEB” for a girl and “DAN” for a boy. The chart below lists various disorders.2
Nonsuicidal self-injury (NSSI) or deliberate destruction of one’s body in the absence of suicidal intent3 is most common in the middle school ages, and exposure to peer NSSI may increase the risk of engaging these behaviors.2,4 Although distinct from suicidal behaviors, there is a comorbidity between them. The normalization of these behaviors through social media and acceptance into the this “Secret Society” can only augment the risk of NSSI.
Parents not only need to be educated about the importance of monitoring their children’s social media but also about what to look for that may be a sign that something more serious is going on with them.
Although we hear so much of the negative impact of social media, it also can be a tool for early intervention.
References
1. Oxford English Dictionary, definition of “hashtag.”
2. J Adolesc Health. 2016 Jan;58(1):78-84.
4. Dev Psychol. 2006 May;42(3):407-17.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.

The Starbucks generation
Iced, Half-Caff, Ristretto, Venti, 4-Pump, Sugar Free, Cinnamon, Dolce Soy Skinny Latte. Or Non-Fat Frappuccino with Extra Whipped Cream and Chocolate Sauce. Sorry, let me simplify: Triple, Venti, Soy, No Foam Latte. If you’re thinking I am speaking a foreign language, just ask a teen and they likely will be able to translate for you. This is normal Starbucks lingo. If you’re not a coffee drinker, you’re likely completely lost, but for those of us who live by the bean, it’s the language of love, caffeine love.
Twenty years ago, the thought of a teen drinking coffee was unheard of. Sure, soda has been there for decades, and in many cultures tea is a common drink, but today many kids are lining up at Starbucks for the caffeine jolt, and the new drinks such as 5-Hour Energy, Jolt, and Red Bull are making this generation the most sleep-deprived ever.

But how bad is caffeine for teens? The average adult consumes approximately 300 mg of caffeine per day,1 which is equivalent to 2-4 cups of coffee; this is considered to be a moderate intake. But the average teen intake of caffeine is not limited to just coffee. Many are consuming their favorite drink from Starbucks, then a few cans of soda, chocolate candy, and maybe even an energy drink – all before the school day is over. When we consider the content of caffeine in these products, the intake of caffeine is staggering.
For example, the average soda contains 35-55 mg of caffeine. Energy drinks such as Red Bull, Amp, and Monster contain approximately 150 mg of caffeine. A tall (small) Starbucks coffee also contains about 150 mg of caffeine, and when we increase the size to a grande, then we are looking at 320 mg.2,4 Simple math will show that the average teen likely has excessive intake of caffeine, resulting in adverse health effects.

The most concerning adverse effect is sleep deprivation.5 Physiologically, the circadian rhythm of adolescents changes and decreases the secretion of melatonin naturally, making it more difficult for them to fall asleep. With the addition of caffeine in high amounts, this is making falling asleep a greater challenge. Sleep deprivation leads to daytime sleepiness and inattention, resulting in learning issues.
Other ill effects found in some studies is that consumption of more than 220 mg of caffeine per day is associated with increased impulsivity, sensation seeking, and risk-taking behaviors.2 In people who are predisposed to arrhythmias, excessive intake can result in the onset of arrhythmias. Nervousness and jitteriness are other common effects.
Another consideration beyond the direct effects of caffeine is that it is usually coupled with sugary substances like those found in syrups used in Starbucks drinks, chocolate candy, and energy drinks. This has led to concerns of obesity as well as dental decay.
Now, when caffeine is taken in small to moderate amounts, less than 300 mg, there are health benefits. It certainly does improve concentration by attaching to the adenosine receptors that block the adenosine effect of sedation on the brain. This leads to improved concentration, memory retention, auditory vigilance, and reaction time.
Recent studies have shown that caffeine in moderate amounts can protect against Alzheimer’s, and is linked to a small decreased risk of cancer and liver disease. Coffee drinkers have also shown a moderate decrease in Parkinson’s disease and stroke.3,6
Regardless of the benefits of caffeine, the American Academy of Pediatrics has been very clear that it does not recommend caffeine in children. In its 2011 guideline,7 the extra calories, the risk of impulsive behavior, and sleep deprivation far outweighed any benefit that caffeine would have. It is critical that physicians educate their patients about foods that contain caffeine and the cumulative effect these foods have on their well-being, now and in the future.
References
1. “Trends in Caffeine Intake Among US Children and Adolescents” (Pediatrics 2014;133:386-93).
2. Caffeine Consumption Among Children and Adolescents. National Council on Strength and Fitness.
3. What is it about coffee? Harvard Health Letter (www.health.harvard.edu/staying-healthy/what-is-it-about-coffee).
4. Caffeine counts. American Physiological Association (Monitor on Psychology. 2001 June;32[6]).
5. J Pediatrics. 2011 March;158(3):508-9.
6. J Alzheimers Dis. 2010;20(suppl 1):s167-74.
7. Pediatrics 2011 June;127(6):1182-9
Dr. Pearce is a pediatrician in Frankfort, Ill.
Iced, Half-Caff, Ristretto, Venti, 4-Pump, Sugar Free, Cinnamon, Dolce Soy Skinny Latte. Or Non-Fat Frappuccino with Extra Whipped Cream and Chocolate Sauce. Sorry, let me simplify: Triple, Venti, Soy, No Foam Latte. If you’re thinking I am speaking a foreign language, just ask a teen and they likely will be able to translate for you. This is normal Starbucks lingo. If you’re not a coffee drinker, you’re likely completely lost, but for those of us who live by the bean, it’s the language of love, caffeine love.
Twenty years ago, the thought of a teen drinking coffee was unheard of. Sure, soda has been there for decades, and in many cultures tea is a common drink, but today many kids are lining up at Starbucks for the caffeine jolt, and the new drinks such as 5-Hour Energy, Jolt, and Red Bull are making this generation the most sleep-deprived ever.
But how bad is caffeine for teens? The average adult consumes approximately 300 mg of caffeine per day,1 which is equivalent to 2-4 cups of coffee; this is considered to be a moderate intake. But the average teen intake of caffeine is not limited to just coffee. Many are consuming their favorite drink from Starbucks, then a few cans of soda, chocolate candy, and maybe even an energy drink – all before the school day is over. When we consider the content of caffeine in these products, the intake of caffeine is staggering.
For example, the average soda contains 35-55 mg of caffeine. Energy drinks such as Red Bull, Amp, and Monster contain approximately 150 mg of caffeine. A tall (small) Starbucks coffee also contains about 150 mg of caffeine, and when we increase the size to a grande, then we are looking at 320 mg.2,4 Simple math will show that the average teen likely has excessive intake of caffeine, resulting in adverse health effects.
The most concerning adverse effect is sleep deprivation.5 Physiologically, the circadian rhythm of adolescents changes and decreases the secretion of melatonin naturally, making it more difficult for them to fall asleep. With the addition of caffeine in high amounts, this is making falling asleep a greater challenge. Sleep deprivation leads to daytime sleepiness and inattention, resulting in learning issues.
Other ill effects found in some studies is that consumption of more than 220 mg of caffeine per day is associated with increased impulsivity, sensation seeking, and risk-taking behaviors.2 In people who are predisposed to arrhythmias, excessive intake can result in the onset of arrhythmias. Nervousness and jitteriness are other common effects.
Another consideration beyond the direct effects of caffeine is that it is usually coupled with sugary substances like those found in syrups used in Starbucks drinks, chocolate candy, and energy drinks. This has led to concerns of obesity as well as dental decay.
Now, when caffeine is taken in small to moderate amounts, less than 300 mg, there are health benefits. It certainly does improve concentration by attaching to the adenosine receptors that block the adenosine effect of sedation on the brain. This leads to improved concentration, memory retention, auditory vigilance, and reaction time.
Recent studies have shown that caffeine in moderate amounts can protect against Alzheimer’s, and is linked to a small decreased risk of cancer and liver disease. Coffee drinkers have also shown a moderate decrease in Parkinson’s disease and stroke.3,6
Regardless of the benefits of caffeine, the American Academy of Pediatrics has been very clear that it does not recommend caffeine in children. In its 2011 guideline,7 the extra calories, the risk of impulsive behavior, and sleep deprivation far outweighed any benefit that caffeine would have. It is critical that physicians educate their patients about foods that contain caffeine and the cumulative effect these foods have on their well-being, now and in the future.
References
1. “Trends in Caffeine Intake Among US Children and Adolescents” (Pediatrics 2014;133:386-93).
2. Caffeine Consumption Among Children and Adolescents. National Council on Strength and Fitness.
3. What is it about coffee? Harvard Health Letter (www.health.harvard.edu/staying-healthy/what-is-it-about-coffee).
4. Caffeine counts. American Physiological Association (Monitor on Psychology. 2001 June;32[6]).
5. J Pediatrics. 2011 March;158(3):508-9.
6. J Alzheimers Dis. 2010;20(suppl 1):s167-74.
7. Pediatrics 2011 June;127(6):1182-9
Dr. Pearce is a pediatrician in Frankfort, Ill.
Iced, Half-Caff, Ristretto, Venti, 4-Pump, Sugar Free, Cinnamon, Dolce Soy Skinny Latte. Or Non-Fat Frappuccino with Extra Whipped Cream and Chocolate Sauce. Sorry, let me simplify: Triple, Venti, Soy, No Foam Latte. If you’re thinking I am speaking a foreign language, just ask a teen and they likely will be able to translate for you. This is normal Starbucks lingo. If you’re not a coffee drinker, you’re likely completely lost, but for those of us who live by the bean, it’s the language of love, caffeine love.
Twenty years ago, the thought of a teen drinking coffee was unheard of. Sure, soda has been there for decades, and in many cultures tea is a common drink, but today many kids are lining up at Starbucks for the caffeine jolt, and the new drinks such as 5-Hour Energy, Jolt, and Red Bull are making this generation the most sleep-deprived ever.
But how bad is caffeine for teens? The average adult consumes approximately 300 mg of caffeine per day,1 which is equivalent to 2-4 cups of coffee; this is considered to be a moderate intake. But the average teen intake of caffeine is not limited to just coffee. Many are consuming their favorite drink from Starbucks, then a few cans of soda, chocolate candy, and maybe even an energy drink – all before the school day is over. When we consider the content of caffeine in these products, the intake of caffeine is staggering.
For example, the average soda contains 35-55 mg of caffeine. Energy drinks such as Red Bull, Amp, and Monster contain approximately 150 mg of caffeine. A tall (small) Starbucks coffee also contains about 150 mg of caffeine, and when we increase the size to a grande, then we are looking at 320 mg.2,4 Simple math will show that the average teen likely has excessive intake of caffeine, resulting in adverse health effects.
The most concerning adverse effect is sleep deprivation.5 Physiologically, the circadian rhythm of adolescents changes and decreases the secretion of melatonin naturally, making it more difficult for them to fall asleep. With the addition of caffeine in high amounts, this is making falling asleep a greater challenge. Sleep deprivation leads to daytime sleepiness and inattention, resulting in learning issues.
Other ill effects found in some studies is that consumption of more than 220 mg of caffeine per day is associated with increased impulsivity, sensation seeking, and risk-taking behaviors.2 In people who are predisposed to arrhythmias, excessive intake can result in the onset of arrhythmias. Nervousness and jitteriness are other common effects.
Another consideration beyond the direct effects of caffeine is that it is usually coupled with sugary substances like those found in syrups used in Starbucks drinks, chocolate candy, and energy drinks. This has led to concerns of obesity as well as dental decay.
Now, when caffeine is taken in small to moderate amounts, less than 300 mg, there are health benefits. It certainly does improve concentration by attaching to the adenosine receptors that block the adenosine effect of sedation on the brain. This leads to improved concentration, memory retention, auditory vigilance, and reaction time.
Recent studies have shown that caffeine in moderate amounts can protect against Alzheimer’s, and is linked to a small decreased risk of cancer and liver disease. Coffee drinkers have also shown a moderate decrease in Parkinson’s disease and stroke.3,6
Regardless of the benefits of caffeine, the American Academy of Pediatrics has been very clear that it does not recommend caffeine in children. In its 2011 guideline,7 the extra calories, the risk of impulsive behavior, and sleep deprivation far outweighed any benefit that caffeine would have. It is critical that physicians educate their patients about foods that contain caffeine and the cumulative effect these foods have on their well-being, now and in the future.
References
1. “Trends in Caffeine Intake Among US Children and Adolescents” (Pediatrics 2014;133:386-93).
2. Caffeine Consumption Among Children and Adolescents. National Council on Strength and Fitness.
3. What is it about coffee? Harvard Health Letter (www.health.harvard.edu/staying-healthy/what-is-it-about-coffee).
4. Caffeine counts. American Physiological Association (Monitor on Psychology. 2001 June;32[6]).
5. J Pediatrics. 2011 March;158(3):508-9.
6. J Alzheimers Dis. 2010;20(suppl 1):s167-74.
7. Pediatrics 2011 June;127(6):1182-9
Dr. Pearce is a pediatrician in Frankfort, Ill.

The HPV vaccine
As physicians, we play a unique role in medicine. Drawing on research data, we provide a gateway of information to patients and families. Governing agencies use that data to make recommendations so that we can promote treatment with confidence. But we also have a responsibility if there is an ill outcome, so being well versed on vaccines and treatments is imperative.
Since the human papillomavirus (HPV) vaccines (Gardasil, Cervarix) were approved for the prevention of HPV, there has been controversy. Despite the ongoing reports of the vaccine’s success in lowering cervical cancer rates, many parents still feel that it puts their children at risk.
A 2012 study – a systematic review of parents’ knowledge of HPV – showed a decline from 2001 to 2011, with a rise in parents’ safety concerns, and fewer parents opting to have their children vaccinated (Obstet Gynecol Int. 2012. doi: 10.1155/2012/921236).

Several studies have shown the overwhelming decline in cervical cancer that is directly related to the implementation of the HPV vaccines. But there has been growing concern, as postural orthostatic hypotension (POTS), complex regional pain syndrome (CRPS), and sudden death have been cited as side effects of theses vaccines. POTS and CRPS have been in the headlines recently, since a report came out linking the vaccine to these syndromes. Although a review by the European Medicines Agency found that the evidence does not support the notion of the HPV vaccine causing POTS or CRPS, many groups still promote a ban of the vaccine.
In 2013, Japan withdrew its recommendation for administration of the HPV vaccine after reports that many girls had been seriously harmed by it, and now calls for follow-up for patients who believe they are having side effects. Researchers argue that the basis for this action is poorly founded, and that many young women are being deprived of a vaccine that would be protective. But just as many say that more investigation needs to be done before the recommendation can be reinstated, given the number of reports about women being seriously injured from the vaccine. The Japan Society of Obstetrics and Gynecology is pleading with the Japanese Health Ministry to commence recommending the HPV cancer-preventing vaccineonce again.
An Internet search of this topic shows there are several articles questioning the safety of the vaccine, and throughout the world, concerns are forcing more research to be done to ensure its safety. Although the research overwhelmingly shows that the risk-to-benefit ratio is in favor of the HPV vaccine, several sites are reporting injury.
In a study of 997,585 girls aged 10-17 years in Denmark and Sweden, among whom 296,826 received a total of 696,420 quadrivalent HPV vaccine doses, 1,043 (less than 1%) were found to have adverse reactions, compared with 11,944 (2%) of unvaccinated girls (BMJ 2013;347:f5906). Although some relationship between HPV vaccine and autoimmune disorders such as Behçet’s syndrome, Raynaud’s disease, and type 1 diabetes was apparent, no consistent evidence for a causal association was found.
“Analysis of data reported to the Vaccine Adverse Event Reporting System revealed disproportionate reporting of venous thromboembolism,” noted Dr. Lisen Arnheim-Dahlström of the Karolinska Institutet, Stockholm, lead author of the BMJ study, and associates. “A study by the Vaccine Safety Datalink, which involved eight outcomes, identified a nonsignificantly increased relative risk (1.98) of venous thromboembolism; medical record review could confirm five of the eight cases identified from databases using international classification of diseases codes, and all five had known risk factors for venous thromboembolism. In our analysis, based on 21 vaccine exposed cases, there was no significant association with venous thromboembolism within 90 days after exposure to [quadrivalent] HPV vaccine.”
These rising concerns are resulting in more parents declining the HPV vaccine, and more questions for the primary care physician to answer. Not only are parents alarmed, but so are the physicians who make the recommendations. Being aware of the most current research and reports for and against the vaccine’s use, and being able to discuss with the family the validity of this information, will help to dispel much of the anxiety.
Dr. Pearce is a pediatrician in Frankfort, Ill. To contact her, send email to pdnews@frontlinemedcom.com.
As physicians, we play a unique role in medicine. Drawing on research data, we provide a gateway of information to patients and families. Governing agencies use that data to make recommendations so that we can promote treatment with confidence. But we also have a responsibility if there is an ill outcome, so being well versed on vaccines and treatments is imperative.
Since the human papillomavirus (HPV) vaccines (Gardasil, Cervarix) were approved for the prevention of HPV, there has been controversy. Despite the ongoing reports of the vaccine’s success in lowering cervical cancer rates, many parents still feel that it puts their children at risk.
A 2012 study – a systematic review of parents’ knowledge of HPV – showed a decline from 2001 to 2011, with a rise in parents’ safety concerns, and fewer parents opting to have their children vaccinated (Obstet Gynecol Int. 2012. doi: 10.1155/2012/921236).
Several studies have shown the overwhelming decline in cervical cancer that is directly related to the implementation of the HPV vaccines. But there has been growing concern, as postural orthostatic hypotension (POTS), complex regional pain syndrome (CRPS), and sudden death have been cited as side effects of theses vaccines. POTS and CRPS have been in the headlines recently, since a report came out linking the vaccine to these syndromes. Although a review by the European Medicines Agency found that the evidence does not support the notion of the HPV vaccine causing POTS or CRPS, many groups still promote a ban of the vaccine.
In 2013, Japan withdrew its recommendation for administration of the HPV vaccine after reports that many girls had been seriously harmed by it, and now calls for follow-up for patients who believe they are having side effects. Researchers argue that the basis for this action is poorly founded, and that many young women are being deprived of a vaccine that would be protective. But just as many say that more investigation needs to be done before the recommendation can be reinstated, given the number of reports about women being seriously injured from the vaccine. The Japan Society of Obstetrics and Gynecology is pleading with the Japanese Health Ministry to commence recommending the HPV cancer-preventing vaccineonce again.
An Internet search of this topic shows there are several articles questioning the safety of the vaccine, and throughout the world, concerns are forcing more research to be done to ensure its safety. Although the research overwhelmingly shows that the risk-to-benefit ratio is in favor of the HPV vaccine, several sites are reporting injury.
In a study of 997,585 girls aged 10-17 years in Denmark and Sweden, among whom 296,826 received a total of 696,420 quadrivalent HPV vaccine doses, 1,043 (less than 1%) were found to have adverse reactions, compared with 11,944 (2%) of unvaccinated girls (BMJ 2013;347:f5906). Although some relationship between HPV vaccine and autoimmune disorders such as Behçet’s syndrome, Raynaud’s disease, and type 1 diabetes was apparent, no consistent evidence for a causal association was found.
“Analysis of data reported to the Vaccine Adverse Event Reporting System revealed disproportionate reporting of venous thromboembolism,” noted Dr. Lisen Arnheim-Dahlström of the Karolinska Institutet, Stockholm, lead author of the BMJ study, and associates. “A study by the Vaccine Safety Datalink, which involved eight outcomes, identified a nonsignificantly increased relative risk (1.98) of venous thromboembolism; medical record review could confirm five of the eight cases identified from databases using international classification of diseases codes, and all five had known risk factors for venous thromboembolism. In our analysis, based on 21 vaccine exposed cases, there was no significant association with venous thromboembolism within 90 days after exposure to [quadrivalent] HPV vaccine.”
These rising concerns are resulting in more parents declining the HPV vaccine, and more questions for the primary care physician to answer. Not only are parents alarmed, but so are the physicians who make the recommendations. Being aware of the most current research and reports for and against the vaccine’s use, and being able to discuss with the family the validity of this information, will help to dispel much of the anxiety.
Dr. Pearce is a pediatrician in Frankfort, Ill. To contact her, send email to pdnews@frontlinemedcom.com.
As physicians, we play a unique role in medicine. Drawing on research data, we provide a gateway of information to patients and families. Governing agencies use that data to make recommendations so that we can promote treatment with confidence. But we also have a responsibility if there is an ill outcome, so being well versed on vaccines and treatments is imperative.
Since the human papillomavirus (HPV) vaccines (Gardasil, Cervarix) were approved for the prevention of HPV, there has been controversy. Despite the ongoing reports of the vaccine’s success in lowering cervical cancer rates, many parents still feel that it puts their children at risk.
A 2012 study – a systematic review of parents’ knowledge of HPV – showed a decline from 2001 to 2011, with a rise in parents’ safety concerns, and fewer parents opting to have their children vaccinated (Obstet Gynecol Int. 2012. doi: 10.1155/2012/921236).
Several studies have shown the overwhelming decline in cervical cancer that is directly related to the implementation of the HPV vaccines. But there has been growing concern, as postural orthostatic hypotension (POTS), complex regional pain syndrome (CRPS), and sudden death have been cited as side effects of theses vaccines. POTS and CRPS have been in the headlines recently, since a report came out linking the vaccine to these syndromes. Although a review by the European Medicines Agency found that the evidence does not support the notion of the HPV vaccine causing POTS or CRPS, many groups still promote a ban of the vaccine.
In 2013, Japan withdrew its recommendation for administration of the HPV vaccine after reports that many girls had been seriously harmed by it, and now calls for follow-up for patients who believe they are having side effects. Researchers argue that the basis for this action is poorly founded, and that many young women are being deprived of a vaccine that would be protective. But just as many say that more investigation needs to be done before the recommendation can be reinstated, given the number of reports about women being seriously injured from the vaccine. The Japan Society of Obstetrics and Gynecology is pleading with the Japanese Health Ministry to commence recommending the HPV cancer-preventing vaccineonce again.
An Internet search of this topic shows there are several articles questioning the safety of the vaccine, and throughout the world, concerns are forcing more research to be done to ensure its safety. Although the research overwhelmingly shows that the risk-to-benefit ratio is in favor of the HPV vaccine, several sites are reporting injury.
In a study of 997,585 girls aged 10-17 years in Denmark and Sweden, among whom 296,826 received a total of 696,420 quadrivalent HPV vaccine doses, 1,043 (less than 1%) were found to have adverse reactions, compared with 11,944 (2%) of unvaccinated girls (BMJ 2013;347:f5906). Although some relationship between HPV vaccine and autoimmune disorders such as Behçet’s syndrome, Raynaud’s disease, and type 1 diabetes was apparent, no consistent evidence for a causal association was found.
“Analysis of data reported to the Vaccine Adverse Event Reporting System revealed disproportionate reporting of venous thromboembolism,” noted Dr. Lisen Arnheim-Dahlström of the Karolinska Institutet, Stockholm, lead author of the BMJ study, and associates. “A study by the Vaccine Safety Datalink, which involved eight outcomes, identified a nonsignificantly increased relative risk (1.98) of venous thromboembolism; medical record review could confirm five of the eight cases identified from databases using international classification of diseases codes, and all five had known risk factors for venous thromboembolism. In our analysis, based on 21 vaccine exposed cases, there was no significant association with venous thromboembolism within 90 days after exposure to [quadrivalent] HPV vaccine.”
These rising concerns are resulting in more parents declining the HPV vaccine, and more questions for the primary care physician to answer. Not only are parents alarmed, but so are the physicians who make the recommendations. Being aware of the most current research and reports for and against the vaccine’s use, and being able to discuss with the family the validity of this information, will help to dispel much of the anxiety.
Dr. Pearce is a pediatrician in Frankfort, Ill. To contact her, send email to pdnews@frontlinemedcom.com.

Careful with that cough…
September, October, and November are well known as the “coughing months” in any general pediatrician’s office. We all can relate to the frustration we feel when that handful of patients returns for the unrelenting cough after steroids and albuterol have failed. Codeine has been known to be a good cough suppressant, and when coupled with promethazine (antihistamine), you have a very effective cough syrup that been used as such for decades.

Unfortunately, over the last few decades, this cough syrup has gained notoriety for use other than cough, and now is under great scrutiny. This common syrup is now the main ingredient of a poplar drink among teens known as “Sizzurp” or the “Purple Drank.” Well known artists tweet about it, post pictures of it on Instagram, sing about it in their songs, and glamorize it in their videos.
The mixture is simple; promethazine with codeine, lemon-lime sodas, and hard candies has all the makings of a party drink. It is fizzy, colorful, and sweet, with no horrible aftertaste, so gulping is easy. Most teens don’t limit their drinking to just the purple drink, so now we have a mixture of codeine with alcohol and or marijuana. All of which result in respiratory depression and potentially death.
The abuse of this cough syrup has become so great that Actavis was reported to pull it from production. Already the pint-size bottle sells on the street for $800, and limited access will only skyrocket its value.
As clinicians, we must be aware of the misuse and abuse of common prescription medications because teens prey on busy practices with false or exaggerated symptoms to try to obtain a prescription. Despite the American Academy of Pediatrics’ warning against codeine’s use as an antitussive in children (Pediatrics. 1997 Jun;99[6]:918-20.), there has not been a significant decline in its use (Pediatrics 2014 May;133[5]:e1139-47). Pediatricians need to use extreme caution, and be vigilant to identify frequent flyers or teens known to be at risk for drug abuse. Prescribe nonnarcotic-containing products first, and only prescribe small amounts promethazine/codeine products to prevent leftovers from being kept around the house for unsupervised use.
Most importantly, educate parents and families about the danger of overdose with these products so they can monitor its use.
Dr. Pearce is a pediatrician in Frankfort, Ill.
September, October, and November are well known as the “coughing months” in any general pediatrician’s office. We all can relate to the frustration we feel when that handful of patients returns for the unrelenting cough after steroids and albuterol have failed. Codeine has been known to be a good cough suppressant, and when coupled with promethazine (antihistamine), you have a very effective cough syrup that been used as such for decades.
Unfortunately, over the last few decades, this cough syrup has gained notoriety for use other than cough, and now is under great scrutiny. This common syrup is now the main ingredient of a poplar drink among teens known as “Sizzurp” or the “Purple Drank.” Well known artists tweet about it, post pictures of it on Instagram, sing about it in their songs, and glamorize it in their videos.
The mixture is simple; promethazine with codeine, lemon-lime sodas, and hard candies has all the makings of a party drink. It is fizzy, colorful, and sweet, with no horrible aftertaste, so gulping is easy. Most teens don’t limit their drinking to just the purple drink, so now we have a mixture of codeine with alcohol and or marijuana. All of which result in respiratory depression and potentially death.
The abuse of this cough syrup has become so great that Actavis was reported to pull it from production. Already the pint-size bottle sells on the street for $800, and limited access will only skyrocket its value.
As clinicians, we must be aware of the misuse and abuse of common prescription medications because teens prey on busy practices with false or exaggerated symptoms to try to obtain a prescription. Despite the American Academy of Pediatrics’ warning against codeine’s use as an antitussive in children (Pediatrics. 1997 Jun;99[6]:918-20.), there has not been a significant decline in its use (Pediatrics 2014 May;133[5]:e1139-47). Pediatricians need to use extreme caution, and be vigilant to identify frequent flyers or teens known to be at risk for drug abuse. Prescribe nonnarcotic-containing products first, and only prescribe small amounts promethazine/codeine products to prevent leftovers from being kept around the house for unsupervised use.
Most importantly, educate parents and families about the danger of overdose with these products so they can monitor its use.
Dr. Pearce is a pediatrician in Frankfort, Ill.
September, October, and November are well known as the “coughing months” in any general pediatrician’s office. We all can relate to the frustration we feel when that handful of patients returns for the unrelenting cough after steroids and albuterol have failed. Codeine has been known to be a good cough suppressant, and when coupled with promethazine (antihistamine), you have a very effective cough syrup that been used as such for decades.
Unfortunately, over the last few decades, this cough syrup has gained notoriety for use other than cough, and now is under great scrutiny. This common syrup is now the main ingredient of a poplar drink among teens known as “Sizzurp” or the “Purple Drank.” Well known artists tweet about it, post pictures of it on Instagram, sing about it in their songs, and glamorize it in their videos.
The mixture is simple; promethazine with codeine, lemon-lime sodas, and hard candies has all the makings of a party drink. It is fizzy, colorful, and sweet, with no horrible aftertaste, so gulping is easy. Most teens don’t limit their drinking to just the purple drink, so now we have a mixture of codeine with alcohol and or marijuana. All of which result in respiratory depression and potentially death.
The abuse of this cough syrup has become so great that Actavis was reported to pull it from production. Already the pint-size bottle sells on the street for $800, and limited access will only skyrocket its value.
As clinicians, we must be aware of the misuse and abuse of common prescription medications because teens prey on busy practices with false or exaggerated symptoms to try to obtain a prescription. Despite the American Academy of Pediatrics’ warning against codeine’s use as an antitussive in children (Pediatrics. 1997 Jun;99[6]:918-20.), there has not been a significant decline in its use (Pediatrics 2014 May;133[5]:e1139-47). Pediatricians need to use extreme caution, and be vigilant to identify frequent flyers or teens known to be at risk for drug abuse. Prescribe nonnarcotic-containing products first, and only prescribe small amounts promethazine/codeine products to prevent leftovers from being kept around the house for unsupervised use.
Most importantly, educate parents and families about the danger of overdose with these products so they can monitor its use.
Dr. Pearce is a pediatrician in Frankfort, Ill.

Reality check about IUDs
The Centers for Disease Control and Prevention recently released data regarding the use of long-acting reversible contraception (LARC), specifically intrauterine devices (IUDs), in adolescents, and suggested ways to increase their use. The American Congress of Obstetricians and Gynecologists then reiterated its recommendation promoting the use of LARC in adolescents (Obstet Gynecol. 2012;120:983-8). Historically, the use of IUDs in nulliparous females was concerning because of the risk of pelvic inflammatory disease (which could lead to infertility), pain at insertion, and the cost. But more recent research has dispelled many of those concerns, and new legislation has made access and affordability a reality; hence, the use of IUDs in teens was recommended. Despite these advances, physicians still are not making teens aware of this method of contraception.
In 2013, two important things occurred. First, emergency contraception was made available over the counter without age restriction. Second, the Affordable Care Act required most private insurance plans to cover at least one type of all 18 Food and Drug Administration–approved contraceptive methods for women as prescribed without cost sharing; this reduced the barrier of cost for IUDs. For patients covered by Medicaid, details vary, but in many cases some type of IUD is covered. In considering the best method of contraception in teens, we can all agree contraception is only as good as its proper use. If we remove the concern of infertility secondary to pelvic inflammatory disease and the barrier of cost, we can make the argument that LARC is an ideal choice for young women.
Birth rates for teenagers fell 9% from 2013 to 2014, to 24.2 births per 1,000 females aged 15-19 years – a record low according to CDC data. The rate has declined 42% since 2007 and 61% since 1991. Considering that the percent of teens who engage in sexual activity has not changed, the cause of the decline has to be related to increased contraception use and education. Although rates have declined significantly, there is much work to be done to protect our teens from unintended pregnancies.
The Contraceptive Choice Project was designed to give teens the option of birth control with the barrier of cost removed. Sixty-nine percent of 10,000 girls aged 14-17 years chose the IUD (Am J Obstet Gynecol. 2010;203[2]:115.e1-e7). The Contraceptive Choice Project also stated that the teens in this study were 20 times more likely to become pregnant using oral contraceptives, the patch, or a vaginal ring, compared with LARC or an injectable contraceptive. That is a significant statistic given that the choice of birth control used is heavily dependent on the options available. As primary care physicians, we are likely the first line of intervention, so it is important that we do not exclude the options most likely to prevent unintended pregnancies.
The rate of adolescents using IUDs increased from 0.2 to 2.5 in the 2002 and 2006-2010 National Surveys of Family Growth (J Adolesc Health. 2013;53:401-6).
There are choices when it comes to IUDs. ParaGard and Mirena are most well known. ParaGard contains copper and is hormone free; it can be used as emergency contraception and can remain in place for 12 years. Mirena releases levonorgestrel, and can be left in place for 5 years; there now is a generic form. There has been hesitation in using this product in teens because of a marketing decision made when Mirena was brought to the U.S. market. The company sought FDA approval only for women who already had children to avoid concerns about fertility. But research shows IUDS are safe and effective in women of all ages.
Unlike birth control pills, Mirena and Paragard do not reduce acne. But Mirena does reduce bloating and cramping associated with periods. Paragard has unpredictable bleeding and, therefore, is a less favorable choice in women who are not restricted to hormone-free contraception.
Newer brands on the market are Skyla and Liletta. Both are comparable to Mirena but have lower amounts of hormone, so these IUDs will be less effective in controlling the cramping and bloating. Skyla, unlike Mirena, is marketed to teens.
Implementing birth control options in your practice is imperative in caring for adolescents. Bedsider.org is a wonderful website that reviews all forms of birth control, and the pros and cons associated with each; it also compares the different types to help young women make the best choice. Another useful website is thenationalcampaign.org; this website is dedicated to educating physicians, parents, and adolescents in birth control choices to reduce unplanned pregnancies.
Dr. Pearce is a pediatrician in Frankfort, Ill.
The Centers for Disease Control and Prevention recently released data regarding the use of long-acting reversible contraception (LARC), specifically intrauterine devices (IUDs), in adolescents, and suggested ways to increase their use. The American Congress of Obstetricians and Gynecologists then reiterated its recommendation promoting the use of LARC in adolescents (Obstet Gynecol. 2012;120:983-8). Historically, the use of IUDs in nulliparous females was concerning because of the risk of pelvic inflammatory disease (which could lead to infertility), pain at insertion, and the cost. But more recent research has dispelled many of those concerns, and new legislation has made access and affordability a reality; hence, the use of IUDs in teens was recommended. Despite these advances, physicians still are not making teens aware of this method of contraception.
In 2013, two important things occurred. First, emergency contraception was made available over the counter without age restriction. Second, the Affordable Care Act required most private insurance plans to cover at least one type of all 18 Food and Drug Administration–approved contraceptive methods for women as prescribed without cost sharing; this reduced the barrier of cost for IUDs. For patients covered by Medicaid, details vary, but in many cases some type of IUD is covered. In considering the best method of contraception in teens, we can all agree contraception is only as good as its proper use. If we remove the concern of infertility secondary to pelvic inflammatory disease and the barrier of cost, we can make the argument that LARC is an ideal choice for young women.
Birth rates for teenagers fell 9% from 2013 to 2014, to 24.2 births per 1,000 females aged 15-19 years – a record low according to CDC data. The rate has declined 42% since 2007 and 61% since 1991. Considering that the percent of teens who engage in sexual activity has not changed, the cause of the decline has to be related to increased contraception use and education. Although rates have declined significantly, there is much work to be done to protect our teens from unintended pregnancies.
The Contraceptive Choice Project was designed to give teens the option of birth control with the barrier of cost removed. Sixty-nine percent of 10,000 girls aged 14-17 years chose the IUD (Am J Obstet Gynecol. 2010;203[2]:115.e1-e7). The Contraceptive Choice Project also stated that the teens in this study were 20 times more likely to become pregnant using oral contraceptives, the patch, or a vaginal ring, compared with LARC or an injectable contraceptive. That is a significant statistic given that the choice of birth control used is heavily dependent on the options available. As primary care physicians, we are likely the first line of intervention, so it is important that we do not exclude the options most likely to prevent unintended pregnancies.
The rate of adolescents using IUDs increased from 0.2 to 2.5 in the 2002 and 2006-2010 National Surveys of Family Growth (J Adolesc Health. 2013;53:401-6).
There are choices when it comes to IUDs. ParaGard and Mirena are most well known. ParaGard contains copper and is hormone free; it can be used as emergency contraception and can remain in place for 12 years. Mirena releases levonorgestrel, and can be left in place for 5 years; there now is a generic form. There has been hesitation in using this product in teens because of a marketing decision made when Mirena was brought to the U.S. market. The company sought FDA approval only for women who already had children to avoid concerns about fertility. But research shows IUDS are safe and effective in women of all ages.
Unlike birth control pills, Mirena and Paragard do not reduce acne. But Mirena does reduce bloating and cramping associated with periods. Paragard has unpredictable bleeding and, therefore, is a less favorable choice in women who are not restricted to hormone-free contraception.
Newer brands on the market are Skyla and Liletta. Both are comparable to Mirena but have lower amounts of hormone, so these IUDs will be less effective in controlling the cramping and bloating. Skyla, unlike Mirena, is marketed to teens.
Implementing birth control options in your practice is imperative in caring for adolescents. Bedsider.org is a wonderful website that reviews all forms of birth control, and the pros and cons associated with each; it also compares the different types to help young women make the best choice. Another useful website is thenationalcampaign.org; this website is dedicated to educating physicians, parents, and adolescents in birth control choices to reduce unplanned pregnancies.
Dr. Pearce is a pediatrician in Frankfort, Ill.
The Centers for Disease Control and Prevention recently released data regarding the use of long-acting reversible contraception (LARC), specifically intrauterine devices (IUDs), in adolescents, and suggested ways to increase their use. The American Congress of Obstetricians and Gynecologists then reiterated its recommendation promoting the use of LARC in adolescents (Obstet Gynecol. 2012;120:983-8). Historically, the use of IUDs in nulliparous females was concerning because of the risk of pelvic inflammatory disease (which could lead to infertility), pain at insertion, and the cost. But more recent research has dispelled many of those concerns, and new legislation has made access and affordability a reality; hence, the use of IUDs in teens was recommended. Despite these advances, physicians still are not making teens aware of this method of contraception.
In 2013, two important things occurred. First, emergency contraception was made available over the counter without age restriction. Second, the Affordable Care Act required most private insurance plans to cover at least one type of all 18 Food and Drug Administration–approved contraceptive methods for women as prescribed without cost sharing; this reduced the barrier of cost for IUDs. For patients covered by Medicaid, details vary, but in many cases some type of IUD is covered. In considering the best method of contraception in teens, we can all agree contraception is only as good as its proper use. If we remove the concern of infertility secondary to pelvic inflammatory disease and the barrier of cost, we can make the argument that LARC is an ideal choice for young women.
Birth rates for teenagers fell 9% from 2013 to 2014, to 24.2 births per 1,000 females aged 15-19 years – a record low according to CDC data. The rate has declined 42% since 2007 and 61% since 1991. Considering that the percent of teens who engage in sexual activity has not changed, the cause of the decline has to be related to increased contraception use and education. Although rates have declined significantly, there is much work to be done to protect our teens from unintended pregnancies.
The Contraceptive Choice Project was designed to give teens the option of birth control with the barrier of cost removed. Sixty-nine percent of 10,000 girls aged 14-17 years chose the IUD (Am J Obstet Gynecol. 2010;203[2]:115.e1-e7). The Contraceptive Choice Project also stated that the teens in this study were 20 times more likely to become pregnant using oral contraceptives, the patch, or a vaginal ring, compared with LARC or an injectable contraceptive. That is a significant statistic given that the choice of birth control used is heavily dependent on the options available. As primary care physicians, we are likely the first line of intervention, so it is important that we do not exclude the options most likely to prevent unintended pregnancies.
The rate of adolescents using IUDs increased from 0.2 to 2.5 in the 2002 and 2006-2010 National Surveys of Family Growth (J Adolesc Health. 2013;53:401-6).
There are choices when it comes to IUDs. ParaGard and Mirena are most well known. ParaGard contains copper and is hormone free; it can be used as emergency contraception and can remain in place for 12 years. Mirena releases levonorgestrel, and can be left in place for 5 years; there now is a generic form. There has been hesitation in using this product in teens because of a marketing decision made when Mirena was brought to the U.S. market. The company sought FDA approval only for women who already had children to avoid concerns about fertility. But research shows IUDS are safe and effective in women of all ages.
Unlike birth control pills, Mirena and Paragard do not reduce acne. But Mirena does reduce bloating and cramping associated with periods. Paragard has unpredictable bleeding and, therefore, is a less favorable choice in women who are not restricted to hormone-free contraception.
Newer brands on the market are Skyla and Liletta. Both are comparable to Mirena but have lower amounts of hormone, so these IUDs will be less effective in controlling the cramping and bloating. Skyla, unlike Mirena, is marketed to teens.
Implementing birth control options in your practice is imperative in caring for adolescents. Bedsider.org is a wonderful website that reviews all forms of birth control, and the pros and cons associated with each; it also compares the different types to help young women make the best choice. Another useful website is thenationalcampaign.org; this website is dedicated to educating physicians, parents, and adolescents in birth control choices to reduce unplanned pregnancies.
Dr. Pearce is a pediatrician in Frankfort, Ill.

Breast reductions
Adolescent medicine presents a unique challenge. Many pediatricians find themselves extrapolating treatment of childhood issues or modifying adult treatment to address adolescent issues. But the reality is adolescents are not big kids or little adults. They are a unique group that require special considerations and analysis for appropriate treatment.
Macromastia, enlarged breast, is a condition that affects many teenagers. It impacts their self-esteem, limits physical ability, and causes musculoskeletal and dermatologic issues, and yet most pediatricians cannot recall a specific lesson that covered the evaluation and treatment of this condition. Juvenile, or virginal, gigantomastia is a rare condition that consists of a period of rapid breast tissue growth followed by sustained growth in the peripubertal years. Growth can be symmetrical or asymmetrical. Either condition can lead to disfigurement, social anxiety, unwanted attention, and withdrawal. Therefore, acknowledging the condition and intervening are essential.
With obesity on the rise, the issue of macromastia continues to grow. Although macromastia and obesity can occur independently, obesity certainly augments the condition, and more and more physicians are confronted with complaints of neck, back, and shoulder pain. Left untreated, macromastia can cause physical limitation leading to further morbidity. The exact etiology is unknown, but it is presumed to be associated with a hypersensitivity of the mammary estrogen receptors and exposure to exogenous estrogen through food, drugs, or the environment.
Although a patient who has significant discomfort may benefit from physical therapy and strengthening exercises to improve posture, the definitive treatment for macromastia and juvenile gigantomastia is surgical breast reduction, even in adolescence. Medical management with injections of tamoxifen will halt the continued growth, but it will not reduce the size, and therefore will not correct the associated side effects. Weight loss may reduce the general appearance, but it will do little to reduce the actual size of the breast tissue itself.
Because breast development arrests before adulthood, delaying surgical intervention to adulthood is not necessary. In a retrospective study, recurrence took place with juvenile gigantomastia only if intervention was done in early adolescence and did not take place at all with macromastia (Mayo Clin Proc. 2001;76:503-10).
Indications for surgical intervention are chronic shoulder, neck, and back pain; shoulder grooving; skin irritation and skin breakdown underneath the breast; and social stress. It is important that the growth of the breast has ceased for at least a year, and a psychological assessment of the impact of the condition is performed.
Misconceptions associated with breast reduction include that it is for cosmetic purposes only; that macromastia can be reduced by weight loss, and therefore a surgical intervention is not necessary; that lactation is not possible after the procedure; and that insurance will not cover this procedure. As explained previously, there is an identifiable negative impact of macromastia on the musculoskeletal system as well as huge self-esteem and social issues.
Decades ago, breast reduction was seen as a cosmetic surgery. Surprisingly, many insurance companies will now cover the procedure if the morbidity is well documented.
Inability to breastfeed was the initial concern with early surgical intervention. Several studies have evaluated this, and all have come to the same conclusion: Although milk production may be reduced, postsurgical patients can breastfeed without difficulty. Given that lactation is not inhibited and continued stress on the musculoskeletal system causes further harm, early intervention is imperative.
Breast reduction surgery is safe. There is a risk of bleeding, infection, fat necrosis, and loss of sensation, but there is no higher incidence of these adverse effects in adolescents than there is in adults (J Pediatr Adolesc Gynecol. 2013;26[4]:228-33).
Macromastia clearly impacts the emotional, social, and physical well-being of an adolescent, and it likely will not be addressed by the young patient because of embarrassment. Therefore, it is up to the pediatrician to inquire about body image with all routine health exams, and to keep up to date with the latest recommendations to ensure the best outcomes.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at pdnews@frontlinemedcom.com.
Adolescent medicine presents a unique challenge. Many pediatricians find themselves extrapolating treatment of childhood issues or modifying adult treatment to address adolescent issues. But the reality is adolescents are not big kids or little adults. They are a unique group that require special considerations and analysis for appropriate treatment.
Macromastia, enlarged breast, is a condition that affects many teenagers. It impacts their self-esteem, limits physical ability, and causes musculoskeletal and dermatologic issues, and yet most pediatricians cannot recall a specific lesson that covered the evaluation and treatment of this condition. Juvenile, or virginal, gigantomastia is a rare condition that consists of a period of rapid breast tissue growth followed by sustained growth in the peripubertal years. Growth can be symmetrical or asymmetrical. Either condition can lead to disfigurement, social anxiety, unwanted attention, and withdrawal. Therefore, acknowledging the condition and intervening are essential.
With obesity on the rise, the issue of macromastia continues to grow. Although macromastia and obesity can occur independently, obesity certainly augments the condition, and more and more physicians are confronted with complaints of neck, back, and shoulder pain. Left untreated, macromastia can cause physical limitation leading to further morbidity. The exact etiology is unknown, but it is presumed to be associated with a hypersensitivity of the mammary estrogen receptors and exposure to exogenous estrogen through food, drugs, or the environment.
Although a patient who has significant discomfort may benefit from physical therapy and strengthening exercises to improve posture, the definitive treatment for macromastia and juvenile gigantomastia is surgical breast reduction, even in adolescence. Medical management with injections of tamoxifen will halt the continued growth, but it will not reduce the size, and therefore will not correct the associated side effects. Weight loss may reduce the general appearance, but it will do little to reduce the actual size of the breast tissue itself.
Because breast development arrests before adulthood, delaying surgical intervention to adulthood is not necessary. In a retrospective study, recurrence took place with juvenile gigantomastia only if intervention was done in early adolescence and did not take place at all with macromastia (Mayo Clin Proc. 2001;76:503-10).
Indications for surgical intervention are chronic shoulder, neck, and back pain; shoulder grooving; skin irritation and skin breakdown underneath the breast; and social stress. It is important that the growth of the breast has ceased for at least a year, and a psychological assessment of the impact of the condition is performed.
Misconceptions associated with breast reduction include that it is for cosmetic purposes only; that macromastia can be reduced by weight loss, and therefore a surgical intervention is not necessary; that lactation is not possible after the procedure; and that insurance will not cover this procedure. As explained previously, there is an identifiable negative impact of macromastia on the musculoskeletal system as well as huge self-esteem and social issues.
Decades ago, breast reduction was seen as a cosmetic surgery. Surprisingly, many insurance companies will now cover the procedure if the morbidity is well documented.
Inability to breastfeed was the initial concern with early surgical intervention. Several studies have evaluated this, and all have come to the same conclusion: Although milk production may be reduced, postsurgical patients can breastfeed without difficulty. Given that lactation is not inhibited and continued stress on the musculoskeletal system causes further harm, early intervention is imperative.
Breast reduction surgery is safe. There is a risk of bleeding, infection, fat necrosis, and loss of sensation, but there is no higher incidence of these adverse effects in adolescents than there is in adults (J Pediatr Adolesc Gynecol. 2013;26[4]:228-33).
Macromastia clearly impacts the emotional, social, and physical well-being of an adolescent, and it likely will not be addressed by the young patient because of embarrassment. Therefore, it is up to the pediatrician to inquire about body image with all routine health exams, and to keep up to date with the latest recommendations to ensure the best outcomes.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at pdnews@frontlinemedcom.com.
Adolescent medicine presents a unique challenge. Many pediatricians find themselves extrapolating treatment of childhood issues or modifying adult treatment to address adolescent issues. But the reality is adolescents are not big kids or little adults. They are a unique group that require special considerations and analysis for appropriate treatment.
Macromastia, enlarged breast, is a condition that affects many teenagers. It impacts their self-esteem, limits physical ability, and causes musculoskeletal and dermatologic issues, and yet most pediatricians cannot recall a specific lesson that covered the evaluation and treatment of this condition. Juvenile, or virginal, gigantomastia is a rare condition that consists of a period of rapid breast tissue growth followed by sustained growth in the peripubertal years. Growth can be symmetrical or asymmetrical. Either condition can lead to disfigurement, social anxiety, unwanted attention, and withdrawal. Therefore, acknowledging the condition and intervening are essential.
With obesity on the rise, the issue of macromastia continues to grow. Although macromastia and obesity can occur independently, obesity certainly augments the condition, and more and more physicians are confronted with complaints of neck, back, and shoulder pain. Left untreated, macromastia can cause physical limitation leading to further morbidity. The exact etiology is unknown, but it is presumed to be associated with a hypersensitivity of the mammary estrogen receptors and exposure to exogenous estrogen through food, drugs, or the environment.
Although a patient who has significant discomfort may benefit from physical therapy and strengthening exercises to improve posture, the definitive treatment for macromastia and juvenile gigantomastia is surgical breast reduction, even in adolescence. Medical management with injections of tamoxifen will halt the continued growth, but it will not reduce the size, and therefore will not correct the associated side effects. Weight loss may reduce the general appearance, but it will do little to reduce the actual size of the breast tissue itself.
Because breast development arrests before adulthood, delaying surgical intervention to adulthood is not necessary. In a retrospective study, recurrence took place with juvenile gigantomastia only if intervention was done in early adolescence and did not take place at all with macromastia (Mayo Clin Proc. 2001;76:503-10).
Indications for surgical intervention are chronic shoulder, neck, and back pain; shoulder grooving; skin irritation and skin breakdown underneath the breast; and social stress. It is important that the growth of the breast has ceased for at least a year, and a psychological assessment of the impact of the condition is performed.
Misconceptions associated with breast reduction include that it is for cosmetic purposes only; that macromastia can be reduced by weight loss, and therefore a surgical intervention is not necessary; that lactation is not possible after the procedure; and that insurance will not cover this procedure. As explained previously, there is an identifiable negative impact of macromastia on the musculoskeletal system as well as huge self-esteem and social issues.
Decades ago, breast reduction was seen as a cosmetic surgery. Surprisingly, many insurance companies will now cover the procedure if the morbidity is well documented.
Inability to breastfeed was the initial concern with early surgical intervention. Several studies have evaluated this, and all have come to the same conclusion: Although milk production may be reduced, postsurgical patients can breastfeed without difficulty. Given that lactation is not inhibited and continued stress on the musculoskeletal system causes further harm, early intervention is imperative.
Breast reduction surgery is safe. There is a risk of bleeding, infection, fat necrosis, and loss of sensation, but there is no higher incidence of these adverse effects in adolescents than there is in adults (J Pediatr Adolesc Gynecol. 2013;26[4]:228-33).
Macromastia clearly impacts the emotional, social, and physical well-being of an adolescent, and it likely will not be addressed by the young patient because of embarrassment. Therefore, it is up to the pediatrician to inquire about body image with all routine health exams, and to keep up to date with the latest recommendations to ensure the best outcomes.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at pdnews@frontlinemedcom.com.

Legal matters – not just child’s play
Social media platforms are by far the most common form of communication among our teens. A 2015 study by the Pew Research Center stated that 71% of teens between the ages of 12 and 18 years use more than one form of social media. But little education and awareness of the legal implications of the information exchanged is provided to these teens, which has landed some of them in significant legal trouble.
Gone are the days when rivals could just pass mean comments to each other in the hallway or leave obnoxious comments on a bathroom wall. Today, within minutes malicious comments are quickly posted on social media to be shared by all. This makes the impact of the impulsive, mindless, and usually immature sentiments much more damaging, and unfortunately can result in severe, sometimes unforeseen consequences.
Cyberbullying is bullying or intimidating through electronic technology. This has become all too commonplace among teenagers because it takes so little to post unflattering pictures, or quotes, or threating messages from the privacy of your home. Much of what would never be spoken face to face is posted without regard. Two teen girls in Florida were charged with a felony for the suicide of a classmate they unrelentingly bullied. This was just one of many stories of a child being brought to despair by immature and cowardly teens misusing social media. Surely they never realized that their immature act would land them in jail. It is a crime to threaten to kill or seriously harm, menace, or harass a person for any reason, regardless of one’s age.
Defamation is a social tort that protects the reputation of a person from untrue comments or innuendos. In the past this was considered to be gossip or rumor-mongering, but now, given the advent of new technology, publishing these same comments makes one the author and, therefore, may be liable for defamation of character. This may not mean jail time for a person, but can certainly land that person in court, requiring his or her parents to incur significant legal fees.
Probably the most important legal issue that teens – as well as adults – should know about are the laws regarding sexual texting or “sexting.” For those of us born in the era before social media, sexting is the distribution of nude pictures of themselves or anyone else. When the image is that of a person under the age of 18 years, it is considered child pornography and subject to punishment by law. Because child pornography is taken very seriously, dosomething.org is a website for young people that promotes social awareness in hopes of changing behavior. This site presents the alarming percentages of teens who send and or receive nude or sexually explicit photos. Many have no idea they are committing a felony.
The unfortunate reality is that many photos or videos that were exchanged between trusted friends end up in the hands of ill-intended teens and get widely disseminated on social media. Anyone caught having or disseminating child pornography, regardless of who started it, is at risk of criminal repercussions. There have been several so-called “THOT” pages (That Ho Over There) started at high schools where students published nude pictures of classmates. These pages go viral within minutes, and although they are taken down quickly, the damage usually is already done. These actions can result in expulsion and suspension of students and significant emotional distress to the victim.
Another legal concern is the issue of privacy. Many users don’t realize that personal information displayed on social media can be easily obtained and misused. Identity theft is on the rise, not just because criminals are more savvy, but because so many people are careless with their information. Disclosure of email, birth date, and cell phone number are all desirable pieces of information that drive marketing, but more importantly, allows information to be used and misconstrued by anyone to create a phony identity, gain access to accounts, stalk, harass, or even resort to blackmail. The unauthorized use of personal information is illegal and punishable by law.
Another legal issue associated with social media are copyright laws. Many teens, as well as adults, have no idea of the laws that protect the music, videos, pictures, and images thoughtlessly placed on social media. Most don’t realize that just because it is commonly done doesn’t mean that it’s legal. Once a picture is posted, it can be shared, altered, and downloaded all over the world by anyone.
There have been reports of lawsuits brought by parents who found pictures of their children were used in advertisements by major companies without their knowledge or permission. Companies, likewise, have brought suit against individuals who have unknowingly misused their product in a post to entertain their friends. In fact, many of the apps that people download have a check box to acknowledge that the owners are free to use material posted at their discretion, which most folks check without reading the fine print. Because the laws on the books lag behind the changing times, there is often a lot of room for interpretation that puts everyone at risk. So teenagers must understand that just because material is published doesn’t mean it is free to be used for personal distribution.
Primary care physicians play a critical role in educating families. Dosomething.org and stopbullying.gov are two great resources for parents and children alike. Educating teens to the legal and social repercussions is key in protecting them. Schools and parents have to be aware themselves and continually stress the importance of Internet safety and appropriate use of social media.
Dr. Pearce is a pediatrician in Frankfort, Ill. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Email her at pdnews@frontlinemedcom.com
Social media platforms are by far the most common form of communication among our teens. A 2015 study by the Pew Research Center stated that 71% of teens between the ages of 12 and 18 years use more than one form of social media. But little education and awareness of the legal implications of the information exchanged is provided to these teens, which has landed some of them in significant legal trouble.
Gone are the days when rivals could just pass mean comments to each other in the hallway or leave obnoxious comments on a bathroom wall. Today, within minutes malicious comments are quickly posted on social media to be shared by all. This makes the impact of the impulsive, mindless, and usually immature sentiments much more damaging, and unfortunately can result in severe, sometimes unforeseen consequences.
Cyberbullying is bullying or intimidating through electronic technology. This has become all too commonplace among teenagers because it takes so little to post unflattering pictures, or quotes, or threating messages from the privacy of your home. Much of what would never be spoken face to face is posted without regard. Two teen girls in Florida were charged with a felony for the suicide of a classmate they unrelentingly bullied. This was just one of many stories of a child being brought to despair by immature and cowardly teens misusing social media. Surely they never realized that their immature act would land them in jail. It is a crime to threaten to kill or seriously harm, menace, or harass a person for any reason, regardless of one’s age.
Defamation is a social tort that protects the reputation of a person from untrue comments or innuendos. In the past this was considered to be gossip or rumor-mongering, but now, given the advent of new technology, publishing these same comments makes one the author and, therefore, may be liable for defamation of character. This may not mean jail time for a person, but can certainly land that person in court, requiring his or her parents to incur significant legal fees.
Probably the most important legal issue that teens – as well as adults – should know about are the laws regarding sexual texting or “sexting.” For those of us born in the era before social media, sexting is the distribution of nude pictures of themselves or anyone else. When the image is that of a person under the age of 18 years, it is considered child pornography and subject to punishment by law. Because child pornography is taken very seriously, dosomething.org is a website for young people that promotes social awareness in hopes of changing behavior. This site presents the alarming percentages of teens who send and or receive nude or sexually explicit photos. Many have no idea they are committing a felony.
The unfortunate reality is that many photos or videos that were exchanged between trusted friends end up in the hands of ill-intended teens and get widely disseminated on social media. Anyone caught having or disseminating child pornography, regardless of who started it, is at risk of criminal repercussions. There have been several so-called “THOT” pages (That Ho Over There) started at high schools where students published nude pictures of classmates. These pages go viral within minutes, and although they are taken down quickly, the damage usually is already done. These actions can result in expulsion and suspension of students and significant emotional distress to the victim.
Another legal concern is the issue of privacy. Many users don’t realize that personal information displayed on social media can be easily obtained and misused. Identity theft is on the rise, not just because criminals are more savvy, but because so many people are careless with their information. Disclosure of email, birth date, and cell phone number are all desirable pieces of information that drive marketing, but more importantly, allows information to be used and misconstrued by anyone to create a phony identity, gain access to accounts, stalk, harass, or even resort to blackmail. The unauthorized use of personal information is illegal and punishable by law.
Another legal issue associated with social media are copyright laws. Many teens, as well as adults, have no idea of the laws that protect the music, videos, pictures, and images thoughtlessly placed on social media. Most don’t realize that just because it is commonly done doesn’t mean that it’s legal. Once a picture is posted, it can be shared, altered, and downloaded all over the world by anyone.
There have been reports of lawsuits brought by parents who found pictures of their children were used in advertisements by major companies without their knowledge or permission. Companies, likewise, have brought suit against individuals who have unknowingly misused their product in a post to entertain their friends. In fact, many of the apps that people download have a check box to acknowledge that the owners are free to use material posted at their discretion, which most folks check without reading the fine print. Because the laws on the books lag behind the changing times, there is often a lot of room for interpretation that puts everyone at risk. So teenagers must understand that just because material is published doesn’t mean it is free to be used for personal distribution.
Primary care physicians play a critical role in educating families. Dosomething.org and stopbullying.gov are two great resources for parents and children alike. Educating teens to the legal and social repercussions is key in protecting them. Schools and parents have to be aware themselves and continually stress the importance of Internet safety and appropriate use of social media.
Dr. Pearce is a pediatrician in Frankfort, Ill. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Email her at pdnews@frontlinemedcom.com
Social media platforms are by far the most common form of communication among our teens. A 2015 study by the Pew Research Center stated that 71% of teens between the ages of 12 and 18 years use more than one form of social media. But little education and awareness of the legal implications of the information exchanged is provided to these teens, which has landed some of them in significant legal trouble.
Gone are the days when rivals could just pass mean comments to each other in the hallway or leave obnoxious comments on a bathroom wall. Today, within minutes malicious comments are quickly posted on social media to be shared by all. This makes the impact of the impulsive, mindless, and usually immature sentiments much more damaging, and unfortunately can result in severe, sometimes unforeseen consequences.
Cyberbullying is bullying or intimidating through electronic technology. This has become all too commonplace among teenagers because it takes so little to post unflattering pictures, or quotes, or threating messages from the privacy of your home. Much of what would never be spoken face to face is posted without regard. Two teen girls in Florida were charged with a felony for the suicide of a classmate they unrelentingly bullied. This was just one of many stories of a child being brought to despair by immature and cowardly teens misusing social media. Surely they never realized that their immature act would land them in jail. It is a crime to threaten to kill or seriously harm, menace, or harass a person for any reason, regardless of one’s age.
Defamation is a social tort that protects the reputation of a person from untrue comments or innuendos. In the past this was considered to be gossip or rumor-mongering, but now, given the advent of new technology, publishing these same comments makes one the author and, therefore, may be liable for defamation of character. This may not mean jail time for a person, but can certainly land that person in court, requiring his or her parents to incur significant legal fees.
Probably the most important legal issue that teens – as well as adults – should know about are the laws regarding sexual texting or “sexting.” For those of us born in the era before social media, sexting is the distribution of nude pictures of themselves or anyone else. When the image is that of a person under the age of 18 years, it is considered child pornography and subject to punishment by law. Because child pornography is taken very seriously, dosomething.org is a website for young people that promotes social awareness in hopes of changing behavior. This site presents the alarming percentages of teens who send and or receive nude or sexually explicit photos. Many have no idea they are committing a felony.
The unfortunate reality is that many photos or videos that were exchanged between trusted friends end up in the hands of ill-intended teens and get widely disseminated on social media. Anyone caught having or disseminating child pornography, regardless of who started it, is at risk of criminal repercussions. There have been several so-called “THOT” pages (That Ho Over There) started at high schools where students published nude pictures of classmates. These pages go viral within minutes, and although they are taken down quickly, the damage usually is already done. These actions can result in expulsion and suspension of students and significant emotional distress to the victim.
Another legal concern is the issue of privacy. Many users don’t realize that personal information displayed on social media can be easily obtained and misused. Identity theft is on the rise, not just because criminals are more savvy, but because so many people are careless with their information. Disclosure of email, birth date, and cell phone number are all desirable pieces of information that drive marketing, but more importantly, allows information to be used and misconstrued by anyone to create a phony identity, gain access to accounts, stalk, harass, or even resort to blackmail. The unauthorized use of personal information is illegal and punishable by law.
Another legal issue associated with social media are copyright laws. Many teens, as well as adults, have no idea of the laws that protect the music, videos, pictures, and images thoughtlessly placed on social media. Most don’t realize that just because it is commonly done doesn’t mean that it’s legal. Once a picture is posted, it can be shared, altered, and downloaded all over the world by anyone.
There have been reports of lawsuits brought by parents who found pictures of their children were used in advertisements by major companies without their knowledge or permission. Companies, likewise, have brought suit against individuals who have unknowingly misused their product in a post to entertain their friends. In fact, many of the apps that people download have a check box to acknowledge that the owners are free to use material posted at their discretion, which most folks check without reading the fine print. Because the laws on the books lag behind the changing times, there is often a lot of room for interpretation that puts everyone at risk. So teenagers must understand that just because material is published doesn’t mean it is free to be used for personal distribution.
Primary care physicians play a critical role in educating families. Dosomething.org and stopbullying.gov are two great resources for parents and children alike. Educating teens to the legal and social repercussions is key in protecting them. Schools and parents have to be aware themselves and continually stress the importance of Internet safety and appropriate use of social media.
Dr. Pearce is a pediatrician in Frankfort, Ill. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Email her at pdnews@frontlinemedcom.com

Safe driver
Reducing morbidity and mortality is the focus of medicine, and much of our day is spent focusing on this, but how much do we as pediatricians address on the leading cause of death in teens? Motor vehicle accidents are the leading cause of death among 15- to 20-year-olds. In 2011, about 2,650 teens in the United States aged 16-19 years were killed and almost 292,000 were treated in emergency departments for injuries suffered in motor vehicle crashes, according to the Centers for Disease Control and Prevention. In 2010, the American Academy of Pediatrics reaffirmed its statement that was published on teen drivers in 2006, which encouraged pediatricians to be active participants in the education and lobbying for laws that promote of safe driving.
It may appear to be out of the scope of treatment to educate on safe driving, but the reality is that many parents are unaware of the risk factors that contribute to unsafe driving, as well the conditions that can be managed to improve their driving ability.
The major risk factors for increased injury among teens are immaturity, which leads to increased risk taking; inexperience; and distractions. Immaturity is the leading risk factor, clearly demonstrated in the number of crashes involving 16-year-old drivers, which is two times greater when compared with 17-year-olds and three times greater when compared with 25- to 29-year-olds.
Although distracted driving is not a problem limited to just teens, that compounded with inexperience certainly explains why they account for 14% of fatal accidents despite being only 6% of drivers. It has been statistically shown that the greater the number of teens in a vehicle, the more likely they are to have an accident. Talking on the phone also increases the risk of an accident, but “hands-free” driving shows little improvement in risk. Texting and driving is the leading cause of death among teens, accounting for 3,000 deaths annually according to a study by Cohen Children’s Medical Center, in New Hyde Park, N.Y., which surpasses drinking and driving; www.teendriversource.org reports the statistics on teen driving and stated that brain activity needed for driving is reduced by 37%. Many teens self-report texting and driving and “near accidents.”
Attention-deficit/hyperactivity disorder (ADHD) also has been shown to put teen drivers at increased risk. Teens with ADHD show two to four times the increased risk of crashes.Psychostimulants have been shown to significantly improve their attention during driving, and long-acting methylphenidate has been shown to more effective, even for nighttime driving, over the short-acting methylphenidate (Pediatrics 2006;118:2570-81).
Fairly recent changes in laws and driver education has shown significant improvement in accident rates. Graduated driver laws started in 1996, and now is the law in every state. The minimum requirements include a learner’s permit of 2 months of longer, night restriction, and passenger restriction; states vary in their requirements. Optimally, graduated driver laws include a three-phase program that starts with the learner’s permit, vision screen, and driver’s test. Phase two is supervised driving, which also requires 6 months of no violations, 12 months of no crashes, and the road test. Phase three is a full license without restrictions.
Analysis of this program by state showed a significant reduction in crashes among the 15- to 19-year-olds. The reduction was mostly attributed to the restriction in nighttime driving, restricted number of passengers, and the extend period of supervised driving. In 1997, Florida’s first full year of its graduated driver law system, there was a 9% reduction in fatal and injury crashes for 15- to 17-year-olds, compared with 1995. All of these are important teaching points for parents; the National Highway Traffic Safety Administration is an excellent resource for statistics on the distracted driver to encourage teens to put the phones down.
Motor vehicle accidents are the No. 1 cause of death for teens, according to the Centers for Disease Control and Prevention. If our role as a pediatrician is to prevent morbidity and mortality, then we must play an active role in educating our patients on seriousness of safe driving. Just as we promote vaccines for the prevention of illness, we must promote the rules of the road to prevent an early and avoidable death.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at pdnews@frontlinemedcom.com.
Reducing morbidity and mortality is the focus of medicine, and much of our day is spent focusing on this, but how much do we as pediatricians address on the leading cause of death in teens? Motor vehicle accidents are the leading cause of death among 15- to 20-year-olds. In 2011, about 2,650 teens in the United States aged 16-19 years were killed and almost 292,000 were treated in emergency departments for injuries suffered in motor vehicle crashes, according to the Centers for Disease Control and Prevention. In 2010, the American Academy of Pediatrics reaffirmed its statement that was published on teen drivers in 2006, which encouraged pediatricians to be active participants in the education and lobbying for laws that promote of safe driving.
It may appear to be out of the scope of treatment to educate on safe driving, but the reality is that many parents are unaware of the risk factors that contribute to unsafe driving, as well the conditions that can be managed to improve their driving ability.
The major risk factors for increased injury among teens are immaturity, which leads to increased risk taking; inexperience; and distractions. Immaturity is the leading risk factor, clearly demonstrated in the number of crashes involving 16-year-old drivers, which is two times greater when compared with 17-year-olds and three times greater when compared with 25- to 29-year-olds.
Although distracted driving is not a problem limited to just teens, that compounded with inexperience certainly explains why they account for 14% of fatal accidents despite being only 6% of drivers. It has been statistically shown that the greater the number of teens in a vehicle, the more likely they are to have an accident. Talking on the phone also increases the risk of an accident, but “hands-free” driving shows little improvement in risk. Texting and driving is the leading cause of death among teens, accounting for 3,000 deaths annually according to a study by Cohen Children’s Medical Center, in New Hyde Park, N.Y., which surpasses drinking and driving; www.teendriversource.org reports the statistics on teen driving and stated that brain activity needed for driving is reduced by 37%. Many teens self-report texting and driving and “near accidents.”
Attention-deficit/hyperactivity disorder (ADHD) also has been shown to put teen drivers at increased risk. Teens with ADHD show two to four times the increased risk of crashes.Psychostimulants have been shown to significantly improve their attention during driving, and long-acting methylphenidate has been shown to more effective, even for nighttime driving, over the short-acting methylphenidate (Pediatrics 2006;118:2570-81).
Fairly recent changes in laws and driver education has shown significant improvement in accident rates. Graduated driver laws started in 1996, and now is the law in every state. The minimum requirements include a learner’s permit of 2 months of longer, night restriction, and passenger restriction; states vary in their requirements. Optimally, graduated driver laws include a three-phase program that starts with the learner’s permit, vision screen, and driver’s test. Phase two is supervised driving, which also requires 6 months of no violations, 12 months of no crashes, and the road test. Phase three is a full license without restrictions.
Analysis of this program by state showed a significant reduction in crashes among the 15- to 19-year-olds. The reduction was mostly attributed to the restriction in nighttime driving, restricted number of passengers, and the extend period of supervised driving. In 1997, Florida’s first full year of its graduated driver law system, there was a 9% reduction in fatal and injury crashes for 15- to 17-year-olds, compared with 1995. All of these are important teaching points for parents; the National Highway Traffic Safety Administration is an excellent resource for statistics on the distracted driver to encourage teens to put the phones down.
Motor vehicle accidents are the No. 1 cause of death for teens, according to the Centers for Disease Control and Prevention. If our role as a pediatrician is to prevent morbidity and mortality, then we must play an active role in educating our patients on seriousness of safe driving. Just as we promote vaccines for the prevention of illness, we must promote the rules of the road to prevent an early and avoidable death.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at pdnews@frontlinemedcom.com.
Reducing morbidity and mortality is the focus of medicine, and much of our day is spent focusing on this, but how much do we as pediatricians address on the leading cause of death in teens? Motor vehicle accidents are the leading cause of death among 15- to 20-year-olds. In 2011, about 2,650 teens in the United States aged 16-19 years were killed and almost 292,000 were treated in emergency departments for injuries suffered in motor vehicle crashes, according to the Centers for Disease Control and Prevention. In 2010, the American Academy of Pediatrics reaffirmed its statement that was published on teen drivers in 2006, which encouraged pediatricians to be active participants in the education and lobbying for laws that promote of safe driving.
It may appear to be out of the scope of treatment to educate on safe driving, but the reality is that many parents are unaware of the risk factors that contribute to unsafe driving, as well the conditions that can be managed to improve their driving ability.
The major risk factors for increased injury among teens are immaturity, which leads to increased risk taking; inexperience; and distractions. Immaturity is the leading risk factor, clearly demonstrated in the number of crashes involving 16-year-old drivers, which is two times greater when compared with 17-year-olds and three times greater when compared with 25- to 29-year-olds.
Although distracted driving is not a problem limited to just teens, that compounded with inexperience certainly explains why they account for 14% of fatal accidents despite being only 6% of drivers. It has been statistically shown that the greater the number of teens in a vehicle, the more likely they are to have an accident. Talking on the phone also increases the risk of an accident, but “hands-free” driving shows little improvement in risk. Texting and driving is the leading cause of death among teens, accounting for 3,000 deaths annually according to a study by Cohen Children’s Medical Center, in New Hyde Park, N.Y., which surpasses drinking and driving; www.teendriversource.org reports the statistics on teen driving and stated that brain activity needed for driving is reduced by 37%. Many teens self-report texting and driving and “near accidents.”
Attention-deficit/hyperactivity disorder (ADHD) also has been shown to put teen drivers at increased risk. Teens with ADHD show two to four times the increased risk of crashes.Psychostimulants have been shown to significantly improve their attention during driving, and long-acting methylphenidate has been shown to more effective, even for nighttime driving, over the short-acting methylphenidate (Pediatrics 2006;118:2570-81).
Fairly recent changes in laws and driver education has shown significant improvement in accident rates. Graduated driver laws started in 1996, and now is the law in every state. The minimum requirements include a learner’s permit of 2 months of longer, night restriction, and passenger restriction; states vary in their requirements. Optimally, graduated driver laws include a three-phase program that starts with the learner’s permit, vision screen, and driver’s test. Phase two is supervised driving, which also requires 6 months of no violations, 12 months of no crashes, and the road test. Phase three is a full license without restrictions.
Analysis of this program by state showed a significant reduction in crashes among the 15- to 19-year-olds. The reduction was mostly attributed to the restriction in nighttime driving, restricted number of passengers, and the extend period of supervised driving. In 1997, Florida’s first full year of its graduated driver law system, there was a 9% reduction in fatal and injury crashes for 15- to 17-year-olds, compared with 1995. All of these are important teaching points for parents; the National Highway Traffic Safety Administration is an excellent resource for statistics on the distracted driver to encourage teens to put the phones down.
Motor vehicle accidents are the No. 1 cause of death for teens, according to the Centers for Disease Control and Prevention. If our role as a pediatrician is to prevent morbidity and mortality, then we must play an active role in educating our patients on seriousness of safe driving. Just as we promote vaccines for the prevention of illness, we must promote the rules of the road to prevent an early and avoidable death.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at pdnews@frontlinemedcom.com.

Sleep matters
Sleep deprivation being a health issue in adolescence is no surprise. We hear repeated reports on cellphone use and excessive video gaming as contributors to sleep deprivation, but how many pediatricians are actually warning their patient during annual exams about the health impact of sleep deprivation?
The American Academy of Pediatrics recently published its policy on sleep and recommended adolescents get at least 8.5 hours of sleep per night and that school start time for middle schools be 8:30 a.m. (Pediatrics 2014;134:642-9). Despite this recommendation, more than 60% of U.S. schools have start times earlier than 8:00 a.m. A recent study also showed that 59% of 6th-8th graders and 87% of high school students obtained less the recommended 8.5 hours.
The reasoning behind the recommendation was based on the natural change in sleep cycle that occurs during adolescence, in which the circadian rhythm changes, resulting in decreased secretion of melatonin and delayed onset of sleep. With later start times, adolescents actually get up to an extra hour of sleep, which in turn results in fewer absences, improved focus, concentration, and better behavior (Pediatrics 2014 [doi:10.1542/peds.2014-1697]).
But beyond biologic cause for delayed sleep, social media, texting, and video games further impact the amount of sleep obtained, which leaves the majority of teens sleep deprived. Watching TV more than 3 hours per night impacts your ability not only to fall asleep, but to stay asleep, which again increases daytime sleepiness. Many may think that the “weekend catch-up” might ameliorate the deprivation, but studies show that the inconsistency of appropriate sleep further disrupts the wake-sleep cycles and further reduces the secretion of melatonin.
So how does sleep deprivation impact health? The obvious increased daytime sleepiness which results in poor concentration and focus is well known, and clearly contributes to the number of car accidents in this age group. But there are clear physiologic changes that occur when there is inadequate sleep that result in increased risk for diabetes, obesity, depression, cardiovascular disease, and even Alzheimer’s (Psychiatry Res. 2010;176:34-9; Sleep 2004;27:1351-8; Endocr. Dev. 2010;17:11-21). Lack of sleep has shown alterations in metabolic profiles, such as insulin, cortisol, and leptin, which lead to insulin resistance, increased sympathetic nervous system activity, increased hunger, and decreased satiety (Pediatrics 2014 [doi:10.1542/peds.2014-1697]).
The resulting lack of sleep in adolescence has cause increased intake of caffeine as well. Recent surveys show that caffeine use has skyrocketed this age group. If it is taken in the form of energy drinks, coffee, or soda, people who drink excessive caffeine are twice as likely to have sleep issues and shortened REM sleep (J. Adolesc. 2009;32:1189-207). It suppresses appetite and has withdrawal symptoms that further increase daytime sleepiness.
Adolescents also show increased use of sleep aids and stimulant drinks that have significant side effects of residual daytime sleepiness and tachycardia, respectively. So the treatment is further impacting the problem.
As physicians, we need to emphasize the physiologic impact of sleep deprivation and how it impacts many of the symptoms with which patients present. Many patients may overlook limited sleep as a cause of their symptoms.
Natural alternatives for improved sleep include chamomile, passionflower, or valerian, which come as a tea, capsule, liquid, or essential oil. Magnesium with or without calcium also is commonly used. Although all are deemed generally safe, there is no definitive effective dose in pediatrics, and they are not without side effects, so caution should be used when recommending these. Almond milk is a rich source of calcium, and calcium in the brain gets converted to melatonin.
Suggesting to parents that cellphones, video games, and computers be removed from the bedrooms by 9 p.m. will allow for the required 8.5 hours sleep. Avoiding sleeping until noon on weekends will improve sleep cycles. Avoiding caffeinated drinks and eating at late hours also will improve the quality of sleep and lessen daytime sleepiness. But the best advice to parents is for them to be good role models, and for them to get the appropriate amount of sleep, so that they also can avoid the hazards of sleep deprivation.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at pdnews@frontlinemedcom.com. Scan this QR code or go to pediatricnews.com.
Sleep deprivation being a health issue in adolescence is no surprise. We hear repeated reports on cellphone use and excessive video gaming as contributors to sleep deprivation, but how many pediatricians are actually warning their patient during annual exams about the health impact of sleep deprivation?
The American Academy of Pediatrics recently published its policy on sleep and recommended adolescents get at least 8.5 hours of sleep per night and that school start time for middle schools be 8:30 a.m. (Pediatrics 2014;134:642-9). Despite this recommendation, more than 60% of U.S. schools have start times earlier than 8:00 a.m. A recent study also showed that 59% of 6th-8th graders and 87% of high school students obtained less the recommended 8.5 hours.
The reasoning behind the recommendation was based on the natural change in sleep cycle that occurs during adolescence, in which the circadian rhythm changes, resulting in decreased secretion of melatonin and delayed onset of sleep. With later start times, adolescents actually get up to an extra hour of sleep, which in turn results in fewer absences, improved focus, concentration, and better behavior (Pediatrics 2014 [doi:10.1542/peds.2014-1697]).
But beyond biologic cause for delayed sleep, social media, texting, and video games further impact the amount of sleep obtained, which leaves the majority of teens sleep deprived. Watching TV more than 3 hours per night impacts your ability not only to fall asleep, but to stay asleep, which again increases daytime sleepiness. Many may think that the “weekend catch-up” might ameliorate the deprivation, but studies show that the inconsistency of appropriate sleep further disrupts the wake-sleep cycles and further reduces the secretion of melatonin.
So how does sleep deprivation impact health? The obvious increased daytime sleepiness which results in poor concentration and focus is well known, and clearly contributes to the number of car accidents in this age group. But there are clear physiologic changes that occur when there is inadequate sleep that result in increased risk for diabetes, obesity, depression, cardiovascular disease, and even Alzheimer’s (Psychiatry Res. 2010;176:34-9; Sleep 2004;27:1351-8; Endocr. Dev. 2010;17:11-21). Lack of sleep has shown alterations in metabolic profiles, such as insulin, cortisol, and leptin, which lead to insulin resistance, increased sympathetic nervous system activity, increased hunger, and decreased satiety (Pediatrics 2014 [doi:10.1542/peds.2014-1697]).
The resulting lack of sleep in adolescence has cause increased intake of caffeine as well. Recent surveys show that caffeine use has skyrocketed this age group. If it is taken in the form of energy drinks, coffee, or soda, people who drink excessive caffeine are twice as likely to have sleep issues and shortened REM sleep (J. Adolesc. 2009;32:1189-207). It suppresses appetite and has withdrawal symptoms that further increase daytime sleepiness.
Adolescents also show increased use of sleep aids and stimulant drinks that have significant side effects of residual daytime sleepiness and tachycardia, respectively. So the treatment is further impacting the problem.
As physicians, we need to emphasize the physiologic impact of sleep deprivation and how it impacts many of the symptoms with which patients present. Many patients may overlook limited sleep as a cause of their symptoms.
Natural alternatives for improved sleep include chamomile, passionflower, or valerian, which come as a tea, capsule, liquid, or essential oil. Magnesium with or without calcium also is commonly used. Although all are deemed generally safe, there is no definitive effective dose in pediatrics, and they are not without side effects, so caution should be used when recommending these. Almond milk is a rich source of calcium, and calcium in the brain gets converted to melatonin.
Suggesting to parents that cellphones, video games, and computers be removed from the bedrooms by 9 p.m. will allow for the required 8.5 hours sleep. Avoiding sleeping until noon on weekends will improve sleep cycles. Avoiding caffeinated drinks and eating at late hours also will improve the quality of sleep and lessen daytime sleepiness. But the best advice to parents is for them to be good role models, and for them to get the appropriate amount of sleep, so that they also can avoid the hazards of sleep deprivation.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at pdnews@frontlinemedcom.com. Scan this QR code or go to pediatricnews.com.
Sleep deprivation being a health issue in adolescence is no surprise. We hear repeated reports on cellphone use and excessive video gaming as contributors to sleep deprivation, but how many pediatricians are actually warning their patient during annual exams about the health impact of sleep deprivation?
The American Academy of Pediatrics recently published its policy on sleep and recommended adolescents get at least 8.5 hours of sleep per night and that school start time for middle schools be 8:30 a.m. (Pediatrics 2014;134:642-9). Despite this recommendation, more than 60% of U.S. schools have start times earlier than 8:00 a.m. A recent study also showed that 59% of 6th-8th graders and 87% of high school students obtained less the recommended 8.5 hours.
The reasoning behind the recommendation was based on the natural change in sleep cycle that occurs during adolescence, in which the circadian rhythm changes, resulting in decreased secretion of melatonin and delayed onset of sleep. With later start times, adolescents actually get up to an extra hour of sleep, which in turn results in fewer absences, improved focus, concentration, and better behavior (Pediatrics 2014 [doi:10.1542/peds.2014-1697]).
But beyond biologic cause for delayed sleep, social media, texting, and video games further impact the amount of sleep obtained, which leaves the majority of teens sleep deprived. Watching TV more than 3 hours per night impacts your ability not only to fall asleep, but to stay asleep, which again increases daytime sleepiness. Many may think that the “weekend catch-up” might ameliorate the deprivation, but studies show that the inconsistency of appropriate sleep further disrupts the wake-sleep cycles and further reduces the secretion of melatonin.
So how does sleep deprivation impact health? The obvious increased daytime sleepiness which results in poor concentration and focus is well known, and clearly contributes to the number of car accidents in this age group. But there are clear physiologic changes that occur when there is inadequate sleep that result in increased risk for diabetes, obesity, depression, cardiovascular disease, and even Alzheimer’s (Psychiatry Res. 2010;176:34-9; Sleep 2004;27:1351-8; Endocr. Dev. 2010;17:11-21). Lack of sleep has shown alterations in metabolic profiles, such as insulin, cortisol, and leptin, which lead to insulin resistance, increased sympathetic nervous system activity, increased hunger, and decreased satiety (Pediatrics 2014 [doi:10.1542/peds.2014-1697]).
The resulting lack of sleep in adolescence has cause increased intake of caffeine as well. Recent surveys show that caffeine use has skyrocketed this age group. If it is taken in the form of energy drinks, coffee, or soda, people who drink excessive caffeine are twice as likely to have sleep issues and shortened REM sleep (J. Adolesc. 2009;32:1189-207). It suppresses appetite and has withdrawal symptoms that further increase daytime sleepiness.
Adolescents also show increased use of sleep aids and stimulant drinks that have significant side effects of residual daytime sleepiness and tachycardia, respectively. So the treatment is further impacting the problem.
As physicians, we need to emphasize the physiologic impact of sleep deprivation and how it impacts many of the symptoms with which patients present. Many patients may overlook limited sleep as a cause of their symptoms.
Natural alternatives for improved sleep include chamomile, passionflower, or valerian, which come as a tea, capsule, liquid, or essential oil. Magnesium with or without calcium also is commonly used. Although all are deemed generally safe, there is no definitive effective dose in pediatrics, and they are not without side effects, so caution should be used when recommending these. Almond milk is a rich source of calcium, and calcium in the brain gets converted to melatonin.
Suggesting to parents that cellphones, video games, and computers be removed from the bedrooms by 9 p.m. will allow for the required 8.5 hours sleep. Avoiding sleeping until noon on weekends will improve sleep cycles. Avoiding caffeinated drinks and eating at late hours also will improve the quality of sleep and lessen daytime sleepiness. But the best advice to parents is for them to be good role models, and for them to get the appropriate amount of sleep, so that they also can avoid the hazards of sleep deprivation.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at pdnews@frontlinemedcom.com. Scan this QR code or go to pediatricnews.com.

Exercise-induced Anaphylaxis
Anaphylaxis is a relatively common occurrence for many adolescents. As primary care doctors, we normally see the patient after the acute phase, and then are required to do the detective work to figure out the causes of the episode. The cause may be obvious, but many times we have to hope for another occurrence with similar circumstances to identify it. Surprisingly, the cause may not be what you think. Factors that contribute to an anaphylaxis response may be related to activity, timing of food ingestion, an environmental factor, or medication.
Let’s look at just one type, exercise-induced anaphylaxis. It’s divided into two categories: food dependent and nonfood dependent. Both are described as an induction of itching, urticaria, and fatigue, with progression to angioedema and hypotension, associated with exercise (J. Allergy Clin. Immunol. 1980;66:106-11).
Food-dependent exercise-induced anaphylaxis occurs when exercise is started 30 minutes after ingesting food. This may be difficult to identify because patients react to the food only if they exercise, so food is usually eliminated as a cause. Wheat and wheat flour are common culprits for this type of reaction because of the omega-5 gliadin, which is the protein in gluten (J. Allergy Clin. Immunol. 1991;87:34-40). In one study, larger amounts of the suspected agent were given; hives and angioedema did start to occur in 20% of patients challenged, which suggested that there was likely a baseline allergy to the food, and exercise itself might be a cofactor in augmentation of the allergic reaction.
In nonfood-dependent exercise-induced anaphylaxis, symptoms of itching, urticaria, and fatigue can occur 5-30 minutes after the start of exercise. Although bronchospasm is rare, it can occur along with angioedema, nausea, vomiting, and hypotension, and can even be fatal if exercise continues. If exercise is stopped, it usually resolves. However, many people try to push through it, which only worsens the symptoms.
Cofactors associated with nonfood-dependent exercise-induced anaphylaxis are ingestion of alcohol and an NSAID several hours beforehand. These agents also might be overlooked if well tolerated independently (Br. J. Dermatol. 2001;145:336-9).
Timing of the episode also plays a role. Premenstrual syndrome can be a factor in augmentation of anaphylaxis, so it also should be considered. Knowing the date of the last menstrual cycle and identifying if the anaphylaxis is episodic will identify premenstrual syndrome as a cause.
The work-up should include standard allergy testing and determination of tryptase levels. Skin testing is essential to identify offending agents, and is rarely negative. If a food is suspected and skin testing is negative, repeat the skin testing in 6 months. In one study, wheat extract was found to be positive in only 29% of persons suspected of having a wheat allergy, but when the paste of wheat flour was tested, 80% were identified. The ImmunoCAP Test also was found to have a sensitivity of 80%, so it is a valuable test to try along with the skin prick.
Tryptase levels should be evaluated because in nonfood-dependent exercise-induced anaphylaxis, these levels are slightly elevated at the time of the anaphylaxis, but return to normal. A patient with mastocytosis, a group of disorders characterized by pathologic mast cells infiltrating the skin, will consistently have elevated tryptase levels. Seasonal allergies associated with pollen, and asthma bronchospasm also should be considered as causes.
Although these exercise-induced anaphylaxis episodes can occur at any age, they are most frequent in the adolescent age group, probably because that’s the time most of this population are involved in organized sports. Upon presentation, a careful detailed history will help to identify the cause of anaphylaxis and result in quicker resolution.
Treatment includes avoidance of the offending agent if identified and an antihistamine, and if symptoms do occur, ceasing exercise immediately to avoid a full-blown anaphylactic reaction.
Dr. Pearce is a pediatrician in Frankfort, Ill.
Anaphylaxis is a relatively common occurrence for many adolescents. As primary care doctors, we normally see the patient after the acute phase, and then are required to do the detective work to figure out the causes of the episode. The cause may be obvious, but many times we have to hope for another occurrence with similar circumstances to identify it. Surprisingly, the cause may not be what you think. Factors that contribute to an anaphylaxis response may be related to activity, timing of food ingestion, an environmental factor, or medication.
Let’s look at just one type, exercise-induced anaphylaxis. It’s divided into two categories: food dependent and nonfood dependent. Both are described as an induction of itching, urticaria, and fatigue, with progression to angioedema and hypotension, associated with exercise (J. Allergy Clin. Immunol. 1980;66:106-11).
Food-dependent exercise-induced anaphylaxis occurs when exercise is started 30 minutes after ingesting food. This may be difficult to identify because patients react to the food only if they exercise, so food is usually eliminated as a cause. Wheat and wheat flour are common culprits for this type of reaction because of the omega-5 gliadin, which is the protein in gluten (J. Allergy Clin. Immunol. 1991;87:34-40). In one study, larger amounts of the suspected agent were given; hives and angioedema did start to occur in 20% of patients challenged, which suggested that there was likely a baseline allergy to the food, and exercise itself might be a cofactor in augmentation of the allergic reaction.
In nonfood-dependent exercise-induced anaphylaxis, symptoms of itching, urticaria, and fatigue can occur 5-30 minutes after the start of exercise. Although bronchospasm is rare, it can occur along with angioedema, nausea, vomiting, and hypotension, and can even be fatal if exercise continues. If exercise is stopped, it usually resolves. However, many people try to push through it, which only worsens the symptoms.
Cofactors associated with nonfood-dependent exercise-induced anaphylaxis are ingestion of alcohol and an NSAID several hours beforehand. These agents also might be overlooked if well tolerated independently (Br. J. Dermatol. 2001;145:336-9).
Timing of the episode also plays a role. Premenstrual syndrome can be a factor in augmentation of anaphylaxis, so it also should be considered. Knowing the date of the last menstrual cycle and identifying if the anaphylaxis is episodic will identify premenstrual syndrome as a cause.
The work-up should include standard allergy testing and determination of tryptase levels. Skin testing is essential to identify offending agents, and is rarely negative. If a food is suspected and skin testing is negative, repeat the skin testing in 6 months. In one study, wheat extract was found to be positive in only 29% of persons suspected of having a wheat allergy, but when the paste of wheat flour was tested, 80% were identified. The ImmunoCAP Test also was found to have a sensitivity of 80%, so it is a valuable test to try along with the skin prick.
Tryptase levels should be evaluated because in nonfood-dependent exercise-induced anaphylaxis, these levels are slightly elevated at the time of the anaphylaxis, but return to normal. A patient with mastocytosis, a group of disorders characterized by pathologic mast cells infiltrating the skin, will consistently have elevated tryptase levels. Seasonal allergies associated with pollen, and asthma bronchospasm also should be considered as causes.
Although these exercise-induced anaphylaxis episodes can occur at any age, they are most frequent in the adolescent age group, probably because that’s the time most of this population are involved in organized sports. Upon presentation, a careful detailed history will help to identify the cause of anaphylaxis and result in quicker resolution.
Treatment includes avoidance of the offending agent if identified and an antihistamine, and if symptoms do occur, ceasing exercise immediately to avoid a full-blown anaphylactic reaction.
Dr. Pearce is a pediatrician in Frankfort, Ill.
Anaphylaxis is a relatively common occurrence for many adolescents. As primary care doctors, we normally see the patient after the acute phase, and then are required to do the detective work to figure out the causes of the episode. The cause may be obvious, but many times we have to hope for another occurrence with similar circumstances to identify it. Surprisingly, the cause may not be what you think. Factors that contribute to an anaphylaxis response may be related to activity, timing of food ingestion, an environmental factor, or medication.
Let’s look at just one type, exercise-induced anaphylaxis. It’s divided into two categories: food dependent and nonfood dependent. Both are described as an induction of itching, urticaria, and fatigue, with progression to angioedema and hypotension, associated with exercise (J. Allergy Clin. Immunol. 1980;66:106-11).
Food-dependent exercise-induced anaphylaxis occurs when exercise is started 30 minutes after ingesting food. This may be difficult to identify because patients react to the food only if they exercise, so food is usually eliminated as a cause. Wheat and wheat flour are common culprits for this type of reaction because of the omega-5 gliadin, which is the protein in gluten (J. Allergy Clin. Immunol. 1991;87:34-40). In one study, larger amounts of the suspected agent were given; hives and angioedema did start to occur in 20% of patients challenged, which suggested that there was likely a baseline allergy to the food, and exercise itself might be a cofactor in augmentation of the allergic reaction.
In nonfood-dependent exercise-induced anaphylaxis, symptoms of itching, urticaria, and fatigue can occur 5-30 minutes after the start of exercise. Although bronchospasm is rare, it can occur along with angioedema, nausea, vomiting, and hypotension, and can even be fatal if exercise continues. If exercise is stopped, it usually resolves. However, many people try to push through it, which only worsens the symptoms.
Cofactors associated with nonfood-dependent exercise-induced anaphylaxis are ingestion of alcohol and an NSAID several hours beforehand. These agents also might be overlooked if well tolerated independently (Br. J. Dermatol. 2001;145:336-9).
Timing of the episode also plays a role. Premenstrual syndrome can be a factor in augmentation of anaphylaxis, so it also should be considered. Knowing the date of the last menstrual cycle and identifying if the anaphylaxis is episodic will identify premenstrual syndrome as a cause.
The work-up should include standard allergy testing and determination of tryptase levels. Skin testing is essential to identify offending agents, and is rarely negative. If a food is suspected and skin testing is negative, repeat the skin testing in 6 months. In one study, wheat extract was found to be positive in only 29% of persons suspected of having a wheat allergy, but when the paste of wheat flour was tested, 80% were identified. The ImmunoCAP Test also was found to have a sensitivity of 80%, so it is a valuable test to try along with the skin prick.
Tryptase levels should be evaluated because in nonfood-dependent exercise-induced anaphylaxis, these levels are slightly elevated at the time of the anaphylaxis, but return to normal. A patient with mastocytosis, a group of disorders characterized by pathologic mast cells infiltrating the skin, will consistently have elevated tryptase levels. Seasonal allergies associated with pollen, and asthma bronchospasm also should be considered as causes.
Although these exercise-induced anaphylaxis episodes can occur at any age, they are most frequent in the adolescent age group, probably because that’s the time most of this population are involved in organized sports. Upon presentation, a careful detailed history will help to identify the cause of anaphylaxis and result in quicker resolution.
Treatment includes avoidance of the offending agent if identified and an antihistamine, and if symptoms do occur, ceasing exercise immediately to avoid a full-blown anaphylactic reaction.
Dr. Pearce is a pediatrician in Frankfort, Ill.
