User login
When macrosomia is suspected at term, does induction of labor lower the risk of cesarean delivery?
Fetal and neonatal macrosomia can lead to morbidity for both mother and infant. Larger babies put the mother at risk of cesarean delivery, severe perineal lacerations, and hemorrhage. The macrosomic fetus faces an elevated risk of birth trauma, shoulder dystocia, and metabolic disorders.
Earlier investigations have concluded that induction of labor does not improve outcomes and may increase the risk of cesarean delivery.1 The American Congress of Obstetricians and Gynecologists (ACOG) does not support suspected fetal macrosomia as an indication for induction of labor.2
Details of the study
The objective of this study was to determine whether women who were carrying a macrosomic fetus and who underwent induction of labor had a higher rate of cesarean delivery than those who were managed expectantly. Using data from the 2003 Vital Statistics Natality birth certificate registry, Cheng and colleagues compared women who underwent induction of labor at 39 weeks with women who were managed expectantly and who delivered at 40, 41, or 42 weeks (by induced or spontaneous labor).
Investigators attempted to adjust for normal gestational growth by assuming a fetal weight gain of 200 g for each additional week of gestation in the women managed expectantly. For instance, one group included women who delivered at 39 weeks (birth weight of 3,875–4,125 g), and they were compared with the group of women who delivered at 40 weeks (birth weight of 4,075–4,325 g), 41 weeks (4,275–4,525 g), and 42 weeks (4,475–4,725 g).
Using this scheme, cesarean delivery was lower in the group of women who underwent induction of labor. The induced groups were also found to have lower odds of composite neonatal morbidity.
Strengths and limitations
Because this was a retrospective study, investigators were able to use known birth weights, rather than estimated birth weights, to overcome misclassifications that can arise with estimates.
Cheng and colleagues refuted the findings of earlier studies that found a higher risk of cesarean delivery with induction of labor. They argued that those investigations compared women who underwent induction of labor with those who experienced spontaneous labor instead of the proper comparison—between women who underwent induction of labor and those who were managed expectantly. Although the comparisons they used in this study alleviate that problem, the retrospective nature of the study necessitated the use of multiple assumptions to allocate each group, creating selection bias.
Group allocations and medical histories cannot be confirmed, and the investigators acknowledge that their conclusions regarding neonatal morbidity lack statistical power.
This study explores an important issue—the prevention of cesarean delivery and poor neonatal outcomes associated with macrosomia. The comparisons in this investigation cast earlier conclusions in question and elucidate potential improvements in neonatal outcomes.
However, because of the numerous assumptions underlying the study groups, I would not recommend induction of labor to reduce the rate of cesarean delivery until further prospective data are available.
Jennifer T. Ahn, MD
We want to hear from you! Tell us what you think.
Fetal and neonatal macrosomia can lead to morbidity for both mother and infant. Larger babies put the mother at risk of cesarean delivery, severe perineal lacerations, and hemorrhage. The macrosomic fetus faces an elevated risk of birth trauma, shoulder dystocia, and metabolic disorders.
Earlier investigations have concluded that induction of labor does not improve outcomes and may increase the risk of cesarean delivery.1 The American Congress of Obstetricians and Gynecologists (ACOG) does not support suspected fetal macrosomia as an indication for induction of labor.2
Details of the study
The objective of this study was to determine whether women who were carrying a macrosomic fetus and who underwent induction of labor had a higher rate of cesarean delivery than those who were managed expectantly. Using data from the 2003 Vital Statistics Natality birth certificate registry, Cheng and colleagues compared women who underwent induction of labor at 39 weeks with women who were managed expectantly and who delivered at 40, 41, or 42 weeks (by induced or spontaneous labor).
Investigators attempted to adjust for normal gestational growth by assuming a fetal weight gain of 200 g for each additional week of gestation in the women managed expectantly. For instance, one group included women who delivered at 39 weeks (birth weight of 3,875–4,125 g), and they were compared with the group of women who delivered at 40 weeks (birth weight of 4,075–4,325 g), 41 weeks (4,275–4,525 g), and 42 weeks (4,475–4,725 g).
Using this scheme, cesarean delivery was lower in the group of women who underwent induction of labor. The induced groups were also found to have lower odds of composite neonatal morbidity.
Strengths and limitations
Because this was a retrospective study, investigators were able to use known birth weights, rather than estimated birth weights, to overcome misclassifications that can arise with estimates.
Cheng and colleagues refuted the findings of earlier studies that found a higher risk of cesarean delivery with induction of labor. They argued that those investigations compared women who underwent induction of labor with those who experienced spontaneous labor instead of the proper comparison—between women who underwent induction of labor and those who were managed expectantly. Although the comparisons they used in this study alleviate that problem, the retrospective nature of the study necessitated the use of multiple assumptions to allocate each group, creating selection bias.
Group allocations and medical histories cannot be confirmed, and the investigators acknowledge that their conclusions regarding neonatal morbidity lack statistical power.
This study explores an important issue—the prevention of cesarean delivery and poor neonatal outcomes associated with macrosomia. The comparisons in this investigation cast earlier conclusions in question and elucidate potential improvements in neonatal outcomes.
However, because of the numerous assumptions underlying the study groups, I would not recommend induction of labor to reduce the rate of cesarean delivery until further prospective data are available.
Jennifer T. Ahn, MD
We want to hear from you! Tell us what you think.
Fetal and neonatal macrosomia can lead to morbidity for both mother and infant. Larger babies put the mother at risk of cesarean delivery, severe perineal lacerations, and hemorrhage. The macrosomic fetus faces an elevated risk of birth trauma, shoulder dystocia, and metabolic disorders.
Earlier investigations have concluded that induction of labor does not improve outcomes and may increase the risk of cesarean delivery.1 The American Congress of Obstetricians and Gynecologists (ACOG) does not support suspected fetal macrosomia as an indication for induction of labor.2
Details of the study
The objective of this study was to determine whether women who were carrying a macrosomic fetus and who underwent induction of labor had a higher rate of cesarean delivery than those who were managed expectantly. Using data from the 2003 Vital Statistics Natality birth certificate registry, Cheng and colleagues compared women who underwent induction of labor at 39 weeks with women who were managed expectantly and who delivered at 40, 41, or 42 weeks (by induced or spontaneous labor).
Investigators attempted to adjust for normal gestational growth by assuming a fetal weight gain of 200 g for each additional week of gestation in the women managed expectantly. For instance, one group included women who delivered at 39 weeks (birth weight of 3,875–4,125 g), and they were compared with the group of women who delivered at 40 weeks (birth weight of 4,075–4,325 g), 41 weeks (4,275–4,525 g), and 42 weeks (4,475–4,725 g).
Using this scheme, cesarean delivery was lower in the group of women who underwent induction of labor. The induced groups were also found to have lower odds of composite neonatal morbidity.
Strengths and limitations
Because this was a retrospective study, investigators were able to use known birth weights, rather than estimated birth weights, to overcome misclassifications that can arise with estimates.
Cheng and colleagues refuted the findings of earlier studies that found a higher risk of cesarean delivery with induction of labor. They argued that those investigations compared women who underwent induction of labor with those who experienced spontaneous labor instead of the proper comparison—between women who underwent induction of labor and those who were managed expectantly. Although the comparisons they used in this study alleviate that problem, the retrospective nature of the study necessitated the use of multiple assumptions to allocate each group, creating selection bias.
Group allocations and medical histories cannot be confirmed, and the investigators acknowledge that their conclusions regarding neonatal morbidity lack statistical power.
This study explores an important issue—the prevention of cesarean delivery and poor neonatal outcomes associated with macrosomia. The comparisons in this investigation cast earlier conclusions in question and elucidate potential improvements in neonatal outcomes.
However, because of the numerous assumptions underlying the study groups, I would not recommend induction of labor to reduce the rate of cesarean delivery until further prospective data are available.
Jennifer T. Ahn, MD
We want to hear from you! Tell us what you think.
The short cervix in pregnancy: Which therapy reduces preterm birth?
- An extensive history is essential to identify the gravida at risk for a shortened cervical length.
- Transvaginal measurement of cervical lengths less than 26 mm has a high predictive value for preterm delivery.
- Prophylactic cerclage should be offered to patients with a classic history of cervical incompetence.
- The benefits of therapeutic cerclage for a shortened cervix remain uncertain, especially in women deemed to have a low risk of preterm delivery.
You are in your busy office, running behind schedule, when you receive a frantic notice from the ultrasound department that your patient—a primigravida scheduled for a routine anatomy survey at 21 weeks’ gestation—has a cervical length of 19 mm with funneling. What are your management options if the patient reports no contractions or changes in vaginal discharge?
With today’s emphasis on evidence-based medicine, it often is difficult to decide on an appropriate course of action, especially when conflicting reports abound. This article reviews the best studies available and presents a practical algorithm (FIGURE 1) to guide management of this difficult dilemma.
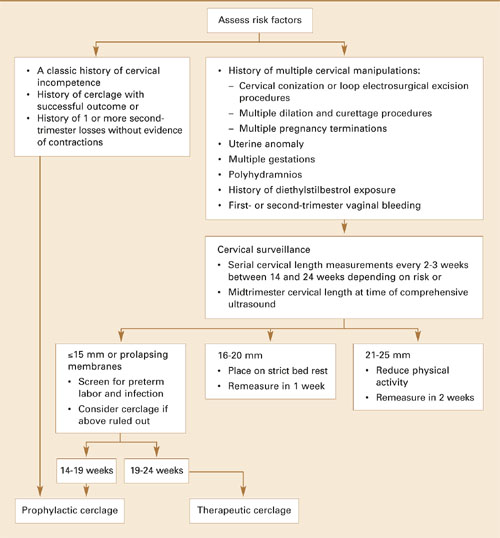
FIGURE 1 Management strategy for women with risk factors for cervical incompetence, preterm delivery
Predicting the need for cerclage
Despite numerous explorations of its pathophysiology, no irrefutable data explain what triggers the cascade of events leading to preterm birth, which remains a leading cause of morbidity and mortality. Cervical incompetence has been studied extensively as a possible cause, often without conclusive results.
Traditionally, cervical incompetence is defined as dilatation in the absence of contractions, usually presenting in the second trimester.1 Possible causes include prior obstetric or gynecologic injury, increased uterine volume (ie, multiple gestation, polyhydramnios), biological variation, and—currently under investigation—response to inflammatory mediators.2
In gravidas deemed to have biological or structural cervical incompetence, prophylactic cerclage is often placed at 12 to 14 weeks’ gestation. Alternatively, a therapeutic or “rescue” cerclage sometimes is placed at 20 weeks or more when evidence of cervical shortening or funneling is noted incidentally on ultrasound examination. At times, therapeutic cerclage becomes an emergency if prolapsing membranes are found.
With improvements in ultrasound imaging, transvaginal measurement of cervical length has become useful for guiding decisions on the need for cerclage.3,4 Unfortunately, current studies report conflicting data on the outcomes of pregnancies managed with cerclage placement based on ultrasound imaging.5-7
Ultrasound evaluation: Cervical length and other variables
In unselected general obstetric populations, preterm birth is associated with decreasing cervical length not only at 24 and 28 weeks’ gestation, but as early as 16 to 22 weeks’ gestation.8-14 Decreasing cervical length also predicts preterm birth in women at risk for early delivery.15,16 As a result, sonographic visualization of cervical length has evolved into a common practice to help predict early delivery.
An extensive history may offer clues as to what may have caused a shortened cervix in a previous pregnancy.
Iams et al17 compared cervical length with fetal fibronectin and noted that cervical length is more sensitive (39% versus 23%) but has a lower positive predictive value (PPV) (14% versus 20%). In combination, the modalities improved PPV to 50%. However, a separate study by Heath et al18 suggested that women with a cervical length of 15 mm or less had a relative risk of preterm birth 6 times greater than those with positive fetal fibronectin alone.
As sonographic technology has advanced, cervical characteristics have been assessed in a variety of ways. Besides measuring cervical length, experts also look for funneling, dilatation, prolapsing membranes, and dynamic changes elicited with transfundal or suprapubic pressure.4,19,20
Although cervical length can be measured transabdominally and transperineally, transvaginal assessment is most accurate. Transvaginal measurements also are more predictive and reproducible than traditional digital cervical examinations.16,21,22
Basic parameters. Standard cervical measurements use the “white stripe” of the internal cervical os as an anatomic landmark for proper caliper placement (FIGURE 2). As for dimensions of the nonlaboring cervix, Anderson23 found an average length of 45±7 mm at 14 to 30 weeks, and Iams et al10 found a mean cervical length of 35±8 mm at 24 weeks’ gestation after studying more than 2,900 gravidas. In another investigation, Hibbard and colleagues found a mean cervical length of 38.5±8 mm at 20 weeks’ gestation.12
Cervical length and diameter should remain constant as gestation progresses in both primiparous and multiparous women.22
Defining the short cervix. In a multicenter clinical trial, Iams et al10 measured the length of the cervix at 24 and 28 weeks in an unselected gravid population and determined that a length less than 26 mm at 24 weeks increases the relative risk for preterm delivery by a factor of 6.19, with a sensitivity of 37% for delivery before 35 weeks and a PPV of 18%—thus establishing the definition of a short cervix.
They also noted that the likelihood of spontaneous preterm delivery increased exponentially the shorter the cervical measurement. Hibbard et al12 attained similar findings with cervical measurements obtained at 16 to 22 weeks’ gestation in an unselected population, verifying the value of cervical measurements at an earlier gestational age in predicting preterm delivery.
In a retrospective cohort study, Hassan et al9 reviewed cervical measurements in an unselected population between 14 and 24 weeks, and found that close to 50% of gravidas with a cervical length of 15 mm or less delivered earlier than 32 weeks’ gestation. They therefore suggest that cervical length be measured early in the second trimester to obtain more accurate assessment of underlying risk for cervical incompetence.9
Interpreting cervical characteristics. As mentioned, other cervical qualities are useful to assess, such as funneling (and measurement of the residual cervix if funneling is present), v-shaped lower uterine segment (FIGURE 2), and dynamic changes with fundal or suprapubic pressure.3,10,19 Consistency of measurement—with careful attention to both intraoperator and interoperator variability—is vital when using these findings for clinical decision-making.1,10
Focus screening on women at risk. The sensitivity and predictive value of cervical length improve when screening is limited to populations at greatest risk: women with a history of preterm delivery, cervical surgery, or previous midtrimester loss or cervical incompetence. Conversely, positive and negative predictive values are low when measurements are performed in a low-risk population.17
Still, determining which gravidas are at highest risk of preterm delivery is a challenge; a careful obstetric history is the most important tool (TABLE).4,15,16,24 In addition to the factors listed in the table, any history of successful cerclage placement is also significant.25 An extensive history also may offer clues as to what may have caused a shortened cervix in a previous pregnancy. Acquiring old medical records may further clarify the situation.
Unfortunately, the aforementioned trials, while documenting the predictive value of cervical measurements, reveal nothing about specific clinical interventions such as cerclage placement. Rather, they indicate the need for well-designed randomized trials.
The advisability of therapeutic cerclage varies from case to case, but prophylactic cerclage, in general, should be offered to women with a classic history of cervical incompetence or prior cerclage with a successful outcome.
FIGURE 2 Transvaginal ultrasound of shortened cervix with funneling

The cervical length is 1.11 cm with a “U”-shaped funnel measuring 2.51 cm by 1.47 cm.TABLE
Preterm delivery: Factors indicating high risk
|
Management options
Once a short cervix has been diagnosed, the obstetrician faces a morass of conflicting data on how to proceed. After reviewing the patient’s history to identify any obvious risk factors, attempt to rule out uterine contractions, ruptured membranes, and clinical or subclinical infection. Once these and any other causes are excluded, the primary management options are bed rest and placement of cervical cerclage. Unfortunately, this is an issue of great controversy, with no definitive evidence on which strategy is best.
Based on the data available, we suggest the following cervical surveillance (FIGURE 1):
- Perform initial cervical measurements in high-risk patients at 14 to 24 weeks’ gestation. Women with cervical lengths exceeding 26 mm should be reassessed in 2 to 3 weeks.
- Women with a cervical length between 21 and 25 mm should be placed on reduced physical activity with remeasurement in 2 weeks.
- Patients with a length between 16 and 20 mm should be placed on strict bed rest with remeasurement in 1 week.
- Only women with a cervical length of 15 mm or less should be considered for therapeutic cerclage.9,24
No evidence supports measuring cervical length or placing a cerclage in the low-risk patient.
Cerclage versus bed rest: Ambiguous evidence
Several nonrandomized retrospective observational trials of cerclage placement versus bed rest in the general obstetric population reported conflicting results. For example, Heath et al26 studied a low-risk obstetric population in Great Britain that underwent transvaginal measurements of cervical length. Women with lengths of 15 mm or less were managed expectantly (n=21) or had a Shirodkar cerclage placed (n=22). Only 5% in the cerclage group delivered prior to 32 weeks’ gestation, compared with 52% in the expectantly managed group. In a general obstetric population, Hibbard et al27 also found an increase in the duration of pregnancy (2 weeks) among women who underwent cerclage placement for a cervical length less than 26 mm (n=43), compared with those who had no cerclage placed (n=42).
In a retrospective review of an obstetric population with cervical lengths of 15 mm or less, Hassan et al28 compared women receiving cerclage (n=25) with those who did not (n=45). In contrast to the 2 trials just mentioned, cervical cerclage failed to decrease the rate of spontaneous preterm delivery. Moreover, patients with a cerclage had an increased incidence of premature rupture of membranes.
In a nonrandomized prospective observational trial of women at high risk for preterm delivery, Berghella et al15 reported that those undergoing cerclage (n=39) for cervical length less than 25 mm and/or for 25% funneling fared no better than women who did not undergo cerclage placement (n=24).
Randomized prospective controlled trials. Only 2 such trials have been reported to date, and their design and patient populations differ.
Althusius et al24 studied a high-risk population in the Cervical Incompetence Prevention Randomized Cervical Trial (CIPRACT), which involved primary randomization to determine the effects of prophylactic cerclage, and secondary randomization to determine the effects of therapeutic cerclage. Women with a history of preterm delivery before 34 weeks who had a “classic” history of cervical incompetence were allocated to prophylactic cerclage or no cerclage in the late first or early second trimester. Thus, these gravidas already met the diagnosis of cervical incompetence. Both groups were then followed with serial measurements of cervical length. A second randomization to therapeutic cerclage or bed rest occurred if a cervical length less than 25 mm was found before 27 weeks’ gestation. This trial showed a statistically significant greater mean gestational age and improved pregnancy outcomes among women in both groups who received a cerclage, suggesting that therapeutic cerclage is a viable management option in at-risk women with cervical shortening. Moreover, the study design of primary and secondary randomization offers a sound strategy for management.
To address the value of therapeutic cerclage, Rust et al5-7 designed a prospective, randomized trial of both high-risk and low-risk women with second-trimester shortened cervical measurements with funneling or a total cervical length less than 25 mm. These women were allocated to therapeutic cerclage or bed rest. Prior to randomization, all women underwent cervical and urinary cultures and amniotic fluid analysis to exclude underlying intra-amniotic infection. Both groups then were followed with weekly transvaginal cervical measurements. A rescue cerclage was placed if prolapsing membranes occurred in either group.
Although decreasing cervical length was associated with poorer pregnancy outcomes, cervical cerclage did not result in a statistically significant greater mean gestational age or improved perinatal outcome, contradicting the results reported in the CIPRACT trial. Furthermore, patients who needed rescue cerclage had the worst outcomes. One explanation may be that the CIPRACT trial included only patients with a history of cervical incompetence, whereas Rust et al included low-risk and high-risk women unexpectedly noted to have a shortened cervix—patients more akin to the woman described at the beginning of this article, and a more likely scenario for most obstetricians.
Until better evidence is available, the limited number of randomized, controlled trials addressing the issue of shortened cervical length should guide management. Using this information, several institutions have initiated “cervical surveillance” programs in which clinicians perform serial ultrasounds to assess changes in cervical length over time. The most recent results from the ongoing randomized trial by Rust et al7—the best evidence to date in both low-risk and high-risk women—offer the promise of answers to this issue.
The authors report no financial relationship with any companies whose products are mentioned in this article.
1. Iams JD. Cervical incompetence. In: Creasy RK, Resnik R, eds. Maternal-Fetal Medicine. 4th ed. Philadelphia, Pa: WB Saunders; 1999;445-464.
2. Guzman ER. Cervical length and spontaneous prematurity: laying the foundation for future interventional randomized trials for the short cervix. Ultrasound Obstet Gynecol. 2001;18:195-199.
3. Guzman ER, Forster JK, Vintzileos AM, et al. Pregnancy outcomes in women treated with elective versus ultrasound-indicated cervical cerclage. Ultrasound Obstet Gynecol. 1998;12:323-327.
4. Berghella V, Hass S, Chervoneva I, Hyslop T. Patients with prior second-trimester loss: prophylactic cerclage or serial transvaginal sonograms? Am J Obstet Gynecol. 2002;187:747-751.
5. Rust OA, Atlas RO, Jones KJ, Benham BN, Balducci J. A randomized trial of cerclage versus no cerclage among patients with ultrasonographically detected secondtrimester preterm dilatation of the internal os. Am J Obstet Gynecol. 2000;183:830-835.
6. Rust OA, Atlas RO, Reed J, van Gaalen J, Balducci J. Revisiting the short cervix detected by transvaginal ultrasound in the second trimester: why cerclage therapy may not help. Am J Obstet Gynecol. 2001;185:1098-1105.
7. Rust OA, Atlas RO, Fischl S, Depuy A, Kimmel S, Hess LW. Does cerclage therapy improve perinatal outcome in patients with a history of previous preterm birth and cervical changes on 2nd trimester transvaginal ultrasound? Am J Obstet Gynecol. 2002;187(suppl):S58.-
8. Iams JD, Johnson FF, Sonek K, et al. Cervical competence as a continuum: a study of ultrasonographic cervical length and obstetric performance. Am J Obstet Gynecol. 1995;174:1097-1106.
9. Hassan SS, Romero R, Berry SM, et al. Patients with an ultrasonographic cervical length ≤15 mm have nearly a 50% risk of early spontaneous preterm delivery. Am J Obstet Gynecol. 2000;182:1458-1467.
10. Iams JD, Goldenberg RL, Meis PJ, et al. The length of the cervix and the risk of spontaneous premature delivery. N Engl J Med. 1996;334:567-572.
11. Taipale P, Hilesmaa V. Sonographic measurement of uterine cervix at 18-22 weeks’ gestation and the risk of preterm delivery. Obstet Gynecol. 1998;92:902-907.
12. Hibbard JU, Tart M, Moawad AH. Cervical length at 16-22 weeks’ gestation and risk for preterm delivery. Obstet Gynecol. 2000;96:972-978.
13. Anderson HF, Nugent CE, Wanty SD, Hayashi RH. Prediction of risk for preterm delivery by ultrasonographic measurement of cervical length. Am J Obstet Gynecol. 1990;163:859-867.
14. Heath VC, Southall TR, Souka AP, Elisseou A, Nicholaides KH. Cervical length at 23 weeks of gestation: prediction of spontaneous preterm delivery. Ultrasound Obstet Gynecol. 1998;12(5):312-317.
15. Berghella V, Daly SF, Tolosa JE, et al. Prediction of preterm delivery with transvaginal ultrasonography of the cervix in patients with high-risk pregnancies: does cerclage prevent prematurity? Am J Obstet Gynecol. 1999;181:809-815.
16. Berghella V, Tolasa JE, Kuhlman K. Cervical ultrasound compared with manual examination as a predictor of preterm delivery. Am J Obstet Gynecol. 1997;177:723-730.
17. Iams JD, Goldenberg RL, Mercer BM, et al. The preterm prediction study: can low-risk women destined for spontaneous preterm birth be identified? Am J Obstet Gynecol. 2001;184:652-655.
18. Heath VC, Daskalakis G, Zagaliki A, Carvalho M, Nicolaides KH. Cervicovaginal fibronectin and cervical length at 23 weeks of gestation:relative risk of early preterm delivery. BJOG. 2000;107:1276-1281.
19. Guzman ER, Pisatowski DM, Vintzileos AM, et al. A comparison of ultrasonographically detected cervical changes in response to transfundal pressure, coughing, and standing in predicting cervical incompetence. Am J Obstet Gynecol. 1997;172:660-665.
20. Sonek J, Blumefeld M, Foley M, Johnson F, Iams J. Cervical length may change during ultrasonographic examination. Am J Obstet Gynecol. 1990;162:1355-1357.
21. Sonek JD, Iams JD, Blumefeld M, Johnson F, Landon M, Gabbe S. Measurement of cervical length in pregnancy: comparison between vaginal ultrasonography and digital examination. Obstet Gynecol. 1990;76:172-175.
22. Cook CM, Ellwood DA. A longitudinal study of the cervix in pregnancy using transvaginal ultrasound. BJOG. 1996;103:16-18.
23. Anderson HF. Transvaginal and transabdominal ultrasonography of the uterine cervix during pregnancy. J Clin Ultrasound. 1991;19:77-83.
24. Althuisius SM, Dekker GA, Hummel P, Bekedam D, van Geijn HP. Final results of the Cervical Incompetence Prevention Randomized Cervical Trial (CIPRACT): therapeutic cerclage with bed rest versus bed rest alone. Am J Obstet Gynecol. 2001;185:1106-1112.
25. Colombo DF, Iams JD. Cervical length and preterm labor. Clin Obstet Gynecol. 2000;43:735-745.
26. Heath VC, Souka AP, Erasmus I, Gibb DM, Nicolaides KH. Cervical length at 23 weeks’ gestation: the value of Shirodkar suture for the short cervix. Ultrasound Obstet Gynecol. 1998;12:318-322.
27. Hibbard JU, Snow J, Moawad AH. Short cervical length by ultrasound and cerclage. J Perinatol. 2000;20:161-165.
28. Hassan SS, Romero R, Maymon E, et al. Does cervical cerclage prevent preterm delivery in patients with short cervix? Am J Obstet Gynecol. 2001;184:1325-1331.
- An extensive history is essential to identify the gravida at risk for a shortened cervical length.
- Transvaginal measurement of cervical lengths less than 26 mm has a high predictive value for preterm delivery.
- Prophylactic cerclage should be offered to patients with a classic history of cervical incompetence.
- The benefits of therapeutic cerclage for a shortened cervix remain uncertain, especially in women deemed to have a low risk of preterm delivery.
You are in your busy office, running behind schedule, when you receive a frantic notice from the ultrasound department that your patient—a primigravida scheduled for a routine anatomy survey at 21 weeks’ gestation—has a cervical length of 19 mm with funneling. What are your management options if the patient reports no contractions or changes in vaginal discharge?
With today’s emphasis on evidence-based medicine, it often is difficult to decide on an appropriate course of action, especially when conflicting reports abound. This article reviews the best studies available and presents a practical algorithm (FIGURE 1) to guide management of this difficult dilemma.
FIGURE 1 Management strategy for women with risk factors for cervical incompetence, preterm delivery
Predicting the need for cerclage
Despite numerous explorations of its pathophysiology, no irrefutable data explain what triggers the cascade of events leading to preterm birth, which remains a leading cause of morbidity and mortality. Cervical incompetence has been studied extensively as a possible cause, often without conclusive results.
Traditionally, cervical incompetence is defined as dilatation in the absence of contractions, usually presenting in the second trimester.1 Possible causes include prior obstetric or gynecologic injury, increased uterine volume (ie, multiple gestation, polyhydramnios), biological variation, and—currently under investigation—response to inflammatory mediators.2
In gravidas deemed to have biological or structural cervical incompetence, prophylactic cerclage is often placed at 12 to 14 weeks’ gestation. Alternatively, a therapeutic or “rescue” cerclage sometimes is placed at 20 weeks or more when evidence of cervical shortening or funneling is noted incidentally on ultrasound examination. At times, therapeutic cerclage becomes an emergency if prolapsing membranes are found.
With improvements in ultrasound imaging, transvaginal measurement of cervical length has become useful for guiding decisions on the need for cerclage.3,4 Unfortunately, current studies report conflicting data on the outcomes of pregnancies managed with cerclage placement based on ultrasound imaging.5-7
Ultrasound evaluation: Cervical length and other variables
In unselected general obstetric populations, preterm birth is associated with decreasing cervical length not only at 24 and 28 weeks’ gestation, but as early as 16 to 22 weeks’ gestation.8-14 Decreasing cervical length also predicts preterm birth in women at risk for early delivery.15,16 As a result, sonographic visualization of cervical length has evolved into a common practice to help predict early delivery.
An extensive history may offer clues as to what may have caused a shortened cervix in a previous pregnancy.
Iams et al17 compared cervical length with fetal fibronectin and noted that cervical length is more sensitive (39% versus 23%) but has a lower positive predictive value (PPV) (14% versus 20%). In combination, the modalities improved PPV to 50%. However, a separate study by Heath et al18 suggested that women with a cervical length of 15 mm or less had a relative risk of preterm birth 6 times greater than those with positive fetal fibronectin alone.
As sonographic technology has advanced, cervical characteristics have been assessed in a variety of ways. Besides measuring cervical length, experts also look for funneling, dilatation, prolapsing membranes, and dynamic changes elicited with transfundal or suprapubic pressure.4,19,20
Although cervical length can be measured transabdominally and transperineally, transvaginal assessment is most accurate. Transvaginal measurements also are more predictive and reproducible than traditional digital cervical examinations.16,21,22
Basic parameters. Standard cervical measurements use the “white stripe” of the internal cervical os as an anatomic landmark for proper caliper placement (FIGURE 2). As for dimensions of the nonlaboring cervix, Anderson23 found an average length of 45±7 mm at 14 to 30 weeks, and Iams et al10 found a mean cervical length of 35±8 mm at 24 weeks’ gestation after studying more than 2,900 gravidas. In another investigation, Hibbard and colleagues found a mean cervical length of 38.5±8 mm at 20 weeks’ gestation.12
Cervical length and diameter should remain constant as gestation progresses in both primiparous and multiparous women.22
Defining the short cervix. In a multicenter clinical trial, Iams et al10 measured the length of the cervix at 24 and 28 weeks in an unselected gravid population and determined that a length less than 26 mm at 24 weeks increases the relative risk for preterm delivery by a factor of 6.19, with a sensitivity of 37% for delivery before 35 weeks and a PPV of 18%—thus establishing the definition of a short cervix.
They also noted that the likelihood of spontaneous preterm delivery increased exponentially the shorter the cervical measurement. Hibbard et al12 attained similar findings with cervical measurements obtained at 16 to 22 weeks’ gestation in an unselected population, verifying the value of cervical measurements at an earlier gestational age in predicting preterm delivery.
In a retrospective cohort study, Hassan et al9 reviewed cervical measurements in an unselected population between 14 and 24 weeks, and found that close to 50% of gravidas with a cervical length of 15 mm or less delivered earlier than 32 weeks’ gestation. They therefore suggest that cervical length be measured early in the second trimester to obtain more accurate assessment of underlying risk for cervical incompetence.9
Interpreting cervical characteristics. As mentioned, other cervical qualities are useful to assess, such as funneling (and measurement of the residual cervix if funneling is present), v-shaped lower uterine segment (FIGURE 2), and dynamic changes with fundal or suprapubic pressure.3,10,19 Consistency of measurement—with careful attention to both intraoperator and interoperator variability—is vital when using these findings for clinical decision-making.1,10
Focus screening on women at risk. The sensitivity and predictive value of cervical length improve when screening is limited to populations at greatest risk: women with a history of preterm delivery, cervical surgery, or previous midtrimester loss or cervical incompetence. Conversely, positive and negative predictive values are low when measurements are performed in a low-risk population.17
Still, determining which gravidas are at highest risk of preterm delivery is a challenge; a careful obstetric history is the most important tool (TABLE).4,15,16,24 In addition to the factors listed in the table, any history of successful cerclage placement is also significant.25 An extensive history also may offer clues as to what may have caused a shortened cervix in a previous pregnancy. Acquiring old medical records may further clarify the situation.
Unfortunately, the aforementioned trials, while documenting the predictive value of cervical measurements, reveal nothing about specific clinical interventions such as cerclage placement. Rather, they indicate the need for well-designed randomized trials.
The advisability of therapeutic cerclage varies from case to case, but prophylactic cerclage, in general, should be offered to women with a classic history of cervical incompetence or prior cerclage with a successful outcome.
FIGURE 2 Transvaginal ultrasound of shortened cervix with funneling
The cervical length is 1.11 cm with a “U”-shaped funnel measuring 2.51 cm by 1.47 cm.TABLE
Preterm delivery: Factors indicating high risk
|
Management options
Once a short cervix has been diagnosed, the obstetrician faces a morass of conflicting data on how to proceed. After reviewing the patient’s history to identify any obvious risk factors, attempt to rule out uterine contractions, ruptured membranes, and clinical or subclinical infection. Once these and any other causes are excluded, the primary management options are bed rest and placement of cervical cerclage. Unfortunately, this is an issue of great controversy, with no definitive evidence on which strategy is best.
Based on the data available, we suggest the following cervical surveillance (FIGURE 1):
- Perform initial cervical measurements in high-risk patients at 14 to 24 weeks’ gestation. Women with cervical lengths exceeding 26 mm should be reassessed in 2 to 3 weeks.
- Women with a cervical length between 21 and 25 mm should be placed on reduced physical activity with remeasurement in 2 weeks.
- Patients with a length between 16 and 20 mm should be placed on strict bed rest with remeasurement in 1 week.
- Only women with a cervical length of 15 mm or less should be considered for therapeutic cerclage.9,24
No evidence supports measuring cervical length or placing a cerclage in the low-risk patient.
Cerclage versus bed rest: Ambiguous evidence
Several nonrandomized retrospective observational trials of cerclage placement versus bed rest in the general obstetric population reported conflicting results. For example, Heath et al26 studied a low-risk obstetric population in Great Britain that underwent transvaginal measurements of cervical length. Women with lengths of 15 mm or less were managed expectantly (n=21) or had a Shirodkar cerclage placed (n=22). Only 5% in the cerclage group delivered prior to 32 weeks’ gestation, compared with 52% in the expectantly managed group. In a general obstetric population, Hibbard et al27 also found an increase in the duration of pregnancy (2 weeks) among women who underwent cerclage placement for a cervical length less than 26 mm (n=43), compared with those who had no cerclage placed (n=42).
In a retrospective review of an obstetric population with cervical lengths of 15 mm or less, Hassan et al28 compared women receiving cerclage (n=25) with those who did not (n=45). In contrast to the 2 trials just mentioned, cervical cerclage failed to decrease the rate of spontaneous preterm delivery. Moreover, patients with a cerclage had an increased incidence of premature rupture of membranes.
In a nonrandomized prospective observational trial of women at high risk for preterm delivery, Berghella et al15 reported that those undergoing cerclage (n=39) for cervical length less than 25 mm and/or for 25% funneling fared no better than women who did not undergo cerclage placement (n=24).
Randomized prospective controlled trials. Only 2 such trials have been reported to date, and their design and patient populations differ.
Althusius et al24 studied a high-risk population in the Cervical Incompetence Prevention Randomized Cervical Trial (CIPRACT), which involved primary randomization to determine the effects of prophylactic cerclage, and secondary randomization to determine the effects of therapeutic cerclage. Women with a history of preterm delivery before 34 weeks who had a “classic” history of cervical incompetence were allocated to prophylactic cerclage or no cerclage in the late first or early second trimester. Thus, these gravidas already met the diagnosis of cervical incompetence. Both groups were then followed with serial measurements of cervical length. A second randomization to therapeutic cerclage or bed rest occurred if a cervical length less than 25 mm was found before 27 weeks’ gestation. This trial showed a statistically significant greater mean gestational age and improved pregnancy outcomes among women in both groups who received a cerclage, suggesting that therapeutic cerclage is a viable management option in at-risk women with cervical shortening. Moreover, the study design of primary and secondary randomization offers a sound strategy for management.
To address the value of therapeutic cerclage, Rust et al5-7 designed a prospective, randomized trial of both high-risk and low-risk women with second-trimester shortened cervical measurements with funneling or a total cervical length less than 25 mm. These women were allocated to therapeutic cerclage or bed rest. Prior to randomization, all women underwent cervical and urinary cultures and amniotic fluid analysis to exclude underlying intra-amniotic infection. Both groups then were followed with weekly transvaginal cervical measurements. A rescue cerclage was placed if prolapsing membranes occurred in either group.
Although decreasing cervical length was associated with poorer pregnancy outcomes, cervical cerclage did not result in a statistically significant greater mean gestational age or improved perinatal outcome, contradicting the results reported in the CIPRACT trial. Furthermore, patients who needed rescue cerclage had the worst outcomes. One explanation may be that the CIPRACT trial included only patients with a history of cervical incompetence, whereas Rust et al included low-risk and high-risk women unexpectedly noted to have a shortened cervix—patients more akin to the woman described at the beginning of this article, and a more likely scenario for most obstetricians.
Until better evidence is available, the limited number of randomized, controlled trials addressing the issue of shortened cervical length should guide management. Using this information, several institutions have initiated “cervical surveillance” programs in which clinicians perform serial ultrasounds to assess changes in cervical length over time. The most recent results from the ongoing randomized trial by Rust et al7—the best evidence to date in both low-risk and high-risk women—offer the promise of answers to this issue.
The authors report no financial relationship with any companies whose products are mentioned in this article.
- An extensive history is essential to identify the gravida at risk for a shortened cervical length.
- Transvaginal measurement of cervical lengths less than 26 mm has a high predictive value for preterm delivery.
- Prophylactic cerclage should be offered to patients with a classic history of cervical incompetence.
- The benefits of therapeutic cerclage for a shortened cervix remain uncertain, especially in women deemed to have a low risk of preterm delivery.
You are in your busy office, running behind schedule, when you receive a frantic notice from the ultrasound department that your patient—a primigravida scheduled for a routine anatomy survey at 21 weeks’ gestation—has a cervical length of 19 mm with funneling. What are your management options if the patient reports no contractions or changes in vaginal discharge?
With today’s emphasis on evidence-based medicine, it often is difficult to decide on an appropriate course of action, especially when conflicting reports abound. This article reviews the best studies available and presents a practical algorithm (FIGURE 1) to guide management of this difficult dilemma.
FIGURE 1 Management strategy for women with risk factors for cervical incompetence, preterm delivery
Predicting the need for cerclage
Despite numerous explorations of its pathophysiology, no irrefutable data explain what triggers the cascade of events leading to preterm birth, which remains a leading cause of morbidity and mortality. Cervical incompetence has been studied extensively as a possible cause, often without conclusive results.
Traditionally, cervical incompetence is defined as dilatation in the absence of contractions, usually presenting in the second trimester.1 Possible causes include prior obstetric or gynecologic injury, increased uterine volume (ie, multiple gestation, polyhydramnios), biological variation, and—currently under investigation—response to inflammatory mediators.2
In gravidas deemed to have biological or structural cervical incompetence, prophylactic cerclage is often placed at 12 to 14 weeks’ gestation. Alternatively, a therapeutic or “rescue” cerclage sometimes is placed at 20 weeks or more when evidence of cervical shortening or funneling is noted incidentally on ultrasound examination. At times, therapeutic cerclage becomes an emergency if prolapsing membranes are found.
With improvements in ultrasound imaging, transvaginal measurement of cervical length has become useful for guiding decisions on the need for cerclage.3,4 Unfortunately, current studies report conflicting data on the outcomes of pregnancies managed with cerclage placement based on ultrasound imaging.5-7
Ultrasound evaluation: Cervical length and other variables
In unselected general obstetric populations, preterm birth is associated with decreasing cervical length not only at 24 and 28 weeks’ gestation, but as early as 16 to 22 weeks’ gestation.8-14 Decreasing cervical length also predicts preterm birth in women at risk for early delivery.15,16 As a result, sonographic visualization of cervical length has evolved into a common practice to help predict early delivery.
An extensive history may offer clues as to what may have caused a shortened cervix in a previous pregnancy.
Iams et al17 compared cervical length with fetal fibronectin and noted that cervical length is more sensitive (39% versus 23%) but has a lower positive predictive value (PPV) (14% versus 20%). In combination, the modalities improved PPV to 50%. However, a separate study by Heath et al18 suggested that women with a cervical length of 15 mm or less had a relative risk of preterm birth 6 times greater than those with positive fetal fibronectin alone.
As sonographic technology has advanced, cervical characteristics have been assessed in a variety of ways. Besides measuring cervical length, experts also look for funneling, dilatation, prolapsing membranes, and dynamic changes elicited with transfundal or suprapubic pressure.4,19,20
Although cervical length can be measured transabdominally and transperineally, transvaginal assessment is most accurate. Transvaginal measurements also are more predictive and reproducible than traditional digital cervical examinations.16,21,22
Basic parameters. Standard cervical measurements use the “white stripe” of the internal cervical os as an anatomic landmark for proper caliper placement (FIGURE 2). As for dimensions of the nonlaboring cervix, Anderson23 found an average length of 45±7 mm at 14 to 30 weeks, and Iams et al10 found a mean cervical length of 35±8 mm at 24 weeks’ gestation after studying more than 2,900 gravidas. In another investigation, Hibbard and colleagues found a mean cervical length of 38.5±8 mm at 20 weeks’ gestation.12
Cervical length and diameter should remain constant as gestation progresses in both primiparous and multiparous women.22
Defining the short cervix. In a multicenter clinical trial, Iams et al10 measured the length of the cervix at 24 and 28 weeks in an unselected gravid population and determined that a length less than 26 mm at 24 weeks increases the relative risk for preterm delivery by a factor of 6.19, with a sensitivity of 37% for delivery before 35 weeks and a PPV of 18%—thus establishing the definition of a short cervix.
They also noted that the likelihood of spontaneous preterm delivery increased exponentially the shorter the cervical measurement. Hibbard et al12 attained similar findings with cervical measurements obtained at 16 to 22 weeks’ gestation in an unselected population, verifying the value of cervical measurements at an earlier gestational age in predicting preterm delivery.
In a retrospective cohort study, Hassan et al9 reviewed cervical measurements in an unselected population between 14 and 24 weeks, and found that close to 50% of gravidas with a cervical length of 15 mm or less delivered earlier than 32 weeks’ gestation. They therefore suggest that cervical length be measured early in the second trimester to obtain more accurate assessment of underlying risk for cervical incompetence.9
Interpreting cervical characteristics. As mentioned, other cervical qualities are useful to assess, such as funneling (and measurement of the residual cervix if funneling is present), v-shaped lower uterine segment (FIGURE 2), and dynamic changes with fundal or suprapubic pressure.3,10,19 Consistency of measurement—with careful attention to both intraoperator and interoperator variability—is vital when using these findings for clinical decision-making.1,10
Focus screening on women at risk. The sensitivity and predictive value of cervical length improve when screening is limited to populations at greatest risk: women with a history of preterm delivery, cervical surgery, or previous midtrimester loss or cervical incompetence. Conversely, positive and negative predictive values are low when measurements are performed in a low-risk population.17
Still, determining which gravidas are at highest risk of preterm delivery is a challenge; a careful obstetric history is the most important tool (TABLE).4,15,16,24 In addition to the factors listed in the table, any history of successful cerclage placement is also significant.25 An extensive history also may offer clues as to what may have caused a shortened cervix in a previous pregnancy. Acquiring old medical records may further clarify the situation.
Unfortunately, the aforementioned trials, while documenting the predictive value of cervical measurements, reveal nothing about specific clinical interventions such as cerclage placement. Rather, they indicate the need for well-designed randomized trials.
The advisability of therapeutic cerclage varies from case to case, but prophylactic cerclage, in general, should be offered to women with a classic history of cervical incompetence or prior cerclage with a successful outcome.
FIGURE 2 Transvaginal ultrasound of shortened cervix with funneling
The cervical length is 1.11 cm with a “U”-shaped funnel measuring 2.51 cm by 1.47 cm.TABLE
Preterm delivery: Factors indicating high risk
|
Management options
Once a short cervix has been diagnosed, the obstetrician faces a morass of conflicting data on how to proceed. After reviewing the patient’s history to identify any obvious risk factors, attempt to rule out uterine contractions, ruptured membranes, and clinical or subclinical infection. Once these and any other causes are excluded, the primary management options are bed rest and placement of cervical cerclage. Unfortunately, this is an issue of great controversy, with no definitive evidence on which strategy is best.
Based on the data available, we suggest the following cervical surveillance (FIGURE 1):
- Perform initial cervical measurements in high-risk patients at 14 to 24 weeks’ gestation. Women with cervical lengths exceeding 26 mm should be reassessed in 2 to 3 weeks.
- Women with a cervical length between 21 and 25 mm should be placed on reduced physical activity with remeasurement in 2 weeks.
- Patients with a length between 16 and 20 mm should be placed on strict bed rest with remeasurement in 1 week.
- Only women with a cervical length of 15 mm or less should be considered for therapeutic cerclage.9,24
No evidence supports measuring cervical length or placing a cerclage in the low-risk patient.
Cerclage versus bed rest: Ambiguous evidence
Several nonrandomized retrospective observational trials of cerclage placement versus bed rest in the general obstetric population reported conflicting results. For example, Heath et al26 studied a low-risk obstetric population in Great Britain that underwent transvaginal measurements of cervical length. Women with lengths of 15 mm or less were managed expectantly (n=21) or had a Shirodkar cerclage placed (n=22). Only 5% in the cerclage group delivered prior to 32 weeks’ gestation, compared with 52% in the expectantly managed group. In a general obstetric population, Hibbard et al27 also found an increase in the duration of pregnancy (2 weeks) among women who underwent cerclage placement for a cervical length less than 26 mm (n=43), compared with those who had no cerclage placed (n=42).
In a retrospective review of an obstetric population with cervical lengths of 15 mm or less, Hassan et al28 compared women receiving cerclage (n=25) with those who did not (n=45). In contrast to the 2 trials just mentioned, cervical cerclage failed to decrease the rate of spontaneous preterm delivery. Moreover, patients with a cerclage had an increased incidence of premature rupture of membranes.
In a nonrandomized prospective observational trial of women at high risk for preterm delivery, Berghella et al15 reported that those undergoing cerclage (n=39) for cervical length less than 25 mm and/or for 25% funneling fared no better than women who did not undergo cerclage placement (n=24).
Randomized prospective controlled trials. Only 2 such trials have been reported to date, and their design and patient populations differ.
Althusius et al24 studied a high-risk population in the Cervical Incompetence Prevention Randomized Cervical Trial (CIPRACT), which involved primary randomization to determine the effects of prophylactic cerclage, and secondary randomization to determine the effects of therapeutic cerclage. Women with a history of preterm delivery before 34 weeks who had a “classic” history of cervical incompetence were allocated to prophylactic cerclage or no cerclage in the late first or early second trimester. Thus, these gravidas already met the diagnosis of cervical incompetence. Both groups were then followed with serial measurements of cervical length. A second randomization to therapeutic cerclage or bed rest occurred if a cervical length less than 25 mm was found before 27 weeks’ gestation. This trial showed a statistically significant greater mean gestational age and improved pregnancy outcomes among women in both groups who received a cerclage, suggesting that therapeutic cerclage is a viable management option in at-risk women with cervical shortening. Moreover, the study design of primary and secondary randomization offers a sound strategy for management.
To address the value of therapeutic cerclage, Rust et al5-7 designed a prospective, randomized trial of both high-risk and low-risk women with second-trimester shortened cervical measurements with funneling or a total cervical length less than 25 mm. These women were allocated to therapeutic cerclage or bed rest. Prior to randomization, all women underwent cervical and urinary cultures and amniotic fluid analysis to exclude underlying intra-amniotic infection. Both groups then were followed with weekly transvaginal cervical measurements. A rescue cerclage was placed if prolapsing membranes occurred in either group.
Although decreasing cervical length was associated with poorer pregnancy outcomes, cervical cerclage did not result in a statistically significant greater mean gestational age or improved perinatal outcome, contradicting the results reported in the CIPRACT trial. Furthermore, patients who needed rescue cerclage had the worst outcomes. One explanation may be that the CIPRACT trial included only patients with a history of cervical incompetence, whereas Rust et al included low-risk and high-risk women unexpectedly noted to have a shortened cervix—patients more akin to the woman described at the beginning of this article, and a more likely scenario for most obstetricians.
Until better evidence is available, the limited number of randomized, controlled trials addressing the issue of shortened cervical length should guide management. Using this information, several institutions have initiated “cervical surveillance” programs in which clinicians perform serial ultrasounds to assess changes in cervical length over time. The most recent results from the ongoing randomized trial by Rust et al7—the best evidence to date in both low-risk and high-risk women—offer the promise of answers to this issue.
The authors report no financial relationship with any companies whose products are mentioned in this article.
1. Iams JD. Cervical incompetence. In: Creasy RK, Resnik R, eds. Maternal-Fetal Medicine. 4th ed. Philadelphia, Pa: WB Saunders; 1999;445-464.
2. Guzman ER. Cervical length and spontaneous prematurity: laying the foundation for future interventional randomized trials for the short cervix. Ultrasound Obstet Gynecol. 2001;18:195-199.
3. Guzman ER, Forster JK, Vintzileos AM, et al. Pregnancy outcomes in women treated with elective versus ultrasound-indicated cervical cerclage. Ultrasound Obstet Gynecol. 1998;12:323-327.
4. Berghella V, Hass S, Chervoneva I, Hyslop T. Patients with prior second-trimester loss: prophylactic cerclage or serial transvaginal sonograms? Am J Obstet Gynecol. 2002;187:747-751.
5. Rust OA, Atlas RO, Jones KJ, Benham BN, Balducci J. A randomized trial of cerclage versus no cerclage among patients with ultrasonographically detected secondtrimester preterm dilatation of the internal os. Am J Obstet Gynecol. 2000;183:830-835.
6. Rust OA, Atlas RO, Reed J, van Gaalen J, Balducci J. Revisiting the short cervix detected by transvaginal ultrasound in the second trimester: why cerclage therapy may not help. Am J Obstet Gynecol. 2001;185:1098-1105.
7. Rust OA, Atlas RO, Fischl S, Depuy A, Kimmel S, Hess LW. Does cerclage therapy improve perinatal outcome in patients with a history of previous preterm birth and cervical changes on 2nd trimester transvaginal ultrasound? Am J Obstet Gynecol. 2002;187(suppl):S58.-
8. Iams JD, Johnson FF, Sonek K, et al. Cervical competence as a continuum: a study of ultrasonographic cervical length and obstetric performance. Am J Obstet Gynecol. 1995;174:1097-1106.
9. Hassan SS, Romero R, Berry SM, et al. Patients with an ultrasonographic cervical length ≤15 mm have nearly a 50% risk of early spontaneous preterm delivery. Am J Obstet Gynecol. 2000;182:1458-1467.
10. Iams JD, Goldenberg RL, Meis PJ, et al. The length of the cervix and the risk of spontaneous premature delivery. N Engl J Med. 1996;334:567-572.
11. Taipale P, Hilesmaa V. Sonographic measurement of uterine cervix at 18-22 weeks’ gestation and the risk of preterm delivery. Obstet Gynecol. 1998;92:902-907.
12. Hibbard JU, Tart M, Moawad AH. Cervical length at 16-22 weeks’ gestation and risk for preterm delivery. Obstet Gynecol. 2000;96:972-978.
13. Anderson HF, Nugent CE, Wanty SD, Hayashi RH. Prediction of risk for preterm delivery by ultrasonographic measurement of cervical length. Am J Obstet Gynecol. 1990;163:859-867.
14. Heath VC, Southall TR, Souka AP, Elisseou A, Nicholaides KH. Cervical length at 23 weeks of gestation: prediction of spontaneous preterm delivery. Ultrasound Obstet Gynecol. 1998;12(5):312-317.
15. Berghella V, Daly SF, Tolosa JE, et al. Prediction of preterm delivery with transvaginal ultrasonography of the cervix in patients with high-risk pregnancies: does cerclage prevent prematurity? Am J Obstet Gynecol. 1999;181:809-815.
16. Berghella V, Tolasa JE, Kuhlman K. Cervical ultrasound compared with manual examination as a predictor of preterm delivery. Am J Obstet Gynecol. 1997;177:723-730.
17. Iams JD, Goldenberg RL, Mercer BM, et al. The preterm prediction study: can low-risk women destined for spontaneous preterm birth be identified? Am J Obstet Gynecol. 2001;184:652-655.
18. Heath VC, Daskalakis G, Zagaliki A, Carvalho M, Nicolaides KH. Cervicovaginal fibronectin and cervical length at 23 weeks of gestation:relative risk of early preterm delivery. BJOG. 2000;107:1276-1281.
19. Guzman ER, Pisatowski DM, Vintzileos AM, et al. A comparison of ultrasonographically detected cervical changes in response to transfundal pressure, coughing, and standing in predicting cervical incompetence. Am J Obstet Gynecol. 1997;172:660-665.
20. Sonek J, Blumefeld M, Foley M, Johnson F, Iams J. Cervical length may change during ultrasonographic examination. Am J Obstet Gynecol. 1990;162:1355-1357.
21. Sonek JD, Iams JD, Blumefeld M, Johnson F, Landon M, Gabbe S. Measurement of cervical length in pregnancy: comparison between vaginal ultrasonography and digital examination. Obstet Gynecol. 1990;76:172-175.
22. Cook CM, Ellwood DA. A longitudinal study of the cervix in pregnancy using transvaginal ultrasound. BJOG. 1996;103:16-18.
23. Anderson HF. Transvaginal and transabdominal ultrasonography of the uterine cervix during pregnancy. J Clin Ultrasound. 1991;19:77-83.
24. Althuisius SM, Dekker GA, Hummel P, Bekedam D, van Geijn HP. Final results of the Cervical Incompetence Prevention Randomized Cervical Trial (CIPRACT): therapeutic cerclage with bed rest versus bed rest alone. Am J Obstet Gynecol. 2001;185:1106-1112.
25. Colombo DF, Iams JD. Cervical length and preterm labor. Clin Obstet Gynecol. 2000;43:735-745.
26. Heath VC, Souka AP, Erasmus I, Gibb DM, Nicolaides KH. Cervical length at 23 weeks’ gestation: the value of Shirodkar suture for the short cervix. Ultrasound Obstet Gynecol. 1998;12:318-322.
27. Hibbard JU, Snow J, Moawad AH. Short cervical length by ultrasound and cerclage. J Perinatol. 2000;20:161-165.
28. Hassan SS, Romero R, Maymon E, et al. Does cervical cerclage prevent preterm delivery in patients with short cervix? Am J Obstet Gynecol. 2001;184:1325-1331.
1. Iams JD. Cervical incompetence. In: Creasy RK, Resnik R, eds. Maternal-Fetal Medicine. 4th ed. Philadelphia, Pa: WB Saunders; 1999;445-464.
2. Guzman ER. Cervical length and spontaneous prematurity: laying the foundation for future interventional randomized trials for the short cervix. Ultrasound Obstet Gynecol. 2001;18:195-199.
3. Guzman ER, Forster JK, Vintzileos AM, et al. Pregnancy outcomes in women treated with elective versus ultrasound-indicated cervical cerclage. Ultrasound Obstet Gynecol. 1998;12:323-327.
4. Berghella V, Hass S, Chervoneva I, Hyslop T. Patients with prior second-trimester loss: prophylactic cerclage or serial transvaginal sonograms? Am J Obstet Gynecol. 2002;187:747-751.
5. Rust OA, Atlas RO, Jones KJ, Benham BN, Balducci J. A randomized trial of cerclage versus no cerclage among patients with ultrasonographically detected secondtrimester preterm dilatation of the internal os. Am J Obstet Gynecol. 2000;183:830-835.
6. Rust OA, Atlas RO, Reed J, van Gaalen J, Balducci J. Revisiting the short cervix detected by transvaginal ultrasound in the second trimester: why cerclage therapy may not help. Am J Obstet Gynecol. 2001;185:1098-1105.
7. Rust OA, Atlas RO, Fischl S, Depuy A, Kimmel S, Hess LW. Does cerclage therapy improve perinatal outcome in patients with a history of previous preterm birth and cervical changes on 2nd trimester transvaginal ultrasound? Am J Obstet Gynecol. 2002;187(suppl):S58.-
8. Iams JD, Johnson FF, Sonek K, et al. Cervical competence as a continuum: a study of ultrasonographic cervical length and obstetric performance. Am J Obstet Gynecol. 1995;174:1097-1106.
9. Hassan SS, Romero R, Berry SM, et al. Patients with an ultrasonographic cervical length ≤15 mm have nearly a 50% risk of early spontaneous preterm delivery. Am J Obstet Gynecol. 2000;182:1458-1467.
10. Iams JD, Goldenberg RL, Meis PJ, et al. The length of the cervix and the risk of spontaneous premature delivery. N Engl J Med. 1996;334:567-572.
11. Taipale P, Hilesmaa V. Sonographic measurement of uterine cervix at 18-22 weeks’ gestation and the risk of preterm delivery. Obstet Gynecol. 1998;92:902-907.
12. Hibbard JU, Tart M, Moawad AH. Cervical length at 16-22 weeks’ gestation and risk for preterm delivery. Obstet Gynecol. 2000;96:972-978.
13. Anderson HF, Nugent CE, Wanty SD, Hayashi RH. Prediction of risk for preterm delivery by ultrasonographic measurement of cervical length. Am J Obstet Gynecol. 1990;163:859-867.
14. Heath VC, Southall TR, Souka AP, Elisseou A, Nicholaides KH. Cervical length at 23 weeks of gestation: prediction of spontaneous preterm delivery. Ultrasound Obstet Gynecol. 1998;12(5):312-317.
15. Berghella V, Daly SF, Tolosa JE, et al. Prediction of preterm delivery with transvaginal ultrasonography of the cervix in patients with high-risk pregnancies: does cerclage prevent prematurity? Am J Obstet Gynecol. 1999;181:809-815.
16. Berghella V, Tolasa JE, Kuhlman K. Cervical ultrasound compared with manual examination as a predictor of preterm delivery. Am J Obstet Gynecol. 1997;177:723-730.
17. Iams JD, Goldenberg RL, Mercer BM, et al. The preterm prediction study: can low-risk women destined for spontaneous preterm birth be identified? Am J Obstet Gynecol. 2001;184:652-655.
18. Heath VC, Daskalakis G, Zagaliki A, Carvalho M, Nicolaides KH. Cervicovaginal fibronectin and cervical length at 23 weeks of gestation:relative risk of early preterm delivery. BJOG. 2000;107:1276-1281.
19. Guzman ER, Pisatowski DM, Vintzileos AM, et al. A comparison of ultrasonographically detected cervical changes in response to transfundal pressure, coughing, and standing in predicting cervical incompetence. Am J Obstet Gynecol. 1997;172:660-665.
20. Sonek J, Blumefeld M, Foley M, Johnson F, Iams J. Cervical length may change during ultrasonographic examination. Am J Obstet Gynecol. 1990;162:1355-1357.
21. Sonek JD, Iams JD, Blumefeld M, Johnson F, Landon M, Gabbe S. Measurement of cervical length in pregnancy: comparison between vaginal ultrasonography and digital examination. Obstet Gynecol. 1990;76:172-175.
22. Cook CM, Ellwood DA. A longitudinal study of the cervix in pregnancy using transvaginal ultrasound. BJOG. 1996;103:16-18.
23. Anderson HF. Transvaginal and transabdominal ultrasonography of the uterine cervix during pregnancy. J Clin Ultrasound. 1991;19:77-83.
24. Althuisius SM, Dekker GA, Hummel P, Bekedam D, van Geijn HP. Final results of the Cervical Incompetence Prevention Randomized Cervical Trial (CIPRACT): therapeutic cerclage with bed rest versus bed rest alone. Am J Obstet Gynecol. 2001;185:1106-1112.
25. Colombo DF, Iams JD. Cervical length and preterm labor. Clin Obstet Gynecol. 2000;43:735-745.
26. Heath VC, Souka AP, Erasmus I, Gibb DM, Nicolaides KH. Cervical length at 23 weeks’ gestation: the value of Shirodkar suture for the short cervix. Ultrasound Obstet Gynecol. 1998;12:318-322.
27. Hibbard JU, Snow J, Moawad AH. Short cervical length by ultrasound and cerclage. J Perinatol. 2000;20:161-165.
28. Hassan SS, Romero R, Maymon E, et al. Does cervical cerclage prevent preterm delivery in patients with short cervix? Am J Obstet Gynecol. 2001;184:1325-1331.