User login
Trichotillomania: A heads-up on severe cases
History: Bald at age 9
Ms. D, age 41, began compulsively pulling out and eating her hair at age 8. When she didn’t get her way at home or was nervous about school, she would sit for hours, pulling and eating a strand or two at a time, ultimately ingesting a clump of hair.
By age 9, Ms. D was bald. In grade school, she often wore hats and scarves to class to avoid teasing from other children about her baldness. In high school, she kept to herself and frequently wore wigs.
Ms. D stops pulling for brief periods and her hair grows out, but she invariably resumes pulling when psychosocial stressors mount. Many of life’s normal anxieties—job interviews, work-related stress, social rejection—trigger episodes.
When she is bald, Ms. D pulls and eats hair off her wig. Over the years, she has spent thousands of dollars on custom-made wigs that mask her baldness while feeding her habit.
Ms. D’s episodes are increasingly interfering with her life. She has been steadily employed as an office assistant, but does not socialize with coworkers. She has not dated in years, and during an exacerbation leaves home only to go to work. She also pulls her eyelashes and eyebrows and picks her nails and cuticles.
Ms. D first presented in 1994 after seeing a television segment I did on trichotillomania. At intake, she was wearing a wig and exhibited anxious mood. She also has Crohn’s disease; a gastroenterologist monitors her closely.
Ms. D reports compulsive counting and checking but denies other similar behaviors. No immediate family members have exhibited obsessive-compulsive or hair-pulling behaviors. Her father abused alcohol and a sister has a stuttering problem, although Ms. D denies that these have affected her psychologically.
Ms. D’s hair-pulling behavior suggests:
- a pica disorder
- an impulse control disorder
- or an obsessive-compulsive disorder?
- Recurrent pulling out of one’s own hair, resulting in noticeable hair loss.
- Increasing tension immediately before pulling out the hair or when attempting to resist the behavior.
- Pleasure, gratification, or relief while pulling out the hair.
- The disturbance is not better explained as another mental disorder and is not caused by a dermatological or other general medical condition.
- The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders, 4th ed., text revision. Copyright 2000. American Psychiatric Association.
Dr. Lundt’s observations
Trichotillomania, defined as compulsive pulling of hair, usually begins in childhood or adolescence. Scalp hair is most commonly pulled, but some patients also pull their eyelashes, pubic hair, and other body hair. Some, especially children, have reportedly pulled their pets’ hair.
Mansueto et al estimate that trichotillomania afflicts approximately 1.5% of males and 3.5% of females.1 These estimates, however, do not include persons with the disorder who are too embarrassed to seek treatment.
DSM-IV-TR classifies trichotillomania as an impulse control disorder (Box). Although comorbid anxiety and depressive disorders are common, Ms. D did not meet criteria for any other psychiatric disorder.
Trichotillomania often is episodic. Months or years of abstinence is common after periods of exacerbation, usually caused by stress (Figure).
Many clinicians mistakenly consider trichotillomania a benign disorder with few consequences beyond alopecia.2 Some patients, however, progress into trichophagia—ingestion of pulled hair. Trichophagia is a form of pica disorder, typically defined as persistent eating of non-nutritive substances. Patients often harbor tremendous shame over their hair-eating behavior and resist psychiatric or medical treatment.2
The undigested hair can form sometimes massive clumps called trichobezoars, which are most common among children and the developmentally disabled.4 Persons with trichophagia face a 37.5% risk of forming a trichobezoar.5 The mass can cause abdominal pain, nausea, vomiting, and weight loss; complications include GI obstruction, ulceration, perforation, and peritonitis.6 An untreated trichobezoar can be fatal,7 although such deaths are rare among patients being treated for trichotillomania.
Patients with trichotillomania often respond to medications used to treat obsessive-compulsive disorder, such as clomipramine. Some clinicians believe this agent is more effective than selective serotonin reuptake inhibitors (SSRIs) but more difficult to tolerate. For Ms. D, I started with both.
Treatment: ‘I Don’t need medication’
Initial treatments—including fluoxetine, 20 mg/d for 6 months; hypnotherapy; and clomipramine, 25 mg/d—were unsuccessful. Ms. D was only marginally compliant, believing that she did not need medication.
I referred Ms. D to an out-of-state residential behavioral program specializing in trichotillomania, but she refused to go even as her hair-pulling intensified. Clomipramine was gradually increased to 75 mg nightly, briefly decreasing her pulling, then to 100 mg nightly when symptoms re-emerged. Clomipramine blood levels were monitored with each dosage change to guard against CNS and cardiac toxicity and other side effects (GI complaints, dizziness, cardiac arrhythmias, somnolence).
After watching for seasonal patterns, I found that Ms. D’s hair-pulling worsened during the winter, although no seasonal change in mood was detected. Phototherapy produced initial success, but Ms. D continued to pull her eyelashes.
Eight weeks later, however, Ms. D’s symptoms escalated. Clomipramine was increased to 150 mg nightly, resulting in blood levels of 99 ng/mL for clomipramine and 204 ng/mL for the metabolite N-desmethylclomipramine—both within the therapeutic range. As she continued pulling, I added buspirone, 10 mg/d.
At this point, would you:
- continue clomipramine and increase the dosage?
- discontinue clomipramine and start another psychotropic?
- or maintain clomipramine at the same dosage and add another psychotropic?
Dr. Lundt’s observations
Drug treatment of trichotillomania has not been studied extensively or long-term, and no consensus exists. Psychoanalysis, cognitive-behavioral therapy (CBT), and hypnotherapy are usually administered with psychotropics.8 Patients often respond to treatment at first, then reach a plateau and resume pulling their hair.9
Numerous psychotropics are used off-label to treat trichotillomania. Several agents have been shown in clinical trials and case reports to reduce hair pulling/eating behaviors (Table), but these findings are limited by small sample size, lack of control groups, and lack of a standard symptom rating scale.
Figure Trichotillomania: Excessive grooming, habit, or vicious circle?
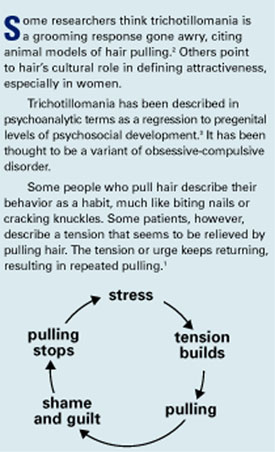
Most clinicians begin with SSRIs because they are generally well tolerated, even at high dosages. Monotherapy often is not adequate for trichotillomania, however. Medication augmentation is common, although little empiric data support this practice.
When clomipramine did not work initally, I explored serotonergic combination strategies.
Table
Medications shown to benefit patients with trichotillomania
| Drug | Evidence | Dosage range (mg/d) | Potential side effects |
|---|---|---|---|
| First-line | |||
| Tricyclic | |||
| Clomipramine | Swedo et al10 | 50 to 300 | Sedation, weight gain, cardiac arrythmias |
| SSRIs | |||
| Fluoxetine | van Minnen et al11 | 20 to 60 | GI symptoms, insomnia |
| Fluvoxamine | Gabriel12 | 50 to 250 | Sexual dysfunction, weight gain |
| Paroxetine | Ravindran et al13 | 20 to 60 | Sexual dysfunction, weight gain |
| Sertraline | Bradford and Gratzer14 | 50 to 200 | Sexual dysfunction, GI symptoms, insomnia |
| Second-line | |||
| Antipsychotics | |||
| Haloperidol | Van Ameringen et al15 | 0.25 to 2 | Sedation, EPS |
| Olanzapine | Gupta and Gupta16 | 2.5 to 10 | Sedation, weight gain |
| Pimozide | Stein and Hollander17 | 25 to 200 | Restlessness, EPS |
| Quetiapine | Khouzam et al8 | 25 to 200 | Sedation |
| Risperidone | Gabriel12 Senturk and Tanriverdi18 | 0.5 to 4.0 | Sedation, hyperprolactinemia |
| Mood stabilizer | |||
| Lithium | Christenson et al19 | 900 to 1,500 | Increased thirst, weight gain, tremor |
| EPS: extrapyramidal symptoms | |||
Further treatment: Relapse, resection
Ms. D was lost to follow-up for 1 year. She returned in 1996, just after undergoing a laparotomy for removal of a trichobezoar large enough to fill two 2-inch-by-6-inch bags. She also had been treated for pneumonia and a pulmonary embolus.
Riddled with shame and embarrassment, Ms. D had stopped pulling for 10 months, during which time she was off medication. Her pulling behaviors re-emerged, however, and clomipramine was restarted and titrated to 250 mg nightly.
One year later, a second trichobezoar was resected. Her clomipramine/N-desmethylclomipramine level reached 1,535 ng/mL, although an ECG reading was normal. Subsequent clomipramine/N-desmethylclomipramine blood levels were within the therapeutic range. Fluvoxamine, 25 mg/d titrated across 6 weeks to 150 mg/d, was added.
Again, Ms. D stopped taking her medications and was lost to follow-up. Her gastroenterologist began managing her care and started sertraline, dosage unknown, to address her depressed mood. A third trichobezoar was removed.
When Ms. D returned to my practice, I resumed CBT and increased sertraline over 1 month from 100 to 300 mg/d. Adding olanzapine, 2.5 mg/d, diminished her anxiety and markedly decreased her hair pulling.
Months later, her hair-pulling/eating behaviors again intensified, resulting in a small-bowel obstruction and a fourth trichobezoar removal. Olanzapine was increased to 5 mg nightly without significant benefit and with sedating effects.
Clomipramine, 125 mg/d, was reintroduced and her symptoms improved dramatically. On a regimen of sertraline, clomipramine and olanzapine, Ms. D remained stable for 2 years.
Last year, however, a fifth trichobezoar measuring 20 x 15 cm was removed. Subsequent trials of methylphenidate, titrated to 72 mg every morning, and tramadol, titrated to 100 mg/d, were unsuccessful.
After 10 years of medication and psychotherapy with three different providers, Ms. D’s hair-pulling/eating behaviors persist. She is taking ziprasidone, 120 mg bid, and naltrexone, 100 mg bid, to help her impulse control, as well as sertraline, 300 mg/d, and clomipramine, 125 mg/d. Another trichobezoar removal—her sixth in 8 years—is scheduled.
What strategies exist for minimizing Ms. D’s hair-pulling behavior and keeping her in therapy?
Dr. Lundt’s observations
Trichotillomania’s waxing and waning course—and its destructive effects on a patient’s self-esteem—pose a clinical challenge. The disorder’s severity can range from cosmetically annoying to life-threatening, as in Ms. D’s case. Patients embarrassed by their behavior often prematurely leave treatment, desperate to cut off all social contact—including medical appointments.
It is crucial to maintain a nonjudgmental, inviting demeanor to alleviate the patient’s fears and facilitate a return to treatment. Support groups, especially online, can help decrease patients’ isolation and provide a reliable information network (see Related resources).
I have had excellent results with other trichotillomania patients—especially children and adolescents. Simply naming their condition and demystifying the problem can be therapeutic. Many patients have responded to SSRIs combined with CBT.
Not long ago, trichotillomania patients were met with ignorance and disbelief within the medical community as the disorder was poorly understood. We need to break this cycle of shame and continue investigating treatment strategies.
- StopPulling.com, an interactive behavioral program for persons with trichotillomania. www.stoppulling.com.
- Penzel F. The hair pulling problem: a complete guide to trichotillomania. New York: Oxford University Press, 2003.
- Keuthen NJ, Stein DJ, Christenson GA. Help for hair pullers: understanding and coping with trichotillomania. Oakland, CA: New Harbinger Publications, 2001.
Drug brand names
- Amitriptyline • Elavil
- Buspirone • BuSpar
- Clomipramine • Anafranil
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Lithium • Eskalith, others
- Methylphenidate • Concerta, Ritalin
- Naltrexone • ReVia
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
- Ziprasidone • Geodon
Disclosure
Dr. Lundt receives research grants from and/or is a speaker for Eli Lilly and Co., Pfizer Inc., GlaxoSmithKline, and Bristol-Myers Squibb Co.
1. Mansueto C, Ninan PT, Rothbaum B. Trichotillomania and its treatment in adults: a guide for clinicians. Available at: (http://www.trich.org/articles/view_default.asp?filename="0305_Cases" aid=22&yd= researchers_intro). Accessed April 13, 2004
2. Bouwer C, Stein DJ. Trichobezoars in trichotillomania. Psychosom Med 1998;60:658-60.
3. Philippopoulos GS. A case of trichotillomania (hair pulling). Doc Geigy Acta Psychosom 1961;9:304-12.
4. Lee J. Bezoars and foreign bodies in the stomach. Gastrointest Endosc 1996;6:605-19.
5. Christenson GA, Crow SJ. The characterization and treatment of trichotillomania. Clin Psychiatry 1996;57(suppl 8):42-7.
6. Lal MM, Dhall JC. Trichobezoar: A collective analysis of 39 cases from India with a case report. Indian J Pediatr 1975;12:351-3.
7. DeBakey M, Ochsner W. Bezoars and concretions: A comprehensive review of the literature with an analysis of 303 collected cases and a presentation of 8 additional cases. Surgery 1939;4:934-63.
8. Khouzam HR, Battista MA, Byers PE. An overview of trichotillomania and its response to treatment with quetiapine. Psychiatry 2002;65:261-70.
9. Keuthen NJ, Fraim C, Deckersbach T, et al. Longitudinal follow-up of naturalistic treatment outcome in patients with trichotillomania. J Clin Psychiatry 2001;62:101-7.
10. Swedo SE, Leonard HL, Rapoport JL, et al. A double-blind comparison of clomipramine and desipramine in the treatment of trichotillomania (hair pulling). N Engl J Med 1989;8:497-501.
11. van Minnen A, Hoogduin KA, Keijsers GP, et al. Treatment of trichotillomania with behavioral therapy or fluoxetine: a randomized, waiting-list controlled study. Arch Gen Psychiatry 2003;60:517-22.
12. Gabriel A. A case of resistant trichotillomania treated with risperidone-augmented fluvoxamine. Can J Psychiatry 2001;46:285-6.
13. Ravindran AV, Lapierre YD, Anisman H. Obsessive-compulsive spectrum disorders: Effective treatment with paroxetine. Can J Psychiatry 1999;44:805-7.
14. Bradford JM, Gratzer TG. A treatment for impulse control disorders and paraphilia: a case report. Can J Psychiatry 1995;40:4-5.
15. Van Ameringen M, Mancini C, Oakman JM, Farvolden p. The potential role of haloperidol in the treatment of trichotillomania. J Affect Disord 1999;56:219-26.
16. Gupta MA, Gupta AK. Olanzapine is effective in the management of some self-induced dermatoses: Three case reports. Cutis 2000;66:143-6.
17. Stein DJ, Hollander E. Low-dose pimozide augmentation of serotonin reuptake blockers in the treatment of trichotillomania. J Clin Psych 1992;53:123-6.
18. Senturk V, Tanriverdi N. Resistant trichotillomania and risperidone. Psychosomatics 2002;43:429-30
19. Christenson GA, Popkin MK, Mackenzie TB, Realmuto GM. Lithium treatment of chronic hair pulling. J Clin Psychiatry 1991;52:116-20.
History: Bald at age 9
Ms. D, age 41, began compulsively pulling out and eating her hair at age 8. When she didn’t get her way at home or was nervous about school, she would sit for hours, pulling and eating a strand or two at a time, ultimately ingesting a clump of hair.
By age 9, Ms. D was bald. In grade school, she often wore hats and scarves to class to avoid teasing from other children about her baldness. In high school, she kept to herself and frequently wore wigs.
Ms. D stops pulling for brief periods and her hair grows out, but she invariably resumes pulling when psychosocial stressors mount. Many of life’s normal anxieties—job interviews, work-related stress, social rejection—trigger episodes.
When she is bald, Ms. D pulls and eats hair off her wig. Over the years, she has spent thousands of dollars on custom-made wigs that mask her baldness while feeding her habit.
Ms. D’s episodes are increasingly interfering with her life. She has been steadily employed as an office assistant, but does not socialize with coworkers. She has not dated in years, and during an exacerbation leaves home only to go to work. She also pulls her eyelashes and eyebrows and picks her nails and cuticles.
Ms. D first presented in 1994 after seeing a television segment I did on trichotillomania. At intake, she was wearing a wig and exhibited anxious mood. She also has Crohn’s disease; a gastroenterologist monitors her closely.
Ms. D reports compulsive counting and checking but denies other similar behaviors. No immediate family members have exhibited obsessive-compulsive or hair-pulling behaviors. Her father abused alcohol and a sister has a stuttering problem, although Ms. D denies that these have affected her psychologically.
Ms. D’s hair-pulling behavior suggests:
- a pica disorder
- an impulse control disorder
- or an obsessive-compulsive disorder?
- Recurrent pulling out of one’s own hair, resulting in noticeable hair loss.
- Increasing tension immediately before pulling out the hair or when attempting to resist the behavior.
- Pleasure, gratification, or relief while pulling out the hair.
- The disturbance is not better explained as another mental disorder and is not caused by a dermatological or other general medical condition.
- The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders, 4th ed., text revision. Copyright 2000. American Psychiatric Association.
Dr. Lundt’s observations
Trichotillomania, defined as compulsive pulling of hair, usually begins in childhood or adolescence. Scalp hair is most commonly pulled, but some patients also pull their eyelashes, pubic hair, and other body hair. Some, especially children, have reportedly pulled their pets’ hair.
Mansueto et al estimate that trichotillomania afflicts approximately 1.5% of males and 3.5% of females.1 These estimates, however, do not include persons with the disorder who are too embarrassed to seek treatment.
DSM-IV-TR classifies trichotillomania as an impulse control disorder (Box). Although comorbid anxiety and depressive disorders are common, Ms. D did not meet criteria for any other psychiatric disorder.
Trichotillomania often is episodic. Months or years of abstinence is common after periods of exacerbation, usually caused by stress (Figure).
Many clinicians mistakenly consider trichotillomania a benign disorder with few consequences beyond alopecia.2 Some patients, however, progress into trichophagia—ingestion of pulled hair. Trichophagia is a form of pica disorder, typically defined as persistent eating of non-nutritive substances. Patients often harbor tremendous shame over their hair-eating behavior and resist psychiatric or medical treatment.2
The undigested hair can form sometimes massive clumps called trichobezoars, which are most common among children and the developmentally disabled.4 Persons with trichophagia face a 37.5% risk of forming a trichobezoar.5 The mass can cause abdominal pain, nausea, vomiting, and weight loss; complications include GI obstruction, ulceration, perforation, and peritonitis.6 An untreated trichobezoar can be fatal,7 although such deaths are rare among patients being treated for trichotillomania.
Patients with trichotillomania often respond to medications used to treat obsessive-compulsive disorder, such as clomipramine. Some clinicians believe this agent is more effective than selective serotonin reuptake inhibitors (SSRIs) but more difficult to tolerate. For Ms. D, I started with both.
Treatment: ‘I Don’t need medication’
Initial treatments—including fluoxetine, 20 mg/d for 6 months; hypnotherapy; and clomipramine, 25 mg/d—were unsuccessful. Ms. D was only marginally compliant, believing that she did not need medication.
I referred Ms. D to an out-of-state residential behavioral program specializing in trichotillomania, but she refused to go even as her hair-pulling intensified. Clomipramine was gradually increased to 75 mg nightly, briefly decreasing her pulling, then to 100 mg nightly when symptoms re-emerged. Clomipramine blood levels were monitored with each dosage change to guard against CNS and cardiac toxicity and other side effects (GI complaints, dizziness, cardiac arrhythmias, somnolence).
After watching for seasonal patterns, I found that Ms. D’s hair-pulling worsened during the winter, although no seasonal change in mood was detected. Phototherapy produced initial success, but Ms. D continued to pull her eyelashes.
Eight weeks later, however, Ms. D’s symptoms escalated. Clomipramine was increased to 150 mg nightly, resulting in blood levels of 99 ng/mL for clomipramine and 204 ng/mL for the metabolite N-desmethylclomipramine—both within the therapeutic range. As she continued pulling, I added buspirone, 10 mg/d.
At this point, would you:
- continue clomipramine and increase the dosage?
- discontinue clomipramine and start another psychotropic?
- or maintain clomipramine at the same dosage and add another psychotropic?
Dr. Lundt’s observations
Drug treatment of trichotillomania has not been studied extensively or long-term, and no consensus exists. Psychoanalysis, cognitive-behavioral therapy (CBT), and hypnotherapy are usually administered with psychotropics.8 Patients often respond to treatment at first, then reach a plateau and resume pulling their hair.9
Numerous psychotropics are used off-label to treat trichotillomania. Several agents have been shown in clinical trials and case reports to reduce hair pulling/eating behaviors (Table), but these findings are limited by small sample size, lack of control groups, and lack of a standard symptom rating scale.
Figure Trichotillomania: Excessive grooming, habit, or vicious circle?
Most clinicians begin with SSRIs because they are generally well tolerated, even at high dosages. Monotherapy often is not adequate for trichotillomania, however. Medication augmentation is common, although little empiric data support this practice.
When clomipramine did not work initally, I explored serotonergic combination strategies.
Table
Medications shown to benefit patients with trichotillomania
| Drug | Evidence | Dosage range (mg/d) | Potential side effects |
|---|---|---|---|
| First-line | |||
| Tricyclic | |||
| Clomipramine | Swedo et al10 | 50 to 300 | Sedation, weight gain, cardiac arrythmias |
| SSRIs | |||
| Fluoxetine | van Minnen et al11 | 20 to 60 | GI symptoms, insomnia |
| Fluvoxamine | Gabriel12 | 50 to 250 | Sexual dysfunction, weight gain |
| Paroxetine | Ravindran et al13 | 20 to 60 | Sexual dysfunction, weight gain |
| Sertraline | Bradford and Gratzer14 | 50 to 200 | Sexual dysfunction, GI symptoms, insomnia |
| Second-line | |||
| Antipsychotics | |||
| Haloperidol | Van Ameringen et al15 | 0.25 to 2 | Sedation, EPS |
| Olanzapine | Gupta and Gupta16 | 2.5 to 10 | Sedation, weight gain |
| Pimozide | Stein and Hollander17 | 25 to 200 | Restlessness, EPS |
| Quetiapine | Khouzam et al8 | 25 to 200 | Sedation |
| Risperidone | Gabriel12 Senturk and Tanriverdi18 | 0.5 to 4.0 | Sedation, hyperprolactinemia |
| Mood stabilizer | |||
| Lithium | Christenson et al19 | 900 to 1,500 | Increased thirst, weight gain, tremor |
| EPS: extrapyramidal symptoms | |||
Further treatment: Relapse, resection
Ms. D was lost to follow-up for 1 year. She returned in 1996, just after undergoing a laparotomy for removal of a trichobezoar large enough to fill two 2-inch-by-6-inch bags. She also had been treated for pneumonia and a pulmonary embolus.
Riddled with shame and embarrassment, Ms. D had stopped pulling for 10 months, during which time she was off medication. Her pulling behaviors re-emerged, however, and clomipramine was restarted and titrated to 250 mg nightly.
One year later, a second trichobezoar was resected. Her clomipramine/N-desmethylclomipramine level reached 1,535 ng/mL, although an ECG reading was normal. Subsequent clomipramine/N-desmethylclomipramine blood levels were within the therapeutic range. Fluvoxamine, 25 mg/d titrated across 6 weeks to 150 mg/d, was added.
Again, Ms. D stopped taking her medications and was lost to follow-up. Her gastroenterologist began managing her care and started sertraline, dosage unknown, to address her depressed mood. A third trichobezoar was removed.
When Ms. D returned to my practice, I resumed CBT and increased sertraline over 1 month from 100 to 300 mg/d. Adding olanzapine, 2.5 mg/d, diminished her anxiety and markedly decreased her hair pulling.
Months later, her hair-pulling/eating behaviors again intensified, resulting in a small-bowel obstruction and a fourth trichobezoar removal. Olanzapine was increased to 5 mg nightly without significant benefit and with sedating effects.
Clomipramine, 125 mg/d, was reintroduced and her symptoms improved dramatically. On a regimen of sertraline, clomipramine and olanzapine, Ms. D remained stable for 2 years.
Last year, however, a fifth trichobezoar measuring 20 x 15 cm was removed. Subsequent trials of methylphenidate, titrated to 72 mg every morning, and tramadol, titrated to 100 mg/d, were unsuccessful.
After 10 years of medication and psychotherapy with three different providers, Ms. D’s hair-pulling/eating behaviors persist. She is taking ziprasidone, 120 mg bid, and naltrexone, 100 mg bid, to help her impulse control, as well as sertraline, 300 mg/d, and clomipramine, 125 mg/d. Another trichobezoar removal—her sixth in 8 years—is scheduled.
What strategies exist for minimizing Ms. D’s hair-pulling behavior and keeping her in therapy?
Dr. Lundt’s observations
Trichotillomania’s waxing and waning course—and its destructive effects on a patient’s self-esteem—pose a clinical challenge. The disorder’s severity can range from cosmetically annoying to life-threatening, as in Ms. D’s case. Patients embarrassed by their behavior often prematurely leave treatment, desperate to cut off all social contact—including medical appointments.
It is crucial to maintain a nonjudgmental, inviting demeanor to alleviate the patient’s fears and facilitate a return to treatment. Support groups, especially online, can help decrease patients’ isolation and provide a reliable information network (see Related resources).
I have had excellent results with other trichotillomania patients—especially children and adolescents. Simply naming their condition and demystifying the problem can be therapeutic. Many patients have responded to SSRIs combined with CBT.
Not long ago, trichotillomania patients were met with ignorance and disbelief within the medical community as the disorder was poorly understood. We need to break this cycle of shame and continue investigating treatment strategies.
- StopPulling.com, an interactive behavioral program for persons with trichotillomania. www.stoppulling.com.
- Penzel F. The hair pulling problem: a complete guide to trichotillomania. New York: Oxford University Press, 2003.
- Keuthen NJ, Stein DJ, Christenson GA. Help for hair pullers: understanding and coping with trichotillomania. Oakland, CA: New Harbinger Publications, 2001.
Drug brand names
- Amitriptyline • Elavil
- Buspirone • BuSpar
- Clomipramine • Anafranil
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Lithium • Eskalith, others
- Methylphenidate • Concerta, Ritalin
- Naltrexone • ReVia
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
- Ziprasidone • Geodon
Disclosure
Dr. Lundt receives research grants from and/or is a speaker for Eli Lilly and Co., Pfizer Inc., GlaxoSmithKline, and Bristol-Myers Squibb Co.
History: Bald at age 9
Ms. D, age 41, began compulsively pulling out and eating her hair at age 8. When she didn’t get her way at home or was nervous about school, she would sit for hours, pulling and eating a strand or two at a time, ultimately ingesting a clump of hair.
By age 9, Ms. D was bald. In grade school, she often wore hats and scarves to class to avoid teasing from other children about her baldness. In high school, she kept to herself and frequently wore wigs.
Ms. D stops pulling for brief periods and her hair grows out, but she invariably resumes pulling when psychosocial stressors mount. Many of life’s normal anxieties—job interviews, work-related stress, social rejection—trigger episodes.
When she is bald, Ms. D pulls and eats hair off her wig. Over the years, she has spent thousands of dollars on custom-made wigs that mask her baldness while feeding her habit.
Ms. D’s episodes are increasingly interfering with her life. She has been steadily employed as an office assistant, but does not socialize with coworkers. She has not dated in years, and during an exacerbation leaves home only to go to work. She also pulls her eyelashes and eyebrows and picks her nails and cuticles.
Ms. D first presented in 1994 after seeing a television segment I did on trichotillomania. At intake, she was wearing a wig and exhibited anxious mood. She also has Crohn’s disease; a gastroenterologist monitors her closely.
Ms. D reports compulsive counting and checking but denies other similar behaviors. No immediate family members have exhibited obsessive-compulsive or hair-pulling behaviors. Her father abused alcohol and a sister has a stuttering problem, although Ms. D denies that these have affected her psychologically.
Ms. D’s hair-pulling behavior suggests:
- a pica disorder
- an impulse control disorder
- or an obsessive-compulsive disorder?
- Recurrent pulling out of one’s own hair, resulting in noticeable hair loss.
- Increasing tension immediately before pulling out the hair or when attempting to resist the behavior.
- Pleasure, gratification, or relief while pulling out the hair.
- The disturbance is not better explained as another mental disorder and is not caused by a dermatological or other general medical condition.
- The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders, 4th ed., text revision. Copyright 2000. American Psychiatric Association.
Dr. Lundt’s observations
Trichotillomania, defined as compulsive pulling of hair, usually begins in childhood or adolescence. Scalp hair is most commonly pulled, but some patients also pull their eyelashes, pubic hair, and other body hair. Some, especially children, have reportedly pulled their pets’ hair.
Mansueto et al estimate that trichotillomania afflicts approximately 1.5% of males and 3.5% of females.1 These estimates, however, do not include persons with the disorder who are too embarrassed to seek treatment.
DSM-IV-TR classifies trichotillomania as an impulse control disorder (Box). Although comorbid anxiety and depressive disorders are common, Ms. D did not meet criteria for any other psychiatric disorder.
Trichotillomania often is episodic. Months or years of abstinence is common after periods of exacerbation, usually caused by stress (Figure).
Many clinicians mistakenly consider trichotillomania a benign disorder with few consequences beyond alopecia.2 Some patients, however, progress into trichophagia—ingestion of pulled hair. Trichophagia is a form of pica disorder, typically defined as persistent eating of non-nutritive substances. Patients often harbor tremendous shame over their hair-eating behavior and resist psychiatric or medical treatment.2
The undigested hair can form sometimes massive clumps called trichobezoars, which are most common among children and the developmentally disabled.4 Persons with trichophagia face a 37.5% risk of forming a trichobezoar.5 The mass can cause abdominal pain, nausea, vomiting, and weight loss; complications include GI obstruction, ulceration, perforation, and peritonitis.6 An untreated trichobezoar can be fatal,7 although such deaths are rare among patients being treated for trichotillomania.
Patients with trichotillomania often respond to medications used to treat obsessive-compulsive disorder, such as clomipramine. Some clinicians believe this agent is more effective than selective serotonin reuptake inhibitors (SSRIs) but more difficult to tolerate. For Ms. D, I started with both.
Treatment: ‘I Don’t need medication’
Initial treatments—including fluoxetine, 20 mg/d for 6 months; hypnotherapy; and clomipramine, 25 mg/d—were unsuccessful. Ms. D was only marginally compliant, believing that she did not need medication.
I referred Ms. D to an out-of-state residential behavioral program specializing in trichotillomania, but she refused to go even as her hair-pulling intensified. Clomipramine was gradually increased to 75 mg nightly, briefly decreasing her pulling, then to 100 mg nightly when symptoms re-emerged. Clomipramine blood levels were monitored with each dosage change to guard against CNS and cardiac toxicity and other side effects (GI complaints, dizziness, cardiac arrhythmias, somnolence).
After watching for seasonal patterns, I found that Ms. D’s hair-pulling worsened during the winter, although no seasonal change in mood was detected. Phototherapy produced initial success, but Ms. D continued to pull her eyelashes.
Eight weeks later, however, Ms. D’s symptoms escalated. Clomipramine was increased to 150 mg nightly, resulting in blood levels of 99 ng/mL for clomipramine and 204 ng/mL for the metabolite N-desmethylclomipramine—both within the therapeutic range. As she continued pulling, I added buspirone, 10 mg/d.
At this point, would you:
- continue clomipramine and increase the dosage?
- discontinue clomipramine and start another psychotropic?
- or maintain clomipramine at the same dosage and add another psychotropic?
Dr. Lundt’s observations
Drug treatment of trichotillomania has not been studied extensively or long-term, and no consensus exists. Psychoanalysis, cognitive-behavioral therapy (CBT), and hypnotherapy are usually administered with psychotropics.8 Patients often respond to treatment at first, then reach a plateau and resume pulling their hair.9
Numerous psychotropics are used off-label to treat trichotillomania. Several agents have been shown in clinical trials and case reports to reduce hair pulling/eating behaviors (Table), but these findings are limited by small sample size, lack of control groups, and lack of a standard symptom rating scale.
Figure Trichotillomania: Excessive grooming, habit, or vicious circle?
Most clinicians begin with SSRIs because they are generally well tolerated, even at high dosages. Monotherapy often is not adequate for trichotillomania, however. Medication augmentation is common, although little empiric data support this practice.
When clomipramine did not work initally, I explored serotonergic combination strategies.
Table
Medications shown to benefit patients with trichotillomania
| Drug | Evidence | Dosage range (mg/d) | Potential side effects |
|---|---|---|---|
| First-line | |||
| Tricyclic | |||
| Clomipramine | Swedo et al10 | 50 to 300 | Sedation, weight gain, cardiac arrythmias |
| SSRIs | |||
| Fluoxetine | van Minnen et al11 | 20 to 60 | GI symptoms, insomnia |
| Fluvoxamine | Gabriel12 | 50 to 250 | Sexual dysfunction, weight gain |
| Paroxetine | Ravindran et al13 | 20 to 60 | Sexual dysfunction, weight gain |
| Sertraline | Bradford and Gratzer14 | 50 to 200 | Sexual dysfunction, GI symptoms, insomnia |
| Second-line | |||
| Antipsychotics | |||
| Haloperidol | Van Ameringen et al15 | 0.25 to 2 | Sedation, EPS |
| Olanzapine | Gupta and Gupta16 | 2.5 to 10 | Sedation, weight gain |
| Pimozide | Stein and Hollander17 | 25 to 200 | Restlessness, EPS |
| Quetiapine | Khouzam et al8 | 25 to 200 | Sedation |
| Risperidone | Gabriel12 Senturk and Tanriverdi18 | 0.5 to 4.0 | Sedation, hyperprolactinemia |
| Mood stabilizer | |||
| Lithium | Christenson et al19 | 900 to 1,500 | Increased thirst, weight gain, tremor |
| EPS: extrapyramidal symptoms | |||
Further treatment: Relapse, resection
Ms. D was lost to follow-up for 1 year. She returned in 1996, just after undergoing a laparotomy for removal of a trichobezoar large enough to fill two 2-inch-by-6-inch bags. She also had been treated for pneumonia and a pulmonary embolus.
Riddled with shame and embarrassment, Ms. D had stopped pulling for 10 months, during which time she was off medication. Her pulling behaviors re-emerged, however, and clomipramine was restarted and titrated to 250 mg nightly.
One year later, a second trichobezoar was resected. Her clomipramine/N-desmethylclomipramine level reached 1,535 ng/mL, although an ECG reading was normal. Subsequent clomipramine/N-desmethylclomipramine blood levels were within the therapeutic range. Fluvoxamine, 25 mg/d titrated across 6 weeks to 150 mg/d, was added.
Again, Ms. D stopped taking her medications and was lost to follow-up. Her gastroenterologist began managing her care and started sertraline, dosage unknown, to address her depressed mood. A third trichobezoar was removed.
When Ms. D returned to my practice, I resumed CBT and increased sertraline over 1 month from 100 to 300 mg/d. Adding olanzapine, 2.5 mg/d, diminished her anxiety and markedly decreased her hair pulling.
Months later, her hair-pulling/eating behaviors again intensified, resulting in a small-bowel obstruction and a fourth trichobezoar removal. Olanzapine was increased to 5 mg nightly without significant benefit and with sedating effects.
Clomipramine, 125 mg/d, was reintroduced and her symptoms improved dramatically. On a regimen of sertraline, clomipramine and olanzapine, Ms. D remained stable for 2 years.
Last year, however, a fifth trichobezoar measuring 20 x 15 cm was removed. Subsequent trials of methylphenidate, titrated to 72 mg every morning, and tramadol, titrated to 100 mg/d, were unsuccessful.
After 10 years of medication and psychotherapy with three different providers, Ms. D’s hair-pulling/eating behaviors persist. She is taking ziprasidone, 120 mg bid, and naltrexone, 100 mg bid, to help her impulse control, as well as sertraline, 300 mg/d, and clomipramine, 125 mg/d. Another trichobezoar removal—her sixth in 8 years—is scheduled.
What strategies exist for minimizing Ms. D’s hair-pulling behavior and keeping her in therapy?
Dr. Lundt’s observations
Trichotillomania’s waxing and waning course—and its destructive effects on a patient’s self-esteem—pose a clinical challenge. The disorder’s severity can range from cosmetically annoying to life-threatening, as in Ms. D’s case. Patients embarrassed by their behavior often prematurely leave treatment, desperate to cut off all social contact—including medical appointments.
It is crucial to maintain a nonjudgmental, inviting demeanor to alleviate the patient’s fears and facilitate a return to treatment. Support groups, especially online, can help decrease patients’ isolation and provide a reliable information network (see Related resources).
I have had excellent results with other trichotillomania patients—especially children and adolescents. Simply naming their condition and demystifying the problem can be therapeutic. Many patients have responded to SSRIs combined with CBT.
Not long ago, trichotillomania patients were met with ignorance and disbelief within the medical community as the disorder was poorly understood. We need to break this cycle of shame and continue investigating treatment strategies.
- StopPulling.com, an interactive behavioral program for persons with trichotillomania. www.stoppulling.com.
- Penzel F. The hair pulling problem: a complete guide to trichotillomania. New York: Oxford University Press, 2003.
- Keuthen NJ, Stein DJ, Christenson GA. Help for hair pullers: understanding and coping with trichotillomania. Oakland, CA: New Harbinger Publications, 2001.
Drug brand names
- Amitriptyline • Elavil
- Buspirone • BuSpar
- Clomipramine • Anafranil
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Lithium • Eskalith, others
- Methylphenidate • Concerta, Ritalin
- Naltrexone • ReVia
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
- Ziprasidone • Geodon
Disclosure
Dr. Lundt receives research grants from and/or is a speaker for Eli Lilly and Co., Pfizer Inc., GlaxoSmithKline, and Bristol-Myers Squibb Co.
1. Mansueto C, Ninan PT, Rothbaum B. Trichotillomania and its treatment in adults: a guide for clinicians. Available at: (http://www.trich.org/articles/view_default.asp?filename="0305_Cases" aid=22&yd= researchers_intro). Accessed April 13, 2004
2. Bouwer C, Stein DJ. Trichobezoars in trichotillomania. Psychosom Med 1998;60:658-60.
3. Philippopoulos GS. A case of trichotillomania (hair pulling). Doc Geigy Acta Psychosom 1961;9:304-12.
4. Lee J. Bezoars and foreign bodies in the stomach. Gastrointest Endosc 1996;6:605-19.
5. Christenson GA, Crow SJ. The characterization and treatment of trichotillomania. Clin Psychiatry 1996;57(suppl 8):42-7.
6. Lal MM, Dhall JC. Trichobezoar: A collective analysis of 39 cases from India with a case report. Indian J Pediatr 1975;12:351-3.
7. DeBakey M, Ochsner W. Bezoars and concretions: A comprehensive review of the literature with an analysis of 303 collected cases and a presentation of 8 additional cases. Surgery 1939;4:934-63.
8. Khouzam HR, Battista MA, Byers PE. An overview of trichotillomania and its response to treatment with quetiapine. Psychiatry 2002;65:261-70.
9. Keuthen NJ, Fraim C, Deckersbach T, et al. Longitudinal follow-up of naturalistic treatment outcome in patients with trichotillomania. J Clin Psychiatry 2001;62:101-7.
10. Swedo SE, Leonard HL, Rapoport JL, et al. A double-blind comparison of clomipramine and desipramine in the treatment of trichotillomania (hair pulling). N Engl J Med 1989;8:497-501.
11. van Minnen A, Hoogduin KA, Keijsers GP, et al. Treatment of trichotillomania with behavioral therapy or fluoxetine: a randomized, waiting-list controlled study. Arch Gen Psychiatry 2003;60:517-22.
12. Gabriel A. A case of resistant trichotillomania treated with risperidone-augmented fluvoxamine. Can J Psychiatry 2001;46:285-6.
13. Ravindran AV, Lapierre YD, Anisman H. Obsessive-compulsive spectrum disorders: Effective treatment with paroxetine. Can J Psychiatry 1999;44:805-7.
14. Bradford JM, Gratzer TG. A treatment for impulse control disorders and paraphilia: a case report. Can J Psychiatry 1995;40:4-5.
15. Van Ameringen M, Mancini C, Oakman JM, Farvolden p. The potential role of haloperidol in the treatment of trichotillomania. J Affect Disord 1999;56:219-26.
16. Gupta MA, Gupta AK. Olanzapine is effective in the management of some self-induced dermatoses: Three case reports. Cutis 2000;66:143-6.
17. Stein DJ, Hollander E. Low-dose pimozide augmentation of serotonin reuptake blockers in the treatment of trichotillomania. J Clin Psych 1992;53:123-6.
18. Senturk V, Tanriverdi N. Resistant trichotillomania and risperidone. Psychosomatics 2002;43:429-30
19. Christenson GA, Popkin MK, Mackenzie TB, Realmuto GM. Lithium treatment of chronic hair pulling. J Clin Psychiatry 1991;52:116-20.
1. Mansueto C, Ninan PT, Rothbaum B. Trichotillomania and its treatment in adults: a guide for clinicians. Available at: (http://www.trich.org/articles/view_default.asp?filename="0305_Cases" aid=22&yd= researchers_intro). Accessed April 13, 2004
2. Bouwer C, Stein DJ. Trichobezoars in trichotillomania. Psychosom Med 1998;60:658-60.
3. Philippopoulos GS. A case of trichotillomania (hair pulling). Doc Geigy Acta Psychosom 1961;9:304-12.
4. Lee J. Bezoars and foreign bodies in the stomach. Gastrointest Endosc 1996;6:605-19.
5. Christenson GA, Crow SJ. The characterization and treatment of trichotillomania. Clin Psychiatry 1996;57(suppl 8):42-7.
6. Lal MM, Dhall JC. Trichobezoar: A collective analysis of 39 cases from India with a case report. Indian J Pediatr 1975;12:351-3.
7. DeBakey M, Ochsner W. Bezoars and concretions: A comprehensive review of the literature with an analysis of 303 collected cases and a presentation of 8 additional cases. Surgery 1939;4:934-63.
8. Khouzam HR, Battista MA, Byers PE. An overview of trichotillomania and its response to treatment with quetiapine. Psychiatry 2002;65:261-70.
9. Keuthen NJ, Fraim C, Deckersbach T, et al. Longitudinal follow-up of naturalistic treatment outcome in patients with trichotillomania. J Clin Psychiatry 2001;62:101-7.
10. Swedo SE, Leonard HL, Rapoport JL, et al. A double-blind comparison of clomipramine and desipramine in the treatment of trichotillomania (hair pulling). N Engl J Med 1989;8:497-501.
11. van Minnen A, Hoogduin KA, Keijsers GP, et al. Treatment of trichotillomania with behavioral therapy or fluoxetine: a randomized, waiting-list controlled study. Arch Gen Psychiatry 2003;60:517-22.
12. Gabriel A. A case of resistant trichotillomania treated with risperidone-augmented fluvoxamine. Can J Psychiatry 2001;46:285-6.
13. Ravindran AV, Lapierre YD, Anisman H. Obsessive-compulsive spectrum disorders: Effective treatment with paroxetine. Can J Psychiatry 1999;44:805-7.
14. Bradford JM, Gratzer TG. A treatment for impulse control disorders and paraphilia: a case report. Can J Psychiatry 1995;40:4-5.
15. Van Ameringen M, Mancini C, Oakman JM, Farvolden p. The potential role of haloperidol in the treatment of trichotillomania. J Affect Disord 1999;56:219-26.
16. Gupta MA, Gupta AK. Olanzapine is effective in the management of some self-induced dermatoses: Three case reports. Cutis 2000;66:143-6.
17. Stein DJ, Hollander E. Low-dose pimozide augmentation of serotonin reuptake blockers in the treatment of trichotillomania. J Clin Psych 1992;53:123-6.
18. Senturk V, Tanriverdi N. Resistant trichotillomania and risperidone. Psychosomatics 2002;43:429-30
19. Christenson GA, Popkin MK, Mackenzie TB, Realmuto GM. Lithium treatment of chronic hair pulling. J Clin Psychiatry 1991;52:116-20.