User login
Gestational diabetes and oral hypoglycemic agents: A fresh look at the safety profile
- Well-designed studies have found no association between oral hypoglycemic agents and congenital malformations. Data suggest that glyburide and possibly metformin are safe and effective for gestational diabetes.
- Reserve medical therapy with oral agents for patients whose fasting plasma glucose levels remain above 95 mg/dL (or postprandial levels above 120 mg/dL) despite diet therapy, and for those who are not appropriate candidates for diet therapy alone.
- Substitute combination or insulin therapy for oral therapy if desired levels of glucose control are not achieved.
Although use of oral hypoglycemic and antihyperglycemic agents in pregnancy has long been thought to increase the risk of fetal anomalies, 2 trials within the past decade indicate otherwise. In those trials, blood glucose levels—rather than the drugs themselves—were responsible for the greater rate of anomalies.1,2
As a result, oral hypoglycemic agents are gaining recognition as a safe and effective alternative to insulin when diet alone fails to optimize the glycemic profile in gestational diabetes. Sulfonylureas are the only oral agents that have been studied in randomized, controlled trials in women with gestational diabetes,3 but other drugs may have an even greater therapeutic effect. Indeed, use of these other agents for type 2 diabetes has become the standard of care for the nongravid patient.4,5 Only recently has their use in pregnancy become arguable in US scientific forums.
Ninety percent of gravidas with diabetes—the most common medical complication of pregnancy—have gestational diabetes, and a significant number (20% to 50%) develop type 2 diabetes within 10 years.6 Both gestational and type 2 diabetes are characterized by peripheral insulin resistance, decreased insulin secretion (declining betacell function), and impaired regulation of hepatic glucose, each of which represents a different point in the continuum of deteriorating glucose tolerance.
Intensified therapy can maximize pregnancy outcome by decreasing the rates of macrosomia, metabolic and respiratory complications, shoulder dystocia, neonatal intensive care admission, and other complications to rates found in the general population. This treatment approach requires self-monitoring of blood glucose several times daily using a memory reflectance meter, adherence to proper criteria when initiating glyburide or insulin therapy (ie, fasting plasma glucose <90 mg/dL), and achievement of targeted glycemic control.7
Here, a specific treatment plan is offered along with a review of the evidence on use of oral agents in pregnancy. In addition, earlier interpretations that may have distorted the overall picture are discussed.
Studies of oral hypoglycemics and fetal anomalies
Early case reports and small-scale studies suggested an association between oral hypoglycemic agents and congenital anomalies. This anecdotal evidence was even translated into guidelines by the American College of Obstetricians and Gynecologists and the American Diabetes Association, among others. Unfortunately, these guidelines were based largely on a retrospective study involving 20 women with type 2 diabetes—all with glycosylated hemoglobin A1c concentrations exceeding 8%—in whom there was an increased rate of anomalies.8 However, the fact that maternal hyperglycemia existed prior to conception makes it impossible to determine whether the increased rate of anomalies was the result of medication or elevated glucose levels.
Other drawbacks of studies from this time: Few of the agents investigated are in common use today; most studies reported perinatal mortality and congenital anomalies, but failed to address neonatal morbidity; and many subjects had type 2 diabetes.9-15
In the past decade, 2 studies have suggested there is no association between oral hypoglycemic agents and congenital malformations. For example, no significant adverse effects associated with oral therapy were found in a study of 332 women with type 2 diabetes treated with diet therapy, exogenous insulin, or sulfonylurea compounds during the first 8 weeks of gestation.1 However, the level of glycemia and maternal age contributed significantly to the rate of anomalies.
Among the factors that determine the placental transfer capability of a drug are molecular weight, pKa, lipid solubility, placental blood flow, blood protein binding, and elimination half-life.
In the early 1990s, my colleagues and I evaluated the potential of first-generation and second-generation sulfonylureas to cross the placenta, and found no significant transport of glyburide in the maternal-to-fetal and fetal-to-maternal directions.1 Even increasing the glyburide concentration to 100 times the therapeutic level did not alter transport noticeably. Glyburide remained undetected when cord blood was analyzed using high-performance lipid chromatography with appropriate gradient concentration between the maternal and fetal sites.2 Moreover, at least 99.8% of the glyburide was bound to protein. Thus, glyburide was neither metabolized nor appropriated by the placenta.
In a second series of studies, we found that second-generation oral hypoglycemic agents—especially glyburide—did not significantly cross diabetic and nondiabetic placentae.3,4 Fetal concentrations reached no more than 1% to 2% of maternal concentrations. Glipizide crossed the placenta in small amounts that were significantly higher than glyburide. Tolbutamide diffused across the placenta most freely.
REFERENCES
1. Elliot B, Langer O, Schenker S, Jonhson RF. Insignificant transfer of glyburide occurs across the human placenta. Am J Obstet Gynecol. 1991;165:807-812.
2. Langer O. Oral hypoglycemic agents and the pregnant diabetic: “from bench to bedside.” Semin Perinatol. 2002;26:215-224.
3. Elliot B, Schenker S, Langer O, Johnson R, Prihoda T. Comparative placental transport of oral hypoglycemic agents. A model of human placental drug transfer. Am J Obstet Gynecol. 1994;171:653-660.
4. Elliot B, Langer O, Schussling F. A model of human placental drug transfer. Am J Obstet Gynecol. 1997;176:527-530.
We reached similar conclusions in a retrospective analysis of 850 women with type 2 diabetes who were exposed to oral hypoglycemic agents, insulin, or diet therapy prior to and during the first trimester of pregnancy.2 Again, it was blood glucose and not the mode of therapy that had the net effect on the rate of anomalies.
In a randomized study in 1971, Notelovitz et al9 compared the efficacies of tolbutamide, chlorpropamide, diet, and insulin in a randomized trial. When glycemic control was good (ie, blood glucose less than 150 mg/dL), there were no significant differences among the groups in perinatal mortality and congenital anomalies.
In a prospective, randomized trial, we also compared the efficacy of glyburide and insulin in 404 women with singleton pregnancies, and found no significant differences in maternal hypoglycemic episodes, preeclampsia, rate of cesarean section—or number of patients achieving the desired level of control.3 As for the neonates, no significant differences were found in the rate of macrosomia; large-for-gestational-age infants; metabolic, respiratory, and hematologic complications; and congenital anomalies.
Interestingly, no glyburide was detected in the arterial cord serum of any infant in the glyburide group, even though fetal insulin levels were comparable between the groups. These results demonstrate that patients with type 2 or gestational diabetes can maintain the desired level of control using oral agents, thereby lowering diabetes-related risks.
To date, no randomized study with an adequate sample size has addressed use of oral hypoglycemic agents during organogenesis. The likelihood of such a study being performed is very small, since most pregnancies are unplanned and we lack the ability to determine the lag time between conception and drug effect. Therefore, the clinical decision to give the drugs should be based on existing data rather than potentially unattainable information (TABLE 1).
TABLE 1
Selected trials using ‘new’-generation oral agents in pregnancy
| AUTHOR | YEAR | NO. OF PATIENTS | DESIGN | DRUG | OUTCOME |
|---|---|---|---|---|---|
| Notelovitz9 | 1971 | 4×52 | Randomized | Tolbutamide | No significant differences in perinatal mortality and congenital anomalies for blood glucose <150 mg/dL |
| Coetzee and Jackson12 | 1980 | 148 | Retrospective | Glibenclamide (glyburide) | Reduced perinatal mortality |
| Coetzee and Jackson11 | 1984 | 171 | Retrospective | Metformin | Drug was deemed safe in first trimester and later pregnancy, if blood glucose control is good |
| Coetzee and Jackson26 | 1986 | 126 | Retrospective | Metformin | Reduced perinatal mortality |
| Langer et al3 | 2000 | 404 | Randomized | Glyburide | No significant differences between the glyburide and insulin groups in large-for-gestational-age and macrosomic infants, hypoglycemia, neonatal intensive care unit admissions, and fetal anomalies |
| Pendsey27 | 2002 | 46 | Randomized | Repaglinide | Same success rate as with insulin therapy |
Success rates of oral agents
Glyburide. In the prospective randomized trial mentioned earlier, we found glyburide to be as effective as insulin, since 82% of the patients receiving glyburide and 88% of those receiving insulin achieved targeted levels of glucose control.3 In the Notelovitz study,9 80% of subjects treated with oral agents or diet maintained blood glucose levels below 150 mg/dL, while only 38% of the insulin-treated patients were able to achieve this goal, probably due to poor compliance. In yet another study, a success rate of 83% was found in glyburide-treated patients, who also claimed complete satisfaction with the mode of therapy.16
Success with oral agents is not universal, however. For example, Kitzmiller17 reported that among 73 women refusing insulin therapy who were assigned to receive glyburide, approximately 47% failed to achieve the targeted glycemic goals after 1 to 9 weeks of treatment. And in a US study of nongravid patients with type 2 diabetes, 62% of those treated with oral therapy failed to achieve the American Diabetes Association hemoglobin A1c goal of less than 7%. However, 73% of the patients treated with insulin also failed to achieve this threshold.18 The conclusion: Glyburide can be as effective as insulin.
Because diminished insulin secretion and sensitivity characterize both gestational and type 2 diabetes, oral hypoglycemic agents that address one or both of these abnormalities would seem to have the greatest potential efficacy. Therapy can consist of a single drug or a combination of oral hypoglycemic and antihyperglycemic agents acting on different abnormalities. Oral administration of these agents offers greater patient acceptance and compliance.
Sulfonylureas. First-generation sulfonylurea drugs, which included tolbutamide and chlorpropamide, were replaced by second-generation agents such as glyburide and glipizide.
Meglitinides. Oral insulin secretagogues were approved for clinical use in the late 1990s. Among this group, repaglinide has gained acceptance as a fast-acting, premeal therapy to limit postprandial hyperglycemia.1
Biguanides. Phenformin was withdrawn from the American market in 1977 because of the side effect of lactic acidosis. In 1995, metformin was approved for use in the United States.1
Thiazolidinediones. Troglitazone, the first agent in this group, was reported to have a high rate of hepatic toxicity and was withdrawn from the market in 2000. Newer agents in this class such as rosiglitazone and pioglitazone are widely used in clinical practice, without reported hepatic toxicity.1
Alpha-glucosidase inhibitors. Acarbose reduces intestinal absorption of starch and glucose. It has excellent potential for use in pregnancy without risk of adverse fetal exposure.1
REFERENCE
1. Hardmons JG, Limbird LE, eds. Goodman and Gilman’s “The Pharmacologic Basis of Therapeutics.” 9th ed. New York: McGraw-Hill; 1996;1712-1792.
The varying success rates are not surprising. Rather, they reflect varying quality of care and patient education, as well as different patient populations, compliance levels, and cultural preferences.
Metformin. Coetzee et al12,13 studied the effect of metformin as single or combination therapy in pregnancy, demonstrating a significant mean decline in plasma glucose concentrations. In one study, the failure of metformin to achieve the targeted level of glycemic control was 53.8% in women with established diabetes and 28.6% in women with gestational diabetes.13
Apart from a high incidence of neonatal jaundice requiring phototherapy, infant morbidity in the metformin group was low. The rates of large-for-gestational-age infants were comparable in the metformin-treated and insulin-treated groups (20%). The 3 fetal anomalies in this study involved women in the metformin group who initiated therapy in the third trimester.
Another study by Coetzee et al19 involved patients treated with dietary therapy alone, metformin or glibenclamide (glyburide) alone, or, when that failed, a combination of diet, metformin, and glibenclamide. Insulin was given when diet and oral therapy failed to achieve glycemic control. The incidence of large-for-gestational-age neonates was 15% in the metformin group, 27% among the glibenclamide users, 33% for combined therapy, and 41% for insulin. These varying rates can be explained by differences in disease severity. Still, it is notable that subjects treated with metformin had the lowest rate.
Metformin is a popular drug in the treatment of polycystic ovary syndrome (PCOS). When these women become pregnant, the fetus is exposed to the drug during the first trimester. Thus, the physician is faced with 2 dilemmas: Should patients on metformin conceive while on the drug? When they do conceive, should the drug be halted during pregnancy?
In a study by Glueck et al,20 women with PCOS received metformin to reduce the occurrence of gestational diabetes. Researchers found no evidence that the drug was teratogenic. Moreover, metformin reduced the likelihood of first-trimester abortion by a factor of 10.
In addition, use of the drug in the preconception period reduced the incidence of gestational diabetes from 31% to 3%—a rate comparable to that found in the general population. No major fetal malformations or fetal hypoglycemic episodes occurred in the 34 live births, thus supporting Coetzee’s findings.
However, in a study of 118 women with preexisting diabetes, Hellmuth et al21 found an incidence of preeclampsia of 32% in women treated with metformin, compared with 7% in the sulfonylurea group. Perinatal mortality was 11.6% and 1.3%, respectively.
The findings of this study were not replicated by other researchers. This can be partially explained by the relatively small number of patients in each arm of the study (metformin, insulin, diet, and sulfonylurea). The data also suggest that these patients were not maintaining optimal glucose control, since similar rates of macrosomia (35%) were found in all treatment groups.
In a study of women with PCOS, metformin therapy decreased the rate of early pregnancy loss to 11%, compared with a rate of 58% among untreated women.22
Although recent trials showed no adverse effect of metformin in terms of anomalies, no current study has evaluated pregnancy outcomes when patients were treated with the drug throughout gestation. Metformin and many other hypoglycemic and antihyperglycemic agents may, in the future, offer alternatives to glyburide with comparable or greater efficacy. However, current research has not provided the evidence for their safe use in pregnancy. Thus, glyburide is the only drug that can be safely recommended at this time (TABLE 2).
TABLE 2
Safety profile of oral hypoglycemic agents in pregnancy28,29
| DRUG | CLASS | FDA PREGNANCY CATEGORY | SAFETY PROFILE |
|---|---|---|---|
| Tolbutamide | Sulfonylurea | C | Risk cannot be ruled out |
| Glyburide | Sulfonylurea | B | No evidence of risk in humans |
| Metformin | Biguanide | B | No evidence of risk in humans |
| Repaglinide | Meglitinide | C | Risk cannot be ruled out |
Clinical management
The different oral hypoglycemic and antihyperglycemic agents have varying mechanisms of action. When properly selected, these drugs offer a more physiologic approach to the treatment of gestational and type 2 diabetes. Thus, several questions should be addressed when contemplating the use of insulin secretagogues or antihyperglycemic agents in pregnancy:
- Can glycemic control be achieved using the optimal dose?
- Can serious postprandial and fasting hypoglycemia be minimized in comparison with insulin therapy?
- Are there maternal or fetal side effects that mitigate the beneficial effects?
The data suggest that glyburide and possibly metformin can be safely and effectively used to manage gestational diabetes (TABLE 3). Medical therapy with oral agents should be reserved for patients in whom diet therapy fails (ie, those with fasting plasma glucose levels above 95 mg/dL or postprandial levels above 120 mg/dL) (FIGURE) or who are not appropriate candidates for diet therapy alone. For optimal results with oral agents, women must adhere to a diabetic diet and maintain the targeted level of glycemic control; compliance to therapy also is important.
Even on oral therapy, a small number of women do not attain desired levels of glucose control. For these patients, combination therapy (eg, insulin secretagogues with antihyperglycemic agents that act to improve insulin sensitivity) or insulin therapy should be substituted (TABLE 3). This approach should prevent overtreatment and unnecessary inconvenience for the patient.23-25
FIGURE Medical therapy decision path
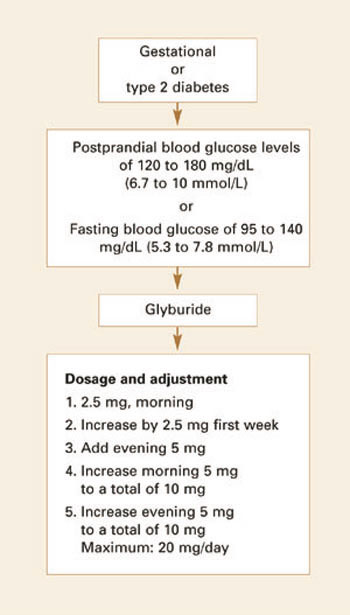
TABLE 3
Treatment plan for gestational and type 2 diabetes
| STAGE OF THERAPY | INDICATIONS | DECREASE IN HBA1C |
|---|---|---|
| Medical nutrition |
| ~1% |
| Oral therapy: glyburide and/or metformin |
| ~2% |
| Insulin |
| ≥4% |
| HbA1c = glycosylated hemoglobin A1c | ||
Dr. Langer reports no financial relationship with any companies whose products are mentioned in this article.
1. Towner D, Kjos SL, Montoro MM, Xian A, Mestman JH, Buchanan TA. Congenital malformations in pregnancies complicated by NIDDM. Diabetes Care. 1995;18:1446-1451.
2. Langer O, Conway D, Berkus M, Xenakis EMJ. There is no association between hypoglycemic use and fetal anomalies. Am J Obstet Gynecol. 1999;180(Abst):S38.-
3. Langer O, Conway DL, Berkus MD, Xenakis EMJ, Gonzales O. A comparison of glyburide vs. insulin in women with gestational diabetes mellitus. N Engl J Med. 2000;343:1134-1138.
4. Turner RC, Cull CA, Fright V. Glycemic control with diet, sulfonylurea, metformin, or insulin in patients with type 2 diabetes mellitus: progressive requirement for multiple therapies. JAMA. 1999;281:2005-2012.
5. Lebovitz HE. Insulin secretagogues: old and new. Diabetes Review. 1999;7:139-153.
6. Kjos SL, Buchanan TA, Greenspoon JS, Montoro M, Berstein GS, Mestman JH. Gestational diabetes mellitus: the prevalence of glucose intolerance and diabetes mellitus in the first two months postpartum. Am J Obstet Gynecol. 1990;163:93-98.
7. Langer O, Rodriguez DA, Xenakis EMJ. Intensified vs. conventional management of gestational diabetes. Am J Obstet Gynecol. 1994;170:1036-1047.
8. Piacquadio K, Hollingsworth DR, Murphy H. Effects of in-utero exposure to oral hypoglycemic drugs. Lancet. 1991;338:866-869.
9. Notelovitz M. Sulfonylurea therapy in the treatment of the pregnant diabetic. S Afr Med J. 1971;45:226-229.
10. Sutherland HW, Bewsher PD, Cormack JD. Effect of moderate dosage of chlorpropamide in pregnancy on fetal outcome. Arch Dis Child. 1974;49:283-291.
11. Coetzee EJ, Jackson WPU. Oral hypoglycemics in the first trimester and fetal outcome. S Afr Med J. 1984;65:635-637.
12. Coetzee EJ, Jackson WPU. Pregnancy in established non-insulin-dependent diabetics. A five-and-a-half year study at Groote Schuur Hospital. S Afr Med J. 1980;61:795-802.
13. Coetzee EJ, Jackson WPU. Metformin in management of pregnant insulin-independent diabetics. Diabetologia. 1979;16:241-245.
14. Kemball ML, McIvert C, Milner RDG, Nourses CH, Schiff D, Tiernan JR. Neonatal hypoglycemia in infants of diabetic mothers given sulphonylurea drugs in pregnancy. Arch Dis Child. 1970;45:696-701.
15. Zucker P, Simon G. Prolonged symptomatic neonatal hypoglycemia associated with maternal chlorpropamide therapy. Pediatrics. 1968;42:824-825.
16. Chmait R, Dinise T, Daneshmand S, Kim M, Moore T. Prospective cohort study to establish predictors of glyburide success in gestational diabetes mellitus. Am J Obstet Gynecol. 2001;185(6)(Abst).-
17. Kitzmiller J. Limited efficacy of glyburide for glycemic control. Am J Obstet Gynecol. 2001;185(6)(Abst).-
18. Harris MI, Eastman RC, Cowie CC, Flegal KM, Eberhardt MS. Racial and ethnic differences in glycemic control of adults with type 2 diabetes. Diabetes Care. 1999;22:403-408.
19. Coetzee EJ, Jackson WPU. Diabetes newly diagnosed in pregnancy: a 4-year study at Groote Schuur Hospital. S Afr Med J. 1979;56:467-475.
20. Glueck CJ, Wang P, Kobayashi S. Metformin therapy throughout pregnancy reduces the development of gestational diabetes in women with polycystic ovary syndrome. Fertil Steril. 2002;77:520-525.
21. Hellmuth E, Damm P, Molsted-Pedersen L. Oral hypoglycemic agents in 118 diabetic pregnancies. Diabetic Med. 2000;17:507-511.
22. Jakubowicz DJ, Iuorno MJ, Jakubowicz S. Effects of metformin on early pregnancy loss in the polycystic ovary syndrome. J Clin Endocrinol Metab. 2002;87:524-529.
23. Langer O. When diet fails: insulin and oral hypoglycemic agents as alternatives for the management of gestational diabetes. J Matern Fetal Neonatal Med. 2002;11:1-8.
24. Langer O. Insulin and other treatment alternatives in gestational diabetes mellitus. Prenatal Neonatal Med. 1998;3:542-549.
25. Langer O. Oral hypoglycemic agents in pregnancy: their time has come. J Matern Fetal Neonatal Med. 2002;12:376-383.
26. Coetzee EJ, Jackson WPU. The management of non-insulin dependent diabetes during pregnancy. Diabetes Res Clin Practice. 1986;1:281-287.
27. Pendsey. Insulin vs glyburide therapy in gestational diabetes. Proceedings of the annual meeting of the International Diabetes Federation, Barcelona, Spain; 2001.
28. Drug Facts and Comparisons 2003. St. Louis, Mo: Facts and Comparisons; 2003.
29. Physicians Desk Reference 2003. Montvale, NJ: Thompson; 2003.
- Well-designed studies have found no association between oral hypoglycemic agents and congenital malformations. Data suggest that glyburide and possibly metformin are safe and effective for gestational diabetes.
- Reserve medical therapy with oral agents for patients whose fasting plasma glucose levels remain above 95 mg/dL (or postprandial levels above 120 mg/dL) despite diet therapy, and for those who are not appropriate candidates for diet therapy alone.
- Substitute combination or insulin therapy for oral therapy if desired levels of glucose control are not achieved.
Although use of oral hypoglycemic and antihyperglycemic agents in pregnancy has long been thought to increase the risk of fetal anomalies, 2 trials within the past decade indicate otherwise. In those trials, blood glucose levels—rather than the drugs themselves—were responsible for the greater rate of anomalies.1,2
As a result, oral hypoglycemic agents are gaining recognition as a safe and effective alternative to insulin when diet alone fails to optimize the glycemic profile in gestational diabetes. Sulfonylureas are the only oral agents that have been studied in randomized, controlled trials in women with gestational diabetes,3 but other drugs may have an even greater therapeutic effect. Indeed, use of these other agents for type 2 diabetes has become the standard of care for the nongravid patient.4,5 Only recently has their use in pregnancy become arguable in US scientific forums.
Ninety percent of gravidas with diabetes—the most common medical complication of pregnancy—have gestational diabetes, and a significant number (20% to 50%) develop type 2 diabetes within 10 years.6 Both gestational and type 2 diabetes are characterized by peripheral insulin resistance, decreased insulin secretion (declining betacell function), and impaired regulation of hepatic glucose, each of which represents a different point in the continuum of deteriorating glucose tolerance.
Intensified therapy can maximize pregnancy outcome by decreasing the rates of macrosomia, metabolic and respiratory complications, shoulder dystocia, neonatal intensive care admission, and other complications to rates found in the general population. This treatment approach requires self-monitoring of blood glucose several times daily using a memory reflectance meter, adherence to proper criteria when initiating glyburide or insulin therapy (ie, fasting plasma glucose <90 mg/dL), and achievement of targeted glycemic control.7
Here, a specific treatment plan is offered along with a review of the evidence on use of oral agents in pregnancy. In addition, earlier interpretations that may have distorted the overall picture are discussed.
Studies of oral hypoglycemics and fetal anomalies
Early case reports and small-scale studies suggested an association between oral hypoglycemic agents and congenital anomalies. This anecdotal evidence was even translated into guidelines by the American College of Obstetricians and Gynecologists and the American Diabetes Association, among others. Unfortunately, these guidelines were based largely on a retrospective study involving 20 women with type 2 diabetes—all with glycosylated hemoglobin A1c concentrations exceeding 8%—in whom there was an increased rate of anomalies.8 However, the fact that maternal hyperglycemia existed prior to conception makes it impossible to determine whether the increased rate of anomalies was the result of medication or elevated glucose levels.
Other drawbacks of studies from this time: Few of the agents investigated are in common use today; most studies reported perinatal mortality and congenital anomalies, but failed to address neonatal morbidity; and many subjects had type 2 diabetes.9-15
In the past decade, 2 studies have suggested there is no association between oral hypoglycemic agents and congenital malformations. For example, no significant adverse effects associated with oral therapy were found in a study of 332 women with type 2 diabetes treated with diet therapy, exogenous insulin, or sulfonylurea compounds during the first 8 weeks of gestation.1 However, the level of glycemia and maternal age contributed significantly to the rate of anomalies.
Among the factors that determine the placental transfer capability of a drug are molecular weight, pKa, lipid solubility, placental blood flow, blood protein binding, and elimination half-life.
In the early 1990s, my colleagues and I evaluated the potential of first-generation and second-generation sulfonylureas to cross the placenta, and found no significant transport of glyburide in the maternal-to-fetal and fetal-to-maternal directions.1 Even increasing the glyburide concentration to 100 times the therapeutic level did not alter transport noticeably. Glyburide remained undetected when cord blood was analyzed using high-performance lipid chromatography with appropriate gradient concentration between the maternal and fetal sites.2 Moreover, at least 99.8% of the glyburide was bound to protein. Thus, glyburide was neither metabolized nor appropriated by the placenta.
In a second series of studies, we found that second-generation oral hypoglycemic agents—especially glyburide—did not significantly cross diabetic and nondiabetic placentae.3,4 Fetal concentrations reached no more than 1% to 2% of maternal concentrations. Glipizide crossed the placenta in small amounts that were significantly higher than glyburide. Tolbutamide diffused across the placenta most freely.
REFERENCES
1. Elliot B, Langer O, Schenker S, Jonhson RF. Insignificant transfer of glyburide occurs across the human placenta. Am J Obstet Gynecol. 1991;165:807-812.
2. Langer O. Oral hypoglycemic agents and the pregnant diabetic: “from bench to bedside.” Semin Perinatol. 2002;26:215-224.
3. Elliot B, Schenker S, Langer O, Johnson R, Prihoda T. Comparative placental transport of oral hypoglycemic agents. A model of human placental drug transfer. Am J Obstet Gynecol. 1994;171:653-660.
4. Elliot B, Langer O, Schussling F. A model of human placental drug transfer. Am J Obstet Gynecol. 1997;176:527-530.
We reached similar conclusions in a retrospective analysis of 850 women with type 2 diabetes who were exposed to oral hypoglycemic agents, insulin, or diet therapy prior to and during the first trimester of pregnancy.2 Again, it was blood glucose and not the mode of therapy that had the net effect on the rate of anomalies.
In a randomized study in 1971, Notelovitz et al9 compared the efficacies of tolbutamide, chlorpropamide, diet, and insulin in a randomized trial. When glycemic control was good (ie, blood glucose less than 150 mg/dL), there were no significant differences among the groups in perinatal mortality and congenital anomalies.
In a prospective, randomized trial, we also compared the efficacy of glyburide and insulin in 404 women with singleton pregnancies, and found no significant differences in maternal hypoglycemic episodes, preeclampsia, rate of cesarean section—or number of patients achieving the desired level of control.3 As for the neonates, no significant differences were found in the rate of macrosomia; large-for-gestational-age infants; metabolic, respiratory, and hematologic complications; and congenital anomalies.
Interestingly, no glyburide was detected in the arterial cord serum of any infant in the glyburide group, even though fetal insulin levels were comparable between the groups. These results demonstrate that patients with type 2 or gestational diabetes can maintain the desired level of control using oral agents, thereby lowering diabetes-related risks.
To date, no randomized study with an adequate sample size has addressed use of oral hypoglycemic agents during organogenesis. The likelihood of such a study being performed is very small, since most pregnancies are unplanned and we lack the ability to determine the lag time between conception and drug effect. Therefore, the clinical decision to give the drugs should be based on existing data rather than potentially unattainable information (TABLE 1).
TABLE 1
Selected trials using ‘new’-generation oral agents in pregnancy
| AUTHOR | YEAR | NO. OF PATIENTS | DESIGN | DRUG | OUTCOME |
|---|---|---|---|---|---|
| Notelovitz9 | 1971 | 4×52 | Randomized | Tolbutamide | No significant differences in perinatal mortality and congenital anomalies for blood glucose <150 mg/dL |
| Coetzee and Jackson12 | 1980 | 148 | Retrospective | Glibenclamide (glyburide) | Reduced perinatal mortality |
| Coetzee and Jackson11 | 1984 | 171 | Retrospective | Metformin | Drug was deemed safe in first trimester and later pregnancy, if blood glucose control is good |
| Coetzee and Jackson26 | 1986 | 126 | Retrospective | Metformin | Reduced perinatal mortality |
| Langer et al3 | 2000 | 404 | Randomized | Glyburide | No significant differences between the glyburide and insulin groups in large-for-gestational-age and macrosomic infants, hypoglycemia, neonatal intensive care unit admissions, and fetal anomalies |
| Pendsey27 | 2002 | 46 | Randomized | Repaglinide | Same success rate as with insulin therapy |
Success rates of oral agents
Glyburide. In the prospective randomized trial mentioned earlier, we found glyburide to be as effective as insulin, since 82% of the patients receiving glyburide and 88% of those receiving insulin achieved targeted levels of glucose control.3 In the Notelovitz study,9 80% of subjects treated with oral agents or diet maintained blood glucose levels below 150 mg/dL, while only 38% of the insulin-treated patients were able to achieve this goal, probably due to poor compliance. In yet another study, a success rate of 83% was found in glyburide-treated patients, who also claimed complete satisfaction with the mode of therapy.16
Success with oral agents is not universal, however. For example, Kitzmiller17 reported that among 73 women refusing insulin therapy who were assigned to receive glyburide, approximately 47% failed to achieve the targeted glycemic goals after 1 to 9 weeks of treatment. And in a US study of nongravid patients with type 2 diabetes, 62% of those treated with oral therapy failed to achieve the American Diabetes Association hemoglobin A1c goal of less than 7%. However, 73% of the patients treated with insulin also failed to achieve this threshold.18 The conclusion: Glyburide can be as effective as insulin.
Because diminished insulin secretion and sensitivity characterize both gestational and type 2 diabetes, oral hypoglycemic agents that address one or both of these abnormalities would seem to have the greatest potential efficacy. Therapy can consist of a single drug or a combination of oral hypoglycemic and antihyperglycemic agents acting on different abnormalities. Oral administration of these agents offers greater patient acceptance and compliance.
Sulfonylureas. First-generation sulfonylurea drugs, which included tolbutamide and chlorpropamide, were replaced by second-generation agents such as glyburide and glipizide.
Meglitinides. Oral insulin secretagogues were approved for clinical use in the late 1990s. Among this group, repaglinide has gained acceptance as a fast-acting, premeal therapy to limit postprandial hyperglycemia.1
Biguanides. Phenformin was withdrawn from the American market in 1977 because of the side effect of lactic acidosis. In 1995, metformin was approved for use in the United States.1
Thiazolidinediones. Troglitazone, the first agent in this group, was reported to have a high rate of hepatic toxicity and was withdrawn from the market in 2000. Newer agents in this class such as rosiglitazone and pioglitazone are widely used in clinical practice, without reported hepatic toxicity.1
Alpha-glucosidase inhibitors. Acarbose reduces intestinal absorption of starch and glucose. It has excellent potential for use in pregnancy without risk of adverse fetal exposure.1
REFERENCE
1. Hardmons JG, Limbird LE, eds. Goodman and Gilman’s “The Pharmacologic Basis of Therapeutics.” 9th ed. New York: McGraw-Hill; 1996;1712-1792.
The varying success rates are not surprising. Rather, they reflect varying quality of care and patient education, as well as different patient populations, compliance levels, and cultural preferences.
Metformin. Coetzee et al12,13 studied the effect of metformin as single or combination therapy in pregnancy, demonstrating a significant mean decline in plasma glucose concentrations. In one study, the failure of metformin to achieve the targeted level of glycemic control was 53.8% in women with established diabetes and 28.6% in women with gestational diabetes.13
Apart from a high incidence of neonatal jaundice requiring phototherapy, infant morbidity in the metformin group was low. The rates of large-for-gestational-age infants were comparable in the metformin-treated and insulin-treated groups (20%). The 3 fetal anomalies in this study involved women in the metformin group who initiated therapy in the third trimester.
Another study by Coetzee et al19 involved patients treated with dietary therapy alone, metformin or glibenclamide (glyburide) alone, or, when that failed, a combination of diet, metformin, and glibenclamide. Insulin was given when diet and oral therapy failed to achieve glycemic control. The incidence of large-for-gestational-age neonates was 15% in the metformin group, 27% among the glibenclamide users, 33% for combined therapy, and 41% for insulin. These varying rates can be explained by differences in disease severity. Still, it is notable that subjects treated with metformin had the lowest rate.
Metformin is a popular drug in the treatment of polycystic ovary syndrome (PCOS). When these women become pregnant, the fetus is exposed to the drug during the first trimester. Thus, the physician is faced with 2 dilemmas: Should patients on metformin conceive while on the drug? When they do conceive, should the drug be halted during pregnancy?
In a study by Glueck et al,20 women with PCOS received metformin to reduce the occurrence of gestational diabetes. Researchers found no evidence that the drug was teratogenic. Moreover, metformin reduced the likelihood of first-trimester abortion by a factor of 10.
In addition, use of the drug in the preconception period reduced the incidence of gestational diabetes from 31% to 3%—a rate comparable to that found in the general population. No major fetal malformations or fetal hypoglycemic episodes occurred in the 34 live births, thus supporting Coetzee’s findings.
However, in a study of 118 women with preexisting diabetes, Hellmuth et al21 found an incidence of preeclampsia of 32% in women treated with metformin, compared with 7% in the sulfonylurea group. Perinatal mortality was 11.6% and 1.3%, respectively.
The findings of this study were not replicated by other researchers. This can be partially explained by the relatively small number of patients in each arm of the study (metformin, insulin, diet, and sulfonylurea). The data also suggest that these patients were not maintaining optimal glucose control, since similar rates of macrosomia (35%) were found in all treatment groups.
In a study of women with PCOS, metformin therapy decreased the rate of early pregnancy loss to 11%, compared with a rate of 58% among untreated women.22
Although recent trials showed no adverse effect of metformin in terms of anomalies, no current study has evaluated pregnancy outcomes when patients were treated with the drug throughout gestation. Metformin and many other hypoglycemic and antihyperglycemic agents may, in the future, offer alternatives to glyburide with comparable or greater efficacy. However, current research has not provided the evidence for their safe use in pregnancy. Thus, glyburide is the only drug that can be safely recommended at this time (TABLE 2).
TABLE 2
Safety profile of oral hypoglycemic agents in pregnancy28,29
| DRUG | CLASS | FDA PREGNANCY CATEGORY | SAFETY PROFILE |
|---|---|---|---|
| Tolbutamide | Sulfonylurea | C | Risk cannot be ruled out |
| Glyburide | Sulfonylurea | B | No evidence of risk in humans |
| Metformin | Biguanide | B | No evidence of risk in humans |
| Repaglinide | Meglitinide | C | Risk cannot be ruled out |
Clinical management
The different oral hypoglycemic and antihyperglycemic agents have varying mechanisms of action. When properly selected, these drugs offer a more physiologic approach to the treatment of gestational and type 2 diabetes. Thus, several questions should be addressed when contemplating the use of insulin secretagogues or antihyperglycemic agents in pregnancy:
- Can glycemic control be achieved using the optimal dose?
- Can serious postprandial and fasting hypoglycemia be minimized in comparison with insulin therapy?
- Are there maternal or fetal side effects that mitigate the beneficial effects?
The data suggest that glyburide and possibly metformin can be safely and effectively used to manage gestational diabetes (TABLE 3). Medical therapy with oral agents should be reserved for patients in whom diet therapy fails (ie, those with fasting plasma glucose levels above 95 mg/dL or postprandial levels above 120 mg/dL) (FIGURE) or who are not appropriate candidates for diet therapy alone. For optimal results with oral agents, women must adhere to a diabetic diet and maintain the targeted level of glycemic control; compliance to therapy also is important.
Even on oral therapy, a small number of women do not attain desired levels of glucose control. For these patients, combination therapy (eg, insulin secretagogues with antihyperglycemic agents that act to improve insulin sensitivity) or insulin therapy should be substituted (TABLE 3). This approach should prevent overtreatment and unnecessary inconvenience for the patient.23-25
FIGURE Medical therapy decision path
TABLE 3
Treatment plan for gestational and type 2 diabetes
| STAGE OF THERAPY | INDICATIONS | DECREASE IN HBA1C |
|---|---|---|
| Medical nutrition |
| ~1% |
| Oral therapy: glyburide and/or metformin |
| ~2% |
| Insulin |
| ≥4% |
| HbA1c = glycosylated hemoglobin A1c | ||
Dr. Langer reports no financial relationship with any companies whose products are mentioned in this article.
- Well-designed studies have found no association between oral hypoglycemic agents and congenital malformations. Data suggest that glyburide and possibly metformin are safe and effective for gestational diabetes.
- Reserve medical therapy with oral agents for patients whose fasting plasma glucose levels remain above 95 mg/dL (or postprandial levels above 120 mg/dL) despite diet therapy, and for those who are not appropriate candidates for diet therapy alone.
- Substitute combination or insulin therapy for oral therapy if desired levels of glucose control are not achieved.
Although use of oral hypoglycemic and antihyperglycemic agents in pregnancy has long been thought to increase the risk of fetal anomalies, 2 trials within the past decade indicate otherwise. In those trials, blood glucose levels—rather than the drugs themselves—were responsible for the greater rate of anomalies.1,2
As a result, oral hypoglycemic agents are gaining recognition as a safe and effective alternative to insulin when diet alone fails to optimize the glycemic profile in gestational diabetes. Sulfonylureas are the only oral agents that have been studied in randomized, controlled trials in women with gestational diabetes,3 but other drugs may have an even greater therapeutic effect. Indeed, use of these other agents for type 2 diabetes has become the standard of care for the nongravid patient.4,5 Only recently has their use in pregnancy become arguable in US scientific forums.
Ninety percent of gravidas with diabetes—the most common medical complication of pregnancy—have gestational diabetes, and a significant number (20% to 50%) develop type 2 diabetes within 10 years.6 Both gestational and type 2 diabetes are characterized by peripheral insulin resistance, decreased insulin secretion (declining betacell function), and impaired regulation of hepatic glucose, each of which represents a different point in the continuum of deteriorating glucose tolerance.
Intensified therapy can maximize pregnancy outcome by decreasing the rates of macrosomia, metabolic and respiratory complications, shoulder dystocia, neonatal intensive care admission, and other complications to rates found in the general population. This treatment approach requires self-monitoring of blood glucose several times daily using a memory reflectance meter, adherence to proper criteria when initiating glyburide or insulin therapy (ie, fasting plasma glucose <90 mg/dL), and achievement of targeted glycemic control.7
Here, a specific treatment plan is offered along with a review of the evidence on use of oral agents in pregnancy. In addition, earlier interpretations that may have distorted the overall picture are discussed.
Studies of oral hypoglycemics and fetal anomalies
Early case reports and small-scale studies suggested an association between oral hypoglycemic agents and congenital anomalies. This anecdotal evidence was even translated into guidelines by the American College of Obstetricians and Gynecologists and the American Diabetes Association, among others. Unfortunately, these guidelines were based largely on a retrospective study involving 20 women with type 2 diabetes—all with glycosylated hemoglobin A1c concentrations exceeding 8%—in whom there was an increased rate of anomalies.8 However, the fact that maternal hyperglycemia existed prior to conception makes it impossible to determine whether the increased rate of anomalies was the result of medication or elevated glucose levels.
Other drawbacks of studies from this time: Few of the agents investigated are in common use today; most studies reported perinatal mortality and congenital anomalies, but failed to address neonatal morbidity; and many subjects had type 2 diabetes.9-15
In the past decade, 2 studies have suggested there is no association between oral hypoglycemic agents and congenital malformations. For example, no significant adverse effects associated with oral therapy were found in a study of 332 women with type 2 diabetes treated with diet therapy, exogenous insulin, or sulfonylurea compounds during the first 8 weeks of gestation.1 However, the level of glycemia and maternal age contributed significantly to the rate of anomalies.
Among the factors that determine the placental transfer capability of a drug are molecular weight, pKa, lipid solubility, placental blood flow, blood protein binding, and elimination half-life.
In the early 1990s, my colleagues and I evaluated the potential of first-generation and second-generation sulfonylureas to cross the placenta, and found no significant transport of glyburide in the maternal-to-fetal and fetal-to-maternal directions.1 Even increasing the glyburide concentration to 100 times the therapeutic level did not alter transport noticeably. Glyburide remained undetected when cord blood was analyzed using high-performance lipid chromatography with appropriate gradient concentration between the maternal and fetal sites.2 Moreover, at least 99.8% of the glyburide was bound to protein. Thus, glyburide was neither metabolized nor appropriated by the placenta.
In a second series of studies, we found that second-generation oral hypoglycemic agents—especially glyburide—did not significantly cross diabetic and nondiabetic placentae.3,4 Fetal concentrations reached no more than 1% to 2% of maternal concentrations. Glipizide crossed the placenta in small amounts that were significantly higher than glyburide. Tolbutamide diffused across the placenta most freely.
REFERENCES
1. Elliot B, Langer O, Schenker S, Jonhson RF. Insignificant transfer of glyburide occurs across the human placenta. Am J Obstet Gynecol. 1991;165:807-812.
2. Langer O. Oral hypoglycemic agents and the pregnant diabetic: “from bench to bedside.” Semin Perinatol. 2002;26:215-224.
3. Elliot B, Schenker S, Langer O, Johnson R, Prihoda T. Comparative placental transport of oral hypoglycemic agents. A model of human placental drug transfer. Am J Obstet Gynecol. 1994;171:653-660.
4. Elliot B, Langer O, Schussling F. A model of human placental drug transfer. Am J Obstet Gynecol. 1997;176:527-530.
We reached similar conclusions in a retrospective analysis of 850 women with type 2 diabetes who were exposed to oral hypoglycemic agents, insulin, or diet therapy prior to and during the first trimester of pregnancy.2 Again, it was blood glucose and not the mode of therapy that had the net effect on the rate of anomalies.
In a randomized study in 1971, Notelovitz et al9 compared the efficacies of tolbutamide, chlorpropamide, diet, and insulin in a randomized trial. When glycemic control was good (ie, blood glucose less than 150 mg/dL), there were no significant differences among the groups in perinatal mortality and congenital anomalies.
In a prospective, randomized trial, we also compared the efficacy of glyburide and insulin in 404 women with singleton pregnancies, and found no significant differences in maternal hypoglycemic episodes, preeclampsia, rate of cesarean section—or number of patients achieving the desired level of control.3 As for the neonates, no significant differences were found in the rate of macrosomia; large-for-gestational-age infants; metabolic, respiratory, and hematologic complications; and congenital anomalies.
Interestingly, no glyburide was detected in the arterial cord serum of any infant in the glyburide group, even though fetal insulin levels were comparable between the groups. These results demonstrate that patients with type 2 or gestational diabetes can maintain the desired level of control using oral agents, thereby lowering diabetes-related risks.
To date, no randomized study with an adequate sample size has addressed use of oral hypoglycemic agents during organogenesis. The likelihood of such a study being performed is very small, since most pregnancies are unplanned and we lack the ability to determine the lag time between conception and drug effect. Therefore, the clinical decision to give the drugs should be based on existing data rather than potentially unattainable information (TABLE 1).
TABLE 1
Selected trials using ‘new’-generation oral agents in pregnancy
| AUTHOR | YEAR | NO. OF PATIENTS | DESIGN | DRUG | OUTCOME |
|---|---|---|---|---|---|
| Notelovitz9 | 1971 | 4×52 | Randomized | Tolbutamide | No significant differences in perinatal mortality and congenital anomalies for blood glucose <150 mg/dL |
| Coetzee and Jackson12 | 1980 | 148 | Retrospective | Glibenclamide (glyburide) | Reduced perinatal mortality |
| Coetzee and Jackson11 | 1984 | 171 | Retrospective | Metformin | Drug was deemed safe in first trimester and later pregnancy, if blood glucose control is good |
| Coetzee and Jackson26 | 1986 | 126 | Retrospective | Metformin | Reduced perinatal mortality |
| Langer et al3 | 2000 | 404 | Randomized | Glyburide | No significant differences between the glyburide and insulin groups in large-for-gestational-age and macrosomic infants, hypoglycemia, neonatal intensive care unit admissions, and fetal anomalies |
| Pendsey27 | 2002 | 46 | Randomized | Repaglinide | Same success rate as with insulin therapy |
Success rates of oral agents
Glyburide. In the prospective randomized trial mentioned earlier, we found glyburide to be as effective as insulin, since 82% of the patients receiving glyburide and 88% of those receiving insulin achieved targeted levels of glucose control.3 In the Notelovitz study,9 80% of subjects treated with oral agents or diet maintained blood glucose levels below 150 mg/dL, while only 38% of the insulin-treated patients were able to achieve this goal, probably due to poor compliance. In yet another study, a success rate of 83% was found in glyburide-treated patients, who also claimed complete satisfaction with the mode of therapy.16
Success with oral agents is not universal, however. For example, Kitzmiller17 reported that among 73 women refusing insulin therapy who were assigned to receive glyburide, approximately 47% failed to achieve the targeted glycemic goals after 1 to 9 weeks of treatment. And in a US study of nongravid patients with type 2 diabetes, 62% of those treated with oral therapy failed to achieve the American Diabetes Association hemoglobin A1c goal of less than 7%. However, 73% of the patients treated with insulin also failed to achieve this threshold.18 The conclusion: Glyburide can be as effective as insulin.
Because diminished insulin secretion and sensitivity characterize both gestational and type 2 diabetes, oral hypoglycemic agents that address one or both of these abnormalities would seem to have the greatest potential efficacy. Therapy can consist of a single drug or a combination of oral hypoglycemic and antihyperglycemic agents acting on different abnormalities. Oral administration of these agents offers greater patient acceptance and compliance.
Sulfonylureas. First-generation sulfonylurea drugs, which included tolbutamide and chlorpropamide, were replaced by second-generation agents such as glyburide and glipizide.
Meglitinides. Oral insulin secretagogues were approved for clinical use in the late 1990s. Among this group, repaglinide has gained acceptance as a fast-acting, premeal therapy to limit postprandial hyperglycemia.1
Biguanides. Phenformin was withdrawn from the American market in 1977 because of the side effect of lactic acidosis. In 1995, metformin was approved for use in the United States.1
Thiazolidinediones. Troglitazone, the first agent in this group, was reported to have a high rate of hepatic toxicity and was withdrawn from the market in 2000. Newer agents in this class such as rosiglitazone and pioglitazone are widely used in clinical practice, without reported hepatic toxicity.1
Alpha-glucosidase inhibitors. Acarbose reduces intestinal absorption of starch and glucose. It has excellent potential for use in pregnancy without risk of adverse fetal exposure.1
REFERENCE
1. Hardmons JG, Limbird LE, eds. Goodman and Gilman’s “The Pharmacologic Basis of Therapeutics.” 9th ed. New York: McGraw-Hill; 1996;1712-1792.
The varying success rates are not surprising. Rather, they reflect varying quality of care and patient education, as well as different patient populations, compliance levels, and cultural preferences.
Metformin. Coetzee et al12,13 studied the effect of metformin as single or combination therapy in pregnancy, demonstrating a significant mean decline in plasma glucose concentrations. In one study, the failure of metformin to achieve the targeted level of glycemic control was 53.8% in women with established diabetes and 28.6% in women with gestational diabetes.13
Apart from a high incidence of neonatal jaundice requiring phototherapy, infant morbidity in the metformin group was low. The rates of large-for-gestational-age infants were comparable in the metformin-treated and insulin-treated groups (20%). The 3 fetal anomalies in this study involved women in the metformin group who initiated therapy in the third trimester.
Another study by Coetzee et al19 involved patients treated with dietary therapy alone, metformin or glibenclamide (glyburide) alone, or, when that failed, a combination of diet, metformin, and glibenclamide. Insulin was given when diet and oral therapy failed to achieve glycemic control. The incidence of large-for-gestational-age neonates was 15% in the metformin group, 27% among the glibenclamide users, 33% for combined therapy, and 41% for insulin. These varying rates can be explained by differences in disease severity. Still, it is notable that subjects treated with metformin had the lowest rate.
Metformin is a popular drug in the treatment of polycystic ovary syndrome (PCOS). When these women become pregnant, the fetus is exposed to the drug during the first trimester. Thus, the physician is faced with 2 dilemmas: Should patients on metformin conceive while on the drug? When they do conceive, should the drug be halted during pregnancy?
In a study by Glueck et al,20 women with PCOS received metformin to reduce the occurrence of gestational diabetes. Researchers found no evidence that the drug was teratogenic. Moreover, metformin reduced the likelihood of first-trimester abortion by a factor of 10.
In addition, use of the drug in the preconception period reduced the incidence of gestational diabetes from 31% to 3%—a rate comparable to that found in the general population. No major fetal malformations or fetal hypoglycemic episodes occurred in the 34 live births, thus supporting Coetzee’s findings.
However, in a study of 118 women with preexisting diabetes, Hellmuth et al21 found an incidence of preeclampsia of 32% in women treated with metformin, compared with 7% in the sulfonylurea group. Perinatal mortality was 11.6% and 1.3%, respectively.
The findings of this study were not replicated by other researchers. This can be partially explained by the relatively small number of patients in each arm of the study (metformin, insulin, diet, and sulfonylurea). The data also suggest that these patients were not maintaining optimal glucose control, since similar rates of macrosomia (35%) were found in all treatment groups.
In a study of women with PCOS, metformin therapy decreased the rate of early pregnancy loss to 11%, compared with a rate of 58% among untreated women.22
Although recent trials showed no adverse effect of metformin in terms of anomalies, no current study has evaluated pregnancy outcomes when patients were treated with the drug throughout gestation. Metformin and many other hypoglycemic and antihyperglycemic agents may, in the future, offer alternatives to glyburide with comparable or greater efficacy. However, current research has not provided the evidence for their safe use in pregnancy. Thus, glyburide is the only drug that can be safely recommended at this time (TABLE 2).
TABLE 2
Safety profile of oral hypoglycemic agents in pregnancy28,29
| DRUG | CLASS | FDA PREGNANCY CATEGORY | SAFETY PROFILE |
|---|---|---|---|
| Tolbutamide | Sulfonylurea | C | Risk cannot be ruled out |
| Glyburide | Sulfonylurea | B | No evidence of risk in humans |
| Metformin | Biguanide | B | No evidence of risk in humans |
| Repaglinide | Meglitinide | C | Risk cannot be ruled out |
Clinical management
The different oral hypoglycemic and antihyperglycemic agents have varying mechanisms of action. When properly selected, these drugs offer a more physiologic approach to the treatment of gestational and type 2 diabetes. Thus, several questions should be addressed when contemplating the use of insulin secretagogues or antihyperglycemic agents in pregnancy:
- Can glycemic control be achieved using the optimal dose?
- Can serious postprandial and fasting hypoglycemia be minimized in comparison with insulin therapy?
- Are there maternal or fetal side effects that mitigate the beneficial effects?
The data suggest that glyburide and possibly metformin can be safely and effectively used to manage gestational diabetes (TABLE 3). Medical therapy with oral agents should be reserved for patients in whom diet therapy fails (ie, those with fasting plasma glucose levels above 95 mg/dL or postprandial levels above 120 mg/dL) (FIGURE) or who are not appropriate candidates for diet therapy alone. For optimal results with oral agents, women must adhere to a diabetic diet and maintain the targeted level of glycemic control; compliance to therapy also is important.
Even on oral therapy, a small number of women do not attain desired levels of glucose control. For these patients, combination therapy (eg, insulin secretagogues with antihyperglycemic agents that act to improve insulin sensitivity) or insulin therapy should be substituted (TABLE 3). This approach should prevent overtreatment and unnecessary inconvenience for the patient.23-25
FIGURE Medical therapy decision path
TABLE 3
Treatment plan for gestational and type 2 diabetes
| STAGE OF THERAPY | INDICATIONS | DECREASE IN HBA1C |
|---|---|---|
| Medical nutrition |
| ~1% |
| Oral therapy: glyburide and/or metformin |
| ~2% |
| Insulin |
| ≥4% |
| HbA1c = glycosylated hemoglobin A1c | ||
Dr. Langer reports no financial relationship with any companies whose products are mentioned in this article.
1. Towner D, Kjos SL, Montoro MM, Xian A, Mestman JH, Buchanan TA. Congenital malformations in pregnancies complicated by NIDDM. Diabetes Care. 1995;18:1446-1451.
2. Langer O, Conway D, Berkus M, Xenakis EMJ. There is no association between hypoglycemic use and fetal anomalies. Am J Obstet Gynecol. 1999;180(Abst):S38.-
3. Langer O, Conway DL, Berkus MD, Xenakis EMJ, Gonzales O. A comparison of glyburide vs. insulin in women with gestational diabetes mellitus. N Engl J Med. 2000;343:1134-1138.
4. Turner RC, Cull CA, Fright V. Glycemic control with diet, sulfonylurea, metformin, or insulin in patients with type 2 diabetes mellitus: progressive requirement for multiple therapies. JAMA. 1999;281:2005-2012.
5. Lebovitz HE. Insulin secretagogues: old and new. Diabetes Review. 1999;7:139-153.
6. Kjos SL, Buchanan TA, Greenspoon JS, Montoro M, Berstein GS, Mestman JH. Gestational diabetes mellitus: the prevalence of glucose intolerance and diabetes mellitus in the first two months postpartum. Am J Obstet Gynecol. 1990;163:93-98.
7. Langer O, Rodriguez DA, Xenakis EMJ. Intensified vs. conventional management of gestational diabetes. Am J Obstet Gynecol. 1994;170:1036-1047.
8. Piacquadio K, Hollingsworth DR, Murphy H. Effects of in-utero exposure to oral hypoglycemic drugs. Lancet. 1991;338:866-869.
9. Notelovitz M. Sulfonylurea therapy in the treatment of the pregnant diabetic. S Afr Med J. 1971;45:226-229.
10. Sutherland HW, Bewsher PD, Cormack JD. Effect of moderate dosage of chlorpropamide in pregnancy on fetal outcome. Arch Dis Child. 1974;49:283-291.
11. Coetzee EJ, Jackson WPU. Oral hypoglycemics in the first trimester and fetal outcome. S Afr Med J. 1984;65:635-637.
12. Coetzee EJ, Jackson WPU. Pregnancy in established non-insulin-dependent diabetics. A five-and-a-half year study at Groote Schuur Hospital. S Afr Med J. 1980;61:795-802.
13. Coetzee EJ, Jackson WPU. Metformin in management of pregnant insulin-independent diabetics. Diabetologia. 1979;16:241-245.
14. Kemball ML, McIvert C, Milner RDG, Nourses CH, Schiff D, Tiernan JR. Neonatal hypoglycemia in infants of diabetic mothers given sulphonylurea drugs in pregnancy. Arch Dis Child. 1970;45:696-701.
15. Zucker P, Simon G. Prolonged symptomatic neonatal hypoglycemia associated with maternal chlorpropamide therapy. Pediatrics. 1968;42:824-825.
16. Chmait R, Dinise T, Daneshmand S, Kim M, Moore T. Prospective cohort study to establish predictors of glyburide success in gestational diabetes mellitus. Am J Obstet Gynecol. 2001;185(6)(Abst).-
17. Kitzmiller J. Limited efficacy of glyburide for glycemic control. Am J Obstet Gynecol. 2001;185(6)(Abst).-
18. Harris MI, Eastman RC, Cowie CC, Flegal KM, Eberhardt MS. Racial and ethnic differences in glycemic control of adults with type 2 diabetes. Diabetes Care. 1999;22:403-408.
19. Coetzee EJ, Jackson WPU. Diabetes newly diagnosed in pregnancy: a 4-year study at Groote Schuur Hospital. S Afr Med J. 1979;56:467-475.
20. Glueck CJ, Wang P, Kobayashi S. Metformin therapy throughout pregnancy reduces the development of gestational diabetes in women with polycystic ovary syndrome. Fertil Steril. 2002;77:520-525.
21. Hellmuth E, Damm P, Molsted-Pedersen L. Oral hypoglycemic agents in 118 diabetic pregnancies. Diabetic Med. 2000;17:507-511.
22. Jakubowicz DJ, Iuorno MJ, Jakubowicz S. Effects of metformin on early pregnancy loss in the polycystic ovary syndrome. J Clin Endocrinol Metab. 2002;87:524-529.
23. Langer O. When diet fails: insulin and oral hypoglycemic agents as alternatives for the management of gestational diabetes. J Matern Fetal Neonatal Med. 2002;11:1-8.
24. Langer O. Insulin and other treatment alternatives in gestational diabetes mellitus. Prenatal Neonatal Med. 1998;3:542-549.
25. Langer O. Oral hypoglycemic agents in pregnancy: their time has come. J Matern Fetal Neonatal Med. 2002;12:376-383.
26. Coetzee EJ, Jackson WPU. The management of non-insulin dependent diabetes during pregnancy. Diabetes Res Clin Practice. 1986;1:281-287.
27. Pendsey. Insulin vs glyburide therapy in gestational diabetes. Proceedings of the annual meeting of the International Diabetes Federation, Barcelona, Spain; 2001.
28. Drug Facts and Comparisons 2003. St. Louis, Mo: Facts and Comparisons; 2003.
29. Physicians Desk Reference 2003. Montvale, NJ: Thompson; 2003.
1. Towner D, Kjos SL, Montoro MM, Xian A, Mestman JH, Buchanan TA. Congenital malformations in pregnancies complicated by NIDDM. Diabetes Care. 1995;18:1446-1451.
2. Langer O, Conway D, Berkus M, Xenakis EMJ. There is no association between hypoglycemic use and fetal anomalies. Am J Obstet Gynecol. 1999;180(Abst):S38.-
3. Langer O, Conway DL, Berkus MD, Xenakis EMJ, Gonzales O. A comparison of glyburide vs. insulin in women with gestational diabetes mellitus. N Engl J Med. 2000;343:1134-1138.
4. Turner RC, Cull CA, Fright V. Glycemic control with diet, sulfonylurea, metformin, or insulin in patients with type 2 diabetes mellitus: progressive requirement for multiple therapies. JAMA. 1999;281:2005-2012.
5. Lebovitz HE. Insulin secretagogues: old and new. Diabetes Review. 1999;7:139-153.
6. Kjos SL, Buchanan TA, Greenspoon JS, Montoro M, Berstein GS, Mestman JH. Gestational diabetes mellitus: the prevalence of glucose intolerance and diabetes mellitus in the first two months postpartum. Am J Obstet Gynecol. 1990;163:93-98.
7. Langer O, Rodriguez DA, Xenakis EMJ. Intensified vs. conventional management of gestational diabetes. Am J Obstet Gynecol. 1994;170:1036-1047.
8. Piacquadio K, Hollingsworth DR, Murphy H. Effects of in-utero exposure to oral hypoglycemic drugs. Lancet. 1991;338:866-869.
9. Notelovitz M. Sulfonylurea therapy in the treatment of the pregnant diabetic. S Afr Med J. 1971;45:226-229.
10. Sutherland HW, Bewsher PD, Cormack JD. Effect of moderate dosage of chlorpropamide in pregnancy on fetal outcome. Arch Dis Child. 1974;49:283-291.
11. Coetzee EJ, Jackson WPU. Oral hypoglycemics in the first trimester and fetal outcome. S Afr Med J. 1984;65:635-637.
12. Coetzee EJ, Jackson WPU. Pregnancy in established non-insulin-dependent diabetics. A five-and-a-half year study at Groote Schuur Hospital. S Afr Med J. 1980;61:795-802.
13. Coetzee EJ, Jackson WPU. Metformin in management of pregnant insulin-independent diabetics. Diabetologia. 1979;16:241-245.
14. Kemball ML, McIvert C, Milner RDG, Nourses CH, Schiff D, Tiernan JR. Neonatal hypoglycemia in infants of diabetic mothers given sulphonylurea drugs in pregnancy. Arch Dis Child. 1970;45:696-701.
15. Zucker P, Simon G. Prolonged symptomatic neonatal hypoglycemia associated with maternal chlorpropamide therapy. Pediatrics. 1968;42:824-825.
16. Chmait R, Dinise T, Daneshmand S, Kim M, Moore T. Prospective cohort study to establish predictors of glyburide success in gestational diabetes mellitus. Am J Obstet Gynecol. 2001;185(6)(Abst).-
17. Kitzmiller J. Limited efficacy of glyburide for glycemic control. Am J Obstet Gynecol. 2001;185(6)(Abst).-
18. Harris MI, Eastman RC, Cowie CC, Flegal KM, Eberhardt MS. Racial and ethnic differences in glycemic control of adults with type 2 diabetes. Diabetes Care. 1999;22:403-408.
19. Coetzee EJ, Jackson WPU. Diabetes newly diagnosed in pregnancy: a 4-year study at Groote Schuur Hospital. S Afr Med J. 1979;56:467-475.
20. Glueck CJ, Wang P, Kobayashi S. Metformin therapy throughout pregnancy reduces the development of gestational diabetes in women with polycystic ovary syndrome. Fertil Steril. 2002;77:520-525.
21. Hellmuth E, Damm P, Molsted-Pedersen L. Oral hypoglycemic agents in 118 diabetic pregnancies. Diabetic Med. 2000;17:507-511.
22. Jakubowicz DJ, Iuorno MJ, Jakubowicz S. Effects of metformin on early pregnancy loss in the polycystic ovary syndrome. J Clin Endocrinol Metab. 2002;87:524-529.
23. Langer O. When diet fails: insulin and oral hypoglycemic agents as alternatives for the management of gestational diabetes. J Matern Fetal Neonatal Med. 2002;11:1-8.
24. Langer O. Insulin and other treatment alternatives in gestational diabetes mellitus. Prenatal Neonatal Med. 1998;3:542-549.
25. Langer O. Oral hypoglycemic agents in pregnancy: their time has come. J Matern Fetal Neonatal Med. 2002;12:376-383.
26. Coetzee EJ, Jackson WPU. The management of non-insulin dependent diabetes during pregnancy. Diabetes Res Clin Practice. 1986;1:281-287.
27. Pendsey. Insulin vs glyburide therapy in gestational diabetes. Proceedings of the annual meeting of the International Diabetes Federation, Barcelona, Spain; 2001.
28. Drug Facts and Comparisons 2003. St. Louis, Mo: Facts and Comparisons; 2003.
29. Physicians Desk Reference 2003. Montvale, NJ: Thompson; 2003.