User login
Clopidogrel Deemed Safe in Vascular Surgery
NEW YORK – Considerable controversy surrounds the use of the anticoagulant clopidogrel in patients before, during, and after surgery for peripheral artery disease, but in a study of more than 10,000 patients, rates of postoperative bleeding complications were similar between those who continued the drugs before surgery and those who did not.
Dr. David H. Stone presented the results of the study, which involved 10,406 patients and 12 centers from the Vascular Study Group of New England, at the annual meeting of the Eastern Vascular Society. Four previously published single-center studies of the use of clopidogrel (Plavix, Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership) in vascular surgery patients accounted for fewer than 200 patients, he noted.
The patients in the New England study had carotid endarterectomy (CEA), lower extremity bypass, or endovascular or open abdominal aortic aneurysm (AAA) repair over a 6-year period. The study looked at reoperation for bleeding across all procedures and at blood transfusions in all procedures except CEA. Across all measures, the variations between the clopidogrel and non-clopidogrel groups were not statistically significant, said Dr. Stone of the Dartmouth-Hitchcock Medical Center in Lebanon, N.H.
The largest variations were seen in the blood transfusion rates in endovascular AAA repair (16% in the clopidogrel group vs. 11% in the non-clopidogrel group), and in open AAA repair (43% vs. 38%, respectively).
The rates of reoperation for rebleeding, however, were almost identical in CEA, lower extremity bypass, and endovascular AAA repair. In open AAA repair, the clopidogrel group actually had a lower rate than did the non-clopidogrel group (1.6% vs. 2.4%). “Based on our sample size, these conclusions are most robust for carotid endarterectomy and open AAA repair,” Dr. Stone said.
Dr. John J. Ricotta of Washington (D.C.) Hospital Center questioned the strength of using the blood transfusion rate as an outcome measure, because standards for using transfusion can vary among centers. “With the exception of open aneurysm repair, you picked operations that are relevant but are not highly associated with bleeding problems,” he said.
“I would agree with that analysis, but surprisingly in our own region and apparently in Europe the majority of surgeons – just looking at carotid endarterectomy – still hold Plavix prior to surgery for obviously a perception of increased bleeding,” Dr. Stone said.
In lower extremity bypass, Dr. Ricotta said, more precise predictors of bleeding problems are reoperation, obesity, and long incisions. “Did you look at these variables?” he asked.
Dr. Stone said that the study did not include an analysis of body mass index specifically, but that the pending CASPAR (Clopidogrel and Acetyl Salicylic Acid in Bypass Surgery for Peripheral Arterial Disease) trial would show no disparity between groups undergoing lower extremity bypass.
“Based on our analysis of over 10,000 patients, perioperative antiplatelet regimens, including Plavix, appear safe among those undergoing commonly performed vascular operations,” Dr. Stone said. “Accordingly, we believe that Plavix can be safely continued in patients with important indications for its use, such as symptomatic carotid disease or recent drug-eluting cardiac stent placement.”
Dr. Stone said that he had no relationships to disclose.
NEW YORK – Considerable controversy surrounds the use of the anticoagulant clopidogrel in patients before, during, and after surgery for peripheral artery disease, but in a study of more than 10,000 patients, rates of postoperative bleeding complications were similar between those who continued the drugs before surgery and those who did not.
Dr. David H. Stone presented the results of the study, which involved 10,406 patients and 12 centers from the Vascular Study Group of New England, at the annual meeting of the Eastern Vascular Society. Four previously published single-center studies of the use of clopidogrel (Plavix, Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership) in vascular surgery patients accounted for fewer than 200 patients, he noted.
The patients in the New England study had carotid endarterectomy (CEA), lower extremity bypass, or endovascular or open abdominal aortic aneurysm (AAA) repair over a 6-year period. The study looked at reoperation for bleeding across all procedures and at blood transfusions in all procedures except CEA. Across all measures, the variations between the clopidogrel and non-clopidogrel groups were not statistically significant, said Dr. Stone of the Dartmouth-Hitchcock Medical Center in Lebanon, N.H.
The largest variations were seen in the blood transfusion rates in endovascular AAA repair (16% in the clopidogrel group vs. 11% in the non-clopidogrel group), and in open AAA repair (43% vs. 38%, respectively).
The rates of reoperation for rebleeding, however, were almost identical in CEA, lower extremity bypass, and endovascular AAA repair. In open AAA repair, the clopidogrel group actually had a lower rate than did the non-clopidogrel group (1.6% vs. 2.4%). “Based on our sample size, these conclusions are most robust for carotid endarterectomy and open AAA repair,” Dr. Stone said.
Dr. John J. Ricotta of Washington (D.C.) Hospital Center questioned the strength of using the blood transfusion rate as an outcome measure, because standards for using transfusion can vary among centers. “With the exception of open aneurysm repair, you picked operations that are relevant but are not highly associated with bleeding problems,” he said.
“I would agree with that analysis, but surprisingly in our own region and apparently in Europe the majority of surgeons – just looking at carotid endarterectomy – still hold Plavix prior to surgery for obviously a perception of increased bleeding,” Dr. Stone said.
In lower extremity bypass, Dr. Ricotta said, more precise predictors of bleeding problems are reoperation, obesity, and long incisions. “Did you look at these variables?” he asked.
Dr. Stone said that the study did not include an analysis of body mass index specifically, but that the pending CASPAR (Clopidogrel and Acetyl Salicylic Acid in Bypass Surgery for Peripheral Arterial Disease) trial would show no disparity between groups undergoing lower extremity bypass.
“Based on our analysis of over 10,000 patients, perioperative antiplatelet regimens, including Plavix, appear safe among those undergoing commonly performed vascular operations,” Dr. Stone said. “Accordingly, we believe that Plavix can be safely continued in patients with important indications for its use, such as symptomatic carotid disease or recent drug-eluting cardiac stent placement.”
Dr. Stone said that he had no relationships to disclose.
NEW YORK – Considerable controversy surrounds the use of the anticoagulant clopidogrel in patients before, during, and after surgery for peripheral artery disease, but in a study of more than 10,000 patients, rates of postoperative bleeding complications were similar between those who continued the drugs before surgery and those who did not.
Dr. David H. Stone presented the results of the study, which involved 10,406 patients and 12 centers from the Vascular Study Group of New England, at the annual meeting of the Eastern Vascular Society. Four previously published single-center studies of the use of clopidogrel (Plavix, Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership) in vascular surgery patients accounted for fewer than 200 patients, he noted.
The patients in the New England study had carotid endarterectomy (CEA), lower extremity bypass, or endovascular or open abdominal aortic aneurysm (AAA) repair over a 6-year period. The study looked at reoperation for bleeding across all procedures and at blood transfusions in all procedures except CEA. Across all measures, the variations between the clopidogrel and non-clopidogrel groups were not statistically significant, said Dr. Stone of the Dartmouth-Hitchcock Medical Center in Lebanon, N.H.
The largest variations were seen in the blood transfusion rates in endovascular AAA repair (16% in the clopidogrel group vs. 11% in the non-clopidogrel group), and in open AAA repair (43% vs. 38%, respectively).
The rates of reoperation for rebleeding, however, were almost identical in CEA, lower extremity bypass, and endovascular AAA repair. In open AAA repair, the clopidogrel group actually had a lower rate than did the non-clopidogrel group (1.6% vs. 2.4%). “Based on our sample size, these conclusions are most robust for carotid endarterectomy and open AAA repair,” Dr. Stone said.
Dr. John J. Ricotta of Washington (D.C.) Hospital Center questioned the strength of using the blood transfusion rate as an outcome measure, because standards for using transfusion can vary among centers. “With the exception of open aneurysm repair, you picked operations that are relevant but are not highly associated with bleeding problems,” he said.
“I would agree with that analysis, but surprisingly in our own region and apparently in Europe the majority of surgeons – just looking at carotid endarterectomy – still hold Plavix prior to surgery for obviously a perception of increased bleeding,” Dr. Stone said.
In lower extremity bypass, Dr. Ricotta said, more precise predictors of bleeding problems are reoperation, obesity, and long incisions. “Did you look at these variables?” he asked.
Dr. Stone said that the study did not include an analysis of body mass index specifically, but that the pending CASPAR (Clopidogrel and Acetyl Salicylic Acid in Bypass Surgery for Peripheral Arterial Disease) trial would show no disparity between groups undergoing lower extremity bypass.
“Based on our analysis of over 10,000 patients, perioperative antiplatelet regimens, including Plavix, appear safe among those undergoing commonly performed vascular operations,” Dr. Stone said. “Accordingly, we believe that Plavix can be safely continued in patients with important indications for its use, such as symptomatic carotid disease or recent drug-eluting cardiac stent placement.”
Dr. Stone said that he had no relationships to disclose.
Radiation Dose Reduction Methods Gain Traction
PHILADELPHIA – Population exposure to medical radiation increased by 700% between 1980 and 2006, and nuclear cardiologists are feeling the pressure to reduce patients’ radiation exposure, according to Dr. Milena J. Henzlova of Mt. Sinai School of Medicine in New York.
“This is the first time in history that exposure to medical radiation exceeds natural radiation in the population,” she reported at the annual scientific session of the American Society of Nuclear Cardiology.
Reasons for this increased radiation exposure are varied and range from the availability of improved technology and deteriorating health of the general population, to the economic interests of manufacturers and providers, Dr. Henzlova said. In addition, “more noncardiologists are also referring [patients] for diagnostic studies, which is unusual in other medical subspecialties”
Dr. Henzlova outlined ways in which nuclear cardiologists could reduce radiation dosing in their patient populations.
One method is to follow existing American Society of Nuclear Cardiology guidelines and appropriateness criteria and the ALARA – as low as reasonably achievable – principle, she advised.
She also encouraged physicians to focus dose-reduction on younger patients, though “if the patient is in the ninth decade of life, maybe this principle becomes irrelevant.”
More broadly, more regulation of the imaging equipment might help rein in the dosing, and physicians and patients should become better educated in the hazards of medical radiation and the benefits of dose reduction, she said.
Dose-reduction methods nuclear cardiologists can use immediately include what she called “stress-first testing” rather than full stress-rest testing.
“At least 50% of our stress-rest studies are normal, and when we looked at huge sets of data, we found that 60%-70% were normal,” Dr. Henzlova said. “If there is a reason for the rest imaging, it’s to find the reversibility of a defect; but in more than half of patients there is no defect to start with.”
Her group studied results of more than 10,000 stress-rest tests and found that outcomes over 5 years were almost identical between the stress-only and image study groups. “We concluded that a normal stress study has the same 1-year prognosis as a full stress-rest study,” she said. “This is an attractive alternative to the stress-rest study in appropriately selected patients. Ultimately, time is saved, radiation is saved, and cost is decreased.”
Nuclear cardiologists could also opt for a 2-day rest study with lower doses of radiation, she said, referring to U.S. and European protocols. In a cohort at the Mt. Sinai School of Medicine, total microcuries (mCi) ranged from 48 to 72, compared with 33.8 to 47.3 in a European report on 2-day studies.
Dr. Benjamin Chow, of the University of Ottawa Heart Institute in Canada, also reported on dose reduction methods for cardiac CT. The methods he described included minimizing tube current (the number of electrons used) and tube voltage (the energy level of the electrons).
“The bottom line is that if you maintain adequate signal dose and adequate initial quality with lower tube current, in general that lowers radiation exposure,” he said.
The dose-reduction methods Dr. Chow reviewed included maintaining the tube current as the CT projects across the chest but reducing it across smaller body areas, turning off the scanner when the patient changes position, using bowtie filters, and activating the padding function, which can also reduce costs by up to 82%. He cautioned, however, that there would be some loss of image quality with padding.
Tube modulation is another method of maximizing imaging during the patient’s diastasis and minimizing it during systole, he said, but this also has its drawbacks, because although it restricts the amount of time the patient is exposed to radiation, “you may lose the ability to read different phases of the study.”
Dr. Chow said that his center routinely uses breast shields for women undergoing cardiac CT, which have been shown to reduce radiation exposure to the breast and lung, by 30% and 15%, respectively.
Neither Dr. Henzlova nor Dr. Chow had any relevant disclosures.
PHILADELPHIA – Population exposure to medical radiation increased by 700% between 1980 and 2006, and nuclear cardiologists are feeling the pressure to reduce patients’ radiation exposure, according to Dr. Milena J. Henzlova of Mt. Sinai School of Medicine in New York.
“This is the first time in history that exposure to medical radiation exceeds natural radiation in the population,” she reported at the annual scientific session of the American Society of Nuclear Cardiology.
Reasons for this increased radiation exposure are varied and range from the availability of improved technology and deteriorating health of the general population, to the economic interests of manufacturers and providers, Dr. Henzlova said. In addition, “more noncardiologists are also referring [patients] for diagnostic studies, which is unusual in other medical subspecialties”
Dr. Henzlova outlined ways in which nuclear cardiologists could reduce radiation dosing in their patient populations.
One method is to follow existing American Society of Nuclear Cardiology guidelines and appropriateness criteria and the ALARA – as low as reasonably achievable – principle, she advised.
She also encouraged physicians to focus dose-reduction on younger patients, though “if the patient is in the ninth decade of life, maybe this principle becomes irrelevant.”
More broadly, more regulation of the imaging equipment might help rein in the dosing, and physicians and patients should become better educated in the hazards of medical radiation and the benefits of dose reduction, she said.
Dose-reduction methods nuclear cardiologists can use immediately include what she called “stress-first testing” rather than full stress-rest testing.
“At least 50% of our stress-rest studies are normal, and when we looked at huge sets of data, we found that 60%-70% were normal,” Dr. Henzlova said. “If there is a reason for the rest imaging, it’s to find the reversibility of a defect; but in more than half of patients there is no defect to start with.”
Her group studied results of more than 10,000 stress-rest tests and found that outcomes over 5 years were almost identical between the stress-only and image study groups. “We concluded that a normal stress study has the same 1-year prognosis as a full stress-rest study,” she said. “This is an attractive alternative to the stress-rest study in appropriately selected patients. Ultimately, time is saved, radiation is saved, and cost is decreased.”
Nuclear cardiologists could also opt for a 2-day rest study with lower doses of radiation, she said, referring to U.S. and European protocols. In a cohort at the Mt. Sinai School of Medicine, total microcuries (mCi) ranged from 48 to 72, compared with 33.8 to 47.3 in a European report on 2-day studies.
Dr. Benjamin Chow, of the University of Ottawa Heart Institute in Canada, also reported on dose reduction methods for cardiac CT. The methods he described included minimizing tube current (the number of electrons used) and tube voltage (the energy level of the electrons).
“The bottom line is that if you maintain adequate signal dose and adequate initial quality with lower tube current, in general that lowers radiation exposure,” he said.
The dose-reduction methods Dr. Chow reviewed included maintaining the tube current as the CT projects across the chest but reducing it across smaller body areas, turning off the scanner when the patient changes position, using bowtie filters, and activating the padding function, which can also reduce costs by up to 82%. He cautioned, however, that there would be some loss of image quality with padding.
Tube modulation is another method of maximizing imaging during the patient’s diastasis and minimizing it during systole, he said, but this also has its drawbacks, because although it restricts the amount of time the patient is exposed to radiation, “you may lose the ability to read different phases of the study.”
Dr. Chow said that his center routinely uses breast shields for women undergoing cardiac CT, which have been shown to reduce radiation exposure to the breast and lung, by 30% and 15%, respectively.
Neither Dr. Henzlova nor Dr. Chow had any relevant disclosures.
PHILADELPHIA – Population exposure to medical radiation increased by 700% between 1980 and 2006, and nuclear cardiologists are feeling the pressure to reduce patients’ radiation exposure, according to Dr. Milena J. Henzlova of Mt. Sinai School of Medicine in New York.
“This is the first time in history that exposure to medical radiation exceeds natural radiation in the population,” she reported at the annual scientific session of the American Society of Nuclear Cardiology.
Reasons for this increased radiation exposure are varied and range from the availability of improved technology and deteriorating health of the general population, to the economic interests of manufacturers and providers, Dr. Henzlova said. In addition, “more noncardiologists are also referring [patients] for diagnostic studies, which is unusual in other medical subspecialties”
Dr. Henzlova outlined ways in which nuclear cardiologists could reduce radiation dosing in their patient populations.
One method is to follow existing American Society of Nuclear Cardiology guidelines and appropriateness criteria and the ALARA – as low as reasonably achievable – principle, she advised.
She also encouraged physicians to focus dose-reduction on younger patients, though “if the patient is in the ninth decade of life, maybe this principle becomes irrelevant.”
More broadly, more regulation of the imaging equipment might help rein in the dosing, and physicians and patients should become better educated in the hazards of medical radiation and the benefits of dose reduction, she said.
Dose-reduction methods nuclear cardiologists can use immediately include what she called “stress-first testing” rather than full stress-rest testing.
“At least 50% of our stress-rest studies are normal, and when we looked at huge sets of data, we found that 60%-70% were normal,” Dr. Henzlova said. “If there is a reason for the rest imaging, it’s to find the reversibility of a defect; but in more than half of patients there is no defect to start with.”
Her group studied results of more than 10,000 stress-rest tests and found that outcomes over 5 years were almost identical between the stress-only and image study groups. “We concluded that a normal stress study has the same 1-year prognosis as a full stress-rest study,” she said. “This is an attractive alternative to the stress-rest study in appropriately selected patients. Ultimately, time is saved, radiation is saved, and cost is decreased.”
Nuclear cardiologists could also opt for a 2-day rest study with lower doses of radiation, she said, referring to U.S. and European protocols. In a cohort at the Mt. Sinai School of Medicine, total microcuries (mCi) ranged from 48 to 72, compared with 33.8 to 47.3 in a European report on 2-day studies.
Dr. Benjamin Chow, of the University of Ottawa Heart Institute in Canada, also reported on dose reduction methods for cardiac CT. The methods he described included minimizing tube current (the number of electrons used) and tube voltage (the energy level of the electrons).
“The bottom line is that if you maintain adequate signal dose and adequate initial quality with lower tube current, in general that lowers radiation exposure,” he said.
The dose-reduction methods Dr. Chow reviewed included maintaining the tube current as the CT projects across the chest but reducing it across smaller body areas, turning off the scanner when the patient changes position, using bowtie filters, and activating the padding function, which can also reduce costs by up to 82%. He cautioned, however, that there would be some loss of image quality with padding.
Tube modulation is another method of maximizing imaging during the patient’s diastasis and minimizing it during systole, he said, but this also has its drawbacks, because although it restricts the amount of time the patient is exposed to radiation, “you may lose the ability to read different phases of the study.”
Dr. Chow said that his center routinely uses breast shields for women undergoing cardiac CT, which have been shown to reduce radiation exposure to the breast and lung, by 30% and 15%, respectively.
Neither Dr. Henzlova nor Dr. Chow had any relevant disclosures.
Strategies for Avoiding the Hospital Buyout
PHILADELPHIA – With hospitals buying up physician practices, many physicians are tempted to take the bait, but Alice G. Gosfield, an attorney who specializes in physician practice ownership strategies, called this the “employment delusion” and the “acquisition fantasy” during the annual meeting of the American Society of Nuclear Cardiology.
Many physicians don’t recognize that “the common law term for the employer-employee relationship is ‘master-servant,’” she said. “It’s a one-on-one relationship [in which the] master gets to tell you who, what, where, when, and why and how, and if you think that a contract can prevent that from happening, you would be wrong.”
Ms. Gosfield fed an audience of cardiologists a real-world dose of how even the best-laid plans go awry when physicians sell out to hospital groups. She also shared strategies on how doctors can avoid selling their practices to hospitals but still affiliate with hospital groups.
She debunked myths about how selling out to a hospital group can guarantee financial security. “The hospital is getting paid under the same stupid reimbursement formula that you are,” she said. “The only way that revenue stream ends up being more than what you’re getting in your practice is if they are paying you for doing other things besides clinical work.”
Another delusion is that the contract is a safeguard, according to Ms. Gosfield. “A contract is only as good as the will of the parties to abide by it,” she said. Not infrequently, one party will break the contract with little recourse outside the courts, “and litigation is a really, really bad way of solving business problems,” she added.
She singled out two strategies for selling a practice to a hospital: the sale of physical assets, including diagnostic “toys and weapons,” in her words, but not the practice per se; and noncompete covenants. “It has to be fair-market value under the Stark regulations,” she said of the latter, “and somebody – not a lawyer – has to do a valuation.”
But hospitals will not pay for good will. “They’re not going to make you whole for what it took you to build your practice,” she said. “I don’t care how long it took, what your sweat equity was, what all the pains were – you are not going to get that back from a hospital in terms of an acquisition or lease or other kind of arrangement.”
For self-preservation, she implored physicians to adopt the quality improvement measures that will provide the basis for Medicare reimbursement in 2012. “Now is the time to change your clinical and administrative processes,” she said. “Don’t wait until the conditions they’re going to be focused on are published. We all know what the conditions are.” That information is already available from the National Quality Forum, she pointed out.
Cardiologists are in a particularly strong position to deal with hospitals, she said. “Hospitals cannot function without cardiologists,” she said, citing the “20/80 rule” in which “20% of the doctors generate 80% of the medical staff’s billings.” She added, “They know that they make money on it, and they pay attention to you because you are cardiologists.”
Among the alternatives to selling the practice offered by Ms. Gosfield were leasing the practice to the hospital, entering into comanagement contracts, having the hospital place a new physician in the practice, gainsharing, giving the hospital the right of first refusal if another entity offers to buy the practice, having the hospital provide continuing education for practice physicians and ancillary staff, leasing practice staff to the hospital, and having the practice provide contract services (such as billing and claims processing) to the hospital.
Ms. Gosfield described how a hospital would lease a practice: “Your group stays as your group,” she said. “In essence what you do is, you reassign your right to get paid to the hospital. They pay you a salary. They will require some kind of productivity measures, but they can pay you irrespective of whether they get paid, which is not how your system works when you’re in private practice.”
A comanagement contract involves the physician providing on-call services or advising the hospital on its care delivery systems. This could include performance bonuses when the hospital achieves specified results, she said, but she advised against getting paid an hourly fee. “Swapping an hour in your office for an hour of their time – you can’t make it up,” she said.
Having the hospital place a physician in the practice should be carefully structured, Ms. Gosfield said. Her preferred arrangement would have the hospital subsidize the up-front costs with a loan, then forgive the loan for each month the doctor stays in the community after the subsidy ends. One problem with this approach, she pointed out, is that “you can’t then have a restricted covenant which prohibits this young doctor that you brought in and introduced to your patients from opening up next door,” she said.
She also cautioned against gainsharing, the concept of hospitals and physicians entering into agreements that award the latter for delivering quality, cost-effective care. “I’m not so sure about this,” she said “It’s not something that’s about quality; it’s about saving the hospital money. It’s not a sustainable business idea. If you want gainsharing money, you should do it on a short-term basis.”
Physicians can benefit from the right collaboration with a hospital, she said. “The things that unite you with the hospital are more than the things that divide you,” Ms. Gosfield noted. “You will do better holding hands crossing the dangerous street of health care in the future with the hospital, but you need to maintain your own identity.”
Ms. Gosfield reported no disclosures.
PHILADELPHIA – With hospitals buying up physician practices, many physicians are tempted to take the bait, but Alice G. Gosfield, an attorney who specializes in physician practice ownership strategies, called this the “employment delusion” and the “acquisition fantasy” during the annual meeting of the American Society of Nuclear Cardiology.
Many physicians don’t recognize that “the common law term for the employer-employee relationship is ‘master-servant,’” she said. “It’s a one-on-one relationship [in which the] master gets to tell you who, what, where, when, and why and how, and if you think that a contract can prevent that from happening, you would be wrong.”
Ms. Gosfield fed an audience of cardiologists a real-world dose of how even the best-laid plans go awry when physicians sell out to hospital groups. She also shared strategies on how doctors can avoid selling their practices to hospitals but still affiliate with hospital groups.
She debunked myths about how selling out to a hospital group can guarantee financial security. “The hospital is getting paid under the same stupid reimbursement formula that you are,” she said. “The only way that revenue stream ends up being more than what you’re getting in your practice is if they are paying you for doing other things besides clinical work.”
Another delusion is that the contract is a safeguard, according to Ms. Gosfield. “A contract is only as good as the will of the parties to abide by it,” she said. Not infrequently, one party will break the contract with little recourse outside the courts, “and litigation is a really, really bad way of solving business problems,” she added.
She singled out two strategies for selling a practice to a hospital: the sale of physical assets, including diagnostic “toys and weapons,” in her words, but not the practice per se; and noncompete covenants. “It has to be fair-market value under the Stark regulations,” she said of the latter, “and somebody – not a lawyer – has to do a valuation.”
But hospitals will not pay for good will. “They’re not going to make you whole for what it took you to build your practice,” she said. “I don’t care how long it took, what your sweat equity was, what all the pains were – you are not going to get that back from a hospital in terms of an acquisition or lease or other kind of arrangement.”
For self-preservation, she implored physicians to adopt the quality improvement measures that will provide the basis for Medicare reimbursement in 2012. “Now is the time to change your clinical and administrative processes,” she said. “Don’t wait until the conditions they’re going to be focused on are published. We all know what the conditions are.” That information is already available from the National Quality Forum, she pointed out.
Cardiologists are in a particularly strong position to deal with hospitals, she said. “Hospitals cannot function without cardiologists,” she said, citing the “20/80 rule” in which “20% of the doctors generate 80% of the medical staff’s billings.” She added, “They know that they make money on it, and they pay attention to you because you are cardiologists.”
Among the alternatives to selling the practice offered by Ms. Gosfield were leasing the practice to the hospital, entering into comanagement contracts, having the hospital place a new physician in the practice, gainsharing, giving the hospital the right of first refusal if another entity offers to buy the practice, having the hospital provide continuing education for practice physicians and ancillary staff, leasing practice staff to the hospital, and having the practice provide contract services (such as billing and claims processing) to the hospital.
Ms. Gosfield described how a hospital would lease a practice: “Your group stays as your group,” she said. “In essence what you do is, you reassign your right to get paid to the hospital. They pay you a salary. They will require some kind of productivity measures, but they can pay you irrespective of whether they get paid, which is not how your system works when you’re in private practice.”
A comanagement contract involves the physician providing on-call services or advising the hospital on its care delivery systems. This could include performance bonuses when the hospital achieves specified results, she said, but she advised against getting paid an hourly fee. “Swapping an hour in your office for an hour of their time – you can’t make it up,” she said.
Having the hospital place a physician in the practice should be carefully structured, Ms. Gosfield said. Her preferred arrangement would have the hospital subsidize the up-front costs with a loan, then forgive the loan for each month the doctor stays in the community after the subsidy ends. One problem with this approach, she pointed out, is that “you can’t then have a restricted covenant which prohibits this young doctor that you brought in and introduced to your patients from opening up next door,” she said.
She also cautioned against gainsharing, the concept of hospitals and physicians entering into agreements that award the latter for delivering quality, cost-effective care. “I’m not so sure about this,” she said “It’s not something that’s about quality; it’s about saving the hospital money. It’s not a sustainable business idea. If you want gainsharing money, you should do it on a short-term basis.”
Physicians can benefit from the right collaboration with a hospital, she said. “The things that unite you with the hospital are more than the things that divide you,” Ms. Gosfield noted. “You will do better holding hands crossing the dangerous street of health care in the future with the hospital, but you need to maintain your own identity.”
Ms. Gosfield reported no disclosures.
PHILADELPHIA – With hospitals buying up physician practices, many physicians are tempted to take the bait, but Alice G. Gosfield, an attorney who specializes in physician practice ownership strategies, called this the “employment delusion” and the “acquisition fantasy” during the annual meeting of the American Society of Nuclear Cardiology.
Many physicians don’t recognize that “the common law term for the employer-employee relationship is ‘master-servant,’” she said. “It’s a one-on-one relationship [in which the] master gets to tell you who, what, where, when, and why and how, and if you think that a contract can prevent that from happening, you would be wrong.”
Ms. Gosfield fed an audience of cardiologists a real-world dose of how even the best-laid plans go awry when physicians sell out to hospital groups. She also shared strategies on how doctors can avoid selling their practices to hospitals but still affiliate with hospital groups.
She debunked myths about how selling out to a hospital group can guarantee financial security. “The hospital is getting paid under the same stupid reimbursement formula that you are,” she said. “The only way that revenue stream ends up being more than what you’re getting in your practice is if they are paying you for doing other things besides clinical work.”
Another delusion is that the contract is a safeguard, according to Ms. Gosfield. “A contract is only as good as the will of the parties to abide by it,” she said. Not infrequently, one party will break the contract with little recourse outside the courts, “and litigation is a really, really bad way of solving business problems,” she added.
She singled out two strategies for selling a practice to a hospital: the sale of physical assets, including diagnostic “toys and weapons,” in her words, but not the practice per se; and noncompete covenants. “It has to be fair-market value under the Stark regulations,” she said of the latter, “and somebody – not a lawyer – has to do a valuation.”
But hospitals will not pay for good will. “They’re not going to make you whole for what it took you to build your practice,” she said. “I don’t care how long it took, what your sweat equity was, what all the pains were – you are not going to get that back from a hospital in terms of an acquisition or lease or other kind of arrangement.”
For self-preservation, she implored physicians to adopt the quality improvement measures that will provide the basis for Medicare reimbursement in 2012. “Now is the time to change your clinical and administrative processes,” she said. “Don’t wait until the conditions they’re going to be focused on are published. We all know what the conditions are.” That information is already available from the National Quality Forum, she pointed out.
Cardiologists are in a particularly strong position to deal with hospitals, she said. “Hospitals cannot function without cardiologists,” she said, citing the “20/80 rule” in which “20% of the doctors generate 80% of the medical staff’s billings.” She added, “They know that they make money on it, and they pay attention to you because you are cardiologists.”
Among the alternatives to selling the practice offered by Ms. Gosfield were leasing the practice to the hospital, entering into comanagement contracts, having the hospital place a new physician in the practice, gainsharing, giving the hospital the right of first refusal if another entity offers to buy the practice, having the hospital provide continuing education for practice physicians and ancillary staff, leasing practice staff to the hospital, and having the practice provide contract services (such as billing and claims processing) to the hospital.
Ms. Gosfield described how a hospital would lease a practice: “Your group stays as your group,” she said. “In essence what you do is, you reassign your right to get paid to the hospital. They pay you a salary. They will require some kind of productivity measures, but they can pay you irrespective of whether they get paid, which is not how your system works when you’re in private practice.”
A comanagement contract involves the physician providing on-call services or advising the hospital on its care delivery systems. This could include performance bonuses when the hospital achieves specified results, she said, but she advised against getting paid an hourly fee. “Swapping an hour in your office for an hour of their time – you can’t make it up,” she said.
Having the hospital place a physician in the practice should be carefully structured, Ms. Gosfield said. Her preferred arrangement would have the hospital subsidize the up-front costs with a loan, then forgive the loan for each month the doctor stays in the community after the subsidy ends. One problem with this approach, she pointed out, is that “you can’t then have a restricted covenant which prohibits this young doctor that you brought in and introduced to your patients from opening up next door,” she said.
She also cautioned against gainsharing, the concept of hospitals and physicians entering into agreements that award the latter for delivering quality, cost-effective care. “I’m not so sure about this,” she said “It’s not something that’s about quality; it’s about saving the hospital money. It’s not a sustainable business idea. If you want gainsharing money, you should do it on a short-term basis.”
Physicians can benefit from the right collaboration with a hospital, she said. “The things that unite you with the hospital are more than the things that divide you,” Ms. Gosfield noted. “You will do better holding hands crossing the dangerous street of health care in the future with the hospital, but you need to maintain your own identity.”
Ms. Gosfield reported no disclosures.
Protocol May Help Predict Outcomes in CRT Implantation
PHILADELPHIA – A protocol for using serial gated single photon emission computed tomography with a single injection radiotracer helped in patient selection for cardiac resynchronization therapy and guided left ventricle lead placement, investigators at the University of Pittsburgh reported at the annual meeting of the American Society of Nuclear Cardiology.
The phased analysis protocol involved leaving the cardiac resynchronization therapy (CRT) device inactive at the time of implantation, injecting a single dose of radiotracer, and acquiring a resting gated single photon emission computed tomography (SPECT); then activating the CRT and acquiring another gated SPECT, said Dr. Mati Friehling. The study was selected as winner of the ASNC’s Young Investigator Award Competition.
“There is great value of phase analysis which suggests a new technique to evaluate LV synchrony,” Dr. Friehling said. “There’s a linear relationship between the count changes throughout the cardiac cycle and myocardial wall thickening.” The count changes are key to determining the precise mechanical contraction for CRT, he said.
“One question is why do we care about the acute response?” Dr. Friehling said. “When we put a CRT device in, based on conventional criteria, we assume that acute resynchronization occurs, and this will give us a long-term benefit, but not always. We decided to use a gated SPECT-based approach because it gives us a congregant evaluation of the patient, including function and scar location and scar extent, which may be helpful for actual LV lead position.” The single-dose radiotracer was devised to limit radiation exposure, he said.
The study analyzed 44 patients after CRT device implantation, 18 of whom had improvement of dyssynchrony, 11 of whom had no change, and 15 of whom actually had deterioration of dyssynchrony, Dr. Friehling said. The leads were concordant in 22 patients, only one of whom actually worsened. In the remaining 22 with discordant leads, 8 had improvement or were unchanged, and 14 saw their dyssynchrony worsen, according to Dr. Friehling.
“There’s a very high specificity and positive predictive value for an improving or unchanged synchrony,” Dr. Friehling said.
“The responses are based on small changes in LV volume injection fraction according to echocardiography, which can be highly variable. We used harder end points such as death, CHF hospitalizations, ICD shocks, and viability of patients secondary to HF failure symptoms.”
Five deaths were reported among the 29 patients in the study group who had improved or unchanged dyssynchrony, Dr. Friehling said, while among the 15 patients who had deterioration of dyssynchrony, 8 had a cardiac event.
“Serial imaging based on conventional criteria can result in acute worsening of synchrony in some patients,” Dr. Friehling said. “The acute change in synchrony does appear to be associated with long-term outcome, and we may be able to use a baseline SPECT study to guide LV lead placement and to predict the acute response. Therefore SPECT may be a valuable tool for selecting patient for CRT.”
Dr. Friehling had no disclosures, but two of his coinvestigators disclosed relationships with Emory Cardiac Toolbox.
PHILADELPHIA – A protocol for using serial gated single photon emission computed tomography with a single injection radiotracer helped in patient selection for cardiac resynchronization therapy and guided left ventricle lead placement, investigators at the University of Pittsburgh reported at the annual meeting of the American Society of Nuclear Cardiology.
The phased analysis protocol involved leaving the cardiac resynchronization therapy (CRT) device inactive at the time of implantation, injecting a single dose of radiotracer, and acquiring a resting gated single photon emission computed tomography (SPECT); then activating the CRT and acquiring another gated SPECT, said Dr. Mati Friehling. The study was selected as winner of the ASNC’s Young Investigator Award Competition.
“There is great value of phase analysis which suggests a new technique to evaluate LV synchrony,” Dr. Friehling said. “There’s a linear relationship between the count changes throughout the cardiac cycle and myocardial wall thickening.” The count changes are key to determining the precise mechanical contraction for CRT, he said.
“One question is why do we care about the acute response?” Dr. Friehling said. “When we put a CRT device in, based on conventional criteria, we assume that acute resynchronization occurs, and this will give us a long-term benefit, but not always. We decided to use a gated SPECT-based approach because it gives us a congregant evaluation of the patient, including function and scar location and scar extent, which may be helpful for actual LV lead position.” The single-dose radiotracer was devised to limit radiation exposure, he said.
The study analyzed 44 patients after CRT device implantation, 18 of whom had improvement of dyssynchrony, 11 of whom had no change, and 15 of whom actually had deterioration of dyssynchrony, Dr. Friehling said. The leads were concordant in 22 patients, only one of whom actually worsened. In the remaining 22 with discordant leads, 8 had improvement or were unchanged, and 14 saw their dyssynchrony worsen, according to Dr. Friehling.
“There’s a very high specificity and positive predictive value for an improving or unchanged synchrony,” Dr. Friehling said.
“The responses are based on small changes in LV volume injection fraction according to echocardiography, which can be highly variable. We used harder end points such as death, CHF hospitalizations, ICD shocks, and viability of patients secondary to HF failure symptoms.”
Five deaths were reported among the 29 patients in the study group who had improved or unchanged dyssynchrony, Dr. Friehling said, while among the 15 patients who had deterioration of dyssynchrony, 8 had a cardiac event.
“Serial imaging based on conventional criteria can result in acute worsening of synchrony in some patients,” Dr. Friehling said. “The acute change in synchrony does appear to be associated with long-term outcome, and we may be able to use a baseline SPECT study to guide LV lead placement and to predict the acute response. Therefore SPECT may be a valuable tool for selecting patient for CRT.”
Dr. Friehling had no disclosures, but two of his coinvestigators disclosed relationships with Emory Cardiac Toolbox.
PHILADELPHIA – A protocol for using serial gated single photon emission computed tomography with a single injection radiotracer helped in patient selection for cardiac resynchronization therapy and guided left ventricle lead placement, investigators at the University of Pittsburgh reported at the annual meeting of the American Society of Nuclear Cardiology.
The phased analysis protocol involved leaving the cardiac resynchronization therapy (CRT) device inactive at the time of implantation, injecting a single dose of radiotracer, and acquiring a resting gated single photon emission computed tomography (SPECT); then activating the CRT and acquiring another gated SPECT, said Dr. Mati Friehling. The study was selected as winner of the ASNC’s Young Investigator Award Competition.
“There is great value of phase analysis which suggests a new technique to evaluate LV synchrony,” Dr. Friehling said. “There’s a linear relationship between the count changes throughout the cardiac cycle and myocardial wall thickening.” The count changes are key to determining the precise mechanical contraction for CRT, he said.
“One question is why do we care about the acute response?” Dr. Friehling said. “When we put a CRT device in, based on conventional criteria, we assume that acute resynchronization occurs, and this will give us a long-term benefit, but not always. We decided to use a gated SPECT-based approach because it gives us a congregant evaluation of the patient, including function and scar location and scar extent, which may be helpful for actual LV lead position.” The single-dose radiotracer was devised to limit radiation exposure, he said.
The study analyzed 44 patients after CRT device implantation, 18 of whom had improvement of dyssynchrony, 11 of whom had no change, and 15 of whom actually had deterioration of dyssynchrony, Dr. Friehling said. The leads were concordant in 22 patients, only one of whom actually worsened. In the remaining 22 with discordant leads, 8 had improvement or were unchanged, and 14 saw their dyssynchrony worsen, according to Dr. Friehling.
“There’s a very high specificity and positive predictive value for an improving or unchanged synchrony,” Dr. Friehling said.
“The responses are based on small changes in LV volume injection fraction according to echocardiography, which can be highly variable. We used harder end points such as death, CHF hospitalizations, ICD shocks, and viability of patients secondary to HF failure symptoms.”
Five deaths were reported among the 29 patients in the study group who had improved or unchanged dyssynchrony, Dr. Friehling said, while among the 15 patients who had deterioration of dyssynchrony, 8 had a cardiac event.
“Serial imaging based on conventional criteria can result in acute worsening of synchrony in some patients,” Dr. Friehling said. “The acute change in synchrony does appear to be associated with long-term outcome, and we may be able to use a baseline SPECT study to guide LV lead placement and to predict the acute response. Therefore SPECT may be a valuable tool for selecting patient for CRT.”
Dr. Friehling had no disclosures, but two of his coinvestigators disclosed relationships with Emory Cardiac Toolbox.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF NUCLEAR CARDIOLOGY
Protocol May Help Predict Outcomes in CRT Implantation
PHILADELPHIA – A protocol for using serial gated single photon emission computed tomography with a single injection radiotracer helped in patient selection for cardiac resynchronization therapy and guided left ventricle lead placement, investigators at the University of Pittsburgh reported at the annual meeting of the American Society of Nuclear Cardiology.
The phased analysis protocol involved leaving the cardiac resynchronization therapy (CRT) device inactive at the time of implantation, injecting a single dose of radiotracer, and acquiring a resting gated single photon emission computed tomography (SPECT); then activating the CRT and acquiring another gated SPECT, said Dr. Mati Friehling. The study was selected as winner of the ASNC’s Young Investigator Award Competition.
“There is great value of phase analysis which suggests a new technique to evaluate LV synchrony,” Dr. Friehling said. “There’s a linear relationship between the count changes throughout the cardiac cycle and myocardial wall thickening.” The count changes are key to determining the precise mechanical contraction for CRT, he said.
“One question is why do we care about the acute response?” Dr. Friehling said. “When we put a CRT device in, based on conventional criteria, we assume that acute resynchronization occurs, and this will give us a long-term benefit, but not always. We decided to use a gated SPECT-based approach because it gives us a congregant evaluation of the patient, including function and scar location and scar extent, which may be helpful for actual LV lead position.” The single-dose radiotracer was devised to limit radiation exposure, he said.
The study analyzed 44 patients after CRT device implantation, 18 of whom had improvement of dyssynchrony, 11 of whom had no change, and 15 of whom actually had deterioration of dyssynchrony, Dr. Friehling said. The leads were concordant in 22 patients, only one of whom actually worsened. In the remaining 22 with discordant leads, 8 had improvement or were unchanged, and 14 saw their dyssynchrony worsen, according to Dr. Friehling.
“There’s a very high specificity and positive predictive value for an improving or unchanged synchrony,” Dr. Friehling said. “The responses are based on small changes in LV volume injection fraction according to echocardiography, which can be highly variable. We used harder end points such as death, CHF hospitalizations, ICD shocks, and viability of patients secondary to HF failure symptoms.”
Five deaths were reported among the 29 patients in the study group who had improved or unchanged dyssynchrony, Dr. Friehling said, while among the 15 patients who had deterioration of dyssynchrony, 8 had a cardiac event.
“Serial imaging based on conventional criteria can result in acute worsening of synchrony in some patients,” Dr. Friehling said. “The acute change in synchrony does appear to be associated with long-term outcome, and we may be able to use a baseline SPECT study to guide LV lead placement and to predict the acute response. Therefore SPECT may be a valuable tool for selecting patient for CRT.”
Dr. Friehling had no disclosures, but two of his coinvestigators disclosed relationships with Emory Cardiac Toolbox.
PHILADELPHIA – A protocol for using serial gated single photon emission computed tomography with a single injection radiotracer helped in patient selection for cardiac resynchronization therapy and guided left ventricle lead placement, investigators at the University of Pittsburgh reported at the annual meeting of the American Society of Nuclear Cardiology.
The phased analysis protocol involved leaving the cardiac resynchronization therapy (CRT) device inactive at the time of implantation, injecting a single dose of radiotracer, and acquiring a resting gated single photon emission computed tomography (SPECT); then activating the CRT and acquiring another gated SPECT, said Dr. Mati Friehling. The study was selected as winner of the ASNC’s Young Investigator Award Competition.
“There is great value of phase analysis which suggests a new technique to evaluate LV synchrony,” Dr. Friehling said. “There’s a linear relationship between the count changes throughout the cardiac cycle and myocardial wall thickening.” The count changes are key to determining the precise mechanical contraction for CRT, he said.
“One question is why do we care about the acute response?” Dr. Friehling said. “When we put a CRT device in, based on conventional criteria, we assume that acute resynchronization occurs, and this will give us a long-term benefit, but not always. We decided to use a gated SPECT-based approach because it gives us a congregant evaluation of the patient, including function and scar location and scar extent, which may be helpful for actual LV lead position.” The single-dose radiotracer was devised to limit radiation exposure, he said.
The study analyzed 44 patients after CRT device implantation, 18 of whom had improvement of dyssynchrony, 11 of whom had no change, and 15 of whom actually had deterioration of dyssynchrony, Dr. Friehling said. The leads were concordant in 22 patients, only one of whom actually worsened. In the remaining 22 with discordant leads, 8 had improvement or were unchanged, and 14 saw their dyssynchrony worsen, according to Dr. Friehling.
“There’s a very high specificity and positive predictive value for an improving or unchanged synchrony,” Dr. Friehling said. “The responses are based on small changes in LV volume injection fraction according to echocardiography, which can be highly variable. We used harder end points such as death, CHF hospitalizations, ICD shocks, and viability of patients secondary to HF failure symptoms.”
Five deaths were reported among the 29 patients in the study group who had improved or unchanged dyssynchrony, Dr. Friehling said, while among the 15 patients who had deterioration of dyssynchrony, 8 had a cardiac event.
“Serial imaging based on conventional criteria can result in acute worsening of synchrony in some patients,” Dr. Friehling said. “The acute change in synchrony does appear to be associated with long-term outcome, and we may be able to use a baseline SPECT study to guide LV lead placement and to predict the acute response. Therefore SPECT may be a valuable tool for selecting patient for CRT.”
Dr. Friehling had no disclosures, but two of his coinvestigators disclosed relationships with Emory Cardiac Toolbox.
PHILADELPHIA – A protocol for using serial gated single photon emission computed tomography with a single injection radiotracer helped in patient selection for cardiac resynchronization therapy and guided left ventricle lead placement, investigators at the University of Pittsburgh reported at the annual meeting of the American Society of Nuclear Cardiology.
The phased analysis protocol involved leaving the cardiac resynchronization therapy (CRT) device inactive at the time of implantation, injecting a single dose of radiotracer, and acquiring a resting gated single photon emission computed tomography (SPECT); then activating the CRT and acquiring another gated SPECT, said Dr. Mati Friehling. The study was selected as winner of the ASNC’s Young Investigator Award Competition.
“There is great value of phase analysis which suggests a new technique to evaluate LV synchrony,” Dr. Friehling said. “There’s a linear relationship between the count changes throughout the cardiac cycle and myocardial wall thickening.” The count changes are key to determining the precise mechanical contraction for CRT, he said.
“One question is why do we care about the acute response?” Dr. Friehling said. “When we put a CRT device in, based on conventional criteria, we assume that acute resynchronization occurs, and this will give us a long-term benefit, but not always. We decided to use a gated SPECT-based approach because it gives us a congregant evaluation of the patient, including function and scar location and scar extent, which may be helpful for actual LV lead position.” The single-dose radiotracer was devised to limit radiation exposure, he said.
The study analyzed 44 patients after CRT device implantation, 18 of whom had improvement of dyssynchrony, 11 of whom had no change, and 15 of whom actually had deterioration of dyssynchrony, Dr. Friehling said. The leads were concordant in 22 patients, only one of whom actually worsened. In the remaining 22 with discordant leads, 8 had improvement or were unchanged, and 14 saw their dyssynchrony worsen, according to Dr. Friehling.
“There’s a very high specificity and positive predictive value for an improving or unchanged synchrony,” Dr. Friehling said. “The responses are based on small changes in LV volume injection fraction according to echocardiography, which can be highly variable. We used harder end points such as death, CHF hospitalizations, ICD shocks, and viability of patients secondary to HF failure symptoms.”
Five deaths were reported among the 29 patients in the study group who had improved or unchanged dyssynchrony, Dr. Friehling said, while among the 15 patients who had deterioration of dyssynchrony, 8 had a cardiac event.
“Serial imaging based on conventional criteria can result in acute worsening of synchrony in some patients,” Dr. Friehling said. “The acute change in synchrony does appear to be associated with long-term outcome, and we may be able to use a baseline SPECT study to guide LV lead placement and to predict the acute response. Therefore SPECT may be a valuable tool for selecting patient for CRT.”
Dr. Friehling had no disclosures, but two of his coinvestigators disclosed relationships with Emory Cardiac Toolbox.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF NUCLEAR CARDIOLOGY
Tighter Rules on Utilization Rates, Self-Referrals
PHILADELPHIA – Health care reform, in the guise of the Patient Protection and Affordable Care Act signed into law by President Obama last spring, will have unique impacts on nuclear cardiology practices as they deal with new regulations on utilization of imaging equipment and self-referrals.
Despite rumblings of overturning the law, Dr. Kim Williams said at the annual meeting of the American Society of Nuclear Cardiology that health care reform is here to stay. “It would be very difficult, though not impossible – but very difficult to flip a house of Congress and to repeal this.” Regulations will be phased in over the next 4 years, he said.
The equipment utilization rate that Medicare uses to establish reimbursements is due in 2011 for an adjustment for three types of imaging – MRI, CT, and PET – but excludes single photon emission computed tomography (SPECT). Dr. Williams of Wayne State University in Detroit, described the equipment utilization rate as “a mechanism to actually decrease reimbursement.” Medicare actually rolled back the rate for MRI, CT, and PET from 90% to 50% in 2010, but will bump it back up to 75% in 2011, he said.
Meanwhile, the Affordable Care Act tightens requirements on self-referrals. Dr. Williams raised a hypothetical situation familiar to all nuclear cardiologists. “Running an EKG – is that self-referral? Yes,” he said, “but it hasn’t come onto anyone’s radar screen because it isn’t a lot of money.” He cited other “elements of the house of medicine” with accusing cardiology and other specialties of inappropriate self-referral.
Like the equipment utilization rate, the disclosure provisions on self-referral cover MRI, CT, and PET but not SPECT, at least not yet, Dr. Williams said. “Most of us look at that [from the viewpoint that] a patient expects a self-respecting practice to own its equipment, so it isn’t that onerous,” he said. “But the devil is in the details.”
Among those details he outlined: “One will have to inform patients in writing at the time of the referral that they can obtain services from someone other than the referring physician or someone in the referring physician’s practice.”
That takes the form of a list of at least 10 other providers within a 25-mile radius, including phone numbers and distance. Dr. Williams outlined the ASNC’s comments on the regulation. “First of all, it should not include any imaging beyond CT, MRI, or PET,” he said. “It’s certainly not going to go any further than 25 miles, and the list requirement should be only for five other providers.” The higher number might compel cardiologists to include providers of questionable quality, he said. The final regulation should be ready by November to go into effect on Jan. 1.
The Affordable Care Act also empowers the Medicare Payment Advisory Commission (MedPAC) to make nonbinding recommendations to Congress on payment revisions. One problematic area MedPAC is looking at is developing payment tools that take into account providers’ utilization rates, Dr. Williams said. “If your utilization is high, you get less reimbursement,” he said. “The problem with that is that nobody mentioned risk adjustment.”
Another goal of MedPAC is to bundle payments for more groups of procedures. “For what we do, there aren’t an awful lot of efficiencies that can be bundled,” Dr. Williams said. MedPAC also may target prior authorizations for providers who have a high volume of studies: “sort of a radiation benefit manager pre-authorization service,” is how Dr. Williams described it.
ASNC is hoping MedPAC steers clear of these two areas: limiting the types of services the in-office ancillary exception covers and excluding payment for any service that’s not provided in an initial office visit. “That’s not going to fly,” Dr. Williams said of the latter.
Dr. Williams called on his colleagues to take an active role in shaping these regulations as they’re written by engaging their representatives. “You should be able to get involved with this. You should be weighing in on every piece of legislation and every Medicare regulation that affects nuclear cardiology,” he said.
Dr. Williams had no relevant disclosures.
PHILADELPHIA – Health care reform, in the guise of the Patient Protection and Affordable Care Act signed into law by President Obama last spring, will have unique impacts on nuclear cardiology practices as they deal with new regulations on utilization of imaging equipment and self-referrals.
Despite rumblings of overturning the law, Dr. Kim Williams said at the annual meeting of the American Society of Nuclear Cardiology that health care reform is here to stay. “It would be very difficult, though not impossible – but very difficult to flip a house of Congress and to repeal this.” Regulations will be phased in over the next 4 years, he said.
The equipment utilization rate that Medicare uses to establish reimbursements is due in 2011 for an adjustment for three types of imaging – MRI, CT, and PET – but excludes single photon emission computed tomography (SPECT). Dr. Williams of Wayne State University in Detroit, described the equipment utilization rate as “a mechanism to actually decrease reimbursement.” Medicare actually rolled back the rate for MRI, CT, and PET from 90% to 50% in 2010, but will bump it back up to 75% in 2011, he said.
Meanwhile, the Affordable Care Act tightens requirements on self-referrals. Dr. Williams raised a hypothetical situation familiar to all nuclear cardiologists. “Running an EKG – is that self-referral? Yes,” he said, “but it hasn’t come onto anyone’s radar screen because it isn’t a lot of money.” He cited other “elements of the house of medicine” with accusing cardiology and other specialties of inappropriate self-referral.
Like the equipment utilization rate, the disclosure provisions on self-referral cover MRI, CT, and PET but not SPECT, at least not yet, Dr. Williams said. “Most of us look at that [from the viewpoint that] a patient expects a self-respecting practice to own its equipment, so it isn’t that onerous,” he said. “But the devil is in the details.”
Among those details he outlined: “One will have to inform patients in writing at the time of the referral that they can obtain services from someone other than the referring physician or someone in the referring physician’s practice.”
That takes the form of a list of at least 10 other providers within a 25-mile radius, including phone numbers and distance. Dr. Williams outlined the ASNC’s comments on the regulation. “First of all, it should not include any imaging beyond CT, MRI, or PET,” he said. “It’s certainly not going to go any further than 25 miles, and the list requirement should be only for five other providers.” The higher number might compel cardiologists to include providers of questionable quality, he said. The final regulation should be ready by November to go into effect on Jan. 1.
The Affordable Care Act also empowers the Medicare Payment Advisory Commission (MedPAC) to make nonbinding recommendations to Congress on payment revisions. One problematic area MedPAC is looking at is developing payment tools that take into account providers’ utilization rates, Dr. Williams said. “If your utilization is high, you get less reimbursement,” he said. “The problem with that is that nobody mentioned risk adjustment.”
Another goal of MedPAC is to bundle payments for more groups of procedures. “For what we do, there aren’t an awful lot of efficiencies that can be bundled,” Dr. Williams said. MedPAC also may target prior authorizations for providers who have a high volume of studies: “sort of a radiation benefit manager pre-authorization service,” is how Dr. Williams described it.
ASNC is hoping MedPAC steers clear of these two areas: limiting the types of services the in-office ancillary exception covers and excluding payment for any service that’s not provided in an initial office visit. “That’s not going to fly,” Dr. Williams said of the latter.
Dr. Williams called on his colleagues to take an active role in shaping these regulations as they’re written by engaging their representatives. “You should be able to get involved with this. You should be weighing in on every piece of legislation and every Medicare regulation that affects nuclear cardiology,” he said.
Dr. Williams had no relevant disclosures.
PHILADELPHIA – Health care reform, in the guise of the Patient Protection and Affordable Care Act signed into law by President Obama last spring, will have unique impacts on nuclear cardiology practices as they deal with new regulations on utilization of imaging equipment and self-referrals.
Despite rumblings of overturning the law, Dr. Kim Williams said at the annual meeting of the American Society of Nuclear Cardiology that health care reform is here to stay. “It would be very difficult, though not impossible – but very difficult to flip a house of Congress and to repeal this.” Regulations will be phased in over the next 4 years, he said.
The equipment utilization rate that Medicare uses to establish reimbursements is due in 2011 for an adjustment for three types of imaging – MRI, CT, and PET – but excludes single photon emission computed tomography (SPECT). Dr. Williams of Wayne State University in Detroit, described the equipment utilization rate as “a mechanism to actually decrease reimbursement.” Medicare actually rolled back the rate for MRI, CT, and PET from 90% to 50% in 2010, but will bump it back up to 75% in 2011, he said.
Meanwhile, the Affordable Care Act tightens requirements on self-referrals. Dr. Williams raised a hypothetical situation familiar to all nuclear cardiologists. “Running an EKG – is that self-referral? Yes,” he said, “but it hasn’t come onto anyone’s radar screen because it isn’t a lot of money.” He cited other “elements of the house of medicine” with accusing cardiology and other specialties of inappropriate self-referral.
Like the equipment utilization rate, the disclosure provisions on self-referral cover MRI, CT, and PET but not SPECT, at least not yet, Dr. Williams said. “Most of us look at that [from the viewpoint that] a patient expects a self-respecting practice to own its equipment, so it isn’t that onerous,” he said. “But the devil is in the details.”
Among those details he outlined: “One will have to inform patients in writing at the time of the referral that they can obtain services from someone other than the referring physician or someone in the referring physician’s practice.”
That takes the form of a list of at least 10 other providers within a 25-mile radius, including phone numbers and distance. Dr. Williams outlined the ASNC’s comments on the regulation. “First of all, it should not include any imaging beyond CT, MRI, or PET,” he said. “It’s certainly not going to go any further than 25 miles, and the list requirement should be only for five other providers.” The higher number might compel cardiologists to include providers of questionable quality, he said. The final regulation should be ready by November to go into effect on Jan. 1.
The Affordable Care Act also empowers the Medicare Payment Advisory Commission (MedPAC) to make nonbinding recommendations to Congress on payment revisions. One problematic area MedPAC is looking at is developing payment tools that take into account providers’ utilization rates, Dr. Williams said. “If your utilization is high, you get less reimbursement,” he said. “The problem with that is that nobody mentioned risk adjustment.”
Another goal of MedPAC is to bundle payments for more groups of procedures. “For what we do, there aren’t an awful lot of efficiencies that can be bundled,” Dr. Williams said. MedPAC also may target prior authorizations for providers who have a high volume of studies: “sort of a radiation benefit manager pre-authorization service,” is how Dr. Williams described it.
ASNC is hoping MedPAC steers clear of these two areas: limiting the types of services the in-office ancillary exception covers and excluding payment for any service that’s not provided in an initial office visit. “That’s not going to fly,” Dr. Williams said of the latter.
Dr. Williams called on his colleagues to take an active role in shaping these regulations as they’re written by engaging their representatives. “You should be able to get involved with this. You should be weighing in on every piece of legislation and every Medicare regulation that affects nuclear cardiology,” he said.
Dr. Williams had no relevant disclosures.
Tighter Rules on Utilization Rates, Self-Referrals
PHILADELPHIA – Health care reform, in the guise of the Patient Protection and Affordable Care Act signed into law by President Obama last spring, will have unique impacts on nuclear cardiology practices as they deal with new regulations on utilization of imaging equipment and self-referrals.
Despite rumblings of overturning the law, Dr. Kim Williams said at the annual meeting of the American Society of Nuclear Cardiology that health care reform is here to stay. “It would be very difficult, though not impossible – but very difficult to flip a house of Congress and to repeal this.” Regulations will be phased in over the next 4 years, he said.
The equipment utilization rate that Medicare uses to establish reimbursements is due in 2011 for an adjustment for three types of imaging – MRI, CT, and PET – but excludes single photon emission computed tomography (SPECT). Dr. Williams of Wayne State University in Detroit, described the equipment utilization rate as “a mechanism to actually decrease reimbursement.” Medicare actually rolled back the rate for MRI, CT, and PET from 90% to 50% in 2010, but will bump it back up to 75% in 2011, he said.
Meanwhile, the Affordable Care Act tightens requirements on self-referrals. Dr. Williams raised a hypothetical situation familiar to all nuclear cardiologists. “Running an EKG – is that self-referral? Yes,” he said, “but it hasn’t come onto anyone’s radar screen because it isn’t a lot of money.” He cited other “elements of the house of medicine” with accusing cardiology and other specialties of inappropriate self-referral.
Like the equipment utilization rate, the disclosure provisions on self-referral cover MRI, CT, and PET but not SPECT, at least not yet, Dr. Williams said. “Most of us look at that [from the viewpoint that] a patient expects a self-respecting practice to own its equipment, so it isn’t that onerous,” he said. “But the devil is in the details.”
Among those details he outlined: “One will have to inform patients in writing at the time of the referral that they can obtain services from someone other than the referring physician or someone in the referring physician’s practice.”
That takes the form of a list of at least 10 other providers within a 25-mile radius, including phone numbers and distance. Dr. Williams outlined the ASNC’s comments on the regulation. “First of all, it should not include any imaging beyond CT, MRI, or PET,” he said. “It’s certainly not going to go any further than 25 miles, and the list requirement should be only for five other providers.” The higher number might compel cardiologists to include providers of questionable quality, he said. The final regulation should be ready by November to go into effect on Jan. 1.
The Affordable Care Act also empowers the Medicare Payment Advisory Commission (MedPAC) to make nonbinding recommendations to Congress on payment revisions. One problematic area MedPAC is looking at is developing payment tools that take into account providers’ utilization rates, Dr. Williams said. “If your utilization is high, you get less reimbursement,” he said. “The problem with that is that nobody mentioned risk adjustment.”
Another goal of MedPAC is to bundle payments for more groups of procedures. “For what we do, there aren’t an awful lot of efficiencies that can be bundled,” Dr. Williams said. MedPAC also may target prior authorizations for providers who have a high volume of studies: “sort of a radiation benefit manager pre-authorization service,” is how Dr. Williams described it.
ASNC is hoping MedPAC steers clear of these two areas: limiting the types of services the in-office ancillary exception covers and excluding payment for any service that’s not provided in an initial office visit. “That’s not going to fly,” Dr. Williams said of the latter.
Dr. Williams called on his colleagues to take an active role in shaping these regulations as they’re written by engaging their representatives. “You should be able to get involved with this. You should be weighing in on every piece of legislation and every Medicare regulation that affects nuclear cardiology,” he said.
Dr. Williams had no relevant disclosures.
PHILADELPHIA – Health care reform, in the guise of the Patient Protection and Affordable Care Act signed into law by President Obama last spring, will have unique impacts on nuclear cardiology practices as they deal with new regulations on utilization of imaging equipment and self-referrals.
Despite rumblings of overturning the law, Dr. Kim Williams said at the annual meeting of the American Society of Nuclear Cardiology that health care reform is here to stay. “It would be very difficult, though not impossible – but very difficult to flip a house of Congress and to repeal this.” Regulations will be phased in over the next 4 years, he said.
The equipment utilization rate that Medicare uses to establish reimbursements is due in 2011 for an adjustment for three types of imaging – MRI, CT, and PET – but excludes single photon emission computed tomography (SPECT). Dr. Williams of Wayne State University in Detroit, described the equipment utilization rate as “a mechanism to actually decrease reimbursement.” Medicare actually rolled back the rate for MRI, CT, and PET from 90% to 50% in 2010, but will bump it back up to 75% in 2011, he said.
Meanwhile, the Affordable Care Act tightens requirements on self-referrals. Dr. Williams raised a hypothetical situation familiar to all nuclear cardiologists. “Running an EKG – is that self-referral? Yes,” he said, “but it hasn’t come onto anyone’s radar screen because it isn’t a lot of money.” He cited other “elements of the house of medicine” with accusing cardiology and other specialties of inappropriate self-referral.
Like the equipment utilization rate, the disclosure provisions on self-referral cover MRI, CT, and PET but not SPECT, at least not yet, Dr. Williams said. “Most of us look at that [from the viewpoint that] a patient expects a self-respecting practice to own its equipment, so it isn’t that onerous,” he said. “But the devil is in the details.”
Among those details he outlined: “One will have to inform patients in writing at the time of the referral that they can obtain services from someone other than the referring physician or someone in the referring physician’s practice.”
That takes the form of a list of at least 10 other providers within a 25-mile radius, including phone numbers and distance. Dr. Williams outlined the ASNC’s comments on the regulation. “First of all, it should not include any imaging beyond CT, MRI, or PET,” he said. “It’s certainly not going to go any further than 25 miles, and the list requirement should be only for five other providers.” The higher number might compel cardiologists to include providers of questionable quality, he said. The final regulation should be ready by November to go into effect on Jan. 1.
The Affordable Care Act also empowers the Medicare Payment Advisory Commission (MedPAC) to make nonbinding recommendations to Congress on payment revisions. One problematic area MedPAC is looking at is developing payment tools that take into account providers’ utilization rates, Dr. Williams said. “If your utilization is high, you get less reimbursement,” he said. “The problem with that is that nobody mentioned risk adjustment.”
Another goal of MedPAC is to bundle payments for more groups of procedures. “For what we do, there aren’t an awful lot of efficiencies that can be bundled,” Dr. Williams said. MedPAC also may target prior authorizations for providers who have a high volume of studies: “sort of a radiation benefit manager pre-authorization service,” is how Dr. Williams described it.
ASNC is hoping MedPAC steers clear of these two areas: limiting the types of services the in-office ancillary exception covers and excluding payment for any service that’s not provided in an initial office visit. “That’s not going to fly,” Dr. Williams said of the latter.
Dr. Williams called on his colleagues to take an active role in shaping these regulations as they’re written by engaging their representatives. “You should be able to get involved with this. You should be weighing in on every piece of legislation and every Medicare regulation that affects nuclear cardiology,” he said.
Dr. Williams had no relevant disclosures.
PHILADELPHIA – Health care reform, in the guise of the Patient Protection and Affordable Care Act signed into law by President Obama last spring, will have unique impacts on nuclear cardiology practices as they deal with new regulations on utilization of imaging equipment and self-referrals.
Despite rumblings of overturning the law, Dr. Kim Williams said at the annual meeting of the American Society of Nuclear Cardiology that health care reform is here to stay. “It would be very difficult, though not impossible – but very difficult to flip a house of Congress and to repeal this.” Regulations will be phased in over the next 4 years, he said.
The equipment utilization rate that Medicare uses to establish reimbursements is due in 2011 for an adjustment for three types of imaging – MRI, CT, and PET – but excludes single photon emission computed tomography (SPECT). Dr. Williams of Wayne State University in Detroit, described the equipment utilization rate as “a mechanism to actually decrease reimbursement.” Medicare actually rolled back the rate for MRI, CT, and PET from 90% to 50% in 2010, but will bump it back up to 75% in 2011, he said.
Meanwhile, the Affordable Care Act tightens requirements on self-referrals. Dr. Williams raised a hypothetical situation familiar to all nuclear cardiologists. “Running an EKG – is that self-referral? Yes,” he said, “but it hasn’t come onto anyone’s radar screen because it isn’t a lot of money.” He cited other “elements of the house of medicine” with accusing cardiology and other specialties of inappropriate self-referral.
Like the equipment utilization rate, the disclosure provisions on self-referral cover MRI, CT, and PET but not SPECT, at least not yet, Dr. Williams said. “Most of us look at that [from the viewpoint that] a patient expects a self-respecting practice to own its equipment, so it isn’t that onerous,” he said. “But the devil is in the details.”
Among those details he outlined: “One will have to inform patients in writing at the time of the referral that they can obtain services from someone other than the referring physician or someone in the referring physician’s practice.”
That takes the form of a list of at least 10 other providers within a 25-mile radius, including phone numbers and distance. Dr. Williams outlined the ASNC’s comments on the regulation. “First of all, it should not include any imaging beyond CT, MRI, or PET,” he said. “It’s certainly not going to go any further than 25 miles, and the list requirement should be only for five other providers.” The higher number might compel cardiologists to include providers of questionable quality, he said. The final regulation should be ready by November to go into effect on Jan. 1.
The Affordable Care Act also empowers the Medicare Payment Advisory Commission (MedPAC) to make nonbinding recommendations to Congress on payment revisions. One problematic area MedPAC is looking at is developing payment tools that take into account providers’ utilization rates, Dr. Williams said. “If your utilization is high, you get less reimbursement,” he said. “The problem with that is that nobody mentioned risk adjustment.”
Another goal of MedPAC is to bundle payments for more groups of procedures. “For what we do, there aren’t an awful lot of efficiencies that can be bundled,” Dr. Williams said. MedPAC also may target prior authorizations for providers who have a high volume of studies: “sort of a radiation benefit manager pre-authorization service,” is how Dr. Williams described it.
ASNC is hoping MedPAC steers clear of these two areas: limiting the types of services the in-office ancillary exception covers and excluding payment for any service that’s not provided in an initial office visit. “That’s not going to fly,” Dr. Williams said of the latter.
Dr. Williams called on his colleagues to take an active role in shaping these regulations as they’re written by engaging their representatives. “You should be able to get involved with this. You should be weighing in on every piece of legislation and every Medicare regulation that affects nuclear cardiology,” he said.
Dr. Williams had no relevant disclosures.
Survival Benefit Seen With EVAR for Ruptured AAA
NEW YORK – Endovascular vs. open repair for ruptured aortic aneurysms has long been a source of controversy, but results of a multicenter international study indicate superior long-term survival with EVAR.
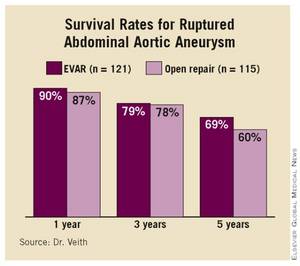
The study, which compared results from 121 patients who underwent EVAR vs. 115 who underwent open surgery, showed that the survival benefit from EVAR was maintained for 5 years, Dr. Frank Veith said at the annual meeting of the Eastern Vascular Society. “Of course, after 6 years there was catch-up because these were old, sick patients who died due to natural causes,” he added. But he emphasized that “the superiority of EVAR over open repair for ruptured abdominal aortic aneurysm is strongly supported in the long-term as well as the short-term data.” (See box.)
Dr. Veith of New York University and a visiting professor at Zurich University, presented the results on behalf of the Zurich group.
Results of other studies support the Zurich group’s conclusion that EVAR should become the standard of care for all patients with ruptured abdominal aortic aneurysm (AAA) who have suitable anatomy, Dr. Veith said. He cited a preliminary study by the Zurich group that looked at outcomes in a limited cohort at 2 years (J. Vasc. Surg. 2005;41:752-7) and another study from the Netherlands that looked at short-term outcomes in 187 patients (J. Vasc. Surg. 2008;48:1396-1400). He also noted that a U.K. study that followed 54 EVAR patients over a 10-year period found no survival advantage over open repair (Vascular 2007;15:191-6).

However, an unpublished 2009 analysis showed a 30-day mortality rate of 21% in EVAR patients, “comparing favorably with open repair,” Dr. Veith said. The “most important data” in this study were “from the 13 centers like our own that did EVAR on all anatomically suitable ruptured AAA patients,” he said. “We collected 680 ruptured AAA patients by EVAR and 763 by open repair by the same surgeons in the same institutions, and the 30-day mortality was dramatically better for EVAR” (19.7% vs. 36.3%), he said.
In the Zurich group’s study, growing numbers of suitable patients underwent EVAR for ruptured AAA between 1998 and 2009. “The increasing use of EVAR was related to increasing experience, increasing enthusiasm, and better devices,” Dr. Veith said. The average age of patients in the study was 72 years, and the investigators followed the patients with annual angiography, CT scan, and physical examination. All but two of the 103 surviving patients who had EVAR were followed long term.
The actual survival rate of all early EVAR patients was 62% in the Zurich study, Dr. Veith said. “In terms of quality of life, 86% of these patients were living at home, 78% were independent in their lifestyle, and 81% considered their quality of life to be good to excellent,” he added.
Dr. Julie Freischlag, chair of the department of surgery at Johns Hopkins Hospital, Baltimore, and coauthor of the Veterans Affairs Cooperative Study Group report comparing EVAR and open repair for ruptured AAA (JAMA 2009;302:1535-42), said she concurred with the conclusions that Dr. Veith reported. “We were real excited about that, because if you had to prove to the government why you should spend extra money to do an endovascular graft repair, one reason would be to increase survival, so we’re glad to see this,” she said.
Dr. Veith had no relevant disclosures.
NEW YORK – Endovascular vs. open repair for ruptured aortic aneurysms has long been a source of controversy, but results of a multicenter international study indicate superior long-term survival with EVAR.
The study, which compared results from 121 patients who underwent EVAR vs. 115 who underwent open surgery, showed that the survival benefit from EVAR was maintained for 5 years, Dr. Frank Veith said at the annual meeting of the Eastern Vascular Society. “Of course, after 6 years there was catch-up because these were old, sick patients who died due to natural causes,” he added. But he emphasized that “the superiority of EVAR over open repair for ruptured abdominal aortic aneurysm is strongly supported in the long-term as well as the short-term data.” (See box.)
Dr. Veith of New York University and a visiting professor at Zurich University, presented the results on behalf of the Zurich group.
Results of other studies support the Zurich group’s conclusion that EVAR should become the standard of care for all patients with ruptured abdominal aortic aneurysm (AAA) who have suitable anatomy, Dr. Veith said. He cited a preliminary study by the Zurich group that looked at outcomes in a limited cohort at 2 years (J. Vasc. Surg. 2005;41:752-7) and another study from the Netherlands that looked at short-term outcomes in 187 patients (J. Vasc. Surg. 2008;48:1396-1400). He also noted that a U.K. study that followed 54 EVAR patients over a 10-year period found no survival advantage over open repair (Vascular 2007;15:191-6).
However, an unpublished 2009 analysis showed a 30-day mortality rate of 21% in EVAR patients, “comparing favorably with open repair,” Dr. Veith said. The “most important data” in this study were “from the 13 centers like our own that did EVAR on all anatomically suitable ruptured AAA patients,” he said. “We collected 680 ruptured AAA patients by EVAR and 763 by open repair by the same surgeons in the same institutions, and the 30-day mortality was dramatically better for EVAR” (19.7% vs. 36.3%), he said.
In the Zurich group’s study, growing numbers of suitable patients underwent EVAR for ruptured AAA between 1998 and 2009. “The increasing use of EVAR was related to increasing experience, increasing enthusiasm, and better devices,” Dr. Veith said. The average age of patients in the study was 72 years, and the investigators followed the patients with annual angiography, CT scan, and physical examination. All but two of the 103 surviving patients who had EVAR were followed long term.
The actual survival rate of all early EVAR patients was 62% in the Zurich study, Dr. Veith said. “In terms of quality of life, 86% of these patients were living at home, 78% were independent in their lifestyle, and 81% considered their quality of life to be good to excellent,” he added.
Dr. Julie Freischlag, chair of the department of surgery at Johns Hopkins Hospital, Baltimore, and coauthor of the Veterans Affairs Cooperative Study Group report comparing EVAR and open repair for ruptured AAA (JAMA 2009;302:1535-42), said she concurred with the conclusions that Dr. Veith reported. “We were real excited about that, because if you had to prove to the government why you should spend extra money to do an endovascular graft repair, one reason would be to increase survival, so we’re glad to see this,” she said.
Dr. Veith had no relevant disclosures.
NEW YORK – Endovascular vs. open repair for ruptured aortic aneurysms has long been a source of controversy, but results of a multicenter international study indicate superior long-term survival with EVAR.
The study, which compared results from 121 patients who underwent EVAR vs. 115 who underwent open surgery, showed that the survival benefit from EVAR was maintained for 5 years, Dr. Frank Veith said at the annual meeting of the Eastern Vascular Society. “Of course, after 6 years there was catch-up because these were old, sick patients who died due to natural causes,” he added. But he emphasized that “the superiority of EVAR over open repair for ruptured abdominal aortic aneurysm is strongly supported in the long-term as well as the short-term data.” (See box.)
Dr. Veith of New York University and a visiting professor at Zurich University, presented the results on behalf of the Zurich group.
Results of other studies support the Zurich group’s conclusion that EVAR should become the standard of care for all patients with ruptured abdominal aortic aneurysm (AAA) who have suitable anatomy, Dr. Veith said. He cited a preliminary study by the Zurich group that looked at outcomes in a limited cohort at 2 years (J. Vasc. Surg. 2005;41:752-7) and another study from the Netherlands that looked at short-term outcomes in 187 patients (J. Vasc. Surg. 2008;48:1396-1400). He also noted that a U.K. study that followed 54 EVAR patients over a 10-year period found no survival advantage over open repair (Vascular 2007;15:191-6).
However, an unpublished 2009 analysis showed a 30-day mortality rate of 21% in EVAR patients, “comparing favorably with open repair,” Dr. Veith said. The “most important data” in this study were “from the 13 centers like our own that did EVAR on all anatomically suitable ruptured AAA patients,” he said. “We collected 680 ruptured AAA patients by EVAR and 763 by open repair by the same surgeons in the same institutions, and the 30-day mortality was dramatically better for EVAR” (19.7% vs. 36.3%), he said.
In the Zurich group’s study, growing numbers of suitable patients underwent EVAR for ruptured AAA between 1998 and 2009. “The increasing use of EVAR was related to increasing experience, increasing enthusiasm, and better devices,” Dr. Veith said. The average age of patients in the study was 72 years, and the investigators followed the patients with annual angiography, CT scan, and physical examination. All but two of the 103 surviving patients who had EVAR were followed long term.
The actual survival rate of all early EVAR patients was 62% in the Zurich study, Dr. Veith said. “In terms of quality of life, 86% of these patients were living at home, 78% were independent in their lifestyle, and 81% considered their quality of life to be good to excellent,” he added.
Dr. Julie Freischlag, chair of the department of surgery at Johns Hopkins Hospital, Baltimore, and coauthor of the Veterans Affairs Cooperative Study Group report comparing EVAR and open repair for ruptured AAA (JAMA 2009;302:1535-42), said she concurred with the conclusions that Dr. Veith reported. “We were real excited about that, because if you had to prove to the government why you should spend extra money to do an endovascular graft repair, one reason would be to increase survival, so we’re glad to see this,” she said.
Dr. Veith had no relevant disclosures.
Survival Benefit Seen With EVAR for Ruptured AAA
NEW YORK – Endovascular vs. open repair for ruptured aortic aneurysms has long been a source of controversy, but results of a multicenter international study indicate superior long-term survival with EVAR.
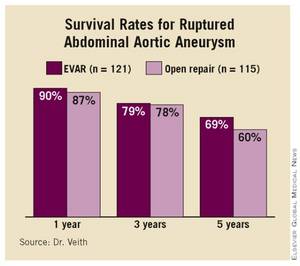
The study, which compared results from 121 patients who underwent EVAR vs. 115 who underwent open surgery, showed that the survival benefit from EVAR was maintained for 5 years, Dr. Frank Veith said at the annual meeting of the Eastern Vascular Society. “Of course, after 6 years there was catch-up because these were old, sick patients who died due to natural causes,” he added. But he emphasized that “the superiority of EVAR over open repair for ruptured abdominal aortic aneurysm is strongly supported in the long-term as well as the short-term data.” (See box.)
Dr. Veith of New York University and a visiting professor at Zurich University, presented the results on behalf of the Zurich group.
Results of other studies support the Zurich group’s conclusion that EVAR should become the standard of care for all patients with ruptured abdominal aortic aneurysm (AAA) who have suitable anatomy, Dr. Veith said. He cited a preliminary study by the Zurich group that looked at outcomes in a limited cohort at 2 years (J. Vasc. Surg. 2005;41:752-7) and another study from the Netherlands that looked at short-term outcomes in 187 patients (J. Vasc. Surg. 2008;48:1396-1400). He also noted that a U.K. study that followed 54 EVAR patients over a 10-year period found no survival advantage over open repair (Vascular 2007;15:191-6).
However, an unpublished 2009 analysis showed a 30-day mortality rate of 21% in EVAR patients, “comparing favorably with open repair,” Dr. Veith said. The “most important data” in this study were “from the 13 centers like our own that did EVAR on all anatomically suitable ruptured AAA patients,” he said. “We collected 680 ruptured AAA patients by EVAR and 763 by open repair by the same surgeons in the same institutions, and the 30-day mortality was dramatically better for EVAR” (19.7% vs. 36.3%), he said.
In the Zurich group’s study, growing numbers of suitable patients underwent EVAR for ruptured AAA between 1998 and 2009. “The increasing use of EVAR was related to increasing experience, increasing enthusiasm, and better devices,” Dr. Veith said. The average age of patients in the study was 72 years, and the investigators followed the patients with annual angiography, CT scan, and physical examination. All but two of the 103 surviving patients who had EVAR were followed long term.
The actual survival rate of all early EVAR patients was 62% in the Zurich study, Dr. Veith said. “In terms of quality of life, 86% of these patients were living at home, 78% were independent in their lifestyle, and 81% considered their quality of life to be good to excellent,” he added.
Dr. Julie Freischlag, chair of the department of surgery at Johns Hopkins Hospital, Baltimore, and coauthor of the Veterans Affairs Cooperative Study Group report comparing EVAR and open repair for ruptured AAA (JAMA 2009;302:1535-42), said she concurred with the conclusions that Dr. Veith reported. “We were real excited about that, because if you had to prove to the government why you should spend extra money to do an endovascular graft repair, one reason would be to increase survival, so we’re glad to see this,” she said.
Dr. Veith had no relevant disclosures.
NEW YORK – Endovascular vs. open repair for ruptured aortic aneurysms has long been a source of controversy, but results of a multicenter international study indicate superior long-term survival with EVAR.
The study, which compared results from 121 patients who underwent EVAR vs. 115 who underwent open surgery, showed that the survival benefit from EVAR was maintained for 5 years, Dr. Frank Veith said at the annual meeting of the Eastern Vascular Society. “Of course, after 6 years there was catch-up because these were old, sick patients who died due to natural causes,” he added. But he emphasized that “the superiority of EVAR over open repair for ruptured abdominal aortic aneurysm is strongly supported in the long-term as well as the short-term data.” (See box.)
Dr. Veith of New York University and a visiting professor at Zurich University, presented the results on behalf of the Zurich group.
Results of other studies support the Zurich group’s conclusion that EVAR should become the standard of care for all patients with ruptured abdominal aortic aneurysm (AAA) who have suitable anatomy, Dr. Veith said. He cited a preliminary study by the Zurich group that looked at outcomes in a limited cohort at 2 years (J. Vasc. Surg. 2005;41:752-7) and another study from the Netherlands that looked at short-term outcomes in 187 patients (J. Vasc. Surg. 2008;48:1396-1400). He also noted that a U.K. study that followed 54 EVAR patients over a 10-year period found no survival advantage over open repair (Vascular 2007;15:191-6).
However, an unpublished 2009 analysis showed a 30-day mortality rate of 21% in EVAR patients, “comparing favorably with open repair,” Dr. Veith said. The “most important data” in this study were “from the 13 centers like our own that did EVAR on all anatomically suitable ruptured AAA patients,” he said. “We collected 680 ruptured AAA patients by EVAR and 763 by open repair by the same surgeons in the same institutions, and the 30-day mortality was dramatically better for EVAR” (19.7% vs. 36.3%), he said.
In the Zurich group’s study, growing numbers of suitable patients underwent EVAR for ruptured AAA between 1998 and 2009. “The increasing use of EVAR was related to increasing experience, increasing enthusiasm, and better devices,” Dr. Veith said. The average age of patients in the study was 72 years, and the investigators followed the patients with annual angiography, CT scan, and physical examination. All but two of the 103 surviving patients who had EVAR were followed long term.
The actual survival rate of all early EVAR patients was 62% in the Zurich study, Dr. Veith said. “In terms of quality of life, 86% of these patients were living at home, 78% were independent in their lifestyle, and 81% considered their quality of life to be good to excellent,” he added.
Dr. Julie Freischlag, chair of the department of surgery at Johns Hopkins Hospital, Baltimore, and coauthor of the Veterans Affairs Cooperative Study Group report comparing EVAR and open repair for ruptured AAA (JAMA 2009;302:1535-42), said she concurred with the conclusions that Dr. Veith reported. “We were real excited about that, because if you had to prove to the government why you should spend extra money to do an endovascular graft repair, one reason would be to increase survival, so we’re glad to see this,” she said.
Dr. Veith had no relevant disclosures.
NEW YORK – Endovascular vs. open repair for ruptured aortic aneurysms has long been a source of controversy, but results of a multicenter international study indicate superior long-term survival with EVAR.
The study, which compared results from 121 patients who underwent EVAR vs. 115 who underwent open surgery, showed that the survival benefit from EVAR was maintained for 5 years, Dr. Frank Veith said at the annual meeting of the Eastern Vascular Society. “Of course, after 6 years there was catch-up because these were old, sick patients who died due to natural causes,” he added. But he emphasized that “the superiority of EVAR over open repair for ruptured abdominal aortic aneurysm is strongly supported in the long-term as well as the short-term data.” (See box.)
Dr. Veith of New York University and a visiting professor at Zurich University, presented the results on behalf of the Zurich group.
Results of other studies support the Zurich group’s conclusion that EVAR should become the standard of care for all patients with ruptured abdominal aortic aneurysm (AAA) who have suitable anatomy, Dr. Veith said. He cited a preliminary study by the Zurich group that looked at outcomes in a limited cohort at 2 years (J. Vasc. Surg. 2005;41:752-7) and another study from the Netherlands that looked at short-term outcomes in 187 patients (J. Vasc. Surg. 2008;48:1396-1400). He also noted that a U.K. study that followed 54 EVAR patients over a 10-year period found no survival advantage over open repair (Vascular 2007;15:191-6).
However, an unpublished 2009 analysis showed a 30-day mortality rate of 21% in EVAR patients, “comparing favorably with open repair,” Dr. Veith said. The “most important data” in this study were “from the 13 centers like our own that did EVAR on all anatomically suitable ruptured AAA patients,” he said. “We collected 680 ruptured AAA patients by EVAR and 763 by open repair by the same surgeons in the same institutions, and the 30-day mortality was dramatically better for EVAR” (19.7% vs. 36.3%), he said.
In the Zurich group’s study, growing numbers of suitable patients underwent EVAR for ruptured AAA between 1998 and 2009. “The increasing use of EVAR was related to increasing experience, increasing enthusiasm, and better devices,” Dr. Veith said. The average age of patients in the study was 72 years, and the investigators followed the patients with annual angiography, CT scan, and physical examination. All but two of the 103 surviving patients who had EVAR were followed long term.
The actual survival rate of all early EVAR patients was 62% in the Zurich study, Dr. Veith said. “In terms of quality of life, 86% of these patients were living at home, 78% were independent in their lifestyle, and 81% considered their quality of life to be good to excellent,” he added.
Dr. Julie Freischlag, chair of the department of surgery at Johns Hopkins Hospital, Baltimore, and coauthor of the Veterans Affairs Cooperative Study Group report comparing EVAR and open repair for ruptured AAA (JAMA 2009;302:1535-42), said she concurred with the conclusions that Dr. Veith reported. “We were real excited about that, because if you had to prove to the government why you should spend extra money to do an endovascular graft repair, one reason would be to increase survival, so we’re glad to see this,” she said.
Dr. Veith had no relevant disclosures.
Major Finding: Survival rates at 5 years were 69% for endovascular aneurysm repair vs. 60% for open repair in patients with ruptured aortic aneurysms.
Data Source: A multicenter international study of 236 patients.
Disclosures: Dr. Veith had no relevant disclosures.
'Top Ten' Forecast for Interventional Cardiology
NEW YORK — Findings in 10 key investigative areas, from platelet inhibition and left main coronary artery disease to the use of fractional flow reserves and the “kissing” stent could have a profound impact on interventional cardiology in the next year or so.
Dr. Samin K. Sharma, co-director of the Cardiovascular Institute at Mt. Sinai Medical Center in New York, provided his take on these findings:
▸ Clopidogrel resistance and proton pump inhibitor interaction studies. In March, the FDA issued a warning that clopidogrel, widely prescribed to patients who have had an MI or stroke, is not as effective in people who cannot metabolize the drug. Dr. Sharma cited numerous reports that have shown that PPI drugs inhibit the activity of clopidogrel. In the clinic, physicians can test patients for platelet inhibition and use those data accordingly to modify dosing of the PPI.
“Avoid routine use of PPI with clopidogrel,” Dr. Sharma said. “If proton pump inhibition is needed, use H2 receptor blockers instead. If you need to use a PPI, many studies have shown it to be safer to use clopidogrel in the morning and the PPI in evening.” In high-risk patients, he advised using a 600-mg loading dose of PPI, then 150 mg daily. While genetic testing may help identify vulnerable groups, he added, it's “a very complex issue cost wise.”
▸ BARI 2D trial. The Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI 2D) found that prompt revascularization offered no significant advantages over medical therapy in terms of mortality and cardiovascular events for diabetes patients (N. Engl. J. Med. 2009;260:2503-15). The BARI 2D findings replicated those of the COURAGE trial (Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation; N. Engl. J. Med. 2007;356:1503-16), Dr. Sharma noted.
“As long as the patient is on excellent medical therapy, percutaneous coronary intervention [PCI] or revascularization is not essential for management of these patients,” Dr. Sharma said. Results of the FREEDOM trial (Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease) are due in 2012, he said, and could either corroborate or contradict the BARI 2D findings.
▸ Bifurcation lesion trials. At Mt. Sinai, Dr. Sharma and his team have investigated the “kissing” stent—the simultaneous placement of two stents in the main and side branch vessels of a bifurcated lesion. This technique was validated in the Nordic Bifurcation Study (Circulation 2006;114:1955-61). More recent trials have determined the two-stent approach is “definitely not inferior, and maybe even better than the one-stent approach,” he said.
▸ Trials on timing of intervention. Dr. Sharma cited two trials—TIMACS (Timing of Intervention in Patients With Acute Coronary Syndromes; N. Engl. J. Med. 2009;360:2165-75) and ABOARD (Angioplasty to Blunt the Rise of Troponin in Acute Coronary Syndromes Randomized for an Immediate or Delayed Intervention; JAMA 2009;302:947-54)—that looked at timing of intervention in patients with acute coronary syndrome. The studies found similar results in patients who had intervention within 2 hours and those who waited 16-24 hours. “Clearly, it seems that to wait for 24 hours is the right approach in treatment of systemic lesions when the patient is hemodynamically stable,” Dr. Sharma said.
▸ Percutaneous heart valve trials. The PARTNER (Placement of Aortic Transcatheter Valve) trial, estimated to be completed in 2014, is comparing transcatheter valvuloplasty with conventional heart valve replacement. Outcomes have improved since the study began enrolling patients in 2007, Dr. Sharma said. “The percutaneous valve field will continue to evolve,” he said.
▸ HORIZONS-AMI trial. The HORIZONS-AMI (Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction) trial investigators concluded that paclitaxel-eluting stents significantly reduced the risk of restenosis in patients with STEMI when compared with bare-metal stents (N. Engl. J. Med. 2009;360:1946-59). “This shows that drug-eluting stents are acceptable in systemic patients,” Dr. Sharma said.
▸ FAME trial. The Fractional Flow Reserve vs. Angiography for Guiding PCI in Patients with Multivessel Coronary Artery Disease trial (N. Engl. J. Med. 2009;360:213-24) looked at using fractional flow reserve (FFR) as an alternative to angiography for stent placement. It found that routinely measuring FFR in patients with multivessel disease for PCI with drug-eluting stents reduced the rate of death, MI, and repeat revascularization at 1 year. “At 1 year, fractional flow reserve is beneficial,” he said.
▸ Drug-eluting stent comparison trials. As trials move into second-generation drug-eluting stents, outcomes are comparing more favorably with those of bare-metal stents, Dr. Sharma said. A breakthrough comparative study of drug-eluting stents concluded that newer designs had advantages over then Food and Drug Administration–approved devices in terms of arterial healing and recovery (J. Am. Coll. Cardiol. 2008;52:333-42). He also cited the ENDEAVOR-IV trial, which showed that the zotarolimus-eluting stent had significantly lower rates of cardiac death and heart attack than did the paclitaxel-eluting Taxus stent after 3 years. Other trials are comparing other drug-eluting stents, he said. “The real issue is late stent thrombosis after 1 year,” he said.
▸ The PLATO trial. The Study of Platelet Inhibition and Patient Outcomes (N. Engl. J. Med. 2009;361:1045-57) trial found that ticagrelor had a significantly lower rate of death from vascular causes, heart attack, or stroke when compared with clopidogrel, with no increase in the overall bleeding rate. “It looks like we have a home run once this drug gets approved,” Dr. Sharma said.
▸ Unprotected left main coronary artery studies. The SYNTAX trial (N. Engl. J. Med. 2009;360:961-72) compared the paclitaxel-eluting Taxus stent with coronary artery bypass grafting (CABG) for atherosclerosis. While the findings confirmed CABG as the standard of care for three-vessel or left main coronary artery disease, Dr. Sharma said that PCI for left main coronary artery disease has shown steadily improving outcomes.
Updated American College of Cardiology/American Heart Association guidelines have elevated PCI for left main coronary artery disease to a class IIb indication from class III for patients at high risk of surgery, Dr. Sharma said. “But I am disappointed they did not take it into consideration for ostial left main disease,” he added. The EXCEL (Evaluation of Xience Prime Versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization) trial, which began enrolling patients this year, will provide what Dr. Sharma called “the final answer” on the use of PCI in left main coronary artery disease.
Dr. Sharma has received honoraria from Boston Scientific Corp., Abbott Laboratories, and the Medicines Company.
{kind=link}
PCI for left main coronary artery disease has shown steadily improving outcomes.
Source DR. SHARMA
NEW YORK — Findings in 10 key investigative areas, from platelet inhibition and left main coronary artery disease to the use of fractional flow reserves and the “kissing” stent could have a profound impact on interventional cardiology in the next year or so.
Dr. Samin K. Sharma, co-director of the Cardiovascular Institute at Mt. Sinai Medical Center in New York, provided his take on these findings:
▸ Clopidogrel resistance and proton pump inhibitor interaction studies. In March, the FDA issued a warning that clopidogrel, widely prescribed to patients who have had an MI or stroke, is not as effective in people who cannot metabolize the drug. Dr. Sharma cited numerous reports that have shown that PPI drugs inhibit the activity of clopidogrel. In the clinic, physicians can test patients for platelet inhibition and use those data accordingly to modify dosing of the PPI.
“Avoid routine use of PPI with clopidogrel,” Dr. Sharma said. “If proton pump inhibition is needed, use H2 receptor blockers instead. If you need to use a PPI, many studies have shown it to be safer to use clopidogrel in the morning and the PPI in evening.” In high-risk patients, he advised using a 600-mg loading dose of PPI, then 150 mg daily. While genetic testing may help identify vulnerable groups, he added, it's “a very complex issue cost wise.”
▸ BARI 2D trial. The Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI 2D) found that prompt revascularization offered no significant advantages over medical therapy in terms of mortality and cardiovascular events for diabetes patients (N. Engl. J. Med. 2009;260:2503-15). The BARI 2D findings replicated those of the COURAGE trial (Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation; N. Engl. J. Med. 2007;356:1503-16), Dr. Sharma noted.
“As long as the patient is on excellent medical therapy, percutaneous coronary intervention [PCI] or revascularization is not essential for management of these patients,” Dr. Sharma said. Results of the FREEDOM trial (Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease) are due in 2012, he said, and could either corroborate or contradict the BARI 2D findings.
▸ Bifurcation lesion trials. At Mt. Sinai, Dr. Sharma and his team have investigated the “kissing” stent—the simultaneous placement of two stents in the main and side branch vessels of a bifurcated lesion. This technique was validated in the Nordic Bifurcation Study (Circulation 2006;114:1955-61). More recent trials have determined the two-stent approach is “definitely not inferior, and maybe even better than the one-stent approach,” he said.
▸ Trials on timing of intervention. Dr. Sharma cited two trials—TIMACS (Timing of Intervention in Patients With Acute Coronary Syndromes; N. Engl. J. Med. 2009;360:2165-75) and ABOARD (Angioplasty to Blunt the Rise of Troponin in Acute Coronary Syndromes Randomized for an Immediate or Delayed Intervention; JAMA 2009;302:947-54)—that looked at timing of intervention in patients with acute coronary syndrome. The studies found similar results in patients who had intervention within 2 hours and those who waited 16-24 hours. “Clearly, it seems that to wait for 24 hours is the right approach in treatment of systemic lesions when the patient is hemodynamically stable,” Dr. Sharma said.
▸ Percutaneous heart valve trials. The PARTNER (Placement of Aortic Transcatheter Valve) trial, estimated to be completed in 2014, is comparing transcatheter valvuloplasty with conventional heart valve replacement. Outcomes have improved since the study began enrolling patients in 2007, Dr. Sharma said. “The percutaneous valve field will continue to evolve,” he said.
▸ HORIZONS-AMI trial. The HORIZONS-AMI (Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction) trial investigators concluded that paclitaxel-eluting stents significantly reduced the risk of restenosis in patients with STEMI when compared with bare-metal stents (N. Engl. J. Med. 2009;360:1946-59). “This shows that drug-eluting stents are acceptable in systemic patients,” Dr. Sharma said.
▸ FAME trial. The Fractional Flow Reserve vs. Angiography for Guiding PCI in Patients with Multivessel Coronary Artery Disease trial (N. Engl. J. Med. 2009;360:213-24) looked at using fractional flow reserve (FFR) as an alternative to angiography for stent placement. It found that routinely measuring FFR in patients with multivessel disease for PCI with drug-eluting stents reduced the rate of death, MI, and repeat revascularization at 1 year. “At 1 year, fractional flow reserve is beneficial,” he said.
▸ Drug-eluting stent comparison trials. As trials move into second-generation drug-eluting stents, outcomes are comparing more favorably with those of bare-metal stents, Dr. Sharma said. A breakthrough comparative study of drug-eluting stents concluded that newer designs had advantages over then Food and Drug Administration–approved devices in terms of arterial healing and recovery (J. Am. Coll. Cardiol. 2008;52:333-42). He also cited the ENDEAVOR-IV trial, which showed that the zotarolimus-eluting stent had significantly lower rates of cardiac death and heart attack than did the paclitaxel-eluting Taxus stent after 3 years. Other trials are comparing other drug-eluting stents, he said. “The real issue is late stent thrombosis after 1 year,” he said.
▸ The PLATO trial. The Study of Platelet Inhibition and Patient Outcomes (N. Engl. J. Med. 2009;361:1045-57) trial found that ticagrelor had a significantly lower rate of death from vascular causes, heart attack, or stroke when compared with clopidogrel, with no increase in the overall bleeding rate. “It looks like we have a home run once this drug gets approved,” Dr. Sharma said.
▸ Unprotected left main coronary artery studies. The SYNTAX trial (N. Engl. J. Med. 2009;360:961-72) compared the paclitaxel-eluting Taxus stent with coronary artery bypass grafting (CABG) for atherosclerosis. While the findings confirmed CABG as the standard of care for three-vessel or left main coronary artery disease, Dr. Sharma said that PCI for left main coronary artery disease has shown steadily improving outcomes.
Updated American College of Cardiology/American Heart Association guidelines have elevated PCI for left main coronary artery disease to a class IIb indication from class III for patients at high risk of surgery, Dr. Sharma said. “But I am disappointed they did not take it into consideration for ostial left main disease,” he added. The EXCEL (Evaluation of Xience Prime Versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization) trial, which began enrolling patients this year, will provide what Dr. Sharma called “the final answer” on the use of PCI in left main coronary artery disease.
Dr. Sharma has received honoraria from Boston Scientific Corp., Abbott Laboratories, and the Medicines Company.
PCI for left main coronary artery disease has shown steadily improving outcomes.
Source DR. SHARMA
NEW YORK — Findings in 10 key investigative areas, from platelet inhibition and left main coronary artery disease to the use of fractional flow reserves and the “kissing” stent could have a profound impact on interventional cardiology in the next year or so.
Dr. Samin K. Sharma, co-director of the Cardiovascular Institute at Mt. Sinai Medical Center in New York, provided his take on these findings:
▸ Clopidogrel resistance and proton pump inhibitor interaction studies. In March, the FDA issued a warning that clopidogrel, widely prescribed to patients who have had an MI or stroke, is not as effective in people who cannot metabolize the drug. Dr. Sharma cited numerous reports that have shown that PPI drugs inhibit the activity of clopidogrel. In the clinic, physicians can test patients for platelet inhibition and use those data accordingly to modify dosing of the PPI.
“Avoid routine use of PPI with clopidogrel,” Dr. Sharma said. “If proton pump inhibition is needed, use H2 receptor blockers instead. If you need to use a PPI, many studies have shown it to be safer to use clopidogrel in the morning and the PPI in evening.” In high-risk patients, he advised using a 600-mg loading dose of PPI, then 150 mg daily. While genetic testing may help identify vulnerable groups, he added, it's “a very complex issue cost wise.”
▸ BARI 2D trial. The Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI 2D) found that prompt revascularization offered no significant advantages over medical therapy in terms of mortality and cardiovascular events for diabetes patients (N. Engl. J. Med. 2009;260:2503-15). The BARI 2D findings replicated those of the COURAGE trial (Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation; N. Engl. J. Med. 2007;356:1503-16), Dr. Sharma noted.
“As long as the patient is on excellent medical therapy, percutaneous coronary intervention [PCI] or revascularization is not essential for management of these patients,” Dr. Sharma said. Results of the FREEDOM trial (Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease) are due in 2012, he said, and could either corroborate or contradict the BARI 2D findings.
▸ Bifurcation lesion trials. At Mt. Sinai, Dr. Sharma and his team have investigated the “kissing” stent—the simultaneous placement of two stents in the main and side branch vessels of a bifurcated lesion. This technique was validated in the Nordic Bifurcation Study (Circulation 2006;114:1955-61). More recent trials have determined the two-stent approach is “definitely not inferior, and maybe even better than the one-stent approach,” he said.
▸ Trials on timing of intervention. Dr. Sharma cited two trials—TIMACS (Timing of Intervention in Patients With Acute Coronary Syndromes; N. Engl. J. Med. 2009;360:2165-75) and ABOARD (Angioplasty to Blunt the Rise of Troponin in Acute Coronary Syndromes Randomized for an Immediate or Delayed Intervention; JAMA 2009;302:947-54)—that looked at timing of intervention in patients with acute coronary syndrome. The studies found similar results in patients who had intervention within 2 hours and those who waited 16-24 hours. “Clearly, it seems that to wait for 24 hours is the right approach in treatment of systemic lesions when the patient is hemodynamically stable,” Dr. Sharma said.
▸ Percutaneous heart valve trials. The PARTNER (Placement of Aortic Transcatheter Valve) trial, estimated to be completed in 2014, is comparing transcatheter valvuloplasty with conventional heart valve replacement. Outcomes have improved since the study began enrolling patients in 2007, Dr. Sharma said. “The percutaneous valve field will continue to evolve,” he said.
▸ HORIZONS-AMI trial. The HORIZONS-AMI (Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction) trial investigators concluded that paclitaxel-eluting stents significantly reduced the risk of restenosis in patients with STEMI when compared with bare-metal stents (N. Engl. J. Med. 2009;360:1946-59). “This shows that drug-eluting stents are acceptable in systemic patients,” Dr. Sharma said.
▸ FAME trial. The Fractional Flow Reserve vs. Angiography for Guiding PCI in Patients with Multivessel Coronary Artery Disease trial (N. Engl. J. Med. 2009;360:213-24) looked at using fractional flow reserve (FFR) as an alternative to angiography for stent placement. It found that routinely measuring FFR in patients with multivessel disease for PCI with drug-eluting stents reduced the rate of death, MI, and repeat revascularization at 1 year. “At 1 year, fractional flow reserve is beneficial,” he said.
▸ Drug-eluting stent comparison trials. As trials move into second-generation drug-eluting stents, outcomes are comparing more favorably with those of bare-metal stents, Dr. Sharma said. A breakthrough comparative study of drug-eluting stents concluded that newer designs had advantages over then Food and Drug Administration–approved devices in terms of arterial healing and recovery (J. Am. Coll. Cardiol. 2008;52:333-42). He also cited the ENDEAVOR-IV trial, which showed that the zotarolimus-eluting stent had significantly lower rates of cardiac death and heart attack than did the paclitaxel-eluting Taxus stent after 3 years. Other trials are comparing other drug-eluting stents, he said. “The real issue is late stent thrombosis after 1 year,” he said.
▸ The PLATO trial. The Study of Platelet Inhibition and Patient Outcomes (N. Engl. J. Med. 2009;361:1045-57) trial found that ticagrelor had a significantly lower rate of death from vascular causes, heart attack, or stroke when compared with clopidogrel, with no increase in the overall bleeding rate. “It looks like we have a home run once this drug gets approved,” Dr. Sharma said.
▸ Unprotected left main coronary artery studies. The SYNTAX trial (N. Engl. J. Med. 2009;360:961-72) compared the paclitaxel-eluting Taxus stent with coronary artery bypass grafting (CABG) for atherosclerosis. While the findings confirmed CABG as the standard of care for three-vessel or left main coronary artery disease, Dr. Sharma said that PCI for left main coronary artery disease has shown steadily improving outcomes.
Updated American College of Cardiology/American Heart Association guidelines have elevated PCI for left main coronary artery disease to a class IIb indication from class III for patients at high risk of surgery, Dr. Sharma said. “But I am disappointed they did not take it into consideration for ostial left main disease,” he added. The EXCEL (Evaluation of Xience Prime Versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization) trial, which began enrolling patients this year, will provide what Dr. Sharma called “the final answer” on the use of PCI in left main coronary artery disease.
Dr. Sharma has received honoraria from Boston Scientific Corp., Abbott Laboratories, and the Medicines Company.
PCI for left main coronary artery disease has shown steadily improving outcomes.
Source DR. SHARMA