User login
Medicare’s revaluation of gastrointestinal endoscopic procedures: Implications for academic and community-based practices
No sentient gastroenterologist has missed the fact that, over the past 3 years, Medicare revalued our endoscopy codes. The impact of those reimbursement changes has been felt both by community gastroenterologists and by those practicing in academic centers. Impacts are different, however, because funds flow, opportunities for ancillary income and compensation formulas all are different for private versus academic physicians. In this month’s Road Ahead column, I have invited leaders from both camps (private practice and academic GI) to describe how reduced procedural reimbursement is affecting their practices. I was impressed and surprised at the level of detail and analysis provided by Dr. Dorn and Dr. Vesy. There are few other sources of financial data that are embedded in real-world experience. We all are concerned about our futures, and this article should spur us into serious discussions about practice strategies going forward. As I wrote in a recent article in Gastroenterology (2016;150:295-9), this is “No Time for WIMPs.”
Gastroenterology practices generate the bulk of their revenue from endoscopic procedures. Over the past decade, the professional fees Medicare pays for these procedures have generally declined. Meanwhile, associated hospital outpatient facility fees have increased while ambulatory surgery center (ASC) fees remain below 2007 levels. This article surveys these changes and examines their significant impact on academic and private gastroenterology practices.
Professional fees for endoscopic procedures
Since 1992 physician professional fees have been linked to the Medicare Physician Fee Schedule, which assigns each service a certain number of relative value units (RVUs). First, the work RVU (wRVU) is based on the estimated physician time, mental effort, technical skill, and psychological stress required to provide a service. Second, a practice expense RVU (PE RVU) reflects the direct and indirect costs of providing the service. For procedures performed in office-based settings the PE RVU includes rent, nonclinician staff, equipment, and supplies, on average amounting to 44% of the total RVU. For procedures performed in hospital outpatient departments (HOPDs) and ASCs, the PE RVU is much lower, because most costs are incurred by the facility (which receives a separate facility fee), rather than the physician practice. Third, a small proportion of the overall RVU is linked to malpractice insurance costs (MP RVU). The RVU components are geographically adjusted, combined, and then multiplied by a conversion factor (CF, which in 2016 is $35.80) to determine actual Medicare payment (Payment = [wRVU + PE RVU + MP RVU] × CF).1
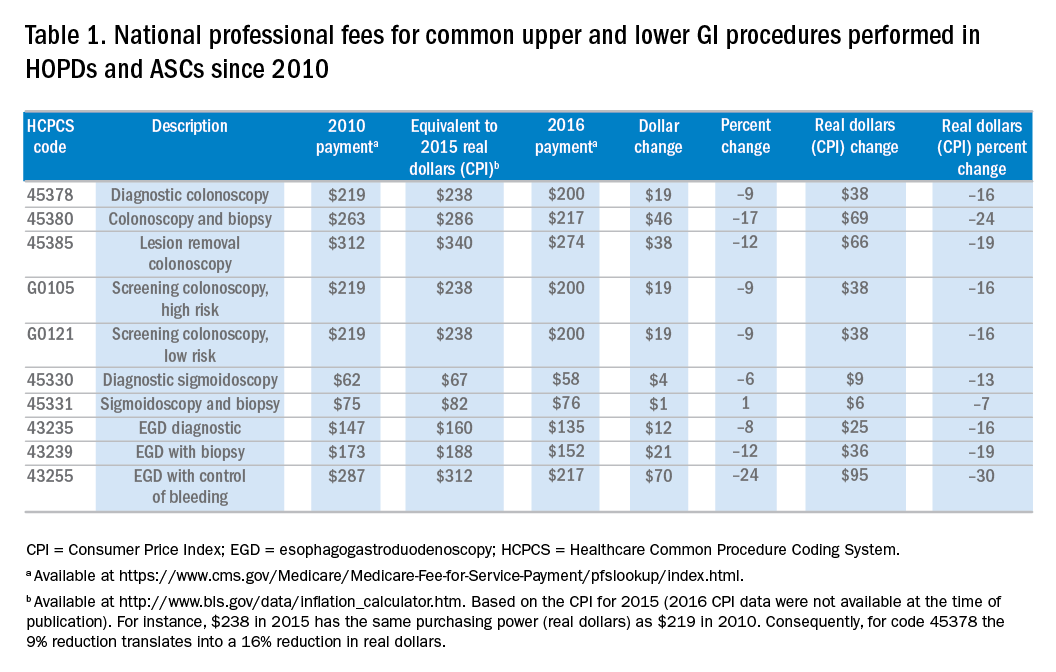
To address potential distortions in this physician fee schedule, The Affordable Care Act directed the Secretary of Health and Human Services to establish a formal process to review potentially misvalued procedure codes. During 2012 and 2014, multiple gastroenterological and surgical societies surveyed practicing physicians on the physician work, time, and intensity required to perform more than 120 services in question, including esophagoscopy, esophagogastroduodenoscopy, endoscopic retrograde cholangiopancreatography, flexible sigmoidoscopy and ileoscopy, pouchoscopy, and colonoscopy. At the same time, these societies assembled an expert panel of practicing physicians to determine the practice expenses associated with these procedures. The societies analyzed the results and presented recommendations to the American Medical Association/Specialty Society Relative Value Scale Update Committee, which, in turn, presented their recommendations to the Centers for Medicare and Medicaid Services.2 In 2014, CMS accepted approximately three-quarters of the Relative Value Scale Update Committee’s recommendations, ultimately decreasing wRVUs, increasing PE RVUs for procedures performed in office-based settings, and leaving MP RVUs unchanged for most upper endoscopy and endoscopic retrograde cholangiopancreatography procedures. These changes translated into significant 2015 payment reductions for esophagoscopy and esophagogastroduodenoscopy (4%-42%), endoscopic ultrasound (10%-35%), and endoscopic retrograde cholangiopancreatography (0%-37%) performed within facilities, with less effect for those performed in office-based settings. At that time, “in light of the substantial nature of [the colonoscopy] code revision and its relationship to the policies on moderate sedation,” CMS delayed revaluation of the lower gastrointestinal (GI) endoscopy codes.3 This reprieve is now over: The 2016 Medicare Physician Fee Schedule Final Rule includes up to 17% cuts (12% on average) to the wRVU associated with these lower GI procedures (Table 1). For office-based procedures (but not facility-based procedures) these wRVU cuts are buffered (and sometimes offset) by general increases in PE RVUs.
Facility fees for endoscopic procedures
Compared with the small percentage of endoscopic procedures that are performed in office-based settings, those performed in HOPDs and ASCs entail a lower professional fee plus a separate facility fee. Since 2000 CMS has paid for services provided in HOPDs using the outpatient prospective payment system (OPPS). Clinical services are first classified into ambulatory payment classifications (APC) on the basis of clinical and cost similarity. Next, services within an APC are assigned a single relative payment rate, which is linked to the resources required to perform the service. The APC payment rate is geographically adjusted and then multiplied by a CF to determine an actual dollar amount.4
Since 2008, CMS has used a nearly identical mechanism to pay for facility services provided in ASCs. Services are classified using the same APCs and same relative weights as the OPPS. The difference is that the ASC CF is less than the OPPS CF (the 2016 ASC CF is 58% of the OPPS CF), translating into lower dollar payments for ASC services.5 Of note, in 2008 ASC rates were cut significantly when CMS adopted this methodology for determining ASC facility fees (previously, ASC rates were approximately 85% of HOPD rates).
CMS reviews the APCs and their relative weights annually, and may adjust how specific services are classified and how APCs are weighed. Since 2006, HOPD rates for the 10 common procedures listed in Table 1 have increased by 26%-93% real (i.e., Consumer Price Index–adjusted) dollars. Meanwhile, given the steep 2008 ASC fee cuts the 2016 ASC fees are still significantly lower than they were 1 decade ago, especially when accounting for inflation. In fact, ASC fees for the most common procedures have decreased by 20% in real dollars (Supplementary Tables 1 and 2 at http://dx.doi.org/10.1016/j.cgh.2016.03.032).
Putting these changes in context
It is important to consider these changes within a broader context. First, the full economic impact of these changes on an individual gastroenterology practice depends on where it performs its services and whether it collects associated facility fees, and fees for anesthesia and pathology services. Second, the Medicare population is growing by more than 10,000 people each day.6 Third, beyond Medicare, most commercial insurers peg their reimbursement rates to a percentage of the Medicare Fee Schedule. Although the details of specific contracts vary, gastroenterologists should expect to see commercial rates move in a similar direction within the next 1–2 years. Fourth, in the 2016 Fee Schedule CMS described its future intention to remove the value of moderate sedation from all GI procedures valued with moderate sedation inherent to the procedure. The more that moderate sedation is ultimately valued, the less that endoscopic procedures will be valued. Consequently, gastroenterologists who rely on anesthesiology professionals to sedate their patients will receive less revenue per procedure. Finally, the 2015 Medicare Access and Children’s Health Insurance Program Reauthorization Act (MACRA) links a higher proportion of these dwindling fee-for-service payments to performance. Starting in 2018, physicians who elect to remain on a fee-for-service tract will receive a composite Merit-Based Incentive Payment System (MIPS) score that will translate into either performance bonuses or penalties (as much as 4% in 2019 and going up to 9% in 2022). Alternatively, providers who “sufficiently” participate in “two-sided” (i.e., risk-bearing) alternative payment models (e.g., bundled payments and accountable care organizations) instead of fee-for-service payments will receive 5% across-the-board bonuses. In sum, it is possible that fee-for-service payments may eventually become so unattractive that many gastroenterologists decide (or hope) to move to alternative payment models that combine both professional and facility fees, such as the CMS now-mandatory Comprehensive Care for Joint Replacement (CJR) program.7
Impact on academic practices
For most academic gastroenterology practices, clinical revenue far exceeds all other sources of funding, including research grants, teaching support, philanthropy, and partnerships with industry. Although a select few academic GI divisions have managed to build their own ASCs to share facility fees, for most academic practices, clinical revenue comes solely from the professional fees for endoscopic procedures and, less so, from office and hospital-based consultations and management of established patients.8 Thus, steep cuts to professional fees for endoscopic procedures, the leading source of overall revenue, will severely strain most academic gastroenterology practices.
In one of our practices (SDD), the 10 common procedures listed in Table 1 accounted for 27% of total direct clinical revenue over the past year. Roughly one-fourth of our patients are Medicare beneficiaries. Assuming no change in volume, the 2016 fee schedule cuts will amount to a 0.9% drop in direct clinical revenue. If all other payers follow with identical cuts, then direct clinical revenue will drop by 3.7%. Although our practice is fortunate to have other well-developed clinical and nonclinical revenue streams, these cuts are not insignificant.
How can academic practices continue to provide accessible clinical care in the face of these fee cuts? It can help to first consider how revenue is distributed for a Medicare beneficiary who undergoes a diagnostic colonoscopy with biopsy to evaluate unexplained diarrhea in an academic medical center’s hospital-based facility. The academic gastroenterologist receives $212 (CPT 45380). From this $212, the academic gastroenterology practice must pay assessments to various entities (sometimes including the school of medicine, department of medicine, and faculty practice plan) that may amount to more than 30% of total revenue. The roughly $150 that remains is used to pay faculty member salaries (the median salary for an academic gastroenterologist is $300,009) and benefits (estimated at $74,000/year); MP insurance (estimated at $2,275/year, higher in certain parts of the United States); and overhead for support staff, supplies, and other expenses (estimated at $50,550/year). Thus, a purely clinical academic gastroenterologist who is paid at the Medical Group Management Association (MGMA) median must generate $610,179 in preassessment revenue. If this hypothetical academic gastroenterologist solely treated Medicare beneficiaries, at $35.82 per RVU he or she would need to generate a staggering 17,035 RVUs per year, an amount that far exceeds the MGMA median (6,445) and 90th percentile (10,991) for academic gastroenterologists. Of course, real-world academic gastroenterologists also treat commercially insured patients and many spend time on nonclinical activities (although clinical income typically supports time devoted to research and teaching, not vice versa). Still, this example highlights a clear fact: Academic gastroenterology practices take a major financial loss delivering services to Medicare beneficiaries. Meanwhile, the HOPD charges more than $2,200 for the procedure. Although it receives $752 facility fee from Medicare (Disproportionate Share Hospitals and NCI Cancer Centers receive more), with a cost-to-charge ratio of roughly 0.2, revenue still clearly exceeds expenses. Finally, the anesthesia professional (if any) receives roughly $198 (CPT 00810) and the pathologist $74 (CPT 88305).
Although some may argue that academic gastroenterologists should simply accept a pay cut, lower salaries may drive many away from academia. To hire enough new (or even maintain enough existing) faculty members to maintain and grow volume, academic gastroenterology practices must find ways to supplement declining professional fees. One option is for academic practices to open their own ASCs, either alone or jointly with their health care system. But this assumes, often erroneously, that the health care system is willing to share facility fees. A second option is to develop incentive programs that transfer revenue from the health care system to the physicians. Importantly, these must be at fair market value and for nonemployed physicians cannot be linked to volume.10 Examples include medical directorships and non–volume-based performance bonuses. A third option is to consider alternative payment models, such as bundled payments that include a single lump sum payment for both professional and facility fees. The practice and health system then negotiates how the bundle is shared. Bundles should motivate hospitals and academic practices to work together to improve care and reduce overall expenses. Along these lines, CMS recently announced the CJR program under which hospitals and physicians in 75 locations will be required to participate. Although AGA recently published a bundled payment framework for screening and surveillance colonoscopy,11 bundles for other endoscopic procedures remain to be defined. But, a clearly defined, attractively priced, and skillfully negotiated bundle could be a means for redistributing revenue in ways that are more favorable to academic practices. No matter the approach, it is critical for academic gastroenterology practices and their health care systems to align their goals and integrate their services. But this is easier said than done.
Impact on private gastroenterology practices
The impact of these professional and facility fee changes on private practice depends on the practice’s payer mix, and whether it owns an ASC and directly provides anesthesia and pathology services. Consider Texas Digestive Disease Consultants (TDDC), an 80-gastroenterologist practice that provides GI care and endoscopic procedures throughout north and central Texas. TDDC revenue comes solely from professional fees generated by gastroenterologists and the pathologists that the practice employs. TDDC operating expenses include employee salaries and benefits, rent, and taxes. Based on an expected work-year of 2,080 hours, each TDDC gastroenterologist must generate $219 per hour to cover practice expenses. Physicians receive income only after practice revenue exceeds $219 per hour.
In the 2016 Medicare Physician Fee Schedule, colonoscopy code 45387 is assigned 3.36 RVUs, based on 67 minutes in total time. Based on this information, 2016 CMS payment for a screening colonoscopy ($200) will result in a loss of $45 in practice revenue over expenses. Across the TDDC practices in 2015, CMS patients represented 29% of all colonoscopies performed, but only 11% of revenue from those procedures. In aggregate, assuming no change in volume, the 2016 fee schedule cuts will translate into $5,472 less physician income for each gastroenterologist. If all other payers follow with identical cuts then each gastroenterologist would forfeit $50,896 of income.
For pathology services, code 88305 reimburses a global service per specimen. The average number of specimens per outpatient GI procedure at TDDC is 1.5. Based on CMS’ per specimen payment of $73 (down from $107 in 2012), average pathology reimbursement per a CMS endoscopic procedure is $110.
What about facility fees? Many TDDC physicians separately own and operate ASCs and anesthesia practices. Because the physician owners of these facilities funded, developed, and operate these facilities on their own, any revenue over expenses from these facilities flow directly to the ASC, rather than to TDDC. Since 2008, when ASC payments were severely reduced, ASC revenue over expenses for a Medicare colonoscopy has ranged from $0 to $70. For anesthesia services, the ASC receives approximately $159 per screening colonoscopy, which is not enough to actually cover the costs of providing anesthesia services. In sum, when TDDC gastroenterologists perform colonoscopies on Medicare patients at an HOPD the physician loses money. When the same procedure is performed at an ASC the physician barely break even.
How can private practice gastroenterologists respond to these fee cuts? First, some gastroenterologists may be forced to accept lower salaries. Second, practices can offset fee cuts by improving efficiency and reducing overall cost of care, assuming they are not already maximally efficient. Third, some private practices can increase Medicare professional payments by reclassifying as nonparticipating with Medicare. Nonparticipating status allows practices to charge the patient up to approximately 109.25% of the Medicare approved rate, with the patient submitting the claim directly to Medicare (“balance billing”). The downside is that patients shoulder the additional cost and may potentially decide to seek care elsewhere. Fourth, private practices should explore alternative payment models, such as bundled payment as described previously, either on their own or by partnering with local health systems to share risk. Finally, some practices may sell equity to and become employees of local health systems.
Conclusions
Changes to Medicare professional and facility fee payments for endoscopic procedures significantly affect academic and private gastroenterology practices. Dwindling professional fees – alongside increasing HOPD facility fees – make academic gastroenterology practices increasingly reliant on support from their parent health care systems. Like academic practices, private gastroenterology practices experience financial losses when treating Medicare beneficiaries. Academic and private gastroenterology practices should consider several potential responses. Although beyond the scope of this article, all practices must continuously strive to improve the quality and reduce the costs of the endoscopic procedures they perform.
Acknowledgments
The authors thank Leslie Narramore, MPA, for her insights and help with reimbursement data. They also thank Bryan Rhodes for providing financial data and Shivan Mehta, MD, MBA, for his feedback on the Relative Value Scale Update Committee process.
References
1. MEDPAC. Payment basics: physician and other health professional payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
2. Mehta, S.J., Brill, J.V. What is the RUC and how does it impact gastroenterology?. Clin Gastroenterol Hepatol. 2014;12:1208-11.
3. American College of Gastroenterology, American Gastroenterological Association, American Society for Gastrointestinal Endoscopy. Key Provisions in the CY 2015 Medicare Physician Fee Schedule Final Rule, 2015. Available at: http://gi.org/wp-content/uploads/2014/11/Tri-Soc_CY15_MPFS_Final_Rule_Summary.pdf.
4. MEDPAC. Payment basics: Outpatient hospital services payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
5. MEDPAC. Payment basics: Ambulatory surgery center services payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
6. Diamond, D. 10,000 people are now enrolling in Medicare – every day. Forbes; 2015 (Available at: http://www.forbes.com/sites/dandiamond/2015/07/13/aging-in-america-10000-people-enroll-in-medicare-every-day/#5177f1f35e07. Accessed January 3, 2016)
7. Mechanic, R.E. Mandatory Medicare bundled payment: Is it ready for prime time?. N Engl J Med. 2015;373:1291-3.
8. Rustgi, A.K., Allen, J.I. The house of gastrointestinal medicine: How academic medical centers can build a sustainable economic clinical model. Clin Gastroenterol Hepatol. 2013;11:1370-3.
9. Academic Practice Compensation and Production Report. Medical Group Management Association, Englewood, Colo.; 2015.
10. Becker S., Townshend G., Carnell H., et al. Physician compensation: 10 core legal and regulatory concepts. Becker’s Hospital Review Available at: http://www.beckershospitalreview.com/legal-regulatory-issues/physician-compensation-10-core-legal-and-regulatory-concepts.html. Accessed Jan. 20, 2016.
11. Brill, J.V., Jain, R., Margolis, P.S., et al. A bundled payment framework for colonoscopy performed for colorectal cancer screening or surveillance. Gastroenterology. 2014;146:849-53, e9.
Dr. Dorn is vice chief, division of gastroenterology and hepatology, associate professor of medicine, health policy & management, University of North Carolina at Chapel Hill; he has received honoraria for consulting and presentations on health reform from AbbVie and Olympus. Dr. Vesy is a gastroenterologist affiliated with Baylor University Medical Center, Dallas.
No sentient gastroenterologist has missed the fact that, over the past 3 years, Medicare revalued our endoscopy codes. The impact of those reimbursement changes has been felt both by community gastroenterologists and by those practicing in academic centers. Impacts are different, however, because funds flow, opportunities for ancillary income and compensation formulas all are different for private versus academic physicians. In this month’s Road Ahead column, I have invited leaders from both camps (private practice and academic GI) to describe how reduced procedural reimbursement is affecting their practices. I was impressed and surprised at the level of detail and analysis provided by Dr. Dorn and Dr. Vesy. There are few other sources of financial data that are embedded in real-world experience. We all are concerned about our futures, and this article should spur us into serious discussions about practice strategies going forward. As I wrote in a recent article in Gastroenterology (2016;150:295-9), this is “No Time for WIMPs.”
Gastroenterology practices generate the bulk of their revenue from endoscopic procedures. Over the past decade, the professional fees Medicare pays for these procedures have generally declined. Meanwhile, associated hospital outpatient facility fees have increased while ambulatory surgery center (ASC) fees remain below 2007 levels. This article surveys these changes and examines their significant impact on academic and private gastroenterology practices.
Professional fees for endoscopic procedures
Since 1992 physician professional fees have been linked to the Medicare Physician Fee Schedule, which assigns each service a certain number of relative value units (RVUs). First, the work RVU (wRVU) is based on the estimated physician time, mental effort, technical skill, and psychological stress required to provide a service. Second, a practice expense RVU (PE RVU) reflects the direct and indirect costs of providing the service. For procedures performed in office-based settings the PE RVU includes rent, nonclinician staff, equipment, and supplies, on average amounting to 44% of the total RVU. For procedures performed in hospital outpatient departments (HOPDs) and ASCs, the PE RVU is much lower, because most costs are incurred by the facility (which receives a separate facility fee), rather than the physician practice. Third, a small proportion of the overall RVU is linked to malpractice insurance costs (MP RVU). The RVU components are geographically adjusted, combined, and then multiplied by a conversion factor (CF, which in 2016 is $35.80) to determine actual Medicare payment (Payment = [wRVU + PE RVU + MP RVU] × CF).1
To address potential distortions in this physician fee schedule, The Affordable Care Act directed the Secretary of Health and Human Services to establish a formal process to review potentially misvalued procedure codes. During 2012 and 2014, multiple gastroenterological and surgical societies surveyed practicing physicians on the physician work, time, and intensity required to perform more than 120 services in question, including esophagoscopy, esophagogastroduodenoscopy, endoscopic retrograde cholangiopancreatography, flexible sigmoidoscopy and ileoscopy, pouchoscopy, and colonoscopy. At the same time, these societies assembled an expert panel of practicing physicians to determine the practice expenses associated with these procedures. The societies analyzed the results and presented recommendations to the American Medical Association/Specialty Society Relative Value Scale Update Committee, which, in turn, presented their recommendations to the Centers for Medicare and Medicaid Services.2 In 2014, CMS accepted approximately three-quarters of the Relative Value Scale Update Committee’s recommendations, ultimately decreasing wRVUs, increasing PE RVUs for procedures performed in office-based settings, and leaving MP RVUs unchanged for most upper endoscopy and endoscopic retrograde cholangiopancreatography procedures. These changes translated into significant 2015 payment reductions for esophagoscopy and esophagogastroduodenoscopy (4%-42%), endoscopic ultrasound (10%-35%), and endoscopic retrograde cholangiopancreatography (0%-37%) performed within facilities, with less effect for those performed in office-based settings. At that time, “in light of the substantial nature of [the colonoscopy] code revision and its relationship to the policies on moderate sedation,” CMS delayed revaluation of the lower gastrointestinal (GI) endoscopy codes.3 This reprieve is now over: The 2016 Medicare Physician Fee Schedule Final Rule includes up to 17% cuts (12% on average) to the wRVU associated with these lower GI procedures (Table 1). For office-based procedures (but not facility-based procedures) these wRVU cuts are buffered (and sometimes offset) by general increases in PE RVUs.
Facility fees for endoscopic procedures
Compared with the small percentage of endoscopic procedures that are performed in office-based settings, those performed in HOPDs and ASCs entail a lower professional fee plus a separate facility fee. Since 2000 CMS has paid for services provided in HOPDs using the outpatient prospective payment system (OPPS). Clinical services are first classified into ambulatory payment classifications (APC) on the basis of clinical and cost similarity. Next, services within an APC are assigned a single relative payment rate, which is linked to the resources required to perform the service. The APC payment rate is geographically adjusted and then multiplied by a CF to determine an actual dollar amount.4
Since 2008, CMS has used a nearly identical mechanism to pay for facility services provided in ASCs. Services are classified using the same APCs and same relative weights as the OPPS. The difference is that the ASC CF is less than the OPPS CF (the 2016 ASC CF is 58% of the OPPS CF), translating into lower dollar payments for ASC services.5 Of note, in 2008 ASC rates were cut significantly when CMS adopted this methodology for determining ASC facility fees (previously, ASC rates were approximately 85% of HOPD rates).
CMS reviews the APCs and their relative weights annually, and may adjust how specific services are classified and how APCs are weighed. Since 2006, HOPD rates for the 10 common procedures listed in Table 1 have increased by 26%-93% real (i.e., Consumer Price Index–adjusted) dollars. Meanwhile, given the steep 2008 ASC fee cuts the 2016 ASC fees are still significantly lower than they were 1 decade ago, especially when accounting for inflation. In fact, ASC fees for the most common procedures have decreased by 20% in real dollars (Supplementary Tables 1 and 2 at http://dx.doi.org/10.1016/j.cgh.2016.03.032).
Putting these changes in context
It is important to consider these changes within a broader context. First, the full economic impact of these changes on an individual gastroenterology practice depends on where it performs its services and whether it collects associated facility fees, and fees for anesthesia and pathology services. Second, the Medicare population is growing by more than 10,000 people each day.6 Third, beyond Medicare, most commercial insurers peg their reimbursement rates to a percentage of the Medicare Fee Schedule. Although the details of specific contracts vary, gastroenterologists should expect to see commercial rates move in a similar direction within the next 1–2 years. Fourth, in the 2016 Fee Schedule CMS described its future intention to remove the value of moderate sedation from all GI procedures valued with moderate sedation inherent to the procedure. The more that moderate sedation is ultimately valued, the less that endoscopic procedures will be valued. Consequently, gastroenterologists who rely on anesthesiology professionals to sedate their patients will receive less revenue per procedure. Finally, the 2015 Medicare Access and Children’s Health Insurance Program Reauthorization Act (MACRA) links a higher proportion of these dwindling fee-for-service payments to performance. Starting in 2018, physicians who elect to remain on a fee-for-service tract will receive a composite Merit-Based Incentive Payment System (MIPS) score that will translate into either performance bonuses or penalties (as much as 4% in 2019 and going up to 9% in 2022). Alternatively, providers who “sufficiently” participate in “two-sided” (i.e., risk-bearing) alternative payment models (e.g., bundled payments and accountable care organizations) instead of fee-for-service payments will receive 5% across-the-board bonuses. In sum, it is possible that fee-for-service payments may eventually become so unattractive that many gastroenterologists decide (or hope) to move to alternative payment models that combine both professional and facility fees, such as the CMS now-mandatory Comprehensive Care for Joint Replacement (CJR) program.7
Impact on academic practices
For most academic gastroenterology practices, clinical revenue far exceeds all other sources of funding, including research grants, teaching support, philanthropy, and partnerships with industry. Although a select few academic GI divisions have managed to build their own ASCs to share facility fees, for most academic practices, clinical revenue comes solely from the professional fees for endoscopic procedures and, less so, from office and hospital-based consultations and management of established patients.8 Thus, steep cuts to professional fees for endoscopic procedures, the leading source of overall revenue, will severely strain most academic gastroenterology practices.
In one of our practices (SDD), the 10 common procedures listed in Table 1 accounted for 27% of total direct clinical revenue over the past year. Roughly one-fourth of our patients are Medicare beneficiaries. Assuming no change in volume, the 2016 fee schedule cuts will amount to a 0.9% drop in direct clinical revenue. If all other payers follow with identical cuts, then direct clinical revenue will drop by 3.7%. Although our practice is fortunate to have other well-developed clinical and nonclinical revenue streams, these cuts are not insignificant.
How can academic practices continue to provide accessible clinical care in the face of these fee cuts? It can help to first consider how revenue is distributed for a Medicare beneficiary who undergoes a diagnostic colonoscopy with biopsy to evaluate unexplained diarrhea in an academic medical center’s hospital-based facility. The academic gastroenterologist receives $212 (CPT 45380). From this $212, the academic gastroenterology practice must pay assessments to various entities (sometimes including the school of medicine, department of medicine, and faculty practice plan) that may amount to more than 30% of total revenue. The roughly $150 that remains is used to pay faculty member salaries (the median salary for an academic gastroenterologist is $300,009) and benefits (estimated at $74,000/year); MP insurance (estimated at $2,275/year, higher in certain parts of the United States); and overhead for support staff, supplies, and other expenses (estimated at $50,550/year). Thus, a purely clinical academic gastroenterologist who is paid at the Medical Group Management Association (MGMA) median must generate $610,179 in preassessment revenue. If this hypothetical academic gastroenterologist solely treated Medicare beneficiaries, at $35.82 per RVU he or she would need to generate a staggering 17,035 RVUs per year, an amount that far exceeds the MGMA median (6,445) and 90th percentile (10,991) for academic gastroenterologists. Of course, real-world academic gastroenterologists also treat commercially insured patients and many spend time on nonclinical activities (although clinical income typically supports time devoted to research and teaching, not vice versa). Still, this example highlights a clear fact: Academic gastroenterology practices take a major financial loss delivering services to Medicare beneficiaries. Meanwhile, the HOPD charges more than $2,200 for the procedure. Although it receives $752 facility fee from Medicare (Disproportionate Share Hospitals and NCI Cancer Centers receive more), with a cost-to-charge ratio of roughly 0.2, revenue still clearly exceeds expenses. Finally, the anesthesia professional (if any) receives roughly $198 (CPT 00810) and the pathologist $74 (CPT 88305).
Although some may argue that academic gastroenterologists should simply accept a pay cut, lower salaries may drive many away from academia. To hire enough new (or even maintain enough existing) faculty members to maintain and grow volume, academic gastroenterology practices must find ways to supplement declining professional fees. One option is for academic practices to open their own ASCs, either alone or jointly with their health care system. But this assumes, often erroneously, that the health care system is willing to share facility fees. A second option is to develop incentive programs that transfer revenue from the health care system to the physicians. Importantly, these must be at fair market value and for nonemployed physicians cannot be linked to volume.10 Examples include medical directorships and non–volume-based performance bonuses. A third option is to consider alternative payment models, such as bundled payments that include a single lump sum payment for both professional and facility fees. The practice and health system then negotiates how the bundle is shared. Bundles should motivate hospitals and academic practices to work together to improve care and reduce overall expenses. Along these lines, CMS recently announced the CJR program under which hospitals and physicians in 75 locations will be required to participate. Although AGA recently published a bundled payment framework for screening and surveillance colonoscopy,11 bundles for other endoscopic procedures remain to be defined. But, a clearly defined, attractively priced, and skillfully negotiated bundle could be a means for redistributing revenue in ways that are more favorable to academic practices. No matter the approach, it is critical for academic gastroenterology practices and their health care systems to align their goals and integrate their services. But this is easier said than done.
Impact on private gastroenterology practices
The impact of these professional and facility fee changes on private practice depends on the practice’s payer mix, and whether it owns an ASC and directly provides anesthesia and pathology services. Consider Texas Digestive Disease Consultants (TDDC), an 80-gastroenterologist practice that provides GI care and endoscopic procedures throughout north and central Texas. TDDC revenue comes solely from professional fees generated by gastroenterologists and the pathologists that the practice employs. TDDC operating expenses include employee salaries and benefits, rent, and taxes. Based on an expected work-year of 2,080 hours, each TDDC gastroenterologist must generate $219 per hour to cover practice expenses. Physicians receive income only after practice revenue exceeds $219 per hour.
In the 2016 Medicare Physician Fee Schedule, colonoscopy code 45387 is assigned 3.36 RVUs, based on 67 minutes in total time. Based on this information, 2016 CMS payment for a screening colonoscopy ($200) will result in a loss of $45 in practice revenue over expenses. Across the TDDC practices in 2015, CMS patients represented 29% of all colonoscopies performed, but only 11% of revenue from those procedures. In aggregate, assuming no change in volume, the 2016 fee schedule cuts will translate into $5,472 less physician income for each gastroenterologist. If all other payers follow with identical cuts then each gastroenterologist would forfeit $50,896 of income.
For pathology services, code 88305 reimburses a global service per specimen. The average number of specimens per outpatient GI procedure at TDDC is 1.5. Based on CMS’ per specimen payment of $73 (down from $107 in 2012), average pathology reimbursement per a CMS endoscopic procedure is $110.
What about facility fees? Many TDDC physicians separately own and operate ASCs and anesthesia practices. Because the physician owners of these facilities funded, developed, and operate these facilities on their own, any revenue over expenses from these facilities flow directly to the ASC, rather than to TDDC. Since 2008, when ASC payments were severely reduced, ASC revenue over expenses for a Medicare colonoscopy has ranged from $0 to $70. For anesthesia services, the ASC receives approximately $159 per screening colonoscopy, which is not enough to actually cover the costs of providing anesthesia services. In sum, when TDDC gastroenterologists perform colonoscopies on Medicare patients at an HOPD the physician loses money. When the same procedure is performed at an ASC the physician barely break even.
How can private practice gastroenterologists respond to these fee cuts? First, some gastroenterologists may be forced to accept lower salaries. Second, practices can offset fee cuts by improving efficiency and reducing overall cost of care, assuming they are not already maximally efficient. Third, some private practices can increase Medicare professional payments by reclassifying as nonparticipating with Medicare. Nonparticipating status allows practices to charge the patient up to approximately 109.25% of the Medicare approved rate, with the patient submitting the claim directly to Medicare (“balance billing”). The downside is that patients shoulder the additional cost and may potentially decide to seek care elsewhere. Fourth, private practices should explore alternative payment models, such as bundled payment as described previously, either on their own or by partnering with local health systems to share risk. Finally, some practices may sell equity to and become employees of local health systems.
Conclusions
Changes to Medicare professional and facility fee payments for endoscopic procedures significantly affect academic and private gastroenterology practices. Dwindling professional fees – alongside increasing HOPD facility fees – make academic gastroenterology practices increasingly reliant on support from their parent health care systems. Like academic practices, private gastroenterology practices experience financial losses when treating Medicare beneficiaries. Academic and private gastroenterology practices should consider several potential responses. Although beyond the scope of this article, all practices must continuously strive to improve the quality and reduce the costs of the endoscopic procedures they perform.
Acknowledgments
The authors thank Leslie Narramore, MPA, for her insights and help with reimbursement data. They also thank Bryan Rhodes for providing financial data and Shivan Mehta, MD, MBA, for his feedback on the Relative Value Scale Update Committee process.
References
1. MEDPAC. Payment basics: physician and other health professional payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
2. Mehta, S.J., Brill, J.V. What is the RUC and how does it impact gastroenterology?. Clin Gastroenterol Hepatol. 2014;12:1208-11.
3. American College of Gastroenterology, American Gastroenterological Association, American Society for Gastrointestinal Endoscopy. Key Provisions in the CY 2015 Medicare Physician Fee Schedule Final Rule, 2015. Available at: http://gi.org/wp-content/uploads/2014/11/Tri-Soc_CY15_MPFS_Final_Rule_Summary.pdf.
4. MEDPAC. Payment basics: Outpatient hospital services payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
5. MEDPAC. Payment basics: Ambulatory surgery center services payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
6. Diamond, D. 10,000 people are now enrolling in Medicare – every day. Forbes; 2015 (Available at: http://www.forbes.com/sites/dandiamond/2015/07/13/aging-in-america-10000-people-enroll-in-medicare-every-day/#5177f1f35e07. Accessed January 3, 2016)
7. Mechanic, R.E. Mandatory Medicare bundled payment: Is it ready for prime time?. N Engl J Med. 2015;373:1291-3.
8. Rustgi, A.K., Allen, J.I. The house of gastrointestinal medicine: How academic medical centers can build a sustainable economic clinical model. Clin Gastroenterol Hepatol. 2013;11:1370-3.
9. Academic Practice Compensation and Production Report. Medical Group Management Association, Englewood, Colo.; 2015.
10. Becker S., Townshend G., Carnell H., et al. Physician compensation: 10 core legal and regulatory concepts. Becker’s Hospital Review Available at: http://www.beckershospitalreview.com/legal-regulatory-issues/physician-compensation-10-core-legal-and-regulatory-concepts.html. Accessed Jan. 20, 2016.
11. Brill, J.V., Jain, R., Margolis, P.S., et al. A bundled payment framework for colonoscopy performed for colorectal cancer screening or surveillance. Gastroenterology. 2014;146:849-53, e9.
Dr. Dorn is vice chief, division of gastroenterology and hepatology, associate professor of medicine, health policy & management, University of North Carolina at Chapel Hill; he has received honoraria for consulting and presentations on health reform from AbbVie and Olympus. Dr. Vesy is a gastroenterologist affiliated with Baylor University Medical Center, Dallas.
No sentient gastroenterologist has missed the fact that, over the past 3 years, Medicare revalued our endoscopy codes. The impact of those reimbursement changes has been felt both by community gastroenterologists and by those practicing in academic centers. Impacts are different, however, because funds flow, opportunities for ancillary income and compensation formulas all are different for private versus academic physicians. In this month’s Road Ahead column, I have invited leaders from both camps (private practice and academic GI) to describe how reduced procedural reimbursement is affecting their practices. I was impressed and surprised at the level of detail and analysis provided by Dr. Dorn and Dr. Vesy. There are few other sources of financial data that are embedded in real-world experience. We all are concerned about our futures, and this article should spur us into serious discussions about practice strategies going forward. As I wrote in a recent article in Gastroenterology (2016;150:295-9), this is “No Time for WIMPs.”
Gastroenterology practices generate the bulk of their revenue from endoscopic procedures. Over the past decade, the professional fees Medicare pays for these procedures have generally declined. Meanwhile, associated hospital outpatient facility fees have increased while ambulatory surgery center (ASC) fees remain below 2007 levels. This article surveys these changes and examines their significant impact on academic and private gastroenterology practices.
Professional fees for endoscopic procedures
Since 1992 physician professional fees have been linked to the Medicare Physician Fee Schedule, which assigns each service a certain number of relative value units (RVUs). First, the work RVU (wRVU) is based on the estimated physician time, mental effort, technical skill, and psychological stress required to provide a service. Second, a practice expense RVU (PE RVU) reflects the direct and indirect costs of providing the service. For procedures performed in office-based settings the PE RVU includes rent, nonclinician staff, equipment, and supplies, on average amounting to 44% of the total RVU. For procedures performed in hospital outpatient departments (HOPDs) and ASCs, the PE RVU is much lower, because most costs are incurred by the facility (which receives a separate facility fee), rather than the physician practice. Third, a small proportion of the overall RVU is linked to malpractice insurance costs (MP RVU). The RVU components are geographically adjusted, combined, and then multiplied by a conversion factor (CF, which in 2016 is $35.80) to determine actual Medicare payment (Payment = [wRVU + PE RVU + MP RVU] × CF).1
To address potential distortions in this physician fee schedule, The Affordable Care Act directed the Secretary of Health and Human Services to establish a formal process to review potentially misvalued procedure codes. During 2012 and 2014, multiple gastroenterological and surgical societies surveyed practicing physicians on the physician work, time, and intensity required to perform more than 120 services in question, including esophagoscopy, esophagogastroduodenoscopy, endoscopic retrograde cholangiopancreatography, flexible sigmoidoscopy and ileoscopy, pouchoscopy, and colonoscopy. At the same time, these societies assembled an expert panel of practicing physicians to determine the practice expenses associated with these procedures. The societies analyzed the results and presented recommendations to the American Medical Association/Specialty Society Relative Value Scale Update Committee, which, in turn, presented their recommendations to the Centers for Medicare and Medicaid Services.2 In 2014, CMS accepted approximately three-quarters of the Relative Value Scale Update Committee’s recommendations, ultimately decreasing wRVUs, increasing PE RVUs for procedures performed in office-based settings, and leaving MP RVUs unchanged for most upper endoscopy and endoscopic retrograde cholangiopancreatography procedures. These changes translated into significant 2015 payment reductions for esophagoscopy and esophagogastroduodenoscopy (4%-42%), endoscopic ultrasound (10%-35%), and endoscopic retrograde cholangiopancreatography (0%-37%) performed within facilities, with less effect for those performed in office-based settings. At that time, “in light of the substantial nature of [the colonoscopy] code revision and its relationship to the policies on moderate sedation,” CMS delayed revaluation of the lower gastrointestinal (GI) endoscopy codes.3 This reprieve is now over: The 2016 Medicare Physician Fee Schedule Final Rule includes up to 17% cuts (12% on average) to the wRVU associated with these lower GI procedures (Table 1). For office-based procedures (but not facility-based procedures) these wRVU cuts are buffered (and sometimes offset) by general increases in PE RVUs.
Facility fees for endoscopic procedures
Compared with the small percentage of endoscopic procedures that are performed in office-based settings, those performed in HOPDs and ASCs entail a lower professional fee plus a separate facility fee. Since 2000 CMS has paid for services provided in HOPDs using the outpatient prospective payment system (OPPS). Clinical services are first classified into ambulatory payment classifications (APC) on the basis of clinical and cost similarity. Next, services within an APC are assigned a single relative payment rate, which is linked to the resources required to perform the service. The APC payment rate is geographically adjusted and then multiplied by a CF to determine an actual dollar amount.4
Since 2008, CMS has used a nearly identical mechanism to pay for facility services provided in ASCs. Services are classified using the same APCs and same relative weights as the OPPS. The difference is that the ASC CF is less than the OPPS CF (the 2016 ASC CF is 58% of the OPPS CF), translating into lower dollar payments for ASC services.5 Of note, in 2008 ASC rates were cut significantly when CMS adopted this methodology for determining ASC facility fees (previously, ASC rates were approximately 85% of HOPD rates).
CMS reviews the APCs and their relative weights annually, and may adjust how specific services are classified and how APCs are weighed. Since 2006, HOPD rates for the 10 common procedures listed in Table 1 have increased by 26%-93% real (i.e., Consumer Price Index–adjusted) dollars. Meanwhile, given the steep 2008 ASC fee cuts the 2016 ASC fees are still significantly lower than they were 1 decade ago, especially when accounting for inflation. In fact, ASC fees for the most common procedures have decreased by 20% in real dollars (Supplementary Tables 1 and 2 at http://dx.doi.org/10.1016/j.cgh.2016.03.032).
Putting these changes in context
It is important to consider these changes within a broader context. First, the full economic impact of these changes on an individual gastroenterology practice depends on where it performs its services and whether it collects associated facility fees, and fees for anesthesia and pathology services. Second, the Medicare population is growing by more than 10,000 people each day.6 Third, beyond Medicare, most commercial insurers peg their reimbursement rates to a percentage of the Medicare Fee Schedule. Although the details of specific contracts vary, gastroenterologists should expect to see commercial rates move in a similar direction within the next 1–2 years. Fourth, in the 2016 Fee Schedule CMS described its future intention to remove the value of moderate sedation from all GI procedures valued with moderate sedation inherent to the procedure. The more that moderate sedation is ultimately valued, the less that endoscopic procedures will be valued. Consequently, gastroenterologists who rely on anesthesiology professionals to sedate their patients will receive less revenue per procedure. Finally, the 2015 Medicare Access and Children’s Health Insurance Program Reauthorization Act (MACRA) links a higher proportion of these dwindling fee-for-service payments to performance. Starting in 2018, physicians who elect to remain on a fee-for-service tract will receive a composite Merit-Based Incentive Payment System (MIPS) score that will translate into either performance bonuses or penalties (as much as 4% in 2019 and going up to 9% in 2022). Alternatively, providers who “sufficiently” participate in “two-sided” (i.e., risk-bearing) alternative payment models (e.g., bundled payments and accountable care organizations) instead of fee-for-service payments will receive 5% across-the-board bonuses. In sum, it is possible that fee-for-service payments may eventually become so unattractive that many gastroenterologists decide (or hope) to move to alternative payment models that combine both professional and facility fees, such as the CMS now-mandatory Comprehensive Care for Joint Replacement (CJR) program.7
Impact on academic practices
For most academic gastroenterology practices, clinical revenue far exceeds all other sources of funding, including research grants, teaching support, philanthropy, and partnerships with industry. Although a select few academic GI divisions have managed to build their own ASCs to share facility fees, for most academic practices, clinical revenue comes solely from the professional fees for endoscopic procedures and, less so, from office and hospital-based consultations and management of established patients.8 Thus, steep cuts to professional fees for endoscopic procedures, the leading source of overall revenue, will severely strain most academic gastroenterology practices.
In one of our practices (SDD), the 10 common procedures listed in Table 1 accounted for 27% of total direct clinical revenue over the past year. Roughly one-fourth of our patients are Medicare beneficiaries. Assuming no change in volume, the 2016 fee schedule cuts will amount to a 0.9% drop in direct clinical revenue. If all other payers follow with identical cuts, then direct clinical revenue will drop by 3.7%. Although our practice is fortunate to have other well-developed clinical and nonclinical revenue streams, these cuts are not insignificant.
How can academic practices continue to provide accessible clinical care in the face of these fee cuts? It can help to first consider how revenue is distributed for a Medicare beneficiary who undergoes a diagnostic colonoscopy with biopsy to evaluate unexplained diarrhea in an academic medical center’s hospital-based facility. The academic gastroenterologist receives $212 (CPT 45380). From this $212, the academic gastroenterology practice must pay assessments to various entities (sometimes including the school of medicine, department of medicine, and faculty practice plan) that may amount to more than 30% of total revenue. The roughly $150 that remains is used to pay faculty member salaries (the median salary for an academic gastroenterologist is $300,009) and benefits (estimated at $74,000/year); MP insurance (estimated at $2,275/year, higher in certain parts of the United States); and overhead for support staff, supplies, and other expenses (estimated at $50,550/year). Thus, a purely clinical academic gastroenterologist who is paid at the Medical Group Management Association (MGMA) median must generate $610,179 in preassessment revenue. If this hypothetical academic gastroenterologist solely treated Medicare beneficiaries, at $35.82 per RVU he or she would need to generate a staggering 17,035 RVUs per year, an amount that far exceeds the MGMA median (6,445) and 90th percentile (10,991) for academic gastroenterologists. Of course, real-world academic gastroenterologists also treat commercially insured patients and many spend time on nonclinical activities (although clinical income typically supports time devoted to research and teaching, not vice versa). Still, this example highlights a clear fact: Academic gastroenterology practices take a major financial loss delivering services to Medicare beneficiaries. Meanwhile, the HOPD charges more than $2,200 for the procedure. Although it receives $752 facility fee from Medicare (Disproportionate Share Hospitals and NCI Cancer Centers receive more), with a cost-to-charge ratio of roughly 0.2, revenue still clearly exceeds expenses. Finally, the anesthesia professional (if any) receives roughly $198 (CPT 00810) and the pathologist $74 (CPT 88305).
Although some may argue that academic gastroenterologists should simply accept a pay cut, lower salaries may drive many away from academia. To hire enough new (or even maintain enough existing) faculty members to maintain and grow volume, academic gastroenterology practices must find ways to supplement declining professional fees. One option is for academic practices to open their own ASCs, either alone or jointly with their health care system. But this assumes, often erroneously, that the health care system is willing to share facility fees. A second option is to develop incentive programs that transfer revenue from the health care system to the physicians. Importantly, these must be at fair market value and for nonemployed physicians cannot be linked to volume.10 Examples include medical directorships and non–volume-based performance bonuses. A third option is to consider alternative payment models, such as bundled payments that include a single lump sum payment for both professional and facility fees. The practice and health system then negotiates how the bundle is shared. Bundles should motivate hospitals and academic practices to work together to improve care and reduce overall expenses. Along these lines, CMS recently announced the CJR program under which hospitals and physicians in 75 locations will be required to participate. Although AGA recently published a bundled payment framework for screening and surveillance colonoscopy,11 bundles for other endoscopic procedures remain to be defined. But, a clearly defined, attractively priced, and skillfully negotiated bundle could be a means for redistributing revenue in ways that are more favorable to academic practices. No matter the approach, it is critical for academic gastroenterology practices and their health care systems to align their goals and integrate their services. But this is easier said than done.
Impact on private gastroenterology practices
The impact of these professional and facility fee changes on private practice depends on the practice’s payer mix, and whether it owns an ASC and directly provides anesthesia and pathology services. Consider Texas Digestive Disease Consultants (TDDC), an 80-gastroenterologist practice that provides GI care and endoscopic procedures throughout north and central Texas. TDDC revenue comes solely from professional fees generated by gastroenterologists and the pathologists that the practice employs. TDDC operating expenses include employee salaries and benefits, rent, and taxes. Based on an expected work-year of 2,080 hours, each TDDC gastroenterologist must generate $219 per hour to cover practice expenses. Physicians receive income only after practice revenue exceeds $219 per hour.
In the 2016 Medicare Physician Fee Schedule, colonoscopy code 45387 is assigned 3.36 RVUs, based on 67 minutes in total time. Based on this information, 2016 CMS payment for a screening colonoscopy ($200) will result in a loss of $45 in practice revenue over expenses. Across the TDDC practices in 2015, CMS patients represented 29% of all colonoscopies performed, but only 11% of revenue from those procedures. In aggregate, assuming no change in volume, the 2016 fee schedule cuts will translate into $5,472 less physician income for each gastroenterologist. If all other payers follow with identical cuts then each gastroenterologist would forfeit $50,896 of income.
For pathology services, code 88305 reimburses a global service per specimen. The average number of specimens per outpatient GI procedure at TDDC is 1.5. Based on CMS’ per specimen payment of $73 (down from $107 in 2012), average pathology reimbursement per a CMS endoscopic procedure is $110.
What about facility fees? Many TDDC physicians separately own and operate ASCs and anesthesia practices. Because the physician owners of these facilities funded, developed, and operate these facilities on their own, any revenue over expenses from these facilities flow directly to the ASC, rather than to TDDC. Since 2008, when ASC payments were severely reduced, ASC revenue over expenses for a Medicare colonoscopy has ranged from $0 to $70. For anesthesia services, the ASC receives approximately $159 per screening colonoscopy, which is not enough to actually cover the costs of providing anesthesia services. In sum, when TDDC gastroenterologists perform colonoscopies on Medicare patients at an HOPD the physician loses money. When the same procedure is performed at an ASC the physician barely break even.
How can private practice gastroenterologists respond to these fee cuts? First, some gastroenterologists may be forced to accept lower salaries. Second, practices can offset fee cuts by improving efficiency and reducing overall cost of care, assuming they are not already maximally efficient. Third, some private practices can increase Medicare professional payments by reclassifying as nonparticipating with Medicare. Nonparticipating status allows practices to charge the patient up to approximately 109.25% of the Medicare approved rate, with the patient submitting the claim directly to Medicare (“balance billing”). The downside is that patients shoulder the additional cost and may potentially decide to seek care elsewhere. Fourth, private practices should explore alternative payment models, such as bundled payment as described previously, either on their own or by partnering with local health systems to share risk. Finally, some practices may sell equity to and become employees of local health systems.
Conclusions
Changes to Medicare professional and facility fee payments for endoscopic procedures significantly affect academic and private gastroenterology practices. Dwindling professional fees – alongside increasing HOPD facility fees – make academic gastroenterology practices increasingly reliant on support from their parent health care systems. Like academic practices, private gastroenterology practices experience financial losses when treating Medicare beneficiaries. Academic and private gastroenterology practices should consider several potential responses. Although beyond the scope of this article, all practices must continuously strive to improve the quality and reduce the costs of the endoscopic procedures they perform.
Acknowledgments
The authors thank Leslie Narramore, MPA, for her insights and help with reimbursement data. They also thank Bryan Rhodes for providing financial data and Shivan Mehta, MD, MBA, for his feedback on the Relative Value Scale Update Committee process.
References
1. MEDPAC. Payment basics: physician and other health professional payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
2. Mehta, S.J., Brill, J.V. What is the RUC and how does it impact gastroenterology?. Clin Gastroenterol Hepatol. 2014;12:1208-11.
3. American College of Gastroenterology, American Gastroenterological Association, American Society for Gastrointestinal Endoscopy. Key Provisions in the CY 2015 Medicare Physician Fee Schedule Final Rule, 2015. Available at: http://gi.org/wp-content/uploads/2014/11/Tri-Soc_CY15_MPFS_Final_Rule_Summary.pdf.
4. MEDPAC. Payment basics: Outpatient hospital services payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
5. MEDPAC. Payment basics: Ambulatory surgery center services payment system. Medicare Payment Advisory Commission, Washington, DC; 2015.
6. Diamond, D. 10,000 people are now enrolling in Medicare – every day. Forbes; 2015 (Available at: http://www.forbes.com/sites/dandiamond/2015/07/13/aging-in-america-10000-people-enroll-in-medicare-every-day/#5177f1f35e07. Accessed January 3, 2016)
7. Mechanic, R.E. Mandatory Medicare bundled payment: Is it ready for prime time?. N Engl J Med. 2015;373:1291-3.
8. Rustgi, A.K., Allen, J.I. The house of gastrointestinal medicine: How academic medical centers can build a sustainable economic clinical model. Clin Gastroenterol Hepatol. 2013;11:1370-3.
9. Academic Practice Compensation and Production Report. Medical Group Management Association, Englewood, Colo.; 2015.
10. Becker S., Townshend G., Carnell H., et al. Physician compensation: 10 core legal and regulatory concepts. Becker’s Hospital Review Available at: http://www.beckershospitalreview.com/legal-regulatory-issues/physician-compensation-10-core-legal-and-regulatory-concepts.html. Accessed Jan. 20, 2016.
11. Brill, J.V., Jain, R., Margolis, P.S., et al. A bundled payment framework for colonoscopy performed for colorectal cancer screening or surveillance. Gastroenterology. 2014;146:849-53, e9.
Dr. Dorn is vice chief, division of gastroenterology and hepatology, associate professor of medicine, health policy & management, University of North Carolina at Chapel Hill; he has received honoraria for consulting and presentations on health reform from AbbVie and Olympus. Dr. Vesy is a gastroenterologist affiliated with Baylor University Medical Center, Dallas.

Changing payments, changing practice
The first article during my tenure as editor of the “Practice Management: The Road Ahead” section of Clinical Gastroenterology and Hepatology published in July 2012 (Clin Gastroenterol Hepatol. 2012;10:692-6) outlined anticipated changes in health care delivery, due in large part to mandates or trends contained in the Patient Protection and Affordable Care Act. A second article was published in 2013 (Health care reform 3.0: The road gets bumpy. Clin Gastroenterol Hepatol. 2013;11:1527-8). In this month’s column, Spencer D. Dorn, MD, MPH, MHA, of the University of North Carolina at Chapel Hill, adds a third update with an article focused on alternative payment models. These new reimbursement models are becoming common and will be part of all of our practice strategies in the years to come. No matter what occurs in the 2016 election, the movement from volume- to value-based payment will continue relentlessly, and practices that do not understand how to respond will struggle. We hope these articles will kick-start conversations in your practice.
Fee-for-service (FFS) reimbursement has been criticized for encouraging quantity over quality, favoring procedures over cognitive services, and fragmenting care.1 The landmark Patient Protection and Affordable Care Act (ACA) and more recent Medicare Access and Children’s Health Insurance Program Reauthorization Act (MACRA) modify Medicare’s FFS and encourage alternative payment models (APMs) that better reward value than volume.
Prior articles in this series have identified the specific trends driving gastroenterology practice strategies and business decisions,2 including an increasing need to demonstrate value, an emphasis on improved population health, an increasing number of practices becoming employees of large integrated delivery networks, reduced FFS reimbursements that are more closely linked to performance metrics, and increasing demands for risk-based contracts.3 In this article, I dive more deeply into these last two trends (declining FFS and the rise of APMs) and consider strategies gastroenterology practices can take in response.
Changes in fee for service
The ACA directed the secretary of Health and Human Services to establish a formal process to review potentially misvalued procedure codes. Compared with the pre-ACA fee schedule, the final 2016 Medicare Physician Fee Schedule includes cuts to professional fees for upper endoscopy, endoscopic retrograde cholangiopancreatography, endoscopic ultrasound, and colonoscopy. At the same time, over the past decade, facility fees paid for procedures performed in hospital outpatient departments have increased. Those to ambulatory surgery centers have gradually increased, although they still remain far below pre-2008 levels. Thus, the full economic impact of fee revaluation on an individual gastroenterology practice depends on whether it collects associated facility and ancillary fees.4
In addition, in the 2016 fee schedule, the Centers for Medicare & Medicaid Services described its intention to remove the value of moderate sedation from all gastrointestinal procedures. This is to prevent paying twice for sedation in procedures that involve anesthesiology professionals (i.e., one payment to the endoscopist as part of the overall procedure fee and a separate payment to the anesthesia professional for sedation they provide and bill for separately). The American Medical Association/Specialty Society Relative Value Scale Update Committee, using survey data from the GI specialty societies and other specialties that perform their own moderate sedation, has submitted recommendations for the value of a new set of moderate sedation Current Procedural Terminology codes to the CMS. The agency is expected to provide the specifics on how it will remove moderate sedation from the GI procedure codes in the 2017 Medicare Physician Fee Schedule Proposed Rule. The more that moderate sedation is valued, the less that endoscopic procedures will be valued. Consequently, gastroenterologists who rely on anesthesiology professionals to sedate their patients will generate less revenue per procedure, unless they rearrange contracts with anesthesia providers. Gastroenterologists who perform moderate sedation will not be impacted, because the sum of the value of the new moderate sedation code plus the underlying endoscopic procedure code will equal the original value of the procedure.
Beyond revaluing services, the CMS outlined its rather ambitious goal “to have 85% of all Medicare fee-for-service (FFS) payments tied to quality or value by 2016, and 90% by 2018.”5 Currently this includes the Physician Quality Reporting System (PQRS), which requires gastroenterologists to report performance on either three or more individual PQRS measures or one PQRS measures group (collection of related individual measures) or face a 2% Medicare payment penalty. It also includes the value-based payment modifier, through which by 2017 all practices with better-than-average quality (linked to PQRS measures) and lower costs will receive bonus payments, whereas those with worse-than-average performance (or who choose not to report) will be penalized.
MACRA changes all of this. Starting in 2019, the meaningful use incentive program, PQRS, and value-based payment modifier will be consolidated into the Merit-Based Incentive Payment System (MIPS). Physicians who elect to remain on an FFS tract will receive a 0-100 composite performance score based on quality (30%), resource use (30%), meaningful use (25%), and clinical practice improvement activities (15%). At the start of a performance period, a composite threshold necessary to achieve incentive payments and avoid penalties will be determined. Throughout the performance period, physicians will receive timely feedback on their performance. At year’s end, those below the threshold will face penalties proportionate to their performance (as much as 4% in 2019 and going up to 9% in 2022), those at threshold will not receive a payment adjustment, and those above threshold will receive bonuses proportionate to their performance (although overall payments will be capped at $500 million).
Alternative payment models
The CMS’s ultimate goal is to move beyond FFS and have “30% of Medicare payments tied to quality or value through APMs by the end of 2016 and 50% of payments by the end of 2018.”5 MACRA supports this ambitious goal: Starting in 2019, providers who “sufficiently” participate in APMs will receive 5% across-the-board bonuses. The three main APMs are bundled payments, accountable care organizations (ACOs), and patient-centered medical homes.
A bundled payment is a single fixed price paid to cover services for a specific episode of care. Depending on how an episode is defined, the bundle may encompass all professional fees, facility fees, and medical device and supply costs for a given service, including postacute care and any complications. If costs are reduced beyond the already discounted price of the bundle and quality metrics are achieved, then participants share the savings. Conversely, if costs exceed the bundled payment amount, then participants lose money. Unlike FFS, bundling incentivizes participants to coordinate care, reduce complications and unnecessary services, and cut purchasing costs.
To date, the CMS has launched three bundling programs. The Acute Care Episode Demonstration Project provided hospitals and clinicians a bundled payment to cover orthopedic and cardiovascular procedure–related episodes of care. This program reduced Medicare costs, primarily because the bundle payment was lower than what the sum of individual payments would have been. Providers were able to cope mainly by reducing their surgical implant costs. Second, more than 6,000 providers are currently participating in Medicare’s Bundled Payments for Care Improvement Program. The results of this program have not yet been released. Third, the CMS recently announced the Comprehensive Care for Joint Replacement Program under which hospitals and physicians in 67 metropolitan areas will be required to participate. Mandatory participation signals the CMS’s strong motivation to shift away from FFS. Beyond Medicare, many commercial insurers offer bundled payment programs, primarily for cardiovascular and orthopedic conditions.6 Although these programs are promising, it is technically challenging to define what is in a bundle, and to adequately risk adjust and mitigate random variation in spending for certain episodes of care. Providers are also challenged to find ways to divide payment among participants, coordinate all care, and accept financial risk.7,8 The American Gastroenterological Association recently published a bundled payment framework for screening and surveillance colonoscopy.9 Bundling other gastroenterology services will be more challenging.
Whereas bundled-care programs focus on a discrete service (e.g., knee replacement or colonoscopy), ACOs are integrated groups of providers who jointly assume responsibility for the cost and quality of all care delivered to a defined population. The ACA requires ACOs to have formal legal, leadership, and management structures; care for at least 5,000 Medicare beneficiaries; fulfill certain patient-centeredness criteria; measure and report quality and cost data; and coordinate care. Different payment models incentivize ACOs to reduce costs and improve quality of care. ACOs operating under a one-sided shared savings model receive FFS payments for each service delivered, along with a bonus for reducing costs below a spending target and meeting quality requirements. There are no potential financial penalties. Alternatively, ACOs operating under a two-sided risk-savings model share a greater proportion of cost savings, in exchange for potential financial penalties if the cost of care exceeds target spending.
To date, Medicare-sponsored ACOs have produced mixed results. In 2014 only 92 of the 322 Medicare Shared Savings ACOs were able to reduce spending below a predetermined benchmark by a predetermined amount (2%-3%) while meeting quality scores, thereby earning a bonus ($341 million in total). Similarly, of the original 32 pioneer ACOs, which by definition are more experienced at managing population health and more willing to take on financial risk, 13 dropped out of the program, and in 2014, only 11 generated enough savings to earn a payout ($82 million in total), whereas 5 incurred financial penalties ($9 million in total) for costs exceeding target thresholds.10 In total, after paying out bonuses, the ACO program cost Medicare a net loss of nearly $3 million, far from the $10-$240 million Medicare had previously projected it would save through the ACO program.11 Clearly, ACOs are not a quick fix for all that ails health care. For many ACOs, the major start-up requirements (time, capital investments, and so forth) needed to manage a population may not be worthwhile.12 Nonetheless, the CMS recently launched the Next Generation ACO model through which 21 participating ACOs will assume higher levels of financial risk (possibly capitated payments) in exchange for greater potential rewards. Similarly, beyond Medicare, there are also many Medicaid-sponsored ACOs and hundreds of commercial payer-sponsored ACOs.13
Finally, practices can qualify for APM status without accepting bundled payments or joining an ACO by qualifying as a patient-centered medical home. One option for gastroenterologists and other specialists is the National Committee for Quality Assurance’s patient-centered specialty practice designation, available to practices that successfully demonstrate their ability to track and coordinate care with primary care providers and other specialists, offer timely appointments and responses to telephone and electronic messages, use evidence-based tools to manage care for specific patient populations, develop patient-centered care plans, and measure and improve performance.14
Consolidation
Health insurers are merging to increase scale (and negotiating power), enhance efficiency (reducing administrative costs makes more room for profits), and diversify their businesses. Recently proposed acquisitions will bring “the big five” health insurers to the “big three.” Likewise, health care systems are rapidly acquiring hospitals and physician groups, so much so that today half of all American health care markets are now considered highly concentrated, and none are considered highly competitive.15 Today only 35% of all physicians are independently employed.16 Physicians employed by health systems trade their complete autonomy to offset declining reimbursement, reduce operating expenses (including health information technology costs), improve work-life balance, and mitigate unknown risks.
Proponents contend that these mergers allow health care systems to better coordinate care, improve care experiences, accommodate new payment models, and assemble the building blocks needed to form ACOs and other integrated care models. Critics argue that locally dominant systems drive volume (by tightening referral relationships and gaining new market share) and increase costs (through enhanced negotiating leverage and by reclassifying newly acquired physician practices as part of the hospital, thereby generating facility fees). It is unclear whether consolidation results in better outcomes or simply increases overall costs.17
Strategic imperatives
What should gastroenterologists do? First, recognize that FFS is not going away anytime soon.18 Most APMs are still largely in their experimentation phase, and it remains unclear which models will work and which will be broadly adopted. Still, it is unrealistic to expect FFS to indefinitely persist as the dominant payment model. For some services FFS may no longer be a payment option (e.g., Medicare’s BCPI [Bundled Payments for Care Improvement]). For others, FFS rates may become so unattractive that APMs seem necessary. Finally, APMs may allow some practices to capture a greater proportion of overall clinical revenue (e.g., academic practices that perform endoscopic procedures within hospital outpatient departments) and to develop new models that meaningfully improve care. Today’s gastroenterology practices must therefore operate on two separate tracks: an FFS track that rewards volume (most practices are optimized for this) and an alternative payment track that rewards value (few practices can accommodate these on their own). The degree and speed with which practices should reorient to the alternative payment track depends on the type of practice and the specific local health care market. But even practices operating in slower-to-evolve markets should start preparing for the APMs, no matter how far off in the distance they may seem. I recommend the following six steps:
1. Integrate. To participate in APMs, preserve referral streams, and maintain negotiating leverage with health plans, independent, community-based practices may need to affiliate or merge with other physician groups, or align with or be acquired by a health care system.19 Academic practices are challenged to define their role within health care systems that are rapidly adding primary care practices, and often community gastroenterology practices, too.
2. Collaborate and communicate. To deliver high-value care to populations of patients, gastroenterologists must closely collaborate and clearly communicate with primary care physicians and other specialists. Collaborative care agreements can help guide these relationships.203. Develop new models of care. Patients with more routine GI and liver-related problems may be served more cost effectively by midlevel providers21 or innovative solutions, such as e-consultations.22 Patients with complex, chronic GI and liver diseases may be best served by multidisciplinary care teams (e.g., gastroenterologists alongside midlevel providers, nurses, care managers, psychologists, and/or pharmacists) who use clinical information systems to identify high-risk patients and to encourage evidence-based decision making, and who support patients to self-manage their own conditions.23 Previously infeasible in a purely FFS world, these models are encouraged by APMs.
4. Care for common, costly conditions. Most gastroenterology practices have built robust colorectal cancer screening programs, sometimes at the expense of cognitive-based services. In today’s more accountable world, practices that can effectively manage common, costly conditions, such as inflammatory bowel disease, functional GI disorders, and advanced liver diseases, will be rewarded better than before and will be more highly sought as partners.
5. Understand and contain costs. The timely, accurate data needed to effectively respond to APMs are challenging to come by.19 Individual clinicians and group practices can roughly gauge their costs of care for Medicare beneficiaries, compared with other practices, using CMS Quality Resource Utilization Reports. Local commercial insurers may be willing to share cost profiles with interested practices. Strategies to reduce costs may include shifting clinically appropriate patients to more cost-effective settings (especially important for academic practices that see the bulk of their patients in costly hospital outpatient departments), standardizing endoscopy supplies and devices, using anesthesia services more selectively, and preferentially prescribing generic drugs, among others.
6. Measure and demonstrate value. Despite the inherent limitations of performance measurement,24 it is imperative that practices measure and report the value of care to their patients, community, and payers so that they are preferred partners and not locked out of insurance or referral networks. Improving patient experiences is intrinsically worthwhile25 and also makes good business sense.26
References
1. Miller, H.D. Creating payment systems to accelerate value-driven health care: Issues and options for policy reform. New York: The Commonwealth Fund, 2007.
2. Allen, J.I. The road ahead. Clin Gastroenterol Hepatol. 2012;10:692–6.
3. Allen, J.I. Health care reform 3.0: The road gets bumpy. Clin Gastroenterol Hepatol. 2013;11:1527-8.
4. Dorn, S.D., Vesy C.J. Medicare’s revaluation of gastrointestinal endoscopic procedures: Implications for academic and community-based practices. Clin Gastroenterol Hepatol. 2016 (in press).
5. Burwell, S.M. Setting value-based payment goals: HHS efforts to improve U.S. health care (N Engl J Med. 2015;372:897–9).
6. The Advisory Board Company. Commercial Bundled Payment Tracker, 2016.
7. Mechanic, R.E. Mandatory Medicare bundled payment – is it ready for prime time? N Engl J Med. 2015;373:1291–3.
8. The National Commission on Physician Payment Reform. Physician Payment Report, 2013.
9. Brill, J.V., Jain, R., Margolis, P.S., et al. A bundled payment framework for colonoscopy performed for colorectal cancer screening or surveillance. Gastroenterology. 2014;146:849–53, e9.
10. Evans, M. Few Medicare ACOs earned bonuses in 2014. Mod Healthc (2015). Available at: www.modernhealthcare.com/article/20150825/NEWS/150829922. Accessed Nov. 14, 2015.
11. Rau, J., Gold, J. Medicare yet to save money through heralded medical payment model. Kaiser Health News. Available at: http://khn.org/news/medicare-yet-to-save-money-through-heralded-medical-payment-model. Accessed Nov. 14, 2015.
12. Goldmsith, J., Kaufman, N. Pioneer ACOs: Anatomy of a victory. Health Affairs Blog, 2015.
13. Tu, T., Muhlestein, D., Kocot, S.L., et al. The impact of accountable care: Origins and future of accountable care organizations. Washington, D.C.: Brookings Institution, 2015.
14. NCQA. Patient-centered specialty practice frequently asked questions.
15. Xu, T., Wu, A.W., Makary, M.A. The potential hazards of hospital consolidation: Implications for quality, access, and price. JAMA. 2015;314:1337–8.
16. The Physician’s Foundation. 2014 survey of America’s physicians. Practice patterns & perspectives: The Physician’s Foundation.
17. Tsai, T.C., Jha, A.K. Hospital consolidation, competition, and quality: Is bigger necessarily better? JAMA. 2014;312:29–30.
18. Ginsburg, P.B. Fee-for-service will remain a feature of major payment reforms, requiring more changes in Medicare physician payment. Health Aff (Millwood). 2012;31:1977–83.
19. Friedberg, M.W., Chen, P.G., White, C., et al. Effects of health care payment models on physician practice in the United States. Santa Monica, Calif.: RAND Corp., 2015.
20. Greenberg, J.O., Barnett, M.L., Spinks, M.A., et al. The “medical neighborhood”: Integrating primary and specialty care for ambulatory patients. JAMA Intern Med. 2014;174:454–7.
21. Dorn, S.D. Mid-level providers in gastroenterology. Am J Gastroenterol. 2010;105:246–51.
22. Wasfy, J.H., Rao, S.K., Kalwani, N., et al. Longer term impact of cardiology e-consults. Am Heart J. 2016;173:86–93.
23. Coleman, K., Austin, B.T., Brach, C., et al. Evidence on the chronic care model in the new millennium. Health Aff (Millwood). 2009;28:75–85.
24. Dorn, S.D. Quality measurement in gastroenterology: confessions of a realist. Clin Gastroenterol Hepatol. 2016;14:648–50.
25. Berwick, D.M. Measuring physicians’ quality and performance: adrift on Lake Wobegon. JAMA. 2009;302:2485-6.
26. Browne, K., Roseman, D., Shaller, D., et al. Analysis & commentary. Measuring patient experience as a strategy for improving primary care. Health Aff (Millwood). 2010;29:921–5.
Dr. Dorn is vice chief, division of gastroenterology and hepatology, associate professor of medicine, health policy & management, University of North Carolina at Chapel Hill. He has received honoraria for consulting and presentations on health reform from AbbVie and Olympus.
The first article during my tenure as editor of the “Practice Management: The Road Ahead” section of Clinical Gastroenterology and Hepatology published in July 2012 (Clin Gastroenterol Hepatol. 2012;10:692-6) outlined anticipated changes in health care delivery, due in large part to mandates or trends contained in the Patient Protection and Affordable Care Act. A second article was published in 2013 (Health care reform 3.0: The road gets bumpy. Clin Gastroenterol Hepatol. 2013;11:1527-8). In this month’s column, Spencer D. Dorn, MD, MPH, MHA, of the University of North Carolina at Chapel Hill, adds a third update with an article focused on alternative payment models. These new reimbursement models are becoming common and will be part of all of our practice strategies in the years to come. No matter what occurs in the 2016 election, the movement from volume- to value-based payment will continue relentlessly, and practices that do not understand how to respond will struggle. We hope these articles will kick-start conversations in your practice.
Fee-for-service (FFS) reimbursement has been criticized for encouraging quantity over quality, favoring procedures over cognitive services, and fragmenting care.1 The landmark Patient Protection and Affordable Care Act (ACA) and more recent Medicare Access and Children’s Health Insurance Program Reauthorization Act (MACRA) modify Medicare’s FFS and encourage alternative payment models (APMs) that better reward value than volume.
Prior articles in this series have identified the specific trends driving gastroenterology practice strategies and business decisions,2 including an increasing need to demonstrate value, an emphasis on improved population health, an increasing number of practices becoming employees of large integrated delivery networks, reduced FFS reimbursements that are more closely linked to performance metrics, and increasing demands for risk-based contracts.3 In this article, I dive more deeply into these last two trends (declining FFS and the rise of APMs) and consider strategies gastroenterology practices can take in response.
Changes in fee for service
The ACA directed the secretary of Health and Human Services to establish a formal process to review potentially misvalued procedure codes. Compared with the pre-ACA fee schedule, the final 2016 Medicare Physician Fee Schedule includes cuts to professional fees for upper endoscopy, endoscopic retrograde cholangiopancreatography, endoscopic ultrasound, and colonoscopy. At the same time, over the past decade, facility fees paid for procedures performed in hospital outpatient departments have increased. Those to ambulatory surgery centers have gradually increased, although they still remain far below pre-2008 levels. Thus, the full economic impact of fee revaluation on an individual gastroenterology practice depends on whether it collects associated facility and ancillary fees.4
In addition, in the 2016 fee schedule, the Centers for Medicare & Medicaid Services described its intention to remove the value of moderate sedation from all gastrointestinal procedures. This is to prevent paying twice for sedation in procedures that involve anesthesiology professionals (i.e., one payment to the endoscopist as part of the overall procedure fee and a separate payment to the anesthesia professional for sedation they provide and bill for separately). The American Medical Association/Specialty Society Relative Value Scale Update Committee, using survey data from the GI specialty societies and other specialties that perform their own moderate sedation, has submitted recommendations for the value of a new set of moderate sedation Current Procedural Terminology codes to the CMS. The agency is expected to provide the specifics on how it will remove moderate sedation from the GI procedure codes in the 2017 Medicare Physician Fee Schedule Proposed Rule. The more that moderate sedation is valued, the less that endoscopic procedures will be valued. Consequently, gastroenterologists who rely on anesthesiology professionals to sedate their patients will generate less revenue per procedure, unless they rearrange contracts with anesthesia providers. Gastroenterologists who perform moderate sedation will not be impacted, because the sum of the value of the new moderate sedation code plus the underlying endoscopic procedure code will equal the original value of the procedure.
Beyond revaluing services, the CMS outlined its rather ambitious goal “to have 85% of all Medicare fee-for-service (FFS) payments tied to quality or value by 2016, and 90% by 2018.”5 Currently this includes the Physician Quality Reporting System (PQRS), which requires gastroenterologists to report performance on either three or more individual PQRS measures or one PQRS measures group (collection of related individual measures) or face a 2% Medicare payment penalty. It also includes the value-based payment modifier, through which by 2017 all practices with better-than-average quality (linked to PQRS measures) and lower costs will receive bonus payments, whereas those with worse-than-average performance (or who choose not to report) will be penalized.
MACRA changes all of this. Starting in 2019, the meaningful use incentive program, PQRS, and value-based payment modifier will be consolidated into the Merit-Based Incentive Payment System (MIPS). Physicians who elect to remain on an FFS tract will receive a 0-100 composite performance score based on quality (30%), resource use (30%), meaningful use (25%), and clinical practice improvement activities (15%). At the start of a performance period, a composite threshold necessary to achieve incentive payments and avoid penalties will be determined. Throughout the performance period, physicians will receive timely feedback on their performance. At year’s end, those below the threshold will face penalties proportionate to their performance (as much as 4% in 2019 and going up to 9% in 2022), those at threshold will not receive a payment adjustment, and those above threshold will receive bonuses proportionate to their performance (although overall payments will be capped at $500 million).
Alternative payment models
The CMS’s ultimate goal is to move beyond FFS and have “30% of Medicare payments tied to quality or value through APMs by the end of 2016 and 50% of payments by the end of 2018.”5 MACRA supports this ambitious goal: Starting in 2019, providers who “sufficiently” participate in APMs will receive 5% across-the-board bonuses. The three main APMs are bundled payments, accountable care organizations (ACOs), and patient-centered medical homes.
A bundled payment is a single fixed price paid to cover services for a specific episode of care. Depending on how an episode is defined, the bundle may encompass all professional fees, facility fees, and medical device and supply costs for a given service, including postacute care and any complications. If costs are reduced beyond the already discounted price of the bundle and quality metrics are achieved, then participants share the savings. Conversely, if costs exceed the bundled payment amount, then participants lose money. Unlike FFS, bundling incentivizes participants to coordinate care, reduce complications and unnecessary services, and cut purchasing costs.
To date, the CMS has launched three bundling programs. The Acute Care Episode Demonstration Project provided hospitals and clinicians a bundled payment to cover orthopedic and cardiovascular procedure–related episodes of care. This program reduced Medicare costs, primarily because the bundle payment was lower than what the sum of individual payments would have been. Providers were able to cope mainly by reducing their surgical implant costs. Second, more than 6,000 providers are currently participating in Medicare’s Bundled Payments for Care Improvement Program. The results of this program have not yet been released. Third, the CMS recently announced the Comprehensive Care for Joint Replacement Program under which hospitals and physicians in 67 metropolitan areas will be required to participate. Mandatory participation signals the CMS’s strong motivation to shift away from FFS. Beyond Medicare, many commercial insurers offer bundled payment programs, primarily for cardiovascular and orthopedic conditions.6 Although these programs are promising, it is technically challenging to define what is in a bundle, and to adequately risk adjust and mitigate random variation in spending for certain episodes of care. Providers are also challenged to find ways to divide payment among participants, coordinate all care, and accept financial risk.7,8 The American Gastroenterological Association recently published a bundled payment framework for screening and surveillance colonoscopy.9 Bundling other gastroenterology services will be more challenging.
Whereas bundled-care programs focus on a discrete service (e.g., knee replacement or colonoscopy), ACOs are integrated groups of providers who jointly assume responsibility for the cost and quality of all care delivered to a defined population. The ACA requires ACOs to have formal legal, leadership, and management structures; care for at least 5,000 Medicare beneficiaries; fulfill certain patient-centeredness criteria; measure and report quality and cost data; and coordinate care. Different payment models incentivize ACOs to reduce costs and improve quality of care. ACOs operating under a one-sided shared savings model receive FFS payments for each service delivered, along with a bonus for reducing costs below a spending target and meeting quality requirements. There are no potential financial penalties. Alternatively, ACOs operating under a two-sided risk-savings model share a greater proportion of cost savings, in exchange for potential financial penalties if the cost of care exceeds target spending.
To date, Medicare-sponsored ACOs have produced mixed results. In 2014 only 92 of the 322 Medicare Shared Savings ACOs were able to reduce spending below a predetermined benchmark by a predetermined amount (2%-3%) while meeting quality scores, thereby earning a bonus ($341 million in total). Similarly, of the original 32 pioneer ACOs, which by definition are more experienced at managing population health and more willing to take on financial risk, 13 dropped out of the program, and in 2014, only 11 generated enough savings to earn a payout ($82 million in total), whereas 5 incurred financial penalties ($9 million in total) for costs exceeding target thresholds.10 In total, after paying out bonuses, the ACO program cost Medicare a net loss of nearly $3 million, far from the $10-$240 million Medicare had previously projected it would save through the ACO program.11 Clearly, ACOs are not a quick fix for all that ails health care. For many ACOs, the major start-up requirements (time, capital investments, and so forth) needed to manage a population may not be worthwhile.12 Nonetheless, the CMS recently launched the Next Generation ACO model through which 21 participating ACOs will assume higher levels of financial risk (possibly capitated payments) in exchange for greater potential rewards. Similarly, beyond Medicare, there are also many Medicaid-sponsored ACOs and hundreds of commercial payer-sponsored ACOs.13
Finally, practices can qualify for APM status without accepting bundled payments or joining an ACO by qualifying as a patient-centered medical home. One option for gastroenterologists and other specialists is the National Committee for Quality Assurance’s patient-centered specialty practice designation, available to practices that successfully demonstrate their ability to track and coordinate care with primary care providers and other specialists, offer timely appointments and responses to telephone and electronic messages, use evidence-based tools to manage care for specific patient populations, develop patient-centered care plans, and measure and improve performance.14
Consolidation
Health insurers are merging to increase scale (and negotiating power), enhance efficiency (reducing administrative costs makes more room for profits), and diversify their businesses. Recently proposed acquisitions will bring “the big five” health insurers to the “big three.” Likewise, health care systems are rapidly acquiring hospitals and physician groups, so much so that today half of all American health care markets are now considered highly concentrated, and none are considered highly competitive.15 Today only 35% of all physicians are independently employed.16 Physicians employed by health systems trade their complete autonomy to offset declining reimbursement, reduce operating expenses (including health information technology costs), improve work-life balance, and mitigate unknown risks.
Proponents contend that these mergers allow health care systems to better coordinate care, improve care experiences, accommodate new payment models, and assemble the building blocks needed to form ACOs and other integrated care models. Critics argue that locally dominant systems drive volume (by tightening referral relationships and gaining new market share) and increase costs (through enhanced negotiating leverage and by reclassifying newly acquired physician practices as part of the hospital, thereby generating facility fees). It is unclear whether consolidation results in better outcomes or simply increases overall costs.17
Strategic imperatives
What should gastroenterologists do? First, recognize that FFS is not going away anytime soon.18 Most APMs are still largely in their experimentation phase, and it remains unclear which models will work and which will be broadly adopted. Still, it is unrealistic to expect FFS to indefinitely persist as the dominant payment model. For some services FFS may no longer be a payment option (e.g., Medicare’s BCPI [Bundled Payments for Care Improvement]). For others, FFS rates may become so unattractive that APMs seem necessary. Finally, APMs may allow some practices to capture a greater proportion of overall clinical revenue (e.g., academic practices that perform endoscopic procedures within hospital outpatient departments) and to develop new models that meaningfully improve care. Today’s gastroenterology practices must therefore operate on two separate tracks: an FFS track that rewards volume (most practices are optimized for this) and an alternative payment track that rewards value (few practices can accommodate these on their own). The degree and speed with which practices should reorient to the alternative payment track depends on the type of practice and the specific local health care market. But even practices operating in slower-to-evolve markets should start preparing for the APMs, no matter how far off in the distance they may seem. I recommend the following six steps:
1. Integrate. To participate in APMs, preserve referral streams, and maintain negotiating leverage with health plans, independent, community-based practices may need to affiliate or merge with other physician groups, or align with or be acquired by a health care system.19 Academic practices are challenged to define their role within health care systems that are rapidly adding primary care practices, and often community gastroenterology practices, too.
2. Collaborate and communicate. To deliver high-value care to populations of patients, gastroenterologists must closely collaborate and clearly communicate with primary care physicians and other specialists. Collaborative care agreements can help guide these relationships.203. Develop new models of care. Patients with more routine GI and liver-related problems may be served more cost effectively by midlevel providers21 or innovative solutions, such as e-consultations.22 Patients with complex, chronic GI and liver diseases may be best served by multidisciplinary care teams (e.g., gastroenterologists alongside midlevel providers, nurses, care managers, psychologists, and/or pharmacists) who use clinical information systems to identify high-risk patients and to encourage evidence-based decision making, and who support patients to self-manage their own conditions.23 Previously infeasible in a purely FFS world, these models are encouraged by APMs.
4. Care for common, costly conditions. Most gastroenterology practices have built robust colorectal cancer screening programs, sometimes at the expense of cognitive-based services. In today’s more accountable world, practices that can effectively manage common, costly conditions, such as inflammatory bowel disease, functional GI disorders, and advanced liver diseases, will be rewarded better than before and will be more highly sought as partners.
5. Understand and contain costs. The timely, accurate data needed to effectively respond to APMs are challenging to come by.19 Individual clinicians and group practices can roughly gauge their costs of care for Medicare beneficiaries, compared with other practices, using CMS Quality Resource Utilization Reports. Local commercial insurers may be willing to share cost profiles with interested practices. Strategies to reduce costs may include shifting clinically appropriate patients to more cost-effective settings (especially important for academic practices that see the bulk of their patients in costly hospital outpatient departments), standardizing endoscopy supplies and devices, using anesthesia services more selectively, and preferentially prescribing generic drugs, among others.
6. Measure and demonstrate value. Despite the inherent limitations of performance measurement,24 it is imperative that practices measure and report the value of care to their patients, community, and payers so that they are preferred partners and not locked out of insurance or referral networks. Improving patient experiences is intrinsically worthwhile25 and also makes good business sense.26
References
1. Miller, H.D. Creating payment systems to accelerate value-driven health care: Issues and options for policy reform. New York: The Commonwealth Fund, 2007.
2. Allen, J.I. The road ahead. Clin Gastroenterol Hepatol. 2012;10:692–6.
3. Allen, J.I. Health care reform 3.0: The road gets bumpy. Clin Gastroenterol Hepatol. 2013;11:1527-8.
4. Dorn, S.D., Vesy C.J. Medicare’s revaluation of gastrointestinal endoscopic procedures: Implications for academic and community-based practices. Clin Gastroenterol Hepatol. 2016 (in press).
5. Burwell, S.M. Setting value-based payment goals: HHS efforts to improve U.S. health care (N Engl J Med. 2015;372:897–9).
6. The Advisory Board Company. Commercial Bundled Payment Tracker, 2016.
7. Mechanic, R.E. Mandatory Medicare bundled payment – is it ready for prime time? N Engl J Med. 2015;373:1291–3.
8. The National Commission on Physician Payment Reform. Physician Payment Report, 2013.
9. Brill, J.V., Jain, R., Margolis, P.S., et al. A bundled payment framework for colonoscopy performed for colorectal cancer screening or surveillance. Gastroenterology. 2014;146:849–53, e9.
10. Evans, M. Few Medicare ACOs earned bonuses in 2014. Mod Healthc (2015). Available at: www.modernhealthcare.com/article/20150825/NEWS/150829922. Accessed Nov. 14, 2015.
11. Rau, J., Gold, J. Medicare yet to save money through heralded medical payment model. Kaiser Health News. Available at: http://khn.org/news/medicare-yet-to-save-money-through-heralded-medical-payment-model. Accessed Nov. 14, 2015.
12. Goldmsith, J., Kaufman, N. Pioneer ACOs: Anatomy of a victory. Health Affairs Blog, 2015.
13. Tu, T., Muhlestein, D., Kocot, S.L., et al. The impact of accountable care: Origins and future of accountable care organizations. Washington, D.C.: Brookings Institution, 2015.
14. NCQA. Patient-centered specialty practice frequently asked questions.
15. Xu, T., Wu, A.W., Makary, M.A. The potential hazards of hospital consolidation: Implications for quality, access, and price. JAMA. 2015;314:1337–8.
16. The Physician’s Foundation. 2014 survey of America’s physicians. Practice patterns & perspectives: The Physician’s Foundation.
17. Tsai, T.C., Jha, A.K. Hospital consolidation, competition, and quality: Is bigger necessarily better? JAMA. 2014;312:29–30.
18. Ginsburg, P.B. Fee-for-service will remain a feature of major payment reforms, requiring more changes in Medicare physician payment. Health Aff (Millwood). 2012;31:1977–83.
19. Friedberg, M.W., Chen, P.G., White, C., et al. Effects of health care payment models on physician practice in the United States. Santa Monica, Calif.: RAND Corp., 2015.
20. Greenberg, J.O., Barnett, M.L., Spinks, M.A., et al. The “medical neighborhood”: Integrating primary and specialty care for ambulatory patients. JAMA Intern Med. 2014;174:454–7.
21. Dorn, S.D. Mid-level providers in gastroenterology. Am J Gastroenterol. 2010;105:246–51.
22. Wasfy, J.H., Rao, S.K., Kalwani, N., et al. Longer term impact of cardiology e-consults. Am Heart J. 2016;173:86–93.
23. Coleman, K., Austin, B.T., Brach, C., et al. Evidence on the chronic care model in the new millennium. Health Aff (Millwood). 2009;28:75–85.
24. Dorn, S.D. Quality measurement in gastroenterology: confessions of a realist. Clin Gastroenterol Hepatol. 2016;14:648–50.
25. Berwick, D.M. Measuring physicians’ quality and performance: adrift on Lake Wobegon. JAMA. 2009;302:2485-6.
26. Browne, K., Roseman, D., Shaller, D., et al. Analysis & commentary. Measuring patient experience as a strategy for improving primary care. Health Aff (Millwood). 2010;29:921–5.
Dr. Dorn is vice chief, division of gastroenterology and hepatology, associate professor of medicine, health policy & management, University of North Carolina at Chapel Hill. He has received honoraria for consulting and presentations on health reform from AbbVie and Olympus.
The first article during my tenure as editor of the “Practice Management: The Road Ahead” section of Clinical Gastroenterology and Hepatology published in July 2012 (Clin Gastroenterol Hepatol. 2012;10:692-6) outlined anticipated changes in health care delivery, due in large part to mandates or trends contained in the Patient Protection and Affordable Care Act. A second article was published in 2013 (Health care reform 3.0: The road gets bumpy. Clin Gastroenterol Hepatol. 2013;11:1527-8). In this month’s column, Spencer D. Dorn, MD, MPH, MHA, of the University of North Carolina at Chapel Hill, adds a third update with an article focused on alternative payment models. These new reimbursement models are becoming common and will be part of all of our practice strategies in the years to come. No matter what occurs in the 2016 election, the movement from volume- to value-based payment will continue relentlessly, and practices that do not understand how to respond will struggle. We hope these articles will kick-start conversations in your practice.
Fee-for-service (FFS) reimbursement has been criticized for encouraging quantity over quality, favoring procedures over cognitive services, and fragmenting care.1 The landmark Patient Protection and Affordable Care Act (ACA) and more recent Medicare Access and Children’s Health Insurance Program Reauthorization Act (MACRA) modify Medicare’s FFS and encourage alternative payment models (APMs) that better reward value than volume.
Prior articles in this series have identified the specific trends driving gastroenterology practice strategies and business decisions,2 including an increasing need to demonstrate value, an emphasis on improved population health, an increasing number of practices becoming employees of large integrated delivery networks, reduced FFS reimbursements that are more closely linked to performance metrics, and increasing demands for risk-based contracts.3 In this article, I dive more deeply into these last two trends (declining FFS and the rise of APMs) and consider strategies gastroenterology practices can take in response.
Changes in fee for service
The ACA directed the secretary of Health and Human Services to establish a formal process to review potentially misvalued procedure codes. Compared with the pre-ACA fee schedule, the final 2016 Medicare Physician Fee Schedule includes cuts to professional fees for upper endoscopy, endoscopic retrograde cholangiopancreatography, endoscopic ultrasound, and colonoscopy. At the same time, over the past decade, facility fees paid for procedures performed in hospital outpatient departments have increased. Those to ambulatory surgery centers have gradually increased, although they still remain far below pre-2008 levels. Thus, the full economic impact of fee revaluation on an individual gastroenterology practice depends on whether it collects associated facility and ancillary fees.4
In addition, in the 2016 fee schedule, the Centers for Medicare & Medicaid Services described its intention to remove the value of moderate sedation from all gastrointestinal procedures. This is to prevent paying twice for sedation in procedures that involve anesthesiology professionals (i.e., one payment to the endoscopist as part of the overall procedure fee and a separate payment to the anesthesia professional for sedation they provide and bill for separately). The American Medical Association/Specialty Society Relative Value Scale Update Committee, using survey data from the GI specialty societies and other specialties that perform their own moderate sedation, has submitted recommendations for the value of a new set of moderate sedation Current Procedural Terminology codes to the CMS. The agency is expected to provide the specifics on how it will remove moderate sedation from the GI procedure codes in the 2017 Medicare Physician Fee Schedule Proposed Rule. The more that moderate sedation is valued, the less that endoscopic procedures will be valued. Consequently, gastroenterologists who rely on anesthesiology professionals to sedate their patients will generate less revenue per procedure, unless they rearrange contracts with anesthesia providers. Gastroenterologists who perform moderate sedation will not be impacted, because the sum of the value of the new moderate sedation code plus the underlying endoscopic procedure code will equal the original value of the procedure.
Beyond revaluing services, the CMS outlined its rather ambitious goal “to have 85% of all Medicare fee-for-service (FFS) payments tied to quality or value by 2016, and 90% by 2018.”5 Currently this includes the Physician Quality Reporting System (PQRS), which requires gastroenterologists to report performance on either three or more individual PQRS measures or one PQRS measures group (collection of related individual measures) or face a 2% Medicare payment penalty. It also includes the value-based payment modifier, through which by 2017 all practices with better-than-average quality (linked to PQRS measures) and lower costs will receive bonus payments, whereas those with worse-than-average performance (or who choose not to report) will be penalized.
MACRA changes all of this. Starting in 2019, the meaningful use incentive program, PQRS, and value-based payment modifier will be consolidated into the Merit-Based Incentive Payment System (MIPS). Physicians who elect to remain on an FFS tract will receive a 0-100 composite performance score based on quality (30%), resource use (30%), meaningful use (25%), and clinical practice improvement activities (15%). At the start of a performance period, a composite threshold necessary to achieve incentive payments and avoid penalties will be determined. Throughout the performance period, physicians will receive timely feedback on their performance. At year’s end, those below the threshold will face penalties proportionate to their performance (as much as 4% in 2019 and going up to 9% in 2022), those at threshold will not receive a payment adjustment, and those above threshold will receive bonuses proportionate to their performance (although overall payments will be capped at $500 million).
Alternative payment models
The CMS’s ultimate goal is to move beyond FFS and have “30% of Medicare payments tied to quality or value through APMs by the end of 2016 and 50% of payments by the end of 2018.”5 MACRA supports this ambitious goal: Starting in 2019, providers who “sufficiently” participate in APMs will receive 5% across-the-board bonuses. The three main APMs are bundled payments, accountable care organizations (ACOs), and patient-centered medical homes.
A bundled payment is a single fixed price paid to cover services for a specific episode of care. Depending on how an episode is defined, the bundle may encompass all professional fees, facility fees, and medical device and supply costs for a given service, including postacute care and any complications. If costs are reduced beyond the already discounted price of the bundle and quality metrics are achieved, then participants share the savings. Conversely, if costs exceed the bundled payment amount, then participants lose money. Unlike FFS, bundling incentivizes participants to coordinate care, reduce complications and unnecessary services, and cut purchasing costs.
To date, the CMS has launched three bundling programs. The Acute Care Episode Demonstration Project provided hospitals and clinicians a bundled payment to cover orthopedic and cardiovascular procedure–related episodes of care. This program reduced Medicare costs, primarily because the bundle payment was lower than what the sum of individual payments would have been. Providers were able to cope mainly by reducing their surgical implant costs. Second, more than 6,000 providers are currently participating in Medicare’s Bundled Payments for Care Improvement Program. The results of this program have not yet been released. Third, the CMS recently announced the Comprehensive Care for Joint Replacement Program under which hospitals and physicians in 67 metropolitan areas will be required to participate. Mandatory participation signals the CMS’s strong motivation to shift away from FFS. Beyond Medicare, many commercial insurers offer bundled payment programs, primarily for cardiovascular and orthopedic conditions.6 Although these programs are promising, it is technically challenging to define what is in a bundle, and to adequately risk adjust and mitigate random variation in spending for certain episodes of care. Providers are also challenged to find ways to divide payment among participants, coordinate all care, and accept financial risk.7,8 The American Gastroenterological Association recently published a bundled payment framework for screening and surveillance colonoscopy.9 Bundling other gastroenterology services will be more challenging.
Whereas bundled-care programs focus on a discrete service (e.g., knee replacement or colonoscopy), ACOs are integrated groups of providers who jointly assume responsibility for the cost and quality of all care delivered to a defined population. The ACA requires ACOs to have formal legal, leadership, and management structures; care for at least 5,000 Medicare beneficiaries; fulfill certain patient-centeredness criteria; measure and report quality and cost data; and coordinate care. Different payment models incentivize ACOs to reduce costs and improve quality of care. ACOs operating under a one-sided shared savings model receive FFS payments for each service delivered, along with a bonus for reducing costs below a spending target and meeting quality requirements. There are no potential financial penalties. Alternatively, ACOs operating under a two-sided risk-savings model share a greater proportion of cost savings, in exchange for potential financial penalties if the cost of care exceeds target spending.
To date, Medicare-sponsored ACOs have produced mixed results. In 2014 only 92 of the 322 Medicare Shared Savings ACOs were able to reduce spending below a predetermined benchmark by a predetermined amount (2%-3%) while meeting quality scores, thereby earning a bonus ($341 million in total). Similarly, of the original 32 pioneer ACOs, which by definition are more experienced at managing population health and more willing to take on financial risk, 13 dropped out of the program, and in 2014, only 11 generated enough savings to earn a payout ($82 million in total), whereas 5 incurred financial penalties ($9 million in total) for costs exceeding target thresholds.10 In total, after paying out bonuses, the ACO program cost Medicare a net loss of nearly $3 million, far from the $10-$240 million Medicare had previously projected it would save through the ACO program.11 Clearly, ACOs are not a quick fix for all that ails health care. For many ACOs, the major start-up requirements (time, capital investments, and so forth) needed to manage a population may not be worthwhile.12 Nonetheless, the CMS recently launched the Next Generation ACO model through which 21 participating ACOs will assume higher levels of financial risk (possibly capitated payments) in exchange for greater potential rewards. Similarly, beyond Medicare, there are also many Medicaid-sponsored ACOs and hundreds of commercial payer-sponsored ACOs.13
Finally, practices can qualify for APM status without accepting bundled payments or joining an ACO by qualifying as a patient-centered medical home. One option for gastroenterologists and other specialists is the National Committee for Quality Assurance’s patient-centered specialty practice designation, available to practices that successfully demonstrate their ability to track and coordinate care with primary care providers and other specialists, offer timely appointments and responses to telephone and electronic messages, use evidence-based tools to manage care for specific patient populations, develop patient-centered care plans, and measure and improve performance.14
Consolidation
Health insurers are merging to increase scale (and negotiating power), enhance efficiency (reducing administrative costs makes more room for profits), and diversify their businesses. Recently proposed acquisitions will bring “the big five” health insurers to the “big three.” Likewise, health care systems are rapidly acquiring hospitals and physician groups, so much so that today half of all American health care markets are now considered highly concentrated, and none are considered highly competitive.15 Today only 35% of all physicians are independently employed.16 Physicians employed by health systems trade their complete autonomy to offset declining reimbursement, reduce operating expenses (including health information technology costs), improve work-life balance, and mitigate unknown risks.
Proponents contend that these mergers allow health care systems to better coordinate care, improve care experiences, accommodate new payment models, and assemble the building blocks needed to form ACOs and other integrated care models. Critics argue that locally dominant systems drive volume (by tightening referral relationships and gaining new market share) and increase costs (through enhanced negotiating leverage and by reclassifying newly acquired physician practices as part of the hospital, thereby generating facility fees). It is unclear whether consolidation results in better outcomes or simply increases overall costs.17
Strategic imperatives
What should gastroenterologists do? First, recognize that FFS is not going away anytime soon.18 Most APMs are still largely in their experimentation phase, and it remains unclear which models will work and which will be broadly adopted. Still, it is unrealistic to expect FFS to indefinitely persist as the dominant payment model. For some services FFS may no longer be a payment option (e.g., Medicare’s BCPI [Bundled Payments for Care Improvement]). For others, FFS rates may become so unattractive that APMs seem necessary. Finally, APMs may allow some practices to capture a greater proportion of overall clinical revenue (e.g., academic practices that perform endoscopic procedures within hospital outpatient departments) and to develop new models that meaningfully improve care. Today’s gastroenterology practices must therefore operate on two separate tracks: an FFS track that rewards volume (most practices are optimized for this) and an alternative payment track that rewards value (few practices can accommodate these on their own). The degree and speed with which practices should reorient to the alternative payment track depends on the type of practice and the specific local health care market. But even practices operating in slower-to-evolve markets should start preparing for the APMs, no matter how far off in the distance they may seem. I recommend the following six steps:
1. Integrate. To participate in APMs, preserve referral streams, and maintain negotiating leverage with health plans, independent, community-based practices may need to affiliate or merge with other physician groups, or align with or be acquired by a health care system.19 Academic practices are challenged to define their role within health care systems that are rapidly adding primary care practices, and often community gastroenterology practices, too.
2. Collaborate and communicate. To deliver high-value care to populations of patients, gastroenterologists must closely collaborate and clearly communicate with primary care physicians and other specialists. Collaborative care agreements can help guide these relationships.203. Develop new models of care. Patients with more routine GI and liver-related problems may be served more cost effectively by midlevel providers21 or innovative solutions, such as e-consultations.22 Patients with complex, chronic GI and liver diseases may be best served by multidisciplinary care teams (e.g., gastroenterologists alongside midlevel providers, nurses, care managers, psychologists, and/or pharmacists) who use clinical information systems to identify high-risk patients and to encourage evidence-based decision making, and who support patients to self-manage their own conditions.23 Previously infeasible in a purely FFS world, these models are encouraged by APMs.
4. Care for common, costly conditions. Most gastroenterology practices have built robust colorectal cancer screening programs, sometimes at the expense of cognitive-based services. In today’s more accountable world, practices that can effectively manage common, costly conditions, such as inflammatory bowel disease, functional GI disorders, and advanced liver diseases, will be rewarded better than before and will be more highly sought as partners.
5. Understand and contain costs. The timely, accurate data needed to effectively respond to APMs are challenging to come by.19 Individual clinicians and group practices can roughly gauge their costs of care for Medicare beneficiaries, compared with other practices, using CMS Quality Resource Utilization Reports. Local commercial insurers may be willing to share cost profiles with interested practices. Strategies to reduce costs may include shifting clinically appropriate patients to more cost-effective settings (especially important for academic practices that see the bulk of their patients in costly hospital outpatient departments), standardizing endoscopy supplies and devices, using anesthesia services more selectively, and preferentially prescribing generic drugs, among others.
6. Measure and demonstrate value. Despite the inherent limitations of performance measurement,24 it is imperative that practices measure and report the value of care to their patients, community, and payers so that they are preferred partners and not locked out of insurance or referral networks. Improving patient experiences is intrinsically worthwhile25 and also makes good business sense.26
References
1. Miller, H.D. Creating payment systems to accelerate value-driven health care: Issues and options for policy reform. New York: The Commonwealth Fund, 2007.
2. Allen, J.I. The road ahead. Clin Gastroenterol Hepatol. 2012;10:692–6.
3. Allen, J.I. Health care reform 3.0: The road gets bumpy. Clin Gastroenterol Hepatol. 2013;11:1527-8.
4. Dorn, S.D., Vesy C.J. Medicare’s revaluation of gastrointestinal endoscopic procedures: Implications for academic and community-based practices. Clin Gastroenterol Hepatol. 2016 (in press).
5. Burwell, S.M. Setting value-based payment goals: HHS efforts to improve U.S. health care (N Engl J Med. 2015;372:897–9).
6. The Advisory Board Company. Commercial Bundled Payment Tracker, 2016.
7. Mechanic, R.E. Mandatory Medicare bundled payment – is it ready for prime time? N Engl J Med. 2015;373:1291–3.
8. The National Commission on Physician Payment Reform. Physician Payment Report, 2013.
9. Brill, J.V., Jain, R., Margolis, P.S., et al. A bundled payment framework for colonoscopy performed for colorectal cancer screening or surveillance. Gastroenterology. 2014;146:849–53, e9.
10. Evans, M. Few Medicare ACOs earned bonuses in 2014. Mod Healthc (2015). Available at: www.modernhealthcare.com/article/20150825/NEWS/150829922. Accessed Nov. 14, 2015.
11. Rau, J., Gold, J. Medicare yet to save money through heralded medical payment model. Kaiser Health News. Available at: http://khn.org/news/medicare-yet-to-save-money-through-heralded-medical-payment-model. Accessed Nov. 14, 2015.
12. Goldmsith, J., Kaufman, N. Pioneer ACOs: Anatomy of a victory. Health Affairs Blog, 2015.
13. Tu, T., Muhlestein, D., Kocot, S.L., et al. The impact of accountable care: Origins and future of accountable care organizations. Washington, D.C.: Brookings Institution, 2015.
14. NCQA. Patient-centered specialty practice frequently asked questions.
15. Xu, T., Wu, A.W., Makary, M.A. The potential hazards of hospital consolidation: Implications for quality, access, and price. JAMA. 2015;314:1337–8.
16. The Physician’s Foundation. 2014 survey of America’s physicians. Practice patterns & perspectives: The Physician’s Foundation.
17. Tsai, T.C., Jha, A.K. Hospital consolidation, competition, and quality: Is bigger necessarily better? JAMA. 2014;312:29–30.
18. Ginsburg, P.B. Fee-for-service will remain a feature of major payment reforms, requiring more changes in Medicare physician payment. Health Aff (Millwood). 2012;31:1977–83.
19. Friedberg, M.W., Chen, P.G., White, C., et al. Effects of health care payment models on physician practice in the United States. Santa Monica, Calif.: RAND Corp., 2015.
20. Greenberg, J.O., Barnett, M.L., Spinks, M.A., et al. The “medical neighborhood”: Integrating primary and specialty care for ambulatory patients. JAMA Intern Med. 2014;174:454–7.
21. Dorn, S.D. Mid-level providers in gastroenterology. Am J Gastroenterol. 2010;105:246–51.
22. Wasfy, J.H., Rao, S.K., Kalwani, N., et al. Longer term impact of cardiology e-consults. Am Heart J. 2016;173:86–93.
23. Coleman, K., Austin, B.T., Brach, C., et al. Evidence on the chronic care model in the new millennium. Health Aff (Millwood). 2009;28:75–85.
24. Dorn, S.D. Quality measurement in gastroenterology: confessions of a realist. Clin Gastroenterol Hepatol. 2016;14:648–50.
25. Berwick, D.M. Measuring physicians’ quality and performance: adrift on Lake Wobegon. JAMA. 2009;302:2485-6.
26. Browne, K., Roseman, D., Shaller, D., et al. Analysis & commentary. Measuring patient experience as a strategy for improving primary care. Health Aff (Millwood). 2010;29:921–5.
Dr. Dorn is vice chief, division of gastroenterology and hepatology, associate professor of medicine, health policy & management, University of North Carolina at Chapel Hill. He has received honoraria for consulting and presentations on health reform from AbbVie and Olympus.