User login
› Schedule twice-monthly visits when prescribing a psychostimulant to assess symptom control, review adverse effects, and record blood pressure, pulse, height, and weight in determining the optimal dose. C
› Keep in mind that using a psychostimulant can put endurance athletes at risk for heat-related injury. C
› Advise college-bound athletes that the NCAA requires a therapeutic use exemption for those who take psychostimulant medications. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
The symptoms typical of attention-deficit/hyperactivity disorder (ADHD)—inability to focus concentration and maintain attention span, and associated hyperactivity—impair normal daily functioning and cause distress for affected individuals.1 For the student athlete with ADHD, sports are a natural outlet, fulfilling the need to be active. In the case of a developing child with ADHD, involvement in sports often is a haven from negative feedback that can occur in the classroom and an environment in which to experience success.
Symptoms of ADHD also may offer an advantage in sports. Impulsivity, or the ability to act without reflection, enables quick decision-making and the spontaneity required of a quarterback or point guard.2 Well-known athletes with ADHD have said that while tasks requiring long stretches of concentration are difficult, aspects of their sport involving instantaneous reactions help them to succeed. Evidence also shows a statistically significant decrease in markers of anxiety and depression among ADHD subjects with higher levels of sports participation.3
Given the positive experience sports can provide, children and adolescents with ADHD are likely to continue participating and be as large a segment of youth athletes as they are of the general population.2,4 Primary care providers often treat student athletes, and in this article we discuss the need for accurate diagnosis through comprehensive clinical evaluation, proper use of psychostimulant medication and other available treatments, and special health concerns for athletes who have ADHD.
Diagnosis: The need for awareness and accurate evaluation
The worldwide prevalence of ADHD is 5.3%.5 In the United States, it is 8.7% among adolescents and 4.4% among adults.6,7 One study of NFL athletes found that 14 of 159 players studied had either ADHD or a learning disability for a combined prevalence of 8.8%.8 ADHD is diagnosed 3 times more often in males than females9; however, studies have shown no gender effect on ADHD, and referral patterns contribute to the higher prevalence pattern for males.10
ADHD usually is diagnosed in childhood, but increasingly, it is not established until adolescence or adulthood.2,9 Although there is no age limit for the diagnosis, the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) calls for the presence of some symptoms before age 12, and symptoms must cause impairment of functioning in multiple settings.1 While hyperactivity symptoms may decrease over time, a significant number of children and adolescents will experience inattention symptoms into adulthood.11 In fact, the disorder may not become evident until college entry, when academic demands overwhelm an individual’s usual coping strategies.2
Multiple reasons for an accurate diagnosis. Initiate evaluation for ADHD for any child 4 to 18 years of age who exhibits symptoms of inattention, hyperactivity, or impulsivity to such a degree that it causes distress or impairment at home, at school, or on the sports field.12 Making an accurate diagnosis of ADHD is vital in student athletes given that treatment, or lack thereof, may put their health at risk and adversely impact their academic and athletic performances. Diagnostic accuracy also aids in distinguishing the student athlete with a legitimate need for treatment from one who is fine and merely looking for a performance enhancer.9 Moreover, having a comprehensive assessment with diagnostic confirmation already in place when an individual enters college greatly facilitates completion of National Collegiate Athletic Association (NCAA) medical exemption documentation.
Essential diagnostic steps. The core clinical evaluation should cover the following:
• Ensure that DSM-5 criteria are met.
• Obtain objective reports to confirm the presence of symptoms in multiple settings. Commonly applied symptom assessment scales include the Brown, Vanderbilt, and Connors questionnaires administered to parents, teachers, and adolescent patients mature enough to complete a self-evaluation.
• Determine whether comorbid conditions are present.
• Rule out medical conditions that can mimic ADHD (eg, lead toxicity or thyroid disorder).
No neurocognitive or laboratory test for ADHD has sufficient sensitivity and specificity to qualify as a standard diagnostic test.2,13 In the future, advanced neuroimaging may provide a means of diagnosing ADHD. Functional magnetic resonance imaging has shown characteristic patterns of reduced activation in the basal ganglia, frontal lobe, and parietal lobes in patients with ADHD.14
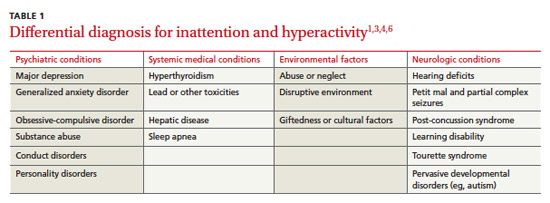
The differential diagnosis for symptoms of inattention and hyperactivity is large (TABLE 1).1,3,4,6 Once underlying medical conditions have been ruled out, screen the patient for mental disorders, including depression and mood disorders, anxiety, and conduct disorders, before concluding that symptoms are likely due to ADHD. When compared with mood disorders, a patient with ADHD will have a persistent course of symptoms rather than periods of recurring and remitting symptoms.2 ADHD is a chronic condition that raises special health care concerns for children and adolescents.12 As many as two-thirds of children with ADHD have at least one coexisting neuropsychiatric condition, and symptoms may overlap, making for a significant diagnostic and management challenge.9 Difficult cases may necessitate consulting a specialist (psychiatrist, neurologist, or neuropsychologist) for guidance. Additionally, in ADHD youth the overall risk of developing a substance use disorder is twice that of children who do not have ADHD.2,15
Treatment: More than medication
Effective treatment for ADHD improves quality of life, decreases the rate of substance abuse, reduces errors when driving vehicles, and decreases the prevalence of comorbid psychological disorders.16,17 Pharmacologic and nonpharmacologic options are available. With athletes, it’s important to be aware of and consider alternatives to medication, particularly given the rules restricting the use of stimulant medication by the NCAA, International Olympic Committee (IOC), and the World Anti-Doping Agency (WADA). The IOC and WADA prohibit any use of stimulant medications, and the NCAA requires a therapeutic-use exemption (TUE) for athletes who take psychostimulant medications (detailed below).3,16
Nonpharmacologic treatment
Published guidelines on managing ADHD show greater agreement on pharmacologic treatment than on psychosocial interventions, based on strength of evidence.18 One evidence-based psychosocial intervention that has shown benefit is behavior therapy, which includes a broad set of specific interventions that modify physical and social environments to change behavior.19 Behavioral training, which primary care providers can introduce to parents, teachers, and coaches, involves the simple principles of reinforcing desired behavior through reward and ignoring undesired behavior to reduce or eliminate it. Consistent application of rewards or unresponsiveness helps patients increase attention to instructions, comply with rules, improve productivity, and decrease disruptive behavior.20
The athlete with ADHD will benefit from a structured environment and, depending on age and level of maturity, can be educated by coaches on self-management strategies such as time management, effective planning and organization, and avoidance of distractions.20 Exercise may help relieve subjective symptoms of ADHD and comorbid mood disorders, but evidence is insufficient to determine its direct impact on ADHD.
Pharmacologic treatment
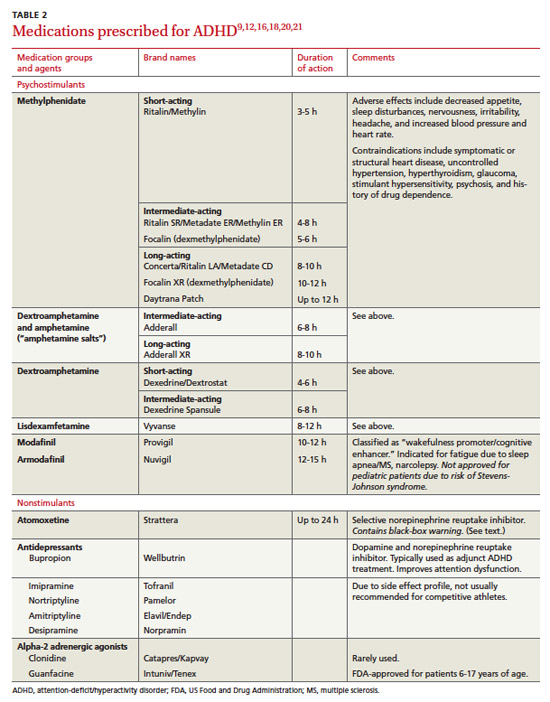
Of the many available medications used to treat ADHD (TABLE 2),9,12,16,18,20,21 psychostimulants are most effective for reducing core symptoms of the disorder.22 It is estimated that 56% of patients with ADHD receive drug therapy, and most of these drugs are psychostimulants.16 These agents increase dopamine and norepinephrine concentrations in the brainstem, midbrain, and frontal cortex, which likely is responsible for increasing attention span and concentration.23 As judged by increased attention or decreased hyperactivity in a recent cohort-based study, the positive response rate to psychostimulants was 73.1%.24
Atomoxetine, a selective norepinephrine reuptake inhibitor, is the primary US Food and Drug Administration (FDA)-approved nonstimulant medication for the treatment of ADHD. In double-blind randomized trials, atomoxetine was roughly equivalent to psychostimulants in reducing target symptoms.21,25 Typically more expensive than psychostimulants, atomoxetine is an acceptable alternative and the more appropriate agent for the ADHD patient with a history of illicit substance abuse or the athlete whose sport bans the use of stimulant medications.
Medication adverse effects. Adverse effects common to psychostimulants are generally mild and include decreased appetite and sleep disturbances. Less common are nervousness, irritability, headache, and increased heart rate and blood pressure (BP).22 Overdose can result in drug-induced psychosis or cardiac arrest.26 Most of these effects are reversible or preventable through dose reduction, increasing the dosing interval, or changing time of dosing during the day. Linear growth rate deceleration in both height and weight may occur in children and adolescents, but this effect is thought to be small and reversible upon discontinuation of medication.27,28
Contraindications to using psychostimulant medications include symptomatic cardiovascular disease, structural heart disease, uncontrolled hypertension, hyperthyroidism, glaucoma, stimulant hypersensitivity, psychosis, and a history of drug dependence.29 Psychostimulants are Schedule II drugs, which means they pose a high potential for abuse and risk for development of physical dependence. The nonstimulant medications listed in TABLE 2 are not Schedule II drugs and, though not as efficacious, generally are safer and lack the adverse effects typically seen with psychostimulants. Atomoxetine, however, carries a black-box warning regarding the risk of suicidality in children and adolescents during the first month of treatment, and patients should be counseled accordingly. Long-term effects of ADHD medications, either adverse or positive, remain unknown; few studies have been done over a period longer than 24 months.25
Medication management
Psychostimulant therapy for ADHD has 3 essential stages: initiation/titration, maintenance, and termination.
With initiation and titration, determining the optimal dose requires twice monthly follow-up visits. With each visit, assess symptom control, review adverse effects, and record BP, pulse, height, and weight. The optimal dose is one at which target outcomes are achieved with minimal adverse effects. Long-acting agents are preferred to enhance compliance, ensure dosing consistency, and reduce abuse potential. If the desired outcome is not being achieved at the highest feasible dose, an alternative psychostimulant may be tried. If a desired response is still not achieved, reevaluate the diagnosis or consider the possibility of comorbid conditions or that the patient has stopped taking the medication.
During the maintenance stage, it is prudent to have monthly contact with the student athlete before writing refill prescription for a Schedule II medication.
Determining when to terminate treatment is a highly individualized decision that entails ongoing analysis of risks vs benefit.9,12,16,26,29 A student athlete’s diagnosis of ADHD might have been based on a positive response to medication in lieu of a comprehensive evaluation, which is regrettable. Response to medication cannot be used to confirm or refute a diagnosis of ADHD because psychostimulant medication will improve behavior in conditions other than ADHD, including learning disability and depression.22
Misuse of psychostimulants among athletes. Some athletes will use a psychostimulant primarily as an appetite suppressant for weight control. However, perceived ergogenic effects are what make psychostimulants especially problematic,16 and are the main reason they are banned from competitive sports. Potential performance enhancements include improved concentration and attention to tasks, increased aggression, decreased pain perception, and euphoria.
A 2006 NCAA study of substance abuse habits of college student athletes (reflecting 2005-2006 data) demonstrated the following findings concerning ergogenic use of psychostimulants:30
• Psychostimulant use has continually increased since 1997 among all student athletes.
• Psychostimulant use has increased across all divisions, with highest use in Division III.
• Psychostimulant use increased in all men’s sports except basketball, football, and swimming.
• Psychostimulant use increased in all women’s sports except tennis, gymnastics, soccer, and volleyball.
• Respondents who used stimulants said they did so to get more energy or to treat ADHD.
• Respondents who didn’t use stimulants said they were concerned about the effect on health, side effects, and going against personal beliefs.30 (The latter issue regarding why student athletes do or do not use specific substances is a focus of the 2012-2013 NCAA National Study of Substance Use Habits of College Student-Athletes, currently underway.)
The rise in the nonprescription use of Adderall among National Football League (NFL) players has become a hot topic. Regarded by the league as a game-day performance enhancer, it has been banned since 2006. Muddying the waters on the true prevalence of Adderall use is the NFL’s policy of silence on identifying the specific performance-enhancing drug that triggered suspension. Only the player, if he so chooses, can disclose the substance in question. It has become convenient for players to name Adderall as the culprit, as it lacks the stigma attached to anabolic steroids and human growth hormone. Whether the drug is being used for ergogenic purposes or as an easy alibi, or both, remains unclear.31
Competition restrictions and therapeutic-use exemption
At the college level and beyond, psychostimulant use is highly regulated in competitive sports. Primary care providers can be supportive by being mindful of existing restrictions when making treatment decisions, and by keeping detailed documentation as stipulated in NCAA policy that became effective on August 1, 2009.30
The policy requires student athletes with ADHD who take psychostimulant medication to provide “evidence that the student athlete has undergone clinical assessment to diagnose the disorder, is being monitored routinely with use of psychostimulant medication and has a current prescription on file.” If the diagnosis of ADHD was made in childhood, policy requires the student athlete to provide their institution with a copy of the comprehensive assessment, including history of treatment. If such documents are not available, then a comprehensive assessment, must be performed to establish the diagnosis.
At minimum, documentation must include a description of the evaluation process and assessment tool(s) used; a statement of the diagnosis; a history of ADHD treatment, both previous and ongoing; a statement that a nonbanned alternative ADHD medication has been considered, if a psychostimulant is currently prescribed; and a statement reflecting evidence of ongoing follow-up/medication monitoring.
If a psychostimulant medication is prescribed, NCAA regulations require that a TUE be included in the documentation. The NCAA asks only that the prescribing physician consider nonstimulants first; they do not require an initial trial of a nonstimulant medication.2,9,16 Per NCAA regulation the student athlete must undergo, at minimum, an annual clinical evaluation by the team physician. The NCAA Committee on Safeguards and Medical Aspects of Sports has issued a new mandatory reporting form that contains criteria, including any known history of substance abuse, to help differentiate legitimate use worthy of medical exemption from use that is abusive.32
The student athlete participating in events sanctioned by WADA or IOC must be aware that use of psychostimulant medication is prohibited in competition. The only FDA-approved ADHD medication allowed for use in competition by all governing bodies is atomoxetine. Encourage student athletes to check governing organization Web sites to review current restrictions on use of psychostimulants in competition. Psychostimulants are banned in all professional sports, though many allow a TUE (except the National Hockey League). The process of obtaining a TUE is rigorous, and Major League Baseball requires a second opinion.2,9,16,33
Specific health concerns for student athletes treated for ADHD
Sudden cardiac death (SCD) is rare among athletes and most often associated with congenital abnormalities affecting heart structure and electrical conduction.16 Although there have been reports of cardiac arrhythmias related to the use of psychostimulants, no compelling clinical evidence has demonstrated a higher incidence of SCD in pediatric ADHD patients treated with psychostimulants compared with the general population.34
The American Academy of Pediatrics, in a policy statement subsequently endorsed by the American Medical Society for Sports Medicine, does not support the routine use of electrocardiograms before initiating psychostimulant therapy.16,34
In light of the cardiovascular side effects of psychostimulants, it remains prudent to obtain a thorough cardiovascular history before starting medication. If no preexisting cardiac disease is identified, psychostimulants can be safely prescribed for the ADHD athlete without worry about the risk of SCD.34
Psychostimulants can confer risk of heat injury
Endurance ADHD athletes on psychostimulants may be at increased risk of heat injury when exercising in warm conditions. Evidence suggests that psychostimulants can increase core temperature while also masking signs and symptoms of fatigue, allowing for a longer duration of exercise and delayed time to exhaustion in the presence of elevated core temperature and heart rate.35
In one placebo-controlled trial of exercise under warm conditions, core temperature measurements in athletes taking 20 mg of methylphenidate often exceeded 104˚F, and the athletes experienced no change in their perception of effort or thermal stress.36 These factors raise concerns for increased risk of heat-related injury in the ADHD athlete taking psychostimulant medication. Close monitoring is required.
Psychostimulant medication, with its direct actions and adverse effects, has great potential for misuse, and the past 10 years have seen a surge in nonprescription stimulant use among adolescents and young adults.26 The reason most commonly given for using a stimulant is to enhance academic performance through improved alertness and sharpened focus.
Adderall is the psychostimulant most in demand as a “study drug.” Among college students, evidence suggests the individual most likely to misuse Adderall is white, male, affiliated with a formal fraternity, and more likely to use other illicit substances.26 Adding to the perpetuation of this phenomenon is that it is relatively stigma-free: Public opinion does not consistently condemn the use of Adderall for academic means, effectively legitimizing nonprescription use.
Very few universities have an academic policy associating nonprescription use of psychostimulants with cheating. The result is an unprecedented demand for psychostimulant medications,37 which are increasingly obtained through diversion by profiteering peers or from clinicians under false pretenses.26
To help curb the problem of misuse, consider stigmatizing such behavior and stress that, in addition to significant health risks associated with inappropriate use, the vast majority of evidence shows no cognitive enhancement with stimulants when compared with placebo in healthy individuals. Given that psychostimulant misuse is more common with an immediate-release formulation, one means of prevention is to restrict legitimate prescriptions to long-acting formulation as much as possible.38-40
Your role as the primary care provider
An optimal treatment plan for the ADHD athlete, especially one using a psychostimulant medication, should always be individualized. Many factors come into play: the nature of impairing symptoms, presence of comorbidities, and prior response to medication.
How the psychostimulant is taken also can vary depending on an athlete’s preference and the nature of the sport. For example, some athletes will take the medication only for academic purposes (studying, testing). Other athletes feel their sport performance improves while on psychostimulants (eg, a baseball catcher who requires game-long concentration), while yet others prefer not to take it during an event so they can remain unfocused, move randomly, and maintain spontaneity (as with a basketball point guard).
If psychostimulants are to be used while playing, it is wise not to initiate therapy during a high-stress event, such as a championship game. In addition, it is important to know when to withhold medication, as in the case of an endurance athlete competing in hot weather.
Coordinating all aspects of care
In providing the best care for the ADHD athlete, the primary care physician must possess comprehensive knowledge of evidence-based best practices. Educate yourself about all available therapies, including behavioral management and use of psychostimulants. And become familiar with available resources and with the referral network (eg, neuropsychologist).
Acknowledgement of NCAA regulations/restrictions is vital to making treatment decisions. In light of the many regulations (both governmental and within the competitive sporting world), consider the use of nonbanned medications and behavioral therapies whenever possible. Throughout the treatment process, involve all stakeholders—parents, athletic trainers, coaches, teachers—to sustain a collaborative approach to care.
Be attentive to signs of inappropriate use of psychostimulant medication (See “Anticipating and addressing the misuse of psychostimulants” above6,37-40). However, fear of potential misuse is not justification for withholding medication, especially when a clear indication is evident. Failure to recognize ADHD as a legitimate problem puts both academic and social hurdles in the path of the student athlete. Evidence shows that adequately treating ADHD with indicated pharmacotherapy actually reduces subsequent substance abuse.41 Finally, education of every ADHD athlete on existing restrictions/regulations/requirements as posed by governing bodies (NCAA, US Anti-Doping Agency, WADA, and IOC) is imperative.
CORRESPONDENCE
Adam E. Perrin, MD, Family Medicine Center at Asylum Hill, University of Connecticut School of Medicine, 99 Woodland Street, Hartford, CT 06105-1207; aperrin@stfranciscare.org
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association Press; 2013.
2. Parr JW. Attention-deficit hyperactivity disorder and the athlete: new advances and understanding. Clin Sports Med. 2011;30:591-610.
3. Kiluk BD, Weden S, Culotta VP. Sport participation and anxiety in children with ADHD. J Atten Disord. 2009;12:499-506.
4. Broshek DK, Freeman JR. Psychiatric and neuropsychological issues in sports medicine. Clin Sports Med. 2005;24:663-679,x.
5. Polanczyk G, de Lima MS, Horta BL, et al. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry. 2006;164:942-948.
6. Merikangas KR, He JP, Burstein M, et al. Lifetime prevalence of mental disorders in US adolescents: results from the National Comorbidity Stud—Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. 2010;49:980-989.
7. Kessler RC, Adler L, Barkley R, et al. The prevalence and correlates of adult ADHD in the United States: results from the National Comorbidity Survey Replication. Am J Psychiatry. 2006;163:716-723.
8. Solomon GS, Haase RF. Biopsychosocial characteristics and neurocognitive test performance in National Football League players: an initial assessment. Arch Clinical Neuropsychol. 2008;23:563-577.
9. Kutcher JS. Treatment of attention-deficit hyperactivity disorder in athletes. Curr Sports Med Reports. 2011;10:32-36.
10 Biederman J, Kwon A, Aleardi M, et al. Absence of gender effects on attention deficit hyperactivity disorder: findings in nonreferred subjects. Am J Psychiatry. 2005;162:1083-1089.
11. Wilens TE, Faraone SV, Biederman J. Attention-deficit/hyperactivity disorder in adults. JAMA. 2004;292:619-623.
12. Subcommittee on Attention-Deficit/Hyperactivity Disorder; Steering Committee on Quality Improvement and Management; Wolraich M, Brown L, Brown RT, et al. ADHD: clinical practice guideline for diagnosis, evaluation, and treatment of attentiondeficit/hyperactivity disorder in children and adolescents. Pediatrics. 2011;128:1007-1022.
13. Boonstra AM, Osterlaan J, Sergeant JA, et al. Executive functioning in adult ADHD: a meta-analytic review. Psychol Med. 2005;35:1097-1108.
14. Silk T, Vance A, Rinehart N, et al. Fronto-parietal activation in attention-deficit/hyperactivity disorder, combined type: functional magnetic resonance imaging study. Br J Psychiatry. 2005;187:282-283.
15. Biederman J, Wilens TE, Mick E, et al. Does attention-deficit hyperactivity disorder impact the developmental course of drug and alcohol abuse and dependence? Biol Psychiatry. 1998;44:269-273.
16. Putukian M, Kreher JB, Coppel DB, et al. Attention deficit hyperactivity disorder and the athlete: an American Medical Society for Sports Medicine position statement. Clin J Sport Med. 2011;21:392-401.
17. Agarwal R, Goldenberg M, Perry R, et al. The quality of life of adults with attention deficit disorder: a systematic review. Innov Clin Neurosci. 2012;9:10-21.
18. Seixas M, Weiss M, Müller U. Systematic review of national and international guidelines on attention-deficit hyperactivity disorder. J Psychopharmacol. 2012;26:753-765.
19. Pelham WE Jr, Fabiano GA. Evidence-based psychosocial treatments for attention-deficit/hyperactivity disorder. J Clin Child Adolesc Psychol. 2008;37:184-214.
20. Searight HR, Burke JM, Rottneck F. Adult ADHD: evaluation and treatment in family medicine. Am Fam Physician. 2000;62:2077-2086,2091-2092.
21. Krull KR. Attention-deficit hyperactivity disorder in children and adolescents: Treatment with medications. Available at: http://www.uptodate.com/contents/attention-deficit-hyperactivitydisorder-in-children-and-adolescents-treatment-with-medications. Accessed March 17, 2014.
22. Conant-Norville DO, Tofler IR. Attention deficit/hyperactivity disorder and psychopharmacologic treatments in the athlete. Clin Sports Med. 2005;24:829-843,viii.
23. Vaidya CJ, Austin G, Kirkorian G, et al. Selective effects of methylphenidate in attention deficit hyperactivity disorder: a functional magnetic resonance study. Proc Natl Acad Sci USA. 1998;95:14494-14499.
24. Barbaresi WJ, Katusic SK, Colligan RC, et al. Long-term stimulant medication treatment of attention-deficit/hyperactivity disorder: results from a population-based study. J Dev Behav Pediatr. 2006;27:1-10.
25. Hanwella R, Senanayake M, de Silva V. Comparative efficacy and acceptability of methylphenidate and atomoxetine in treatment of attention deficit hyperactivity disorder in children and adolescents: a meta-analysis. BMC Psychiatry. 2011;11:176.
26. Lakhan SE, Kirchgessner A. Prescription stimulants in individuals with and without attention deficit hyperactivity disorder: misuse, cognitive impact, and adverse effects. Brain Behav. 2012:2:661-677.
27. Biederman J, Spencer TJ, Monuteaux MC, et al. A naturalistic 10-year prospective study of height and weight in children with attention-deficit hyperactivity disorder grown up: sex and treatment effects. J Pediatr. 2010;157:635-640.
28. Goldman RD. ADHD stimulants and their effect on height in children. Can Fam Physician. 2010;56:145-146.
29. Conant-Norville DO, Tofler IR. Attention deficit/hyperactivity disorder and psychopharmacologic treatments in the athlete. Clin Sports Med. 2005;24:829-843,viii.
30. National Collegiate Athletic Association Web site. 2012-13 NCAA Sports Medicine Handbook. Available at: http://www.ncaa.org/sites/default/files/MD12.pdf. Accessed March 17, 2014.
31. Battista J. Adderall, a drug of focus, is often blamed as NFL suspensions rise. New York Times. December 2, 2012. Available at: http://www.nytimes.com/2012/12/02/sports/football/adderall-a-drug-of-increased-focus-for-nfl-players.html?pagewanted=all&_r=0. Accessed March 17, 2014.
32. CBS Sports Web site. NCAA medical exception documentation reporting form to support the diagnosis of attention deficit hyperactivity disorder (ADHD) and treatment with banned stimulant medication. Available at: http://grfx.cstv.com/photos/schools/grva/genrel/auto_pdf/2012-13/misc_non_event/adhdreporting.pdf. Accessed March 17, 2014.
33. World Anti-Doping Agency Web site. The 2013 list of prohibited substances and methods. Available at: http://www.wada-ama.org/en/Science-Medicine/Prohibited-List/. Accessed March 17, 2014.
34. Perrin JM, Friedman RA, Knilans TK; Black Box Working Group; Section on Cardiology and Cardiac Surgery. Cardiovascular monitoring and stimulant drugs for attention-deficit/hyperactivity disorder. Pediatrics. 2008;122:451-453.
35. Watson P, Hasegawa H, Roelands B, et al. Acute dopamine/noradrenaline reuptake inhibition enhances human exercise performance in warm, but not temperate conditions. J Physiol. 2005;565(pt 3):873-883.
36. Roelands B, Hasegawa H, Watson P, et al. The effects of acute dopamine reuptake inhibition on performance. Med Sci Sports Exerc. 2008;40:879-885.
37. Sinclair L. ADHD drugs on critical list as medication shortages soar. Psychiatric News. Available at: http://psychnews.psychiatryonline.org/newsarticle.aspx?articleid=481189. Accessed March 17, 2014.
38. Forlini C, Gauthier S, Racine E. Should physicians prescribe cognitive enhancers to healthy individuals? CMAJ. 2013;185:1047-1050.
39. McDuff DR, Baron D. Substance abuse in athletes: a sports psychiatry perspective. Clin Sports Med. 2005;24:885-897,ix-x.
40. Desantis AD, Hane AC. “Adderall is definitely not a drug”: justifications for the illegal use of ADHD stimulants. Subst Use Misuse. 2010;45:31-46.
41. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111:179-185.
› Schedule twice-monthly visits when prescribing a psychostimulant to assess symptom control, review adverse effects, and record blood pressure, pulse, height, and weight in determining the optimal dose. C
› Keep in mind that using a psychostimulant can put endurance athletes at risk for heat-related injury. C
› Advise college-bound athletes that the NCAA requires a therapeutic use exemption for those who take psychostimulant medications. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
The symptoms typical of attention-deficit/hyperactivity disorder (ADHD)—inability to focus concentration and maintain attention span, and associated hyperactivity—impair normal daily functioning and cause distress for affected individuals.1 For the student athlete with ADHD, sports are a natural outlet, fulfilling the need to be active. In the case of a developing child with ADHD, involvement in sports often is a haven from negative feedback that can occur in the classroom and an environment in which to experience success.
Symptoms of ADHD also may offer an advantage in sports. Impulsivity, or the ability to act without reflection, enables quick decision-making and the spontaneity required of a quarterback or point guard.2 Well-known athletes with ADHD have said that while tasks requiring long stretches of concentration are difficult, aspects of their sport involving instantaneous reactions help them to succeed. Evidence also shows a statistically significant decrease in markers of anxiety and depression among ADHD subjects with higher levels of sports participation.3
Given the positive experience sports can provide, children and adolescents with ADHD are likely to continue participating and be as large a segment of youth athletes as they are of the general population.2,4 Primary care providers often treat student athletes, and in this article we discuss the need for accurate diagnosis through comprehensive clinical evaluation, proper use of psychostimulant medication and other available treatments, and special health concerns for athletes who have ADHD.
Diagnosis: The need for awareness and accurate evaluation
The worldwide prevalence of ADHD is 5.3%.5 In the United States, it is 8.7% among adolescents and 4.4% among adults.6,7 One study of NFL athletes found that 14 of 159 players studied had either ADHD or a learning disability for a combined prevalence of 8.8%.8 ADHD is diagnosed 3 times more often in males than females9; however, studies have shown no gender effect on ADHD, and referral patterns contribute to the higher prevalence pattern for males.10
ADHD usually is diagnosed in childhood, but increasingly, it is not established until adolescence or adulthood.2,9 Although there is no age limit for the diagnosis, the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) calls for the presence of some symptoms before age 12, and symptoms must cause impairment of functioning in multiple settings.1 While hyperactivity symptoms may decrease over time, a significant number of children and adolescents will experience inattention symptoms into adulthood.11 In fact, the disorder may not become evident until college entry, when academic demands overwhelm an individual’s usual coping strategies.2
Multiple reasons for an accurate diagnosis. Initiate evaluation for ADHD for any child 4 to 18 years of age who exhibits symptoms of inattention, hyperactivity, or impulsivity to such a degree that it causes distress or impairment at home, at school, or on the sports field.12 Making an accurate diagnosis of ADHD is vital in student athletes given that treatment, or lack thereof, may put their health at risk and adversely impact their academic and athletic performances. Diagnostic accuracy also aids in distinguishing the student athlete with a legitimate need for treatment from one who is fine and merely looking for a performance enhancer.9 Moreover, having a comprehensive assessment with diagnostic confirmation already in place when an individual enters college greatly facilitates completion of National Collegiate Athletic Association (NCAA) medical exemption documentation.
Essential diagnostic steps. The core clinical evaluation should cover the following:
• Ensure that DSM-5 criteria are met.
• Obtain objective reports to confirm the presence of symptoms in multiple settings. Commonly applied symptom assessment scales include the Brown, Vanderbilt, and Connors questionnaires administered to parents, teachers, and adolescent patients mature enough to complete a self-evaluation.
• Determine whether comorbid conditions are present.
• Rule out medical conditions that can mimic ADHD (eg, lead toxicity or thyroid disorder).
No neurocognitive or laboratory test for ADHD has sufficient sensitivity and specificity to qualify as a standard diagnostic test.2,13 In the future, advanced neuroimaging may provide a means of diagnosing ADHD. Functional magnetic resonance imaging has shown characteristic patterns of reduced activation in the basal ganglia, frontal lobe, and parietal lobes in patients with ADHD.14
The differential diagnosis for symptoms of inattention and hyperactivity is large (TABLE 1).1,3,4,6 Once underlying medical conditions have been ruled out, screen the patient for mental disorders, including depression and mood disorders, anxiety, and conduct disorders, before concluding that symptoms are likely due to ADHD. When compared with mood disorders, a patient with ADHD will have a persistent course of symptoms rather than periods of recurring and remitting symptoms.2 ADHD is a chronic condition that raises special health care concerns for children and adolescents.12 As many as two-thirds of children with ADHD have at least one coexisting neuropsychiatric condition, and symptoms may overlap, making for a significant diagnostic and management challenge.9 Difficult cases may necessitate consulting a specialist (psychiatrist, neurologist, or neuropsychologist) for guidance. Additionally, in ADHD youth the overall risk of developing a substance use disorder is twice that of children who do not have ADHD.2,15
Treatment: More than medication
Effective treatment for ADHD improves quality of life, decreases the rate of substance abuse, reduces errors when driving vehicles, and decreases the prevalence of comorbid psychological disorders.16,17 Pharmacologic and nonpharmacologic options are available. With athletes, it’s important to be aware of and consider alternatives to medication, particularly given the rules restricting the use of stimulant medication by the NCAA, International Olympic Committee (IOC), and the World Anti-Doping Agency (WADA). The IOC and WADA prohibit any use of stimulant medications, and the NCAA requires a therapeutic-use exemption (TUE) for athletes who take psychostimulant medications (detailed below).3,16
Nonpharmacologic treatment
Published guidelines on managing ADHD show greater agreement on pharmacologic treatment than on psychosocial interventions, based on strength of evidence.18 One evidence-based psychosocial intervention that has shown benefit is behavior therapy, which includes a broad set of specific interventions that modify physical and social environments to change behavior.19 Behavioral training, which primary care providers can introduce to parents, teachers, and coaches, involves the simple principles of reinforcing desired behavior through reward and ignoring undesired behavior to reduce or eliminate it. Consistent application of rewards or unresponsiveness helps patients increase attention to instructions, comply with rules, improve productivity, and decrease disruptive behavior.20
The athlete with ADHD will benefit from a structured environment and, depending on age and level of maturity, can be educated by coaches on self-management strategies such as time management, effective planning and organization, and avoidance of distractions.20 Exercise may help relieve subjective symptoms of ADHD and comorbid mood disorders, but evidence is insufficient to determine its direct impact on ADHD.
Pharmacologic treatment
Of the many available medications used to treat ADHD (TABLE 2),9,12,16,18,20,21 psychostimulants are most effective for reducing core symptoms of the disorder.22 It is estimated that 56% of patients with ADHD receive drug therapy, and most of these drugs are psychostimulants.16 These agents increase dopamine and norepinephrine concentrations in the brainstem, midbrain, and frontal cortex, which likely is responsible for increasing attention span and concentration.23 As judged by increased attention or decreased hyperactivity in a recent cohort-based study, the positive response rate to psychostimulants was 73.1%.24
Atomoxetine, a selective norepinephrine reuptake inhibitor, is the primary US Food and Drug Administration (FDA)-approved nonstimulant medication for the treatment of ADHD. In double-blind randomized trials, atomoxetine was roughly equivalent to psychostimulants in reducing target symptoms.21,25 Typically more expensive than psychostimulants, atomoxetine is an acceptable alternative and the more appropriate agent for the ADHD patient with a history of illicit substance abuse or the athlete whose sport bans the use of stimulant medications.
Medication adverse effects. Adverse effects common to psychostimulants are generally mild and include decreased appetite and sleep disturbances. Less common are nervousness, irritability, headache, and increased heart rate and blood pressure (BP).22 Overdose can result in drug-induced psychosis or cardiac arrest.26 Most of these effects are reversible or preventable through dose reduction, increasing the dosing interval, or changing time of dosing during the day. Linear growth rate deceleration in both height and weight may occur in children and adolescents, but this effect is thought to be small and reversible upon discontinuation of medication.27,28
Contraindications to using psychostimulant medications include symptomatic cardiovascular disease, structural heart disease, uncontrolled hypertension, hyperthyroidism, glaucoma, stimulant hypersensitivity, psychosis, and a history of drug dependence.29 Psychostimulants are Schedule II drugs, which means they pose a high potential for abuse and risk for development of physical dependence. The nonstimulant medications listed in TABLE 2 are not Schedule II drugs and, though not as efficacious, generally are safer and lack the adverse effects typically seen with psychostimulants. Atomoxetine, however, carries a black-box warning regarding the risk of suicidality in children and adolescents during the first month of treatment, and patients should be counseled accordingly. Long-term effects of ADHD medications, either adverse or positive, remain unknown; few studies have been done over a period longer than 24 months.25
Medication management
Psychostimulant therapy for ADHD has 3 essential stages: initiation/titration, maintenance, and termination.
With initiation and titration, determining the optimal dose requires twice monthly follow-up visits. With each visit, assess symptom control, review adverse effects, and record BP, pulse, height, and weight. The optimal dose is one at which target outcomes are achieved with minimal adverse effects. Long-acting agents are preferred to enhance compliance, ensure dosing consistency, and reduce abuse potential. If the desired outcome is not being achieved at the highest feasible dose, an alternative psychostimulant may be tried. If a desired response is still not achieved, reevaluate the diagnosis or consider the possibility of comorbid conditions or that the patient has stopped taking the medication.
During the maintenance stage, it is prudent to have monthly contact with the student athlete before writing refill prescription for a Schedule II medication.
Determining when to terminate treatment is a highly individualized decision that entails ongoing analysis of risks vs benefit.9,12,16,26,29 A student athlete’s diagnosis of ADHD might have been based on a positive response to medication in lieu of a comprehensive evaluation, which is regrettable. Response to medication cannot be used to confirm or refute a diagnosis of ADHD because psychostimulant medication will improve behavior in conditions other than ADHD, including learning disability and depression.22
Misuse of psychostimulants among athletes. Some athletes will use a psychostimulant primarily as an appetite suppressant for weight control. However, perceived ergogenic effects are what make psychostimulants especially problematic,16 and are the main reason they are banned from competitive sports. Potential performance enhancements include improved concentration and attention to tasks, increased aggression, decreased pain perception, and euphoria.
A 2006 NCAA study of substance abuse habits of college student athletes (reflecting 2005-2006 data) demonstrated the following findings concerning ergogenic use of psychostimulants:30
• Psychostimulant use has continually increased since 1997 among all student athletes.
• Psychostimulant use has increased across all divisions, with highest use in Division III.
• Psychostimulant use increased in all men’s sports except basketball, football, and swimming.
• Psychostimulant use increased in all women’s sports except tennis, gymnastics, soccer, and volleyball.
• Respondents who used stimulants said they did so to get more energy or to treat ADHD.
• Respondents who didn’t use stimulants said they were concerned about the effect on health, side effects, and going against personal beliefs.30 (The latter issue regarding why student athletes do or do not use specific substances is a focus of the 2012-2013 NCAA National Study of Substance Use Habits of College Student-Athletes, currently underway.)
The rise in the nonprescription use of Adderall among National Football League (NFL) players has become a hot topic. Regarded by the league as a game-day performance enhancer, it has been banned since 2006. Muddying the waters on the true prevalence of Adderall use is the NFL’s policy of silence on identifying the specific performance-enhancing drug that triggered suspension. Only the player, if he so chooses, can disclose the substance in question. It has become convenient for players to name Adderall as the culprit, as it lacks the stigma attached to anabolic steroids and human growth hormone. Whether the drug is being used for ergogenic purposes or as an easy alibi, or both, remains unclear.31
Competition restrictions and therapeutic-use exemption
At the college level and beyond, psychostimulant use is highly regulated in competitive sports. Primary care providers can be supportive by being mindful of existing restrictions when making treatment decisions, and by keeping detailed documentation as stipulated in NCAA policy that became effective on August 1, 2009.30
The policy requires student athletes with ADHD who take psychostimulant medication to provide “evidence that the student athlete has undergone clinical assessment to diagnose the disorder, is being monitored routinely with use of psychostimulant medication and has a current prescription on file.” If the diagnosis of ADHD was made in childhood, policy requires the student athlete to provide their institution with a copy of the comprehensive assessment, including history of treatment. If such documents are not available, then a comprehensive assessment, must be performed to establish the diagnosis.
At minimum, documentation must include a description of the evaluation process and assessment tool(s) used; a statement of the diagnosis; a history of ADHD treatment, both previous and ongoing; a statement that a nonbanned alternative ADHD medication has been considered, if a psychostimulant is currently prescribed; and a statement reflecting evidence of ongoing follow-up/medication monitoring.
If a psychostimulant medication is prescribed, NCAA regulations require that a TUE be included in the documentation. The NCAA asks only that the prescribing physician consider nonstimulants first; they do not require an initial trial of a nonstimulant medication.2,9,16 Per NCAA regulation the student athlete must undergo, at minimum, an annual clinical evaluation by the team physician. The NCAA Committee on Safeguards and Medical Aspects of Sports has issued a new mandatory reporting form that contains criteria, including any known history of substance abuse, to help differentiate legitimate use worthy of medical exemption from use that is abusive.32
The student athlete participating in events sanctioned by WADA or IOC must be aware that use of psychostimulant medication is prohibited in competition. The only FDA-approved ADHD medication allowed for use in competition by all governing bodies is atomoxetine. Encourage student athletes to check governing organization Web sites to review current restrictions on use of psychostimulants in competition. Psychostimulants are banned in all professional sports, though many allow a TUE (except the National Hockey League). The process of obtaining a TUE is rigorous, and Major League Baseball requires a second opinion.2,9,16,33
Specific health concerns for student athletes treated for ADHD
Sudden cardiac death (SCD) is rare among athletes and most often associated with congenital abnormalities affecting heart structure and electrical conduction.16 Although there have been reports of cardiac arrhythmias related to the use of psychostimulants, no compelling clinical evidence has demonstrated a higher incidence of SCD in pediatric ADHD patients treated with psychostimulants compared with the general population.34
The American Academy of Pediatrics, in a policy statement subsequently endorsed by the American Medical Society for Sports Medicine, does not support the routine use of electrocardiograms before initiating psychostimulant therapy.16,34
In light of the cardiovascular side effects of psychostimulants, it remains prudent to obtain a thorough cardiovascular history before starting medication. If no preexisting cardiac disease is identified, psychostimulants can be safely prescribed for the ADHD athlete without worry about the risk of SCD.34
Psychostimulants can confer risk of heat injury
Endurance ADHD athletes on psychostimulants may be at increased risk of heat injury when exercising in warm conditions. Evidence suggests that psychostimulants can increase core temperature while also masking signs and symptoms of fatigue, allowing for a longer duration of exercise and delayed time to exhaustion in the presence of elevated core temperature and heart rate.35
In one placebo-controlled trial of exercise under warm conditions, core temperature measurements in athletes taking 20 mg of methylphenidate often exceeded 104˚F, and the athletes experienced no change in their perception of effort or thermal stress.36 These factors raise concerns for increased risk of heat-related injury in the ADHD athlete taking psychostimulant medication. Close monitoring is required.
Psychostimulant medication, with its direct actions and adverse effects, has great potential for misuse, and the past 10 years have seen a surge in nonprescription stimulant use among adolescents and young adults.26 The reason most commonly given for using a stimulant is to enhance academic performance through improved alertness and sharpened focus.
Adderall is the psychostimulant most in demand as a “study drug.” Among college students, evidence suggests the individual most likely to misuse Adderall is white, male, affiliated with a formal fraternity, and more likely to use other illicit substances.26 Adding to the perpetuation of this phenomenon is that it is relatively stigma-free: Public opinion does not consistently condemn the use of Adderall for academic means, effectively legitimizing nonprescription use.
Very few universities have an academic policy associating nonprescription use of psychostimulants with cheating. The result is an unprecedented demand for psychostimulant medications,37 which are increasingly obtained through diversion by profiteering peers or from clinicians under false pretenses.26
To help curb the problem of misuse, consider stigmatizing such behavior and stress that, in addition to significant health risks associated with inappropriate use, the vast majority of evidence shows no cognitive enhancement with stimulants when compared with placebo in healthy individuals. Given that psychostimulant misuse is more common with an immediate-release formulation, one means of prevention is to restrict legitimate prescriptions to long-acting formulation as much as possible.38-40
Your role as the primary care provider
An optimal treatment plan for the ADHD athlete, especially one using a psychostimulant medication, should always be individualized. Many factors come into play: the nature of impairing symptoms, presence of comorbidities, and prior response to medication.
How the psychostimulant is taken also can vary depending on an athlete’s preference and the nature of the sport. For example, some athletes will take the medication only for academic purposes (studying, testing). Other athletes feel their sport performance improves while on psychostimulants (eg, a baseball catcher who requires game-long concentration), while yet others prefer not to take it during an event so they can remain unfocused, move randomly, and maintain spontaneity (as with a basketball point guard).
If psychostimulants are to be used while playing, it is wise not to initiate therapy during a high-stress event, such as a championship game. In addition, it is important to know when to withhold medication, as in the case of an endurance athlete competing in hot weather.
Coordinating all aspects of care
In providing the best care for the ADHD athlete, the primary care physician must possess comprehensive knowledge of evidence-based best practices. Educate yourself about all available therapies, including behavioral management and use of psychostimulants. And become familiar with available resources and with the referral network (eg, neuropsychologist).
Acknowledgement of NCAA regulations/restrictions is vital to making treatment decisions. In light of the many regulations (both governmental and within the competitive sporting world), consider the use of nonbanned medications and behavioral therapies whenever possible. Throughout the treatment process, involve all stakeholders—parents, athletic trainers, coaches, teachers—to sustain a collaborative approach to care.
Be attentive to signs of inappropriate use of psychostimulant medication (See “Anticipating and addressing the misuse of psychostimulants” above6,37-40). However, fear of potential misuse is not justification for withholding medication, especially when a clear indication is evident. Failure to recognize ADHD as a legitimate problem puts both academic and social hurdles in the path of the student athlete. Evidence shows that adequately treating ADHD with indicated pharmacotherapy actually reduces subsequent substance abuse.41 Finally, education of every ADHD athlete on existing restrictions/regulations/requirements as posed by governing bodies (NCAA, US Anti-Doping Agency, WADA, and IOC) is imperative.
CORRESPONDENCE
Adam E. Perrin, MD, Family Medicine Center at Asylum Hill, University of Connecticut School of Medicine, 99 Woodland Street, Hartford, CT 06105-1207; aperrin@stfranciscare.org
› Schedule twice-monthly visits when prescribing a psychostimulant to assess symptom control, review adverse effects, and record blood pressure, pulse, height, and weight in determining the optimal dose. C
› Keep in mind that using a psychostimulant can put endurance athletes at risk for heat-related injury. C
› Advise college-bound athletes that the NCAA requires a therapeutic use exemption for those who take psychostimulant medications. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
The symptoms typical of attention-deficit/hyperactivity disorder (ADHD)—inability to focus concentration and maintain attention span, and associated hyperactivity—impair normal daily functioning and cause distress for affected individuals.1 For the student athlete with ADHD, sports are a natural outlet, fulfilling the need to be active. In the case of a developing child with ADHD, involvement in sports often is a haven from negative feedback that can occur in the classroom and an environment in which to experience success.
Symptoms of ADHD also may offer an advantage in sports. Impulsivity, or the ability to act without reflection, enables quick decision-making and the spontaneity required of a quarterback or point guard.2 Well-known athletes with ADHD have said that while tasks requiring long stretches of concentration are difficult, aspects of their sport involving instantaneous reactions help them to succeed. Evidence also shows a statistically significant decrease in markers of anxiety and depression among ADHD subjects with higher levels of sports participation.3
Given the positive experience sports can provide, children and adolescents with ADHD are likely to continue participating and be as large a segment of youth athletes as they are of the general population.2,4 Primary care providers often treat student athletes, and in this article we discuss the need for accurate diagnosis through comprehensive clinical evaluation, proper use of psychostimulant medication and other available treatments, and special health concerns for athletes who have ADHD.
Diagnosis: The need for awareness and accurate evaluation
The worldwide prevalence of ADHD is 5.3%.5 In the United States, it is 8.7% among adolescents and 4.4% among adults.6,7 One study of NFL athletes found that 14 of 159 players studied had either ADHD or a learning disability for a combined prevalence of 8.8%.8 ADHD is diagnosed 3 times more often in males than females9; however, studies have shown no gender effect on ADHD, and referral patterns contribute to the higher prevalence pattern for males.10
ADHD usually is diagnosed in childhood, but increasingly, it is not established until adolescence or adulthood.2,9 Although there is no age limit for the diagnosis, the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) calls for the presence of some symptoms before age 12, and symptoms must cause impairment of functioning in multiple settings.1 While hyperactivity symptoms may decrease over time, a significant number of children and adolescents will experience inattention symptoms into adulthood.11 In fact, the disorder may not become evident until college entry, when academic demands overwhelm an individual’s usual coping strategies.2
Multiple reasons for an accurate diagnosis. Initiate evaluation for ADHD for any child 4 to 18 years of age who exhibits symptoms of inattention, hyperactivity, or impulsivity to such a degree that it causes distress or impairment at home, at school, or on the sports field.12 Making an accurate diagnosis of ADHD is vital in student athletes given that treatment, or lack thereof, may put their health at risk and adversely impact their academic and athletic performances. Diagnostic accuracy also aids in distinguishing the student athlete with a legitimate need for treatment from one who is fine and merely looking for a performance enhancer.9 Moreover, having a comprehensive assessment with diagnostic confirmation already in place when an individual enters college greatly facilitates completion of National Collegiate Athletic Association (NCAA) medical exemption documentation.
Essential diagnostic steps. The core clinical evaluation should cover the following:
• Ensure that DSM-5 criteria are met.
• Obtain objective reports to confirm the presence of symptoms in multiple settings. Commonly applied symptom assessment scales include the Brown, Vanderbilt, and Connors questionnaires administered to parents, teachers, and adolescent patients mature enough to complete a self-evaluation.
• Determine whether comorbid conditions are present.
• Rule out medical conditions that can mimic ADHD (eg, lead toxicity or thyroid disorder).
No neurocognitive or laboratory test for ADHD has sufficient sensitivity and specificity to qualify as a standard diagnostic test.2,13 In the future, advanced neuroimaging may provide a means of diagnosing ADHD. Functional magnetic resonance imaging has shown characteristic patterns of reduced activation in the basal ganglia, frontal lobe, and parietal lobes in patients with ADHD.14
The differential diagnosis for symptoms of inattention and hyperactivity is large (TABLE 1).1,3,4,6 Once underlying medical conditions have been ruled out, screen the patient for mental disorders, including depression and mood disorders, anxiety, and conduct disorders, before concluding that symptoms are likely due to ADHD. When compared with mood disorders, a patient with ADHD will have a persistent course of symptoms rather than periods of recurring and remitting symptoms.2 ADHD is a chronic condition that raises special health care concerns for children and adolescents.12 As many as two-thirds of children with ADHD have at least one coexisting neuropsychiatric condition, and symptoms may overlap, making for a significant diagnostic and management challenge.9 Difficult cases may necessitate consulting a specialist (psychiatrist, neurologist, or neuropsychologist) for guidance. Additionally, in ADHD youth the overall risk of developing a substance use disorder is twice that of children who do not have ADHD.2,15
Treatment: More than medication
Effective treatment for ADHD improves quality of life, decreases the rate of substance abuse, reduces errors when driving vehicles, and decreases the prevalence of comorbid psychological disorders.16,17 Pharmacologic and nonpharmacologic options are available. With athletes, it’s important to be aware of and consider alternatives to medication, particularly given the rules restricting the use of stimulant medication by the NCAA, International Olympic Committee (IOC), and the World Anti-Doping Agency (WADA). The IOC and WADA prohibit any use of stimulant medications, and the NCAA requires a therapeutic-use exemption (TUE) for athletes who take psychostimulant medications (detailed below).3,16
Nonpharmacologic treatment
Published guidelines on managing ADHD show greater agreement on pharmacologic treatment than on psychosocial interventions, based on strength of evidence.18 One evidence-based psychosocial intervention that has shown benefit is behavior therapy, which includes a broad set of specific interventions that modify physical and social environments to change behavior.19 Behavioral training, which primary care providers can introduce to parents, teachers, and coaches, involves the simple principles of reinforcing desired behavior through reward and ignoring undesired behavior to reduce or eliminate it. Consistent application of rewards or unresponsiveness helps patients increase attention to instructions, comply with rules, improve productivity, and decrease disruptive behavior.20
The athlete with ADHD will benefit from a structured environment and, depending on age and level of maturity, can be educated by coaches on self-management strategies such as time management, effective planning and organization, and avoidance of distractions.20 Exercise may help relieve subjective symptoms of ADHD and comorbid mood disorders, but evidence is insufficient to determine its direct impact on ADHD.
Pharmacologic treatment
Of the many available medications used to treat ADHD (TABLE 2),9,12,16,18,20,21 psychostimulants are most effective for reducing core symptoms of the disorder.22 It is estimated that 56% of patients with ADHD receive drug therapy, and most of these drugs are psychostimulants.16 These agents increase dopamine and norepinephrine concentrations in the brainstem, midbrain, and frontal cortex, which likely is responsible for increasing attention span and concentration.23 As judged by increased attention or decreased hyperactivity in a recent cohort-based study, the positive response rate to psychostimulants was 73.1%.24
Atomoxetine, a selective norepinephrine reuptake inhibitor, is the primary US Food and Drug Administration (FDA)-approved nonstimulant medication for the treatment of ADHD. In double-blind randomized trials, atomoxetine was roughly equivalent to psychostimulants in reducing target symptoms.21,25 Typically more expensive than psychostimulants, atomoxetine is an acceptable alternative and the more appropriate agent for the ADHD patient with a history of illicit substance abuse or the athlete whose sport bans the use of stimulant medications.
Medication adverse effects. Adverse effects common to psychostimulants are generally mild and include decreased appetite and sleep disturbances. Less common are nervousness, irritability, headache, and increased heart rate and blood pressure (BP).22 Overdose can result in drug-induced psychosis or cardiac arrest.26 Most of these effects are reversible or preventable through dose reduction, increasing the dosing interval, or changing time of dosing during the day. Linear growth rate deceleration in both height and weight may occur in children and adolescents, but this effect is thought to be small and reversible upon discontinuation of medication.27,28
Contraindications to using psychostimulant medications include symptomatic cardiovascular disease, structural heart disease, uncontrolled hypertension, hyperthyroidism, glaucoma, stimulant hypersensitivity, psychosis, and a history of drug dependence.29 Psychostimulants are Schedule II drugs, which means they pose a high potential for abuse and risk for development of physical dependence. The nonstimulant medications listed in TABLE 2 are not Schedule II drugs and, though not as efficacious, generally are safer and lack the adverse effects typically seen with psychostimulants. Atomoxetine, however, carries a black-box warning regarding the risk of suicidality in children and adolescents during the first month of treatment, and patients should be counseled accordingly. Long-term effects of ADHD medications, either adverse or positive, remain unknown; few studies have been done over a period longer than 24 months.25
Medication management
Psychostimulant therapy for ADHD has 3 essential stages: initiation/titration, maintenance, and termination.
With initiation and titration, determining the optimal dose requires twice monthly follow-up visits. With each visit, assess symptom control, review adverse effects, and record BP, pulse, height, and weight. The optimal dose is one at which target outcomes are achieved with minimal adverse effects. Long-acting agents are preferred to enhance compliance, ensure dosing consistency, and reduce abuse potential. If the desired outcome is not being achieved at the highest feasible dose, an alternative psychostimulant may be tried. If a desired response is still not achieved, reevaluate the diagnosis or consider the possibility of comorbid conditions or that the patient has stopped taking the medication.
During the maintenance stage, it is prudent to have monthly contact with the student athlete before writing refill prescription for a Schedule II medication.
Determining when to terminate treatment is a highly individualized decision that entails ongoing analysis of risks vs benefit.9,12,16,26,29 A student athlete’s diagnosis of ADHD might have been based on a positive response to medication in lieu of a comprehensive evaluation, which is regrettable. Response to medication cannot be used to confirm or refute a diagnosis of ADHD because psychostimulant medication will improve behavior in conditions other than ADHD, including learning disability and depression.22
Misuse of psychostimulants among athletes. Some athletes will use a psychostimulant primarily as an appetite suppressant for weight control. However, perceived ergogenic effects are what make psychostimulants especially problematic,16 and are the main reason they are banned from competitive sports. Potential performance enhancements include improved concentration and attention to tasks, increased aggression, decreased pain perception, and euphoria.
A 2006 NCAA study of substance abuse habits of college student athletes (reflecting 2005-2006 data) demonstrated the following findings concerning ergogenic use of psychostimulants:30
• Psychostimulant use has continually increased since 1997 among all student athletes.
• Psychostimulant use has increased across all divisions, with highest use in Division III.
• Psychostimulant use increased in all men’s sports except basketball, football, and swimming.
• Psychostimulant use increased in all women’s sports except tennis, gymnastics, soccer, and volleyball.
• Respondents who used stimulants said they did so to get more energy or to treat ADHD.
• Respondents who didn’t use stimulants said they were concerned about the effect on health, side effects, and going against personal beliefs.30 (The latter issue regarding why student athletes do or do not use specific substances is a focus of the 2012-2013 NCAA National Study of Substance Use Habits of College Student-Athletes, currently underway.)
The rise in the nonprescription use of Adderall among National Football League (NFL) players has become a hot topic. Regarded by the league as a game-day performance enhancer, it has been banned since 2006. Muddying the waters on the true prevalence of Adderall use is the NFL’s policy of silence on identifying the specific performance-enhancing drug that triggered suspension. Only the player, if he so chooses, can disclose the substance in question. It has become convenient for players to name Adderall as the culprit, as it lacks the stigma attached to anabolic steroids and human growth hormone. Whether the drug is being used for ergogenic purposes or as an easy alibi, or both, remains unclear.31
Competition restrictions and therapeutic-use exemption
At the college level and beyond, psychostimulant use is highly regulated in competitive sports. Primary care providers can be supportive by being mindful of existing restrictions when making treatment decisions, and by keeping detailed documentation as stipulated in NCAA policy that became effective on August 1, 2009.30
The policy requires student athletes with ADHD who take psychostimulant medication to provide “evidence that the student athlete has undergone clinical assessment to diagnose the disorder, is being monitored routinely with use of psychostimulant medication and has a current prescription on file.” If the diagnosis of ADHD was made in childhood, policy requires the student athlete to provide their institution with a copy of the comprehensive assessment, including history of treatment. If such documents are not available, then a comprehensive assessment, must be performed to establish the diagnosis.
At minimum, documentation must include a description of the evaluation process and assessment tool(s) used; a statement of the diagnosis; a history of ADHD treatment, both previous and ongoing; a statement that a nonbanned alternative ADHD medication has been considered, if a psychostimulant is currently prescribed; and a statement reflecting evidence of ongoing follow-up/medication monitoring.
If a psychostimulant medication is prescribed, NCAA regulations require that a TUE be included in the documentation. The NCAA asks only that the prescribing physician consider nonstimulants first; they do not require an initial trial of a nonstimulant medication.2,9,16 Per NCAA regulation the student athlete must undergo, at minimum, an annual clinical evaluation by the team physician. The NCAA Committee on Safeguards and Medical Aspects of Sports has issued a new mandatory reporting form that contains criteria, including any known history of substance abuse, to help differentiate legitimate use worthy of medical exemption from use that is abusive.32
The student athlete participating in events sanctioned by WADA or IOC must be aware that use of psychostimulant medication is prohibited in competition. The only FDA-approved ADHD medication allowed for use in competition by all governing bodies is atomoxetine. Encourage student athletes to check governing organization Web sites to review current restrictions on use of psychostimulants in competition. Psychostimulants are banned in all professional sports, though many allow a TUE (except the National Hockey League). The process of obtaining a TUE is rigorous, and Major League Baseball requires a second opinion.2,9,16,33
Specific health concerns for student athletes treated for ADHD
Sudden cardiac death (SCD) is rare among athletes and most often associated with congenital abnormalities affecting heart structure and electrical conduction.16 Although there have been reports of cardiac arrhythmias related to the use of psychostimulants, no compelling clinical evidence has demonstrated a higher incidence of SCD in pediatric ADHD patients treated with psychostimulants compared with the general population.34
The American Academy of Pediatrics, in a policy statement subsequently endorsed by the American Medical Society for Sports Medicine, does not support the routine use of electrocardiograms before initiating psychostimulant therapy.16,34
In light of the cardiovascular side effects of psychostimulants, it remains prudent to obtain a thorough cardiovascular history before starting medication. If no preexisting cardiac disease is identified, psychostimulants can be safely prescribed for the ADHD athlete without worry about the risk of SCD.34
Psychostimulants can confer risk of heat injury
Endurance ADHD athletes on psychostimulants may be at increased risk of heat injury when exercising in warm conditions. Evidence suggests that psychostimulants can increase core temperature while also masking signs and symptoms of fatigue, allowing for a longer duration of exercise and delayed time to exhaustion in the presence of elevated core temperature and heart rate.35
In one placebo-controlled trial of exercise under warm conditions, core temperature measurements in athletes taking 20 mg of methylphenidate often exceeded 104˚F, and the athletes experienced no change in their perception of effort or thermal stress.36 These factors raise concerns for increased risk of heat-related injury in the ADHD athlete taking psychostimulant medication. Close monitoring is required.
Psychostimulant medication, with its direct actions and adverse effects, has great potential for misuse, and the past 10 years have seen a surge in nonprescription stimulant use among adolescents and young adults.26 The reason most commonly given for using a stimulant is to enhance academic performance through improved alertness and sharpened focus.
Adderall is the psychostimulant most in demand as a “study drug.” Among college students, evidence suggests the individual most likely to misuse Adderall is white, male, affiliated with a formal fraternity, and more likely to use other illicit substances.26 Adding to the perpetuation of this phenomenon is that it is relatively stigma-free: Public opinion does not consistently condemn the use of Adderall for academic means, effectively legitimizing nonprescription use.
Very few universities have an academic policy associating nonprescription use of psychostimulants with cheating. The result is an unprecedented demand for psychostimulant medications,37 which are increasingly obtained through diversion by profiteering peers or from clinicians under false pretenses.26
To help curb the problem of misuse, consider stigmatizing such behavior and stress that, in addition to significant health risks associated with inappropriate use, the vast majority of evidence shows no cognitive enhancement with stimulants when compared with placebo in healthy individuals. Given that psychostimulant misuse is more common with an immediate-release formulation, one means of prevention is to restrict legitimate prescriptions to long-acting formulation as much as possible.38-40
Your role as the primary care provider
An optimal treatment plan for the ADHD athlete, especially one using a psychostimulant medication, should always be individualized. Many factors come into play: the nature of impairing symptoms, presence of comorbidities, and prior response to medication.
How the psychostimulant is taken also can vary depending on an athlete’s preference and the nature of the sport. For example, some athletes will take the medication only for academic purposes (studying, testing). Other athletes feel their sport performance improves while on psychostimulants (eg, a baseball catcher who requires game-long concentration), while yet others prefer not to take it during an event so they can remain unfocused, move randomly, and maintain spontaneity (as with a basketball point guard).
If psychostimulants are to be used while playing, it is wise not to initiate therapy during a high-stress event, such as a championship game. In addition, it is important to know when to withhold medication, as in the case of an endurance athlete competing in hot weather.
Coordinating all aspects of care
In providing the best care for the ADHD athlete, the primary care physician must possess comprehensive knowledge of evidence-based best practices. Educate yourself about all available therapies, including behavioral management and use of psychostimulants. And become familiar with available resources and with the referral network (eg, neuropsychologist).
Acknowledgement of NCAA regulations/restrictions is vital to making treatment decisions. In light of the many regulations (both governmental and within the competitive sporting world), consider the use of nonbanned medications and behavioral therapies whenever possible. Throughout the treatment process, involve all stakeholders—parents, athletic trainers, coaches, teachers—to sustain a collaborative approach to care.
Be attentive to signs of inappropriate use of psychostimulant medication (See “Anticipating and addressing the misuse of psychostimulants” above6,37-40). However, fear of potential misuse is not justification for withholding medication, especially when a clear indication is evident. Failure to recognize ADHD as a legitimate problem puts both academic and social hurdles in the path of the student athlete. Evidence shows that adequately treating ADHD with indicated pharmacotherapy actually reduces subsequent substance abuse.41 Finally, education of every ADHD athlete on existing restrictions/regulations/requirements as posed by governing bodies (NCAA, US Anti-Doping Agency, WADA, and IOC) is imperative.
CORRESPONDENCE
Adam E. Perrin, MD, Family Medicine Center at Asylum Hill, University of Connecticut School of Medicine, 99 Woodland Street, Hartford, CT 06105-1207; aperrin@stfranciscare.org
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association Press; 2013.
2. Parr JW. Attention-deficit hyperactivity disorder and the athlete: new advances and understanding. Clin Sports Med. 2011;30:591-610.
3. Kiluk BD, Weden S, Culotta VP. Sport participation and anxiety in children with ADHD. J Atten Disord. 2009;12:499-506.
4. Broshek DK, Freeman JR. Psychiatric and neuropsychological issues in sports medicine. Clin Sports Med. 2005;24:663-679,x.
5. Polanczyk G, de Lima MS, Horta BL, et al. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry. 2006;164:942-948.
6. Merikangas KR, He JP, Burstein M, et al. Lifetime prevalence of mental disorders in US adolescents: results from the National Comorbidity Stud—Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. 2010;49:980-989.
7. Kessler RC, Adler L, Barkley R, et al. The prevalence and correlates of adult ADHD in the United States: results from the National Comorbidity Survey Replication. Am J Psychiatry. 2006;163:716-723.
8. Solomon GS, Haase RF. Biopsychosocial characteristics and neurocognitive test performance in National Football League players: an initial assessment. Arch Clinical Neuropsychol. 2008;23:563-577.
9. Kutcher JS. Treatment of attention-deficit hyperactivity disorder in athletes. Curr Sports Med Reports. 2011;10:32-36.
10 Biederman J, Kwon A, Aleardi M, et al. Absence of gender effects on attention deficit hyperactivity disorder: findings in nonreferred subjects. Am J Psychiatry. 2005;162:1083-1089.
11. Wilens TE, Faraone SV, Biederman J. Attention-deficit/hyperactivity disorder in adults. JAMA. 2004;292:619-623.
12. Subcommittee on Attention-Deficit/Hyperactivity Disorder; Steering Committee on Quality Improvement and Management; Wolraich M, Brown L, Brown RT, et al. ADHD: clinical practice guideline for diagnosis, evaluation, and treatment of attentiondeficit/hyperactivity disorder in children and adolescents. Pediatrics. 2011;128:1007-1022.
13. Boonstra AM, Osterlaan J, Sergeant JA, et al. Executive functioning in adult ADHD: a meta-analytic review. Psychol Med. 2005;35:1097-1108.
14. Silk T, Vance A, Rinehart N, et al. Fronto-parietal activation in attention-deficit/hyperactivity disorder, combined type: functional magnetic resonance imaging study. Br J Psychiatry. 2005;187:282-283.
15. Biederman J, Wilens TE, Mick E, et al. Does attention-deficit hyperactivity disorder impact the developmental course of drug and alcohol abuse and dependence? Biol Psychiatry. 1998;44:269-273.
16. Putukian M, Kreher JB, Coppel DB, et al. Attention deficit hyperactivity disorder and the athlete: an American Medical Society for Sports Medicine position statement. Clin J Sport Med. 2011;21:392-401.
17. Agarwal R, Goldenberg M, Perry R, et al. The quality of life of adults with attention deficit disorder: a systematic review. Innov Clin Neurosci. 2012;9:10-21.
18. Seixas M, Weiss M, Müller U. Systematic review of national and international guidelines on attention-deficit hyperactivity disorder. J Psychopharmacol. 2012;26:753-765.
19. Pelham WE Jr, Fabiano GA. Evidence-based psychosocial treatments for attention-deficit/hyperactivity disorder. J Clin Child Adolesc Psychol. 2008;37:184-214.
20. Searight HR, Burke JM, Rottneck F. Adult ADHD: evaluation and treatment in family medicine. Am Fam Physician. 2000;62:2077-2086,2091-2092.
21. Krull KR. Attention-deficit hyperactivity disorder in children and adolescents: Treatment with medications. Available at: http://www.uptodate.com/contents/attention-deficit-hyperactivitydisorder-in-children-and-adolescents-treatment-with-medications. Accessed March 17, 2014.
22. Conant-Norville DO, Tofler IR. Attention deficit/hyperactivity disorder and psychopharmacologic treatments in the athlete. Clin Sports Med. 2005;24:829-843,viii.
23. Vaidya CJ, Austin G, Kirkorian G, et al. Selective effects of methylphenidate in attention deficit hyperactivity disorder: a functional magnetic resonance study. Proc Natl Acad Sci USA. 1998;95:14494-14499.
24. Barbaresi WJ, Katusic SK, Colligan RC, et al. Long-term stimulant medication treatment of attention-deficit/hyperactivity disorder: results from a population-based study. J Dev Behav Pediatr. 2006;27:1-10.
25. Hanwella R, Senanayake M, de Silva V. Comparative efficacy and acceptability of methylphenidate and atomoxetine in treatment of attention deficit hyperactivity disorder in children and adolescents: a meta-analysis. BMC Psychiatry. 2011;11:176.
26. Lakhan SE, Kirchgessner A. Prescription stimulants in individuals with and without attention deficit hyperactivity disorder: misuse, cognitive impact, and adverse effects. Brain Behav. 2012:2:661-677.
27. Biederman J, Spencer TJ, Monuteaux MC, et al. A naturalistic 10-year prospective study of height and weight in children with attention-deficit hyperactivity disorder grown up: sex and treatment effects. J Pediatr. 2010;157:635-640.
28. Goldman RD. ADHD stimulants and their effect on height in children. Can Fam Physician. 2010;56:145-146.
29. Conant-Norville DO, Tofler IR. Attention deficit/hyperactivity disorder and psychopharmacologic treatments in the athlete. Clin Sports Med. 2005;24:829-843,viii.
30. National Collegiate Athletic Association Web site. 2012-13 NCAA Sports Medicine Handbook. Available at: http://www.ncaa.org/sites/default/files/MD12.pdf. Accessed March 17, 2014.
31. Battista J. Adderall, a drug of focus, is often blamed as NFL suspensions rise. New York Times. December 2, 2012. Available at: http://www.nytimes.com/2012/12/02/sports/football/adderall-a-drug-of-increased-focus-for-nfl-players.html?pagewanted=all&_r=0. Accessed March 17, 2014.
32. CBS Sports Web site. NCAA medical exception documentation reporting form to support the diagnosis of attention deficit hyperactivity disorder (ADHD) and treatment with banned stimulant medication. Available at: http://grfx.cstv.com/photos/schools/grva/genrel/auto_pdf/2012-13/misc_non_event/adhdreporting.pdf. Accessed March 17, 2014.
33. World Anti-Doping Agency Web site. The 2013 list of prohibited substances and methods. Available at: http://www.wada-ama.org/en/Science-Medicine/Prohibited-List/. Accessed March 17, 2014.
34. Perrin JM, Friedman RA, Knilans TK; Black Box Working Group; Section on Cardiology and Cardiac Surgery. Cardiovascular monitoring and stimulant drugs for attention-deficit/hyperactivity disorder. Pediatrics. 2008;122:451-453.
35. Watson P, Hasegawa H, Roelands B, et al. Acute dopamine/noradrenaline reuptake inhibition enhances human exercise performance in warm, but not temperate conditions. J Physiol. 2005;565(pt 3):873-883.
36. Roelands B, Hasegawa H, Watson P, et al. The effects of acute dopamine reuptake inhibition on performance. Med Sci Sports Exerc. 2008;40:879-885.
37. Sinclair L. ADHD drugs on critical list as medication shortages soar. Psychiatric News. Available at: http://psychnews.psychiatryonline.org/newsarticle.aspx?articleid=481189. Accessed March 17, 2014.
38. Forlini C, Gauthier S, Racine E. Should physicians prescribe cognitive enhancers to healthy individuals? CMAJ. 2013;185:1047-1050.
39. McDuff DR, Baron D. Substance abuse in athletes: a sports psychiatry perspective. Clin Sports Med. 2005;24:885-897,ix-x.
40. Desantis AD, Hane AC. “Adderall is definitely not a drug”: justifications for the illegal use of ADHD stimulants. Subst Use Misuse. 2010;45:31-46.
41. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111:179-185.
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association Press; 2013.
2. Parr JW. Attention-deficit hyperactivity disorder and the athlete: new advances and understanding. Clin Sports Med. 2011;30:591-610.
3. Kiluk BD, Weden S, Culotta VP. Sport participation and anxiety in children with ADHD. J Atten Disord. 2009;12:499-506.
4. Broshek DK, Freeman JR. Psychiatric and neuropsychological issues in sports medicine. Clin Sports Med. 2005;24:663-679,x.
5. Polanczyk G, de Lima MS, Horta BL, et al. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry. 2006;164:942-948.
6. Merikangas KR, He JP, Burstein M, et al. Lifetime prevalence of mental disorders in US adolescents: results from the National Comorbidity Stud—Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. 2010;49:980-989.
7. Kessler RC, Adler L, Barkley R, et al. The prevalence and correlates of adult ADHD in the United States: results from the National Comorbidity Survey Replication. Am J Psychiatry. 2006;163:716-723.
8. Solomon GS, Haase RF. Biopsychosocial characteristics and neurocognitive test performance in National Football League players: an initial assessment. Arch Clinical Neuropsychol. 2008;23:563-577.
9. Kutcher JS. Treatment of attention-deficit hyperactivity disorder in athletes. Curr Sports Med Reports. 2011;10:32-36.
10 Biederman J, Kwon A, Aleardi M, et al. Absence of gender effects on attention deficit hyperactivity disorder: findings in nonreferred subjects. Am J Psychiatry. 2005;162:1083-1089.
11. Wilens TE, Faraone SV, Biederman J. Attention-deficit/hyperactivity disorder in adults. JAMA. 2004;292:619-623.
12. Subcommittee on Attention-Deficit/Hyperactivity Disorder; Steering Committee on Quality Improvement and Management; Wolraich M, Brown L, Brown RT, et al. ADHD: clinical practice guideline for diagnosis, evaluation, and treatment of attentiondeficit/hyperactivity disorder in children and adolescents. Pediatrics. 2011;128:1007-1022.
13. Boonstra AM, Osterlaan J, Sergeant JA, et al. Executive functioning in adult ADHD: a meta-analytic review. Psychol Med. 2005;35:1097-1108.
14. Silk T, Vance A, Rinehart N, et al. Fronto-parietal activation in attention-deficit/hyperactivity disorder, combined type: functional magnetic resonance imaging study. Br J Psychiatry. 2005;187:282-283.
15. Biederman J, Wilens TE, Mick E, et al. Does attention-deficit hyperactivity disorder impact the developmental course of drug and alcohol abuse and dependence? Biol Psychiatry. 1998;44:269-273.
16. Putukian M, Kreher JB, Coppel DB, et al. Attention deficit hyperactivity disorder and the athlete: an American Medical Society for Sports Medicine position statement. Clin J Sport Med. 2011;21:392-401.
17. Agarwal R, Goldenberg M, Perry R, et al. The quality of life of adults with attention deficit disorder: a systematic review. Innov Clin Neurosci. 2012;9:10-21.
18. Seixas M, Weiss M, Müller U. Systematic review of national and international guidelines on attention-deficit hyperactivity disorder. J Psychopharmacol. 2012;26:753-765.
19. Pelham WE Jr, Fabiano GA. Evidence-based psychosocial treatments for attention-deficit/hyperactivity disorder. J Clin Child Adolesc Psychol. 2008;37:184-214.
20. Searight HR, Burke JM, Rottneck F. Adult ADHD: evaluation and treatment in family medicine. Am Fam Physician. 2000;62:2077-2086,2091-2092.
21. Krull KR. Attention-deficit hyperactivity disorder in children and adolescents: Treatment with medications. Available at: http://www.uptodate.com/contents/attention-deficit-hyperactivitydisorder-in-children-and-adolescents-treatment-with-medications. Accessed March 17, 2014.
22. Conant-Norville DO, Tofler IR. Attention deficit/hyperactivity disorder and psychopharmacologic treatments in the athlete. Clin Sports Med. 2005;24:829-843,viii.
23. Vaidya CJ, Austin G, Kirkorian G, et al. Selective effects of methylphenidate in attention deficit hyperactivity disorder: a functional magnetic resonance study. Proc Natl Acad Sci USA. 1998;95:14494-14499.
24. Barbaresi WJ, Katusic SK, Colligan RC, et al. Long-term stimulant medication treatment of attention-deficit/hyperactivity disorder: results from a population-based study. J Dev Behav Pediatr. 2006;27:1-10.
25. Hanwella R, Senanayake M, de Silva V. Comparative efficacy and acceptability of methylphenidate and atomoxetine in treatment of attention deficit hyperactivity disorder in children and adolescents: a meta-analysis. BMC Psychiatry. 2011;11:176.
26. Lakhan SE, Kirchgessner A. Prescription stimulants in individuals with and without attention deficit hyperactivity disorder: misuse, cognitive impact, and adverse effects. Brain Behav. 2012:2:661-677.
27. Biederman J, Spencer TJ, Monuteaux MC, et al. A naturalistic 10-year prospective study of height and weight in children with attention-deficit hyperactivity disorder grown up: sex and treatment effects. J Pediatr. 2010;157:635-640.
28. Goldman RD. ADHD stimulants and their effect on height in children. Can Fam Physician. 2010;56:145-146.
29. Conant-Norville DO, Tofler IR. Attention deficit/hyperactivity disorder and psychopharmacologic treatments in the athlete. Clin Sports Med. 2005;24:829-843,viii.
30. National Collegiate Athletic Association Web site. 2012-13 NCAA Sports Medicine Handbook. Available at: http://www.ncaa.org/sites/default/files/MD12.pdf. Accessed March 17, 2014.
31. Battista J. Adderall, a drug of focus, is often blamed as NFL suspensions rise. New York Times. December 2, 2012. Available at: http://www.nytimes.com/2012/12/02/sports/football/adderall-a-drug-of-increased-focus-for-nfl-players.html?pagewanted=all&_r=0. Accessed March 17, 2014.
32. CBS Sports Web site. NCAA medical exception documentation reporting form to support the diagnosis of attention deficit hyperactivity disorder (ADHD) and treatment with banned stimulant medication. Available at: http://grfx.cstv.com/photos/schools/grva/genrel/auto_pdf/2012-13/misc_non_event/adhdreporting.pdf. Accessed March 17, 2014.
33. World Anti-Doping Agency Web site. The 2013 list of prohibited substances and methods. Available at: http://www.wada-ama.org/en/Science-Medicine/Prohibited-List/. Accessed March 17, 2014.
34. Perrin JM, Friedman RA, Knilans TK; Black Box Working Group; Section on Cardiology and Cardiac Surgery. Cardiovascular monitoring and stimulant drugs for attention-deficit/hyperactivity disorder. Pediatrics. 2008;122:451-453.
35. Watson P, Hasegawa H, Roelands B, et al. Acute dopamine/noradrenaline reuptake inhibition enhances human exercise performance in warm, but not temperate conditions. J Physiol. 2005;565(pt 3):873-883.
36. Roelands B, Hasegawa H, Watson P, et al. The effects of acute dopamine reuptake inhibition on performance. Med Sci Sports Exerc. 2008;40:879-885.
37. Sinclair L. ADHD drugs on critical list as medication shortages soar. Psychiatric News. Available at: http://psychnews.psychiatryonline.org/newsarticle.aspx?articleid=481189. Accessed March 17, 2014.
38. Forlini C, Gauthier S, Racine E. Should physicians prescribe cognitive enhancers to healthy individuals? CMAJ. 2013;185:1047-1050.
39. McDuff DR, Baron D. Substance abuse in athletes: a sports psychiatry perspective. Clin Sports Med. 2005;24:885-897,ix-x.
40. Desantis AD, Hane AC. “Adderall is definitely not a drug”: justifications for the illegal use of ADHD stimulants. Subst Use Misuse. 2010;45:31-46.
41. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111:179-185.
