User login
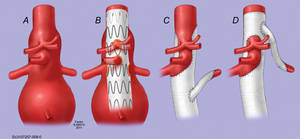
CHICAGO – Fenestrated grafts increasingly are being used for endovascular aneurysm repair of complex abdominal aortic aneurysms, but there are few benchmarks for comparing outcomes achieved with open repair and EVAR in these situations.
Dr. Gustavo S. Oderich and his colleagues at the Mayo Clinic, Rochester, Minn., found that open complex abdominal aortic aneurysm (cAAA) repair can be done safely, but there is an increasing risk of complications and mortality with more complex anatomies.
They reviewed the outcomes of a series of 461 patients undergoing open cAAA repair from 2000 to 2010, Dr. Oderich said at the Vascular Annual Meeting.
In their study, available preoperative digital imaging data were analyzed by a blinded investigator.
A centerline of flow was used to define aneurysm extent and to predict the expected number of fenestrations that would have been required to provide 2 cm of proximal seal for a fenestrated EVAR procedure, had one been performed. End points examined were mortality, morbidity, renal function (RF) deterioration, reinterventions, and survival.
Among the 354 male and 107 female patients (mean age, 73 years), the overall operative mortality was 1.3% (6/461). Some level of morbidity occurred in 57% (260) of the patients treated, and it was severe in 20% (91) of the overall patients.
The overall 5-year patient survival rate was 72%, with a freedom from reintervention rate of 90% and a freedom from RF deterioration rate of 84%.
Dr. Oderich discussed how the increasing level of aneurysm complexity was significantly associated with greater operative mortality, severe morbidity, and dialysis rates – regardless of whether the complexity was classified by anatomic considerations (from juxtarenal to suprarenal to type IV thoracic aortic aneurysm, TAA) or by the expected number of fenestrations (one through four), with more fenestrations equivalent to increasing complexity.
At 5 years, patient survival ranged from 76% in juxtarenal patients to 62% for type IV TAA, with severe morbidity ranging from 13% (juxtarenal) to 43% (type IV TAA).
Similarly, severe morbidity in patients with only one expected fenestration was 0%, but reached 42% in patients who would have an expected number of four fenestrations.
"Open cAAA repair can be performed safely with low overall mortality (1.3%), but the risk of complications and mortality increases with worse anatomic classification and a higher expected number of fenestrations. These data can provide a needed benchmark for comparison with results of fenestrated EVAR," said Dr. Oderich.

Dr. Oderich stated that he received consulting fees and other remuneration from Medtronic and Cook Medical.
CHICAGO – Fenestrated grafts increasingly are being used for endovascular aneurysm repair of complex abdominal aortic aneurysms, but there are few benchmarks for comparing outcomes achieved with open repair and EVAR in these situations.
Dr. Gustavo S. Oderich and his colleagues at the Mayo Clinic, Rochester, Minn., found that open complex abdominal aortic aneurysm (cAAA) repair can be done safely, but there is an increasing risk of complications and mortality with more complex anatomies.
They reviewed the outcomes of a series of 461 patients undergoing open cAAA repair from 2000 to 2010, Dr. Oderich said at the Vascular Annual Meeting.
In their study, available preoperative digital imaging data were analyzed by a blinded investigator.
A centerline of flow was used to define aneurysm extent and to predict the expected number of fenestrations that would have been required to provide 2 cm of proximal seal for a fenestrated EVAR procedure, had one been performed. End points examined were mortality, morbidity, renal function (RF) deterioration, reinterventions, and survival.
Among the 354 male and 107 female patients (mean age, 73 years), the overall operative mortality was 1.3% (6/461). Some level of morbidity occurred in 57% (260) of the patients treated, and it was severe in 20% (91) of the overall patients.
The overall 5-year patient survival rate was 72%, with a freedom from reintervention rate of 90% and a freedom from RF deterioration rate of 84%.
Dr. Oderich discussed how the increasing level of aneurysm complexity was significantly associated with greater operative mortality, severe morbidity, and dialysis rates – regardless of whether the complexity was classified by anatomic considerations (from juxtarenal to suprarenal to type IV thoracic aortic aneurysm, TAA) or by the expected number of fenestrations (one through four), with more fenestrations equivalent to increasing complexity.
At 5 years, patient survival ranged from 76% in juxtarenal patients to 62% for type IV TAA, with severe morbidity ranging from 13% (juxtarenal) to 43% (type IV TAA).
Similarly, severe morbidity in patients with only one expected fenestration was 0%, but reached 42% in patients who would have an expected number of four fenestrations.
"Open cAAA repair can be performed safely with low overall mortality (1.3%), but the risk of complications and mortality increases with worse anatomic classification and a higher expected number of fenestrations. These data can provide a needed benchmark for comparison with results of fenestrated EVAR," said Dr. Oderich.
Dr. Oderich stated that he received consulting fees and other remuneration from Medtronic and Cook Medical.
CHICAGO – Fenestrated grafts increasingly are being used for endovascular aneurysm repair of complex abdominal aortic aneurysms, but there are few benchmarks for comparing outcomes achieved with open repair and EVAR in these situations.
Dr. Gustavo S. Oderich and his colleagues at the Mayo Clinic, Rochester, Minn., found that open complex abdominal aortic aneurysm (cAAA) repair can be done safely, but there is an increasing risk of complications and mortality with more complex anatomies.
They reviewed the outcomes of a series of 461 patients undergoing open cAAA repair from 2000 to 2010, Dr. Oderich said at the Vascular Annual Meeting.
In their study, available preoperative digital imaging data were analyzed by a blinded investigator.
A centerline of flow was used to define aneurysm extent and to predict the expected number of fenestrations that would have been required to provide 2 cm of proximal seal for a fenestrated EVAR procedure, had one been performed. End points examined were mortality, morbidity, renal function (RF) deterioration, reinterventions, and survival.
Among the 354 male and 107 female patients (mean age, 73 years), the overall operative mortality was 1.3% (6/461). Some level of morbidity occurred in 57% (260) of the patients treated, and it was severe in 20% (91) of the overall patients.
The overall 5-year patient survival rate was 72%, with a freedom from reintervention rate of 90% and a freedom from RF deterioration rate of 84%.
Dr. Oderich discussed how the increasing level of aneurysm complexity was significantly associated with greater operative mortality, severe morbidity, and dialysis rates – regardless of whether the complexity was classified by anatomic considerations (from juxtarenal to suprarenal to type IV thoracic aortic aneurysm, TAA) or by the expected number of fenestrations (one through four), with more fenestrations equivalent to increasing complexity.
At 5 years, patient survival ranged from 76% in juxtarenal patients to 62% for type IV TAA, with severe morbidity ranging from 13% (juxtarenal) to 43% (type IV TAA).
Similarly, severe morbidity in patients with only one expected fenestration was 0%, but reached 42% in patients who would have an expected number of four fenestrations.
"Open cAAA repair can be performed safely with low overall mortality (1.3%), but the risk of complications and mortality increases with worse anatomic classification and a higher expected number of fenestrations. These data can provide a needed benchmark for comparison with results of fenestrated EVAR," said Dr. Oderich.
Dr. Oderich stated that he received consulting fees and other remuneration from Medtronic and Cook Medical.