User login

I am on a plane on my way back to Minnesota after being professionally rejuvenated by the content of the Institute of Healthcare Improvement’s 16th Annual Forum, in Orlando, FL. The theme of the meeting called on all hospitals, and hence I believe all hospitalists, to save lives. Dr. Donald Berwick, President and CEO of the Institute of Healthcare Improvement (IHI) kicked off this years’ Annual Forum with his plenary speech “Some is not a number, Soon is not a time.” Saving some lives, some time in the future is not a clear goal. “Some is not a number and soon is not a time.” So, he put the challenge forth for hospitals to join IHI in a campaign to save 100K lives by June 14, 2006 at 9:00 a.m. EDT.
“Some is not a number. Soon is not a time.” We all get “why” this is important, at least in so much as what we have been told by the Institute of Medicine Reports “To Err is Human” and “Crossing the Quality Chasm”. But “how” can this be done? By doing things that we already know impact mortality in a hospital setting. By engaging in the reliable care delivery of six changes that save lives. These include recommendations in each of the following areas: rapid response or emergency medical teams, reliable care for acute myocardial infarctions, reliable use of the ventilator pneumonia and central venous line “bundles”, surgical site infection prophylaxis, and prevention of adverse drug events with reconciliation. Each is described in more detail below.
- Rapid Response Teams (also known as Medical Emergency or Pre-Code Teams): This is a team of healthcare providers that may be summoned at any time by anyone in the hospital to assist in the care of a patient who appears acutely ill, before the patient has respiratory failure, a cardiac arrest or other adverse event. The aim is to prevent situations of “failure to rescue”, to recognize the early signs and symptoms of clinical deterioration prior to requiring transfer to the intensive care unit.
- Reliable Care for Acute Myocardial Infarction (AMI): For appropriate AMI patients, reliable use of all of the following treatments: early administration of aspirin, aspirin at discharge, early administration of a beta-blocker, beta-blocker at discharge, ACE‑inhibitor or angiotensin receptor blocker (ARB) at discharge (if systolic dysfunction), timely reperfusion, and smoking cessation counseling.
- Reliable use of the Ventilator Bundle: A number of hospitals have initiated the use of the ventilator bundle to prevent ventilator associated pneumonia (VAP). VAP carries a high mortality rate. The “bundle” is a grouping of 5 treatments/preventions measured as a composite (% of patients that get all 5).
- Elevate head of bed to 30 degrees
- Peptic ulcer prophylaxis
- Deep venous thrombosis prophylaxis
- Daily “sedation vacation”
- Daily assessment of readiness to extubate
Not all of the items have a specific relationship to VAP (e.g., DVT prophylaxis), but when reliably performed in concert with the other items, leads to a decrease in VAP.
- Reliable use of Central Venous Line Bundles: This is a grouping of 5 preventative measures that when done in concert and measured as a composite have had maximal effectiveness for the reduction of central line associated blood stream infections (CLABs) in some hospitals.
- Hand hygiene
- Maximal barrier precautions
- Chlorhexidine skin antisepsis
- Appropriate catheter site and administration system care
- No routine line replacement
- Surgical site infection (SSI) prophylaxis with a “SSI bundle”: Hospitals participating with the IHI in a variety of different formats have found the most substantial reduction/prevention of SSIs when 3 preventative measures are done in concert with each other for every surgical patient. These preventative measures include:
- Guideline-based use of prophylactic perioperative antibiotics (including both choice and timing of administration of antibiotic)
- Appropriate hair removal (avoiding shaving)
- Perioperative glucose control
- Prevention of adverse drug events with medication reconciliation: This refers to the procedures that can be put in place at the time of any transition of care to mitigate the increased risk of wrong dose of medication or even wrong drug being administered immediately following that transition. Each time we have to transfer information from one sheet of paper to another or from a sheet of paper to a computer, there is chance for human error. Medication reconciliation can virtually eliminate errors occurring at transitions in care.
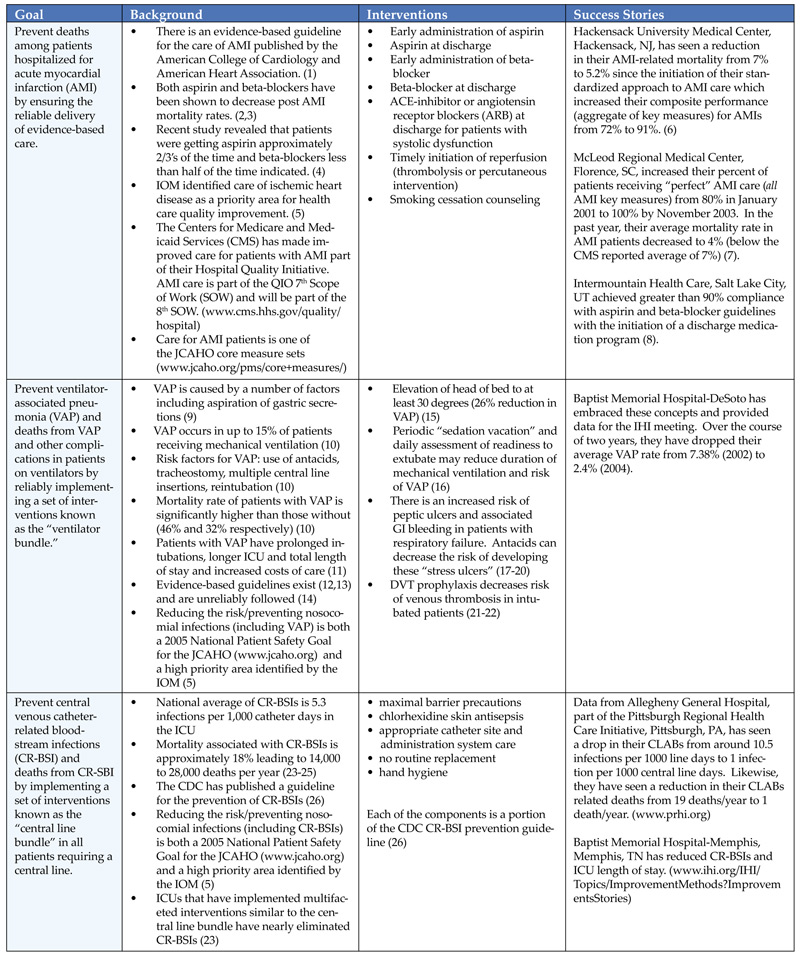
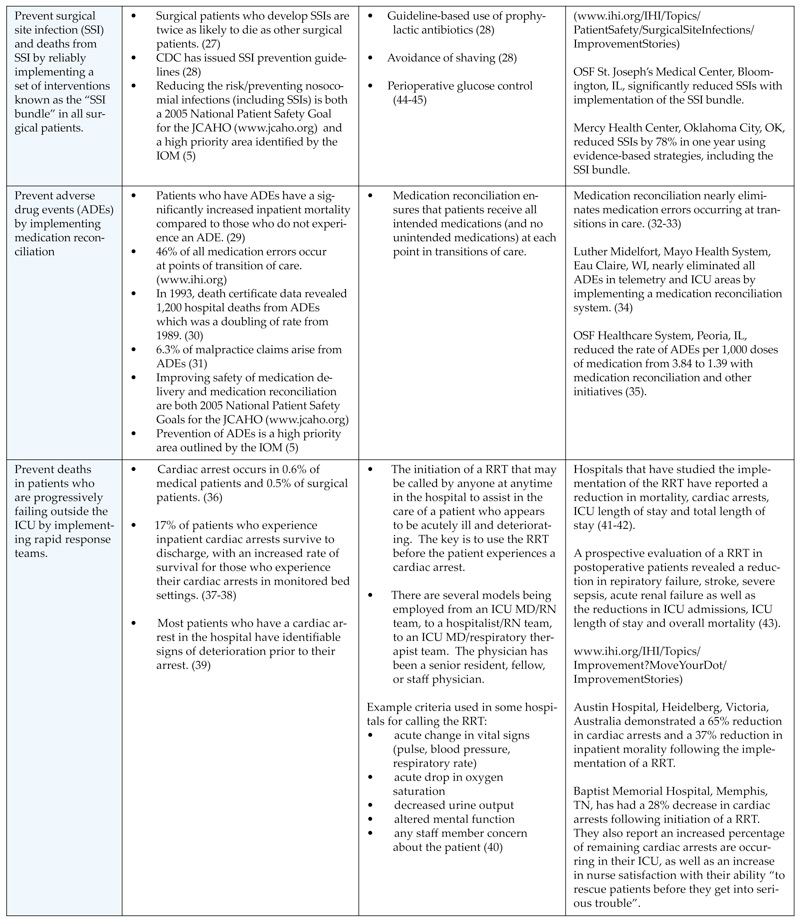
I have placed in Table 1, the information (goals, background, proposed interventions and success stories) handed out during Dr. Donald Berwick’s opening plenary session, the kick-off for the campaign to save 100,000 lives.
Two key components of the descriptions above deserve further explanation. One of the key components is the concept of reliability. Reliability is how often something in health care does what it is supposed to do, in the time frame it is supposed to do it in. The formula is the number of times that something (delivery of a medication or service) is done correctly divided by the number of times that same something is attempted. In work published by Karl Weick, one common principle within high reliability organizations is that of a preoccupation with failure. As such, the notation of reliability is a measure of defects. Currently much of healthcare (including use of beta-blockers after AMI) functions at a 10-1 level of performance (one defect in 10 tries) or less than a 90% success rate. Organizations that have actively embraced this concept of reliability in their quality improvement work have rejected the usual satisfaction with 10-1 performance. Shouldn’t 99 out of 100 (or 999 out of a 1,000) patients with an AMI get what they are supposed to get?
The other key component embedded within some of the six items that save lives is the concept of bundles. Rather than considering individual measures for each of the items within a bundle, a composite or aggregate measure is reported. Bottom line is that doing any one or two of the items in a bundle is not good enough. It will not achieve the same reduction in hospital acquired infection rates or mortality, as doing all of the items in concert for every appropriate patient.
How can hospitalists help achieve this national goal, to participate in this campaign with the IHI? As individuals, we can be a hospital “precinct captain” or champion, speak to our hospital boards, convene colleagues to standardize to science, start medication reconciliation, and seek composite reliability in our own individual practices.
The IHI will measure this campaign in four ways.
Level 1. Number of hospitals “signing up”
Level 2. Changes in process of care reported
Level 3. Actual changes in deaths and death rates (sample amongst volunteer hospitals)
Level 4. Hospital Standardized Mortality Rates (work of Brian Jarman)
More detailed and specific information about the campaign (and how to participate) can be found on IHI’s Web site (www.ihi.org/ihi/programs/campaign).
“Some is not a number. Soon is not a time.”
The number: 100,000 lives.
The time: June 14, 2006 – 9 a.m. EDT.
References
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction – executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). J Am Coll Cardiol. 2004;44:671-719.
- Antman EM, Lau J, Kupelnick B, Mosteller F, Chalmers TC. A comparison of results of meta-analyses of randomized controlled trials and recommendations of clinical experts: treatments for myocardial infarction. JAMA. 1992;268:240-8.
- Hennekens CH, Albert CM, Godfried SL, Gaziano JM, Buring JE. Adjunctive drug therapy of acute myocardial infarction – evidence from clinical trials. N Engl J Med. 1996;335:1660-7.
- McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348:2635-45.
- Adams K, Corrigan JM, eds. Priority areas for national action: transforming health care quality. Washington, DC: The National Academics Press, 2003.
- Lappe JM, Muhlstein JB, Lappe DL, et al. Improvements in 1-year cardiovascular clinical outcomes associated with a hospital-based discharge medication program. Ann Intern Med. 2004;141:446-53.
- Hackensack University Medical Center AMI Report, Sept 10, 2004.
- McLeod Regional Medical Center Storyboard for the 2004 IHI National Forum.
- Craven DE, Steger KA. Nosocomial pneumonia in mechanically ventilated adult patients: epidemiology and prevention in 1996. Semin Respir Infect. 1996;11:32-53.
- Ibrahim EH, Tracy L, Hill C, Fraser VJ, Kollef MH. The occurrence of ventilator-associated pneumonia in a community hospital: risk factors and clinical outcomes. Chest. 2001;120:555-61.
- Rello J, Ollendorf DA, Oster G, et al. Epidemiology and outcomes of ventilator associated pneumonia in a large U.S. database. Chest. 2002;122:2115-21.
- Guidelines for Preventing Health-Care-Associated Pneumonia, 2003. Recommendations of CDC and the Healthcare Infection Control Practices Advisory Commi Tee. MMWR. 2004;53(No.RR‑3):1-36.
- Dodek P, Keenan S, Cook D, et al. Evidence-based clinical practice guideline for the prevention of ventilator-associated pneumonia. Ann Intern Med. 2004;141:305-13.
- Rello J, Lorente C, Bodi M, Diaz E, Ricart M, Kollef MH. Why do physicians not follow evidence-based guidelines for preventing ventilator-associated pneumonia? A survey based on the opinions of an international panel of intensivists. Chest. 2002;122:656-61.
- Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomized trial. Lancet. 1999;354:1851-58.
- Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342:1471-77.
- Cook DJ, Fuller HD, Guyatt GH, et al. Risk factors for gastrointestinal bleeding in critically ill patients. N Engl J Med. 1994;330:377-81.
- Cook DJ, Reeve BK, Guyatt GH, et al. Stress ulcer prophylaxis in critically ill patients: resolving discordant meta-analyses. JAMA. 1996;275:308-314.
- Cook D, Guyatt G, Marshall J, et al. A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. N Engl J Med. 1998;338:791-97.
- Cook D, Heyland, Griffith L, Cook R, Marshall J, Pagliarello J. Risk factors for clinically important upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. Crit Care Med. 1999;27:2812-17.
- Attia J, Ray JG, Cook DJ, Douketis J, Ginsberg JS, Geerts WH. Deep vein thrombosis and its prevention in critically ill adults. Arch Intern Med. 2001;161:1268-79.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism. The seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest. 2004;126:338S-400S.
- Berenholtz SM, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Crit Care Med. 2004;32:2014-20.
- Pittet D, Tarara D, Wenzel RP. Nosocomial bloodstream infection in critically ill patients. Excess length of stay, extra costs, and aTributable mortality. JAMA. 1994;271:1598-1601.
- Saint S. Chapter 16. Prevention of intravascular catheter-related infection. Making health care safer: a critical analysis of patient safety practices. AHRQ evidence report, number 43, July 20, 2001. www.ncbi.nlm.nih.gov/vooks.
- O’Grady NP; Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections. MMWR Morb Mort Wkly Rep. 2002;51(RR-10):1-29.
- Kirkland KB, et al. The impact of surgical-site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infect Control Hosp Epidemiol. 1999;20:725-30.
- Mangram AJ, Horan TC, Pearson ML, et al. Guidelines for prevention of surgical site infection, 1999. Infect Control Hosp Epidemiol. 1999;20:247-78.
- Classen DC, Pestotnik SL, Evans RS, Lloyd JF, Burke JP. Adverse drug events in hospitalized patients. Excess length of stay, extra costs, and attributable mortality. JAMA. 1997;277:301-06.
- Phillips DP, Christenfeld N, Glynn LM. Increase in U.S. medication-error deaths between 1983 and 1993. Lancet. 1998;351:643-4.
- Rothschild JM, Federic FA, Gandhi TK, Kaushal R, Williams DH, Bates DW. Analysis of medication-related malpractice claims. Causes, preventability, and costs. Arch Intern Med. 2002;162:2414-20.
- Pronovost P, Weast B, Schwarz M, et al. Medication reconciliation: a practical tool to reduce the risk of medication errors. J Crit Care. 2003;18:201-205.
- Rozich JD, Resar RK. Medication safety: one organization’s approach to the challenge. JCOM. 2001;8(10):27-34.
- Rozich JD, Howard RJ, Justeson JM, Macken PD, Lindsay ME, Resar RK. Standardization as a mechanism to improve safety in healthcare. Jt Comm J Qual Saf. 2004;30:5-14.
- Whittington J, Cohen H. OSF Healthcare’s journey in patient safety. Qual Manag Health Care. 2004;13:53-59.
- Needleman J, Buerhaus P, Mattke S, et al. Nursing-staffing levels and the quality of care in hospitals. N Engl J Med. 2002;346:1715-22.
- Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14,270 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58:297-308.
- Sandroni C, Ferro G, Santangelo S, et al. In-hospital cardiac arrest: survival depends mainly on the emergency response. Resuscitation. 2004;62:291-7.
- Schein RM, Hazday N, Pena M, et al. Clinical antecedents to in-hospital cardiopulmonary arrest. Chest. 1990;98:1388-92.
- Hillman K, Parr M, Flabouris A, Bishop G, Stewart A. Redefining in-hospital resuscitation: the concept of the medical emergency team. Resuscitation. 2001;48:105-10.
- Buist MD, Moore GE, Bernard SA, Waxman BP, Anderson JN, Nguyen TV. Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study. BMJ. 2002;324:387-90.
- Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. MJA. 2003;179:283-7.
- Bellomo R, Goldsmith D, Uchino S, et al. Prospective controlled trail of effect of medical emergency team on postoperative morbidity and mortality rates. Crit Car Med. 2004;32:916-21.
- Furnary AP, Zerr KJ, Grunkemeier GL, Starr AL. Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann Thorac Surg. 1999;67: 352-62.
- Van de Berghe G, Wouters P, Weekers F, et all. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359-67.
I am on a plane on my way back to Minnesota after being professionally rejuvenated by the content of the Institute of Healthcare Improvement’s 16th Annual Forum, in Orlando, FL. The theme of the meeting called on all hospitals, and hence I believe all hospitalists, to save lives. Dr. Donald Berwick, President and CEO of the Institute of Healthcare Improvement (IHI) kicked off this years’ Annual Forum with his plenary speech “Some is not a number, Soon is not a time.” Saving some lives, some time in the future is not a clear goal. “Some is not a number and soon is not a time.” So, he put the challenge forth for hospitals to join IHI in a campaign to save 100K lives by June 14, 2006 at 9:00 a.m. EDT.
“Some is not a number. Soon is not a time.” We all get “why” this is important, at least in so much as what we have been told by the Institute of Medicine Reports “To Err is Human” and “Crossing the Quality Chasm”. But “how” can this be done? By doing things that we already know impact mortality in a hospital setting. By engaging in the reliable care delivery of six changes that save lives. These include recommendations in each of the following areas: rapid response or emergency medical teams, reliable care for acute myocardial infarctions, reliable use of the ventilator pneumonia and central venous line “bundles”, surgical site infection prophylaxis, and prevention of adverse drug events with reconciliation. Each is described in more detail below.
- Rapid Response Teams (also known as Medical Emergency or Pre-Code Teams): This is a team of healthcare providers that may be summoned at any time by anyone in the hospital to assist in the care of a patient who appears acutely ill, before the patient has respiratory failure, a cardiac arrest or other adverse event. The aim is to prevent situations of “failure to rescue”, to recognize the early signs and symptoms of clinical deterioration prior to requiring transfer to the intensive care unit.
- Reliable Care for Acute Myocardial Infarction (AMI): For appropriate AMI patients, reliable use of all of the following treatments: early administration of aspirin, aspirin at discharge, early administration of a beta-blocker, beta-blocker at discharge, ACE‑inhibitor or angiotensin receptor blocker (ARB) at discharge (if systolic dysfunction), timely reperfusion, and smoking cessation counseling.
- Reliable use of the Ventilator Bundle: A number of hospitals have initiated the use of the ventilator bundle to prevent ventilator associated pneumonia (VAP). VAP carries a high mortality rate. The “bundle” is a grouping of 5 treatments/preventions measured as a composite (% of patients that get all 5).
- Elevate head of bed to 30 degrees
- Peptic ulcer prophylaxis
- Deep venous thrombosis prophylaxis
- Daily “sedation vacation”
- Daily assessment of readiness to extubate
Not all of the items have a specific relationship to VAP (e.g., DVT prophylaxis), but when reliably performed in concert with the other items, leads to a decrease in VAP.
- Reliable use of Central Venous Line Bundles: This is a grouping of 5 preventative measures that when done in concert and measured as a composite have had maximal effectiveness for the reduction of central line associated blood stream infections (CLABs) in some hospitals.
- Hand hygiene
- Maximal barrier precautions
- Chlorhexidine skin antisepsis
- Appropriate catheter site and administration system care
- No routine line replacement
- Surgical site infection (SSI) prophylaxis with a “SSI bundle”: Hospitals participating with the IHI in a variety of different formats have found the most substantial reduction/prevention of SSIs when 3 preventative measures are done in concert with each other for every surgical patient. These preventative measures include:
- Guideline-based use of prophylactic perioperative antibiotics (including both choice and timing of administration of antibiotic)
- Appropriate hair removal (avoiding shaving)
- Perioperative glucose control
- Prevention of adverse drug events with medication reconciliation: This refers to the procedures that can be put in place at the time of any transition of care to mitigate the increased risk of wrong dose of medication or even wrong drug being administered immediately following that transition. Each time we have to transfer information from one sheet of paper to another or from a sheet of paper to a computer, there is chance for human error. Medication reconciliation can virtually eliminate errors occurring at transitions in care.
I have placed in Table 1, the information (goals, background, proposed interventions and success stories) handed out during Dr. Donald Berwick’s opening plenary session, the kick-off for the campaign to save 100,000 lives.
Two key components of the descriptions above deserve further explanation. One of the key components is the concept of reliability. Reliability is how often something in health care does what it is supposed to do, in the time frame it is supposed to do it in. The formula is the number of times that something (delivery of a medication or service) is done correctly divided by the number of times that same something is attempted. In work published by Karl Weick, one common principle within high reliability organizations is that of a preoccupation with failure. As such, the notation of reliability is a measure of defects. Currently much of healthcare (including use of beta-blockers after AMI) functions at a 10-1 level of performance (one defect in 10 tries) or less than a 90% success rate. Organizations that have actively embraced this concept of reliability in their quality improvement work have rejected the usual satisfaction with 10-1 performance. Shouldn’t 99 out of 100 (or 999 out of a 1,000) patients with an AMI get what they are supposed to get?
The other key component embedded within some of the six items that save lives is the concept of bundles. Rather than considering individual measures for each of the items within a bundle, a composite or aggregate measure is reported. Bottom line is that doing any one or two of the items in a bundle is not good enough. It will not achieve the same reduction in hospital acquired infection rates or mortality, as doing all of the items in concert for every appropriate patient.
How can hospitalists help achieve this national goal, to participate in this campaign with the IHI? As individuals, we can be a hospital “precinct captain” or champion, speak to our hospital boards, convene colleagues to standardize to science, start medication reconciliation, and seek composite reliability in our own individual practices.
The IHI will measure this campaign in four ways.
Level 1. Number of hospitals “signing up”
Level 2. Changes in process of care reported
Level 3. Actual changes in deaths and death rates (sample amongst volunteer hospitals)
Level 4. Hospital Standardized Mortality Rates (work of Brian Jarman)
More detailed and specific information about the campaign (and how to participate) can be found on IHI’s Web site (www.ihi.org/ihi/programs/campaign).
“Some is not a number. Soon is not a time.”
The number: 100,000 lives.
The time: June 14, 2006 – 9 a.m. EDT.
References
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction – executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). J Am Coll Cardiol. 2004;44:671-719.
- Antman EM, Lau J, Kupelnick B, Mosteller F, Chalmers TC. A comparison of results of meta-analyses of randomized controlled trials and recommendations of clinical experts: treatments for myocardial infarction. JAMA. 1992;268:240-8.
- Hennekens CH, Albert CM, Godfried SL, Gaziano JM, Buring JE. Adjunctive drug therapy of acute myocardial infarction – evidence from clinical trials. N Engl J Med. 1996;335:1660-7.
- McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348:2635-45.
- Adams K, Corrigan JM, eds. Priority areas for national action: transforming health care quality. Washington, DC: The National Academics Press, 2003.
- Lappe JM, Muhlstein JB, Lappe DL, et al. Improvements in 1-year cardiovascular clinical outcomes associated with a hospital-based discharge medication program. Ann Intern Med. 2004;141:446-53.
- Hackensack University Medical Center AMI Report, Sept 10, 2004.
- McLeod Regional Medical Center Storyboard for the 2004 IHI National Forum.
- Craven DE, Steger KA. Nosocomial pneumonia in mechanically ventilated adult patients: epidemiology and prevention in 1996. Semin Respir Infect. 1996;11:32-53.
- Ibrahim EH, Tracy L, Hill C, Fraser VJ, Kollef MH. The occurrence of ventilator-associated pneumonia in a community hospital: risk factors and clinical outcomes. Chest. 2001;120:555-61.
- Rello J, Ollendorf DA, Oster G, et al. Epidemiology and outcomes of ventilator associated pneumonia in a large U.S. database. Chest. 2002;122:2115-21.
- Guidelines for Preventing Health-Care-Associated Pneumonia, 2003. Recommendations of CDC and the Healthcare Infection Control Practices Advisory Commi Tee. MMWR. 2004;53(No.RR‑3):1-36.
- Dodek P, Keenan S, Cook D, et al. Evidence-based clinical practice guideline for the prevention of ventilator-associated pneumonia. Ann Intern Med. 2004;141:305-13.
- Rello J, Lorente C, Bodi M, Diaz E, Ricart M, Kollef MH. Why do physicians not follow evidence-based guidelines for preventing ventilator-associated pneumonia? A survey based on the opinions of an international panel of intensivists. Chest. 2002;122:656-61.
- Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomized trial. Lancet. 1999;354:1851-58.
- Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342:1471-77.
- Cook DJ, Fuller HD, Guyatt GH, et al. Risk factors for gastrointestinal bleeding in critically ill patients. N Engl J Med. 1994;330:377-81.
- Cook DJ, Reeve BK, Guyatt GH, et al. Stress ulcer prophylaxis in critically ill patients: resolving discordant meta-analyses. JAMA. 1996;275:308-314.
- Cook D, Guyatt G, Marshall J, et al. A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. N Engl J Med. 1998;338:791-97.
- Cook D, Heyland, Griffith L, Cook R, Marshall J, Pagliarello J. Risk factors for clinically important upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. Crit Care Med. 1999;27:2812-17.
- Attia J, Ray JG, Cook DJ, Douketis J, Ginsberg JS, Geerts WH. Deep vein thrombosis and its prevention in critically ill adults. Arch Intern Med. 2001;161:1268-79.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism. The seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest. 2004;126:338S-400S.
- Berenholtz SM, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Crit Care Med. 2004;32:2014-20.
- Pittet D, Tarara D, Wenzel RP. Nosocomial bloodstream infection in critically ill patients. Excess length of stay, extra costs, and aTributable mortality. JAMA. 1994;271:1598-1601.
- Saint S. Chapter 16. Prevention of intravascular catheter-related infection. Making health care safer: a critical analysis of patient safety practices. AHRQ evidence report, number 43, July 20, 2001. www.ncbi.nlm.nih.gov/vooks.
- O’Grady NP; Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections. MMWR Morb Mort Wkly Rep. 2002;51(RR-10):1-29.
- Kirkland KB, et al. The impact of surgical-site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infect Control Hosp Epidemiol. 1999;20:725-30.
- Mangram AJ, Horan TC, Pearson ML, et al. Guidelines for prevention of surgical site infection, 1999. Infect Control Hosp Epidemiol. 1999;20:247-78.
- Classen DC, Pestotnik SL, Evans RS, Lloyd JF, Burke JP. Adverse drug events in hospitalized patients. Excess length of stay, extra costs, and attributable mortality. JAMA. 1997;277:301-06.
- Phillips DP, Christenfeld N, Glynn LM. Increase in U.S. medication-error deaths between 1983 and 1993. Lancet. 1998;351:643-4.
- Rothschild JM, Federic FA, Gandhi TK, Kaushal R, Williams DH, Bates DW. Analysis of medication-related malpractice claims. Causes, preventability, and costs. Arch Intern Med. 2002;162:2414-20.
- Pronovost P, Weast B, Schwarz M, et al. Medication reconciliation: a practical tool to reduce the risk of medication errors. J Crit Care. 2003;18:201-205.
- Rozich JD, Resar RK. Medication safety: one organization’s approach to the challenge. JCOM. 2001;8(10):27-34.
- Rozich JD, Howard RJ, Justeson JM, Macken PD, Lindsay ME, Resar RK. Standardization as a mechanism to improve safety in healthcare. Jt Comm J Qual Saf. 2004;30:5-14.
- Whittington J, Cohen H. OSF Healthcare’s journey in patient safety. Qual Manag Health Care. 2004;13:53-59.
- Needleman J, Buerhaus P, Mattke S, et al. Nursing-staffing levels and the quality of care in hospitals. N Engl J Med. 2002;346:1715-22.
- Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14,270 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58:297-308.
- Sandroni C, Ferro G, Santangelo S, et al. In-hospital cardiac arrest: survival depends mainly on the emergency response. Resuscitation. 2004;62:291-7.
- Schein RM, Hazday N, Pena M, et al. Clinical antecedents to in-hospital cardiopulmonary arrest. Chest. 1990;98:1388-92.
- Hillman K, Parr M, Flabouris A, Bishop G, Stewart A. Redefining in-hospital resuscitation: the concept of the medical emergency team. Resuscitation. 2001;48:105-10.
- Buist MD, Moore GE, Bernard SA, Waxman BP, Anderson JN, Nguyen TV. Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study. BMJ. 2002;324:387-90.
- Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. MJA. 2003;179:283-7.
- Bellomo R, Goldsmith D, Uchino S, et al. Prospective controlled trail of effect of medical emergency team on postoperative morbidity and mortality rates. Crit Car Med. 2004;32:916-21.
- Furnary AP, Zerr KJ, Grunkemeier GL, Starr AL. Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann Thorac Surg. 1999;67: 352-62.
- Van de Berghe G, Wouters P, Weekers F, et all. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359-67.
I am on a plane on my way back to Minnesota after being professionally rejuvenated by the content of the Institute of Healthcare Improvement’s 16th Annual Forum, in Orlando, FL. The theme of the meeting called on all hospitals, and hence I believe all hospitalists, to save lives. Dr. Donald Berwick, President and CEO of the Institute of Healthcare Improvement (IHI) kicked off this years’ Annual Forum with his plenary speech “Some is not a number, Soon is not a time.” Saving some lives, some time in the future is not a clear goal. “Some is not a number and soon is not a time.” So, he put the challenge forth for hospitals to join IHI in a campaign to save 100K lives by June 14, 2006 at 9:00 a.m. EDT.
“Some is not a number. Soon is not a time.” We all get “why” this is important, at least in so much as what we have been told by the Institute of Medicine Reports “To Err is Human” and “Crossing the Quality Chasm”. But “how” can this be done? By doing things that we already know impact mortality in a hospital setting. By engaging in the reliable care delivery of six changes that save lives. These include recommendations in each of the following areas: rapid response or emergency medical teams, reliable care for acute myocardial infarctions, reliable use of the ventilator pneumonia and central venous line “bundles”, surgical site infection prophylaxis, and prevention of adverse drug events with reconciliation. Each is described in more detail below.
- Rapid Response Teams (also known as Medical Emergency or Pre-Code Teams): This is a team of healthcare providers that may be summoned at any time by anyone in the hospital to assist in the care of a patient who appears acutely ill, before the patient has respiratory failure, a cardiac arrest or other adverse event. The aim is to prevent situations of “failure to rescue”, to recognize the early signs and symptoms of clinical deterioration prior to requiring transfer to the intensive care unit.
- Reliable Care for Acute Myocardial Infarction (AMI): For appropriate AMI patients, reliable use of all of the following treatments: early administration of aspirin, aspirin at discharge, early administration of a beta-blocker, beta-blocker at discharge, ACE‑inhibitor or angiotensin receptor blocker (ARB) at discharge (if systolic dysfunction), timely reperfusion, and smoking cessation counseling.
- Reliable use of the Ventilator Bundle: A number of hospitals have initiated the use of the ventilator bundle to prevent ventilator associated pneumonia (VAP). VAP carries a high mortality rate. The “bundle” is a grouping of 5 treatments/preventions measured as a composite (% of patients that get all 5).
- Elevate head of bed to 30 degrees
- Peptic ulcer prophylaxis
- Deep venous thrombosis prophylaxis
- Daily “sedation vacation”
- Daily assessment of readiness to extubate
Not all of the items have a specific relationship to VAP (e.g., DVT prophylaxis), but when reliably performed in concert with the other items, leads to a decrease in VAP.
- Reliable use of Central Venous Line Bundles: This is a grouping of 5 preventative measures that when done in concert and measured as a composite have had maximal effectiveness for the reduction of central line associated blood stream infections (CLABs) in some hospitals.
- Hand hygiene
- Maximal barrier precautions
- Chlorhexidine skin antisepsis
- Appropriate catheter site and administration system care
- No routine line replacement
- Surgical site infection (SSI) prophylaxis with a “SSI bundle”: Hospitals participating with the IHI in a variety of different formats have found the most substantial reduction/prevention of SSIs when 3 preventative measures are done in concert with each other for every surgical patient. These preventative measures include:
- Guideline-based use of prophylactic perioperative antibiotics (including both choice and timing of administration of antibiotic)
- Appropriate hair removal (avoiding shaving)
- Perioperative glucose control
- Prevention of adverse drug events with medication reconciliation: This refers to the procedures that can be put in place at the time of any transition of care to mitigate the increased risk of wrong dose of medication or even wrong drug being administered immediately following that transition. Each time we have to transfer information from one sheet of paper to another or from a sheet of paper to a computer, there is chance for human error. Medication reconciliation can virtually eliminate errors occurring at transitions in care.
I have placed in Table 1, the information (goals, background, proposed interventions and success stories) handed out during Dr. Donald Berwick’s opening plenary session, the kick-off for the campaign to save 100,000 lives.
Two key components of the descriptions above deserve further explanation. One of the key components is the concept of reliability. Reliability is how often something in health care does what it is supposed to do, in the time frame it is supposed to do it in. The formula is the number of times that something (delivery of a medication or service) is done correctly divided by the number of times that same something is attempted. In work published by Karl Weick, one common principle within high reliability organizations is that of a preoccupation with failure. As such, the notation of reliability is a measure of defects. Currently much of healthcare (including use of beta-blockers after AMI) functions at a 10-1 level of performance (one defect in 10 tries) or less than a 90% success rate. Organizations that have actively embraced this concept of reliability in their quality improvement work have rejected the usual satisfaction with 10-1 performance. Shouldn’t 99 out of 100 (or 999 out of a 1,000) patients with an AMI get what they are supposed to get?
The other key component embedded within some of the six items that save lives is the concept of bundles. Rather than considering individual measures for each of the items within a bundle, a composite or aggregate measure is reported. Bottom line is that doing any one or two of the items in a bundle is not good enough. It will not achieve the same reduction in hospital acquired infection rates or mortality, as doing all of the items in concert for every appropriate patient.
How can hospitalists help achieve this national goal, to participate in this campaign with the IHI? As individuals, we can be a hospital “precinct captain” or champion, speak to our hospital boards, convene colleagues to standardize to science, start medication reconciliation, and seek composite reliability in our own individual practices.
The IHI will measure this campaign in four ways.
Level 1. Number of hospitals “signing up”
Level 2. Changes in process of care reported
Level 3. Actual changes in deaths and death rates (sample amongst volunteer hospitals)
Level 4. Hospital Standardized Mortality Rates (work of Brian Jarman)
More detailed and specific information about the campaign (and how to participate) can be found on IHI’s Web site (www.ihi.org/ihi/programs/campaign).
“Some is not a number. Soon is not a time.”
The number: 100,000 lives.
The time: June 14, 2006 – 9 a.m. EDT.
References
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction – executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). J Am Coll Cardiol. 2004;44:671-719.
- Antman EM, Lau J, Kupelnick B, Mosteller F, Chalmers TC. A comparison of results of meta-analyses of randomized controlled trials and recommendations of clinical experts: treatments for myocardial infarction. JAMA. 1992;268:240-8.
- Hennekens CH, Albert CM, Godfried SL, Gaziano JM, Buring JE. Adjunctive drug therapy of acute myocardial infarction – evidence from clinical trials. N Engl J Med. 1996;335:1660-7.
- McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348:2635-45.
- Adams K, Corrigan JM, eds. Priority areas for national action: transforming health care quality. Washington, DC: The National Academics Press, 2003.
- Lappe JM, Muhlstein JB, Lappe DL, et al. Improvements in 1-year cardiovascular clinical outcomes associated with a hospital-based discharge medication program. Ann Intern Med. 2004;141:446-53.
- Hackensack University Medical Center AMI Report, Sept 10, 2004.
- McLeod Regional Medical Center Storyboard for the 2004 IHI National Forum.
- Craven DE, Steger KA. Nosocomial pneumonia in mechanically ventilated adult patients: epidemiology and prevention in 1996. Semin Respir Infect. 1996;11:32-53.
- Ibrahim EH, Tracy L, Hill C, Fraser VJ, Kollef MH. The occurrence of ventilator-associated pneumonia in a community hospital: risk factors and clinical outcomes. Chest. 2001;120:555-61.
- Rello J, Ollendorf DA, Oster G, et al. Epidemiology and outcomes of ventilator associated pneumonia in a large U.S. database. Chest. 2002;122:2115-21.
- Guidelines for Preventing Health-Care-Associated Pneumonia, 2003. Recommendations of CDC and the Healthcare Infection Control Practices Advisory Commi Tee. MMWR. 2004;53(No.RR‑3):1-36.
- Dodek P, Keenan S, Cook D, et al. Evidence-based clinical practice guideline for the prevention of ventilator-associated pneumonia. Ann Intern Med. 2004;141:305-13.
- Rello J, Lorente C, Bodi M, Diaz E, Ricart M, Kollef MH. Why do physicians not follow evidence-based guidelines for preventing ventilator-associated pneumonia? A survey based on the opinions of an international panel of intensivists. Chest. 2002;122:656-61.
- Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomized trial. Lancet. 1999;354:1851-58.
- Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342:1471-77.
- Cook DJ, Fuller HD, Guyatt GH, et al. Risk factors for gastrointestinal bleeding in critically ill patients. N Engl J Med. 1994;330:377-81.
- Cook DJ, Reeve BK, Guyatt GH, et al. Stress ulcer prophylaxis in critically ill patients: resolving discordant meta-analyses. JAMA. 1996;275:308-314.
- Cook D, Guyatt G, Marshall J, et al. A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. N Engl J Med. 1998;338:791-97.
- Cook D, Heyland, Griffith L, Cook R, Marshall J, Pagliarello J. Risk factors for clinically important upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. Crit Care Med. 1999;27:2812-17.
- Attia J, Ray JG, Cook DJ, Douketis J, Ginsberg JS, Geerts WH. Deep vein thrombosis and its prevention in critically ill adults. Arch Intern Med. 2001;161:1268-79.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism. The seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest. 2004;126:338S-400S.
- Berenholtz SM, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Crit Care Med. 2004;32:2014-20.
- Pittet D, Tarara D, Wenzel RP. Nosocomial bloodstream infection in critically ill patients. Excess length of stay, extra costs, and aTributable mortality. JAMA. 1994;271:1598-1601.
- Saint S. Chapter 16. Prevention of intravascular catheter-related infection. Making health care safer: a critical analysis of patient safety practices. AHRQ evidence report, number 43, July 20, 2001. www.ncbi.nlm.nih.gov/vooks.
- O’Grady NP; Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections. MMWR Morb Mort Wkly Rep. 2002;51(RR-10):1-29.
- Kirkland KB, et al. The impact of surgical-site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infect Control Hosp Epidemiol. 1999;20:725-30.
- Mangram AJ, Horan TC, Pearson ML, et al. Guidelines for prevention of surgical site infection, 1999. Infect Control Hosp Epidemiol. 1999;20:247-78.
- Classen DC, Pestotnik SL, Evans RS, Lloyd JF, Burke JP. Adverse drug events in hospitalized patients. Excess length of stay, extra costs, and attributable mortality. JAMA. 1997;277:301-06.
- Phillips DP, Christenfeld N, Glynn LM. Increase in U.S. medication-error deaths between 1983 and 1993. Lancet. 1998;351:643-4.
- Rothschild JM, Federic FA, Gandhi TK, Kaushal R, Williams DH, Bates DW. Analysis of medication-related malpractice claims. Causes, preventability, and costs. Arch Intern Med. 2002;162:2414-20.
- Pronovost P, Weast B, Schwarz M, et al. Medication reconciliation: a practical tool to reduce the risk of medication errors. J Crit Care. 2003;18:201-205.
- Rozich JD, Resar RK. Medication safety: one organization’s approach to the challenge. JCOM. 2001;8(10):27-34.
- Rozich JD, Howard RJ, Justeson JM, Macken PD, Lindsay ME, Resar RK. Standardization as a mechanism to improve safety in healthcare. Jt Comm J Qual Saf. 2004;30:5-14.
- Whittington J, Cohen H. OSF Healthcare’s journey in patient safety. Qual Manag Health Care. 2004;13:53-59.
- Needleman J, Buerhaus P, Mattke S, et al. Nursing-staffing levels and the quality of care in hospitals. N Engl J Med. 2002;346:1715-22.
- Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14,270 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58:297-308.
- Sandroni C, Ferro G, Santangelo S, et al. In-hospital cardiac arrest: survival depends mainly on the emergency response. Resuscitation. 2004;62:291-7.
- Schein RM, Hazday N, Pena M, et al. Clinical antecedents to in-hospital cardiopulmonary arrest. Chest. 1990;98:1388-92.
- Hillman K, Parr M, Flabouris A, Bishop G, Stewart A. Redefining in-hospital resuscitation: the concept of the medical emergency team. Resuscitation. 2001;48:105-10.
- Buist MD, Moore GE, Bernard SA, Waxman BP, Anderson JN, Nguyen TV. Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study. BMJ. 2002;324:387-90.
- Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. MJA. 2003;179:283-7.
- Bellomo R, Goldsmith D, Uchino S, et al. Prospective controlled trail of effect of medical emergency team on postoperative morbidity and mortality rates. Crit Car Med. 2004;32:916-21.
- Furnary AP, Zerr KJ, Grunkemeier GL, Starr AL. Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann Thorac Surg. 1999;67: 352-62.
- Van de Berghe G, Wouters P, Weekers F, et all. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359-67.