User login
Studies analyzing the causes of and patterns associated with polypharmacy have increased over the past decade.1-3 Disadvantages to polypharmacy include but are not limited to higher risk of drug-drug interactions, greater potential for adverse effects (AEs), higher risk of nonadherence, and higher costs for the patient and health care systems.1 Compounding the disadvantages associated with polypharmacy, medication storage and disposal are areas of environmental concern. A recent study by Wieczorkiewicz and colleagues examined how patients use, store, and dispose of medications and found that “almost all respondents had excess and leftover medications in their homes.”4 The authors concluded that both overprescribing and poor medication adherence contribute to excess medications at home.
As health care systems become more fiscally responsible, it is beneficial to review prescribing and dispensing patterns, which contribute to polypharmacy and excess medications in patient homes. One of the specific areas that came to the attention of the authors was the number of medication returns received at Evans Army Community Hospital (EACH). As Wiesczorkiewicz and colleagues discovered, it is common that medicine cabinets are filled with expired drugs or medications no longer in use. Although some of these medications can be disposed of in the trash or toilets, some facilities take back unused drugs.5
In an attempt to keep patients and the environment safe, EACH takes back unused medications daily for destruction. These patient returns must be destroyed for both legal and ethical reasons, because there is the potential that medications that have left the system may have been adulterated. The purpose of this quality improvement (QI) project was to evaluate the cost of patient medication returns and explore any additional sources of waste in the prescribing and dispensing processes.
Methods
As a QI project assessing current prescribing and dispensing processes and improving patient-centered performance, Institutional Review Board approval was not required. The QI project and manuscript submission did receive approval from the EACH Command Team. Patient prescription returns were collected at the main and outlying hospital pharmacies between December 16, 2012, and April 5, 2013. Patients were encouraged to bring all medications to clinic visits, and if it was determined that the patient was no longer taking the medication or that the medication was discontinued, the clinician would bring the medication(s) to the patient return collection bin for destruction.
Related: New Guidance on Compounded Drugs
Patients also presented medications no longer used to the pharmacy for the patient return collection bin. A pharmacy technician recorded the medication name, strength, original amount prescribed, and the number of tablets/capsules remaining in the vial. Quantities dispensed greater than the quantities prescribed were later segregated for additional analysis. The brand name of the product was recorded only when the brand name was dispensed. The cost per unit was obtained from the pharmaceutical distributor and recorded to quantify the total cost of each prescription and the total cost of the medications returned. Medications that were classified as hazardous waste were assessed, as were all other medications, and then were segregated to the hospital’s satellite accumulation point for disposal by the Directorate of Public Works Environmental Division. Partial creams and ointments were excluded from the analysis, because the total amount returned was not easily quantifiable.
Results
The total value of the medications collected from December 16, 2012, through April 5, 2013, was $63,183 (1,174 prescriptions). Furthermore, there was the cost of the vials; printer ink; labels; labor to pay pharmacists to process, check, and dispense the medications; and the time of technician staff to fill the prescriptions and later sort the medications to look for hazardous waste and controlled substances. These additional expenses were not quantified and therefore were not included in the aforementioned value.
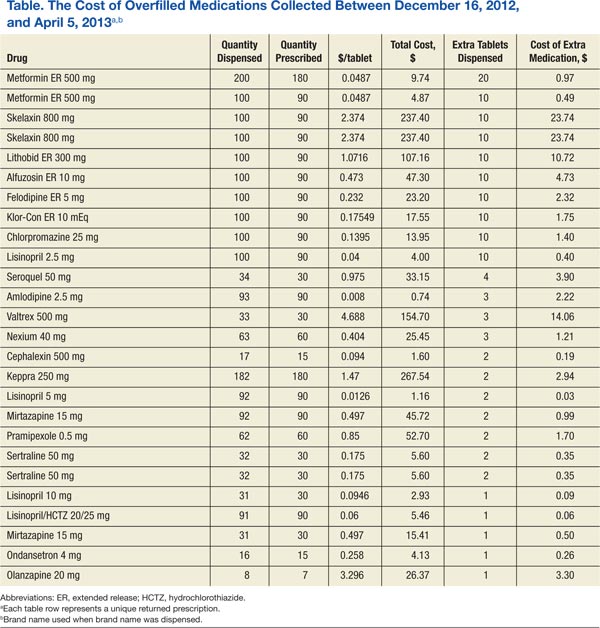
A subanalysis was conducted after it was observed that several prescriptions had greater quantities dispensed than the quantity prescribed (Table). An excess of $102.41 was dispensed and later collected during the study period. Of the 26 prescriptions that were overfilled, 10 were not due to human error but were intentionally overfilled as evidenced by sealed manufacturer bottles; the cost of the medications overfilled for these 10 prescriptions was $70.26.
The top returned drugs in descending order were lisinopril (42), bupropion (32), prazosin (28), gabapentin (27), and ondansetron (26). The top classifications of medications returned in descending order were antidepressants (198), antihypertensives (185), anticonvulsants (61), antilipemics (60), antibiotics (57), and antipsychotics (57). Also noteworthy is that a total of 91 prescriptions (7.8%) for over-the-counter (OTC) products were returned.
Discussion
As suggested by Wieczorkiewicz and colleagues, prescribing and dispensing patterns may be contributing to the accumulation of unwanted and unused medications.4 Patient feedback would also give insight to this problem. Furthermore, the data highlighted improvement opportunities related to back order/shortage and high-dollar medications. Additional exploration into prescribing, dispensing, and consumer patterns as well as potential cost-saving strategies addressing the aforementioned processes is warranted.
Prescribing Patterns
An editorial by Ruef addressed overprescribing patterns and hypothesized that prescribers may be more cautious and prescribe antibiotics (without laboratory confirmation), because if medications are not prescribed, patients with a potentially serious, quickly developing infection may experience an adverse outcome.6 Additionally, there is the anticipation and pressure from patients to receive a medication. Although only 60 of the 1,174 prescriptions were antibiotics or antifungals, one could easily insert other indications into this rationale.
Related: Pharmacists in the Emergency Department: Feasibility and Cost
During the collection period, the problem of polypharmacy stemming from the emergency department (ED), independent of this QI project, was brought to the authors’ attention. Consequently, data were collected from patients who presented for what was perceived (by both the patient and the pharmacy) as a high number of prescriptions from the ED. The data were reviewed and analyzed to determine whether there were any correlations between perceived excessive prescribing and the patient medication return data.
This study found that of 54 patient visits, there were a total of 324 prescriptions with a median of 6 prescriptions per person. The majority (56%) of these prescriptions were for OTC medications. The top 5 medications prescribed were ibuprofen, acetaminophen, ondansetron, oxymetazoline, and pseudoephedrine; 4 of which are OTC medications. The top 5 classifications of medications were decongestants, nonsteroidal anti-inflammatory drugs, analgesics, antibiotics, and antiemetics.
In contrast to the patient return data with 5 of the 6 top medications prescribed for chronic conditions, it is no surprise that the top 5 ED medications were prescribed for acute conditions. Ondansetron, which costs up to $0.37 per tablet, was one of the top prescribed medications from the ED and one of the most frequently returned medications. One might question whether this was a misuse of ED resources, considering patients were seen in this costly setting and received OTC medications. Further study of misappropriation of resources in the ED and trends from other clinic areas are needed.
Dispensing Patterns
In addition, it was observed that the pharmacy was overfilling prescriptions. Inaccurate quantities dispensed may have been due to human error and also due to staff belief that it would cost more (in staff time) to count the exact quantity prescribed for medications supplied in a manufacturer bottle near the amount needed for the prescription. It has been noted by pharmacy staff that deviation from exact counts is only done with medications that do not have a significant cost per tablet or capsule. The cost of medications intentionally overfilled was $70.26—not an insignificant source of waste.
Related: Pharmacist-Managed Collaborative Practice for Chronic Stable Angina
Medications returned to stock (because patients never picked up the prescription) were not used for future prescriptions but rather placed in the patient return collection for destruction. After this practice was noted, these returned-to-stock products were segregated to evaluate the value of the medications that could have been used for future prescriptions. Seventy-six prescriptions could have been dispensed, and the value of these unused medications was $3,049. Whereas civilian retail settings would not allow the practice of destroying medications that can otherwise be dispensed, this practice was permitted at EACH.
Consumer Patterns
It was hypothesized in this study that patients were returning medications because the prescriber switched the medication, the patient ultimately did not need the medication because symptoms resolved on their own, the patient may have had an AE or tolerance issues, the patient died, the dose was adjusted, or the patient had duplicate prescriptions. Further exploration regarding patients’ perspectives should be considered.
Back Orders and Shortages
Similar to many other institutions across the country, EACH has been affected by drug product shortages. There are a number of contributing factors to these shortages, including raw and bulk material unavailability, manufacturer difficulties and regulatory issues, voluntary recalls, change in product formulation or manufacturer, unexpected increases in demand, and shifts in clinical practice.7
An example of a recently recalled medication is atorvastatin. Historical data indicate that EACH paid $0.08 per tablet ($6.77 for a 90-day supply). After the generic manufacturer recalled atorvastatin, the brand-name product needed to be ordered, which cost $1.93 per tablet (or $173.70 for a 90-day supply). During the study, 370 atorvastatin tablets were returned, 90 of which were the brand-name tablets. It was unfortunate that this quantity was dispensed, considering these tablets were destroyed. If it is possible to limit quantities dispensed on manufacturer recall/ back order products until the price is more reasonable, without a significant disruption in patient care, pharmacies may consider policy changes.
High-Dollar Medications
Although the cost of a number of generic medications may be negligible, a number of medications continue to have a significant associated cost. Of the prescriptions returned, 170 cost > $100. Of these, 16 prescriptions cost > $500, and the total was > $13,000.
The U.S. Air Force had a high dollar program, in which patients were limited to a 30-day supply if the 30-day supply cost > $500 for treatment of a chronic condition. The staff burden and difficulty of maintaining such a program is unknown; however, the program is thought-provoking. Specifically, instead of dispensing 90-day supplies, the facility might consider limiting expensive prescriptions to ≤ 30 days for medications with additional refills if needed. Quantity limitations are already implemented for medications such as sildenafil, migraine medications, and opioids.
There is clearly a financial burden that needs to be addressed, and as this study evaluated the waste involved in patient returns, additional sources of waste were illuminated. Lean Six Sigma highlights several forms of waste: transportation, inventory, motion, waiting, overprocessing, overproduction, and defects/errors.8,9 This study found that there were several forms of waste in the prescribing and dispensing processes. Specifically, the authors found inventory mismanagement, overprocessing (overprescribing), overproduction (dispensing more than prescribed), possible misuse of costly resources, and defects/errors.
Limitations
The results of this QI project were limited to unused medications that patients returned to the facility. Returning unused medications is neither requested nor mandatory. Therefore, it is estimated that the true amount of unused medications that could be returned for destruction is vastly greater than the brief collection obtained in this data set. Furthermore, this collection is only a snapshot at one military treatment facility. With multiple facilities within the DoD, the total amount and value of unused medications is likely to be immensely greater than the $63,000 collected in this study.
Additionally, the cost to discard hazardous waste medications was not quantified. Evans Army Community Hospital pays $1.95 per lb for disposal of hazardous waste medications (eg, fluticasone/salmeterol, albuterol, warfarin, insulins), but this financial burden was not addressed in this QI project.
Recommendations
There are a number of behaviors that could be addressed to reduce the waste observed in this study:
- Prescribers should reevaluate prescribing habits to assess whether they are overprescribing medications. They may consider asking the patient whether they plan to take the medication prior to writing the prescription. If the patient is not agreeable to the treatment plan, then the treatment plan may need to be reevaluated.
- Facilities may consider a policy that allows no more than a 30-day supply for new medication prescriptions. Patients should have a follow-up to determine whether the treatment is effective or whether there are AEs, and a new maintenance prescription may be written at that time.
- Pharmacies should ensure that pharmacists fill the quantity prescribed. Prescriptions that have overfills in quantities are considered misbranded.
- Pharmacies should enforce policies for returning to stock the prescriptions that were prepared but never dispensed to patients.
- For medications that are on back order or in short supply, prescribers should consider changing the quantity dispensed to a 30-day supply (or less as appropriate) with refills.
- Pharmacies should consider limiting quantities of high-dollar medications and adding refills for any additional therapy needed.
- Hospitals should evaluate patient use of emergency resources. Other local health treatment facilities outline clearly for patients what constitutes an emergency and what does not. A similar policy change should be considered at EACH.
Summary
Polypharmacy is an increasing problem in today’s medical field. Consequently, unwanted and unused medications accumulate in patients’ homes. In an attempt to keep patients and the environment safe, EACH takes back unused medications every day for destruction. During the collection period of patient returns from December 16, 2012, through April 5, 2013, > $63,000 of unused medications were returned for destruction, which did not include the cost of labor or additional supplies. These data illuminated possible prescribing and dispensing patterns contributing to this waste and inspired further exploration of additional sources of waste, such as overprocessing, overproduction, inventory mismanagement, misuse of resources, and defects/ errors. This study highlighted a number of strategies that, if implemented, may significantly reduce the deficit burden and reduce costs associated with polypharmacy.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Kaur G. Polypharmacy: The past, present and the future. J Adv Pharm Technol Res. 2013;4(4):224-225.
2. Calderón-Larrañaga A, Gimeno-Feliu LA, González-Rubio F, et al. Polypharmacy patterns: Unravelling systematic associations between prescribed medications. PLoS One. 2013;8(12):e84967.
3. Murray MD, Kroenke K. Polypharmacy and medication adherence: Small steps on a long road. J Gen Intern Med. 2001;16(2):137-139.
4. Wieczorkiewicz SM, Kassamali Z, Danziger LH. Behind closed doors: Medication storage and disposal in the home. Ann Pharmacother. 2013;47(4):482-489.
5. U.S. Food and Drug Administration. How to dispose of unused medicines. U.S. Department of Health and Human Services Website. http://www.fda.gov/forconsumers/consumerupdates/ucm101653.htm. Updated February 18, 2015. Accessed March 11, 2015.
6. Ruef C. Why do physicians prescribe antibiotics? Infect. 2011;39(4):287.
7. ASHP Expert Panel on Drug Product Shortages; Fox ER, Birt A, James KB, Kokko H, Salverson S, Soflin DL. ASHP Guidelines on Managing Drug Product Shortages in Hospitals and Health Systems. Am J Health Syst Pharm. 2009;66(15):1399-1406.
8. George M, Rowlands D, Kastle B. What is Lean Six Sigma? New York, NY: McGraw-Hill; 2004.
9. Womack JP, Jones DT. Lean Thinking: Banish Waste and Create Wealth in Your Corporation. New York, NY: Free Press; 2003.
Studies analyzing the causes of and patterns associated with polypharmacy have increased over the past decade.1-3 Disadvantages to polypharmacy include but are not limited to higher risk of drug-drug interactions, greater potential for adverse effects (AEs), higher risk of nonadherence, and higher costs for the patient and health care systems.1 Compounding the disadvantages associated with polypharmacy, medication storage and disposal are areas of environmental concern. A recent study by Wieczorkiewicz and colleagues examined how patients use, store, and dispose of medications and found that “almost all respondents had excess and leftover medications in their homes.”4 The authors concluded that both overprescribing and poor medication adherence contribute to excess medications at home.
As health care systems become more fiscally responsible, it is beneficial to review prescribing and dispensing patterns, which contribute to polypharmacy and excess medications in patient homes. One of the specific areas that came to the attention of the authors was the number of medication returns received at Evans Army Community Hospital (EACH). As Wiesczorkiewicz and colleagues discovered, it is common that medicine cabinets are filled with expired drugs or medications no longer in use. Although some of these medications can be disposed of in the trash or toilets, some facilities take back unused drugs.5
In an attempt to keep patients and the environment safe, EACH takes back unused medications daily for destruction. These patient returns must be destroyed for both legal and ethical reasons, because there is the potential that medications that have left the system may have been adulterated. The purpose of this quality improvement (QI) project was to evaluate the cost of patient medication returns and explore any additional sources of waste in the prescribing and dispensing processes.
Methods
As a QI project assessing current prescribing and dispensing processes and improving patient-centered performance, Institutional Review Board approval was not required. The QI project and manuscript submission did receive approval from the EACH Command Team. Patient prescription returns were collected at the main and outlying hospital pharmacies between December 16, 2012, and April 5, 2013. Patients were encouraged to bring all medications to clinic visits, and if it was determined that the patient was no longer taking the medication or that the medication was discontinued, the clinician would bring the medication(s) to the patient return collection bin for destruction.
Related: New Guidance on Compounded Drugs
Patients also presented medications no longer used to the pharmacy for the patient return collection bin. A pharmacy technician recorded the medication name, strength, original amount prescribed, and the number of tablets/capsules remaining in the vial. Quantities dispensed greater than the quantities prescribed were later segregated for additional analysis. The brand name of the product was recorded only when the brand name was dispensed. The cost per unit was obtained from the pharmaceutical distributor and recorded to quantify the total cost of each prescription and the total cost of the medications returned. Medications that were classified as hazardous waste were assessed, as were all other medications, and then were segregated to the hospital’s satellite accumulation point for disposal by the Directorate of Public Works Environmental Division. Partial creams and ointments were excluded from the analysis, because the total amount returned was not easily quantifiable.
Results
The total value of the medications collected from December 16, 2012, through April 5, 2013, was $63,183 (1,174 prescriptions). Furthermore, there was the cost of the vials; printer ink; labels; labor to pay pharmacists to process, check, and dispense the medications; and the time of technician staff to fill the prescriptions and later sort the medications to look for hazardous waste and controlled substances. These additional expenses were not quantified and therefore were not included in the aforementioned value.
A subanalysis was conducted after it was observed that several prescriptions had greater quantities dispensed than the quantity prescribed (Table). An excess of $102.41 was dispensed and later collected during the study period. Of the 26 prescriptions that were overfilled, 10 were not due to human error but were intentionally overfilled as evidenced by sealed manufacturer bottles; the cost of the medications overfilled for these 10 prescriptions was $70.26.
The top returned drugs in descending order were lisinopril (42), bupropion (32), prazosin (28), gabapentin (27), and ondansetron (26). The top classifications of medications returned in descending order were antidepressants (198), antihypertensives (185), anticonvulsants (61), antilipemics (60), antibiotics (57), and antipsychotics (57). Also noteworthy is that a total of 91 prescriptions (7.8%) for over-the-counter (OTC) products were returned.
Discussion
As suggested by Wieczorkiewicz and colleagues, prescribing and dispensing patterns may be contributing to the accumulation of unwanted and unused medications.4 Patient feedback would also give insight to this problem. Furthermore, the data highlighted improvement opportunities related to back order/shortage and high-dollar medications. Additional exploration into prescribing, dispensing, and consumer patterns as well as potential cost-saving strategies addressing the aforementioned processes is warranted.
Prescribing Patterns
An editorial by Ruef addressed overprescribing patterns and hypothesized that prescribers may be more cautious and prescribe antibiotics (without laboratory confirmation), because if medications are not prescribed, patients with a potentially serious, quickly developing infection may experience an adverse outcome.6 Additionally, there is the anticipation and pressure from patients to receive a medication. Although only 60 of the 1,174 prescriptions were antibiotics or antifungals, one could easily insert other indications into this rationale.
Related: Pharmacists in the Emergency Department: Feasibility and Cost
During the collection period, the problem of polypharmacy stemming from the emergency department (ED), independent of this QI project, was brought to the authors’ attention. Consequently, data were collected from patients who presented for what was perceived (by both the patient and the pharmacy) as a high number of prescriptions from the ED. The data were reviewed and analyzed to determine whether there were any correlations between perceived excessive prescribing and the patient medication return data.
This study found that of 54 patient visits, there were a total of 324 prescriptions with a median of 6 prescriptions per person. The majority (56%) of these prescriptions were for OTC medications. The top 5 medications prescribed were ibuprofen, acetaminophen, ondansetron, oxymetazoline, and pseudoephedrine; 4 of which are OTC medications. The top 5 classifications of medications were decongestants, nonsteroidal anti-inflammatory drugs, analgesics, antibiotics, and antiemetics.
In contrast to the patient return data with 5 of the 6 top medications prescribed for chronic conditions, it is no surprise that the top 5 ED medications were prescribed for acute conditions. Ondansetron, which costs up to $0.37 per tablet, was one of the top prescribed medications from the ED and one of the most frequently returned medications. One might question whether this was a misuse of ED resources, considering patients were seen in this costly setting and received OTC medications. Further study of misappropriation of resources in the ED and trends from other clinic areas are needed.
Dispensing Patterns
In addition, it was observed that the pharmacy was overfilling prescriptions. Inaccurate quantities dispensed may have been due to human error and also due to staff belief that it would cost more (in staff time) to count the exact quantity prescribed for medications supplied in a manufacturer bottle near the amount needed for the prescription. It has been noted by pharmacy staff that deviation from exact counts is only done with medications that do not have a significant cost per tablet or capsule. The cost of medications intentionally overfilled was $70.26—not an insignificant source of waste.
Related: Pharmacist-Managed Collaborative Practice for Chronic Stable Angina
Medications returned to stock (because patients never picked up the prescription) were not used for future prescriptions but rather placed in the patient return collection for destruction. After this practice was noted, these returned-to-stock products were segregated to evaluate the value of the medications that could have been used for future prescriptions. Seventy-six prescriptions could have been dispensed, and the value of these unused medications was $3,049. Whereas civilian retail settings would not allow the practice of destroying medications that can otherwise be dispensed, this practice was permitted at EACH.
Consumer Patterns
It was hypothesized in this study that patients were returning medications because the prescriber switched the medication, the patient ultimately did not need the medication because symptoms resolved on their own, the patient may have had an AE or tolerance issues, the patient died, the dose was adjusted, or the patient had duplicate prescriptions. Further exploration regarding patients’ perspectives should be considered.
Back Orders and Shortages
Similar to many other institutions across the country, EACH has been affected by drug product shortages. There are a number of contributing factors to these shortages, including raw and bulk material unavailability, manufacturer difficulties and regulatory issues, voluntary recalls, change in product formulation or manufacturer, unexpected increases in demand, and shifts in clinical practice.7
An example of a recently recalled medication is atorvastatin. Historical data indicate that EACH paid $0.08 per tablet ($6.77 for a 90-day supply). After the generic manufacturer recalled atorvastatin, the brand-name product needed to be ordered, which cost $1.93 per tablet (or $173.70 for a 90-day supply). During the study, 370 atorvastatin tablets were returned, 90 of which were the brand-name tablets. It was unfortunate that this quantity was dispensed, considering these tablets were destroyed. If it is possible to limit quantities dispensed on manufacturer recall/ back order products until the price is more reasonable, without a significant disruption in patient care, pharmacies may consider policy changes.
High-Dollar Medications
Although the cost of a number of generic medications may be negligible, a number of medications continue to have a significant associated cost. Of the prescriptions returned, 170 cost > $100. Of these, 16 prescriptions cost > $500, and the total was > $13,000.
The U.S. Air Force had a high dollar program, in which patients were limited to a 30-day supply if the 30-day supply cost > $500 for treatment of a chronic condition. The staff burden and difficulty of maintaining such a program is unknown; however, the program is thought-provoking. Specifically, instead of dispensing 90-day supplies, the facility might consider limiting expensive prescriptions to ≤ 30 days for medications with additional refills if needed. Quantity limitations are already implemented for medications such as sildenafil, migraine medications, and opioids.
There is clearly a financial burden that needs to be addressed, and as this study evaluated the waste involved in patient returns, additional sources of waste were illuminated. Lean Six Sigma highlights several forms of waste: transportation, inventory, motion, waiting, overprocessing, overproduction, and defects/errors.8,9 This study found that there were several forms of waste in the prescribing and dispensing processes. Specifically, the authors found inventory mismanagement, overprocessing (overprescribing), overproduction (dispensing more than prescribed), possible misuse of costly resources, and defects/errors.
Limitations
The results of this QI project were limited to unused medications that patients returned to the facility. Returning unused medications is neither requested nor mandatory. Therefore, it is estimated that the true amount of unused medications that could be returned for destruction is vastly greater than the brief collection obtained in this data set. Furthermore, this collection is only a snapshot at one military treatment facility. With multiple facilities within the DoD, the total amount and value of unused medications is likely to be immensely greater than the $63,000 collected in this study.
Additionally, the cost to discard hazardous waste medications was not quantified. Evans Army Community Hospital pays $1.95 per lb for disposal of hazardous waste medications (eg, fluticasone/salmeterol, albuterol, warfarin, insulins), but this financial burden was not addressed in this QI project.
Recommendations
There are a number of behaviors that could be addressed to reduce the waste observed in this study:
- Prescribers should reevaluate prescribing habits to assess whether they are overprescribing medications. They may consider asking the patient whether they plan to take the medication prior to writing the prescription. If the patient is not agreeable to the treatment plan, then the treatment plan may need to be reevaluated.
- Facilities may consider a policy that allows no more than a 30-day supply for new medication prescriptions. Patients should have a follow-up to determine whether the treatment is effective or whether there are AEs, and a new maintenance prescription may be written at that time.
- Pharmacies should ensure that pharmacists fill the quantity prescribed. Prescriptions that have overfills in quantities are considered misbranded.
- Pharmacies should enforce policies for returning to stock the prescriptions that were prepared but never dispensed to patients.
- For medications that are on back order or in short supply, prescribers should consider changing the quantity dispensed to a 30-day supply (or less as appropriate) with refills.
- Pharmacies should consider limiting quantities of high-dollar medications and adding refills for any additional therapy needed.
- Hospitals should evaluate patient use of emergency resources. Other local health treatment facilities outline clearly for patients what constitutes an emergency and what does not. A similar policy change should be considered at EACH.
Summary
Polypharmacy is an increasing problem in today’s medical field. Consequently, unwanted and unused medications accumulate in patients’ homes. In an attempt to keep patients and the environment safe, EACH takes back unused medications every day for destruction. During the collection period of patient returns from December 16, 2012, through April 5, 2013, > $63,000 of unused medications were returned for destruction, which did not include the cost of labor or additional supplies. These data illuminated possible prescribing and dispensing patterns contributing to this waste and inspired further exploration of additional sources of waste, such as overprocessing, overproduction, inventory mismanagement, misuse of resources, and defects/ errors. This study highlighted a number of strategies that, if implemented, may significantly reduce the deficit burden and reduce costs associated with polypharmacy.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Studies analyzing the causes of and patterns associated with polypharmacy have increased over the past decade.1-3 Disadvantages to polypharmacy include but are not limited to higher risk of drug-drug interactions, greater potential for adverse effects (AEs), higher risk of nonadherence, and higher costs for the patient and health care systems.1 Compounding the disadvantages associated with polypharmacy, medication storage and disposal are areas of environmental concern. A recent study by Wieczorkiewicz and colleagues examined how patients use, store, and dispose of medications and found that “almost all respondents had excess and leftover medications in their homes.”4 The authors concluded that both overprescribing and poor medication adherence contribute to excess medications at home.
As health care systems become more fiscally responsible, it is beneficial to review prescribing and dispensing patterns, which contribute to polypharmacy and excess medications in patient homes. One of the specific areas that came to the attention of the authors was the number of medication returns received at Evans Army Community Hospital (EACH). As Wiesczorkiewicz and colleagues discovered, it is common that medicine cabinets are filled with expired drugs or medications no longer in use. Although some of these medications can be disposed of in the trash or toilets, some facilities take back unused drugs.5
In an attempt to keep patients and the environment safe, EACH takes back unused medications daily for destruction. These patient returns must be destroyed for both legal and ethical reasons, because there is the potential that medications that have left the system may have been adulterated. The purpose of this quality improvement (QI) project was to evaluate the cost of patient medication returns and explore any additional sources of waste in the prescribing and dispensing processes.
Methods
As a QI project assessing current prescribing and dispensing processes and improving patient-centered performance, Institutional Review Board approval was not required. The QI project and manuscript submission did receive approval from the EACH Command Team. Patient prescription returns were collected at the main and outlying hospital pharmacies between December 16, 2012, and April 5, 2013. Patients were encouraged to bring all medications to clinic visits, and if it was determined that the patient was no longer taking the medication or that the medication was discontinued, the clinician would bring the medication(s) to the patient return collection bin for destruction.
Related: New Guidance on Compounded Drugs
Patients also presented medications no longer used to the pharmacy for the patient return collection bin. A pharmacy technician recorded the medication name, strength, original amount prescribed, and the number of tablets/capsules remaining in the vial. Quantities dispensed greater than the quantities prescribed were later segregated for additional analysis. The brand name of the product was recorded only when the brand name was dispensed. The cost per unit was obtained from the pharmaceutical distributor and recorded to quantify the total cost of each prescription and the total cost of the medications returned. Medications that were classified as hazardous waste were assessed, as were all other medications, and then were segregated to the hospital’s satellite accumulation point for disposal by the Directorate of Public Works Environmental Division. Partial creams and ointments were excluded from the analysis, because the total amount returned was not easily quantifiable.
Results
The total value of the medications collected from December 16, 2012, through April 5, 2013, was $63,183 (1,174 prescriptions). Furthermore, there was the cost of the vials; printer ink; labels; labor to pay pharmacists to process, check, and dispense the medications; and the time of technician staff to fill the prescriptions and later sort the medications to look for hazardous waste and controlled substances. These additional expenses were not quantified and therefore were not included in the aforementioned value.
A subanalysis was conducted after it was observed that several prescriptions had greater quantities dispensed than the quantity prescribed (Table). An excess of $102.41 was dispensed and later collected during the study period. Of the 26 prescriptions that were overfilled, 10 were not due to human error but were intentionally overfilled as evidenced by sealed manufacturer bottles; the cost of the medications overfilled for these 10 prescriptions was $70.26.
The top returned drugs in descending order were lisinopril (42), bupropion (32), prazosin (28), gabapentin (27), and ondansetron (26). The top classifications of medications returned in descending order were antidepressants (198), antihypertensives (185), anticonvulsants (61), antilipemics (60), antibiotics (57), and antipsychotics (57). Also noteworthy is that a total of 91 prescriptions (7.8%) for over-the-counter (OTC) products were returned.
Discussion
As suggested by Wieczorkiewicz and colleagues, prescribing and dispensing patterns may be contributing to the accumulation of unwanted and unused medications.4 Patient feedback would also give insight to this problem. Furthermore, the data highlighted improvement opportunities related to back order/shortage and high-dollar medications. Additional exploration into prescribing, dispensing, and consumer patterns as well as potential cost-saving strategies addressing the aforementioned processes is warranted.
Prescribing Patterns
An editorial by Ruef addressed overprescribing patterns and hypothesized that prescribers may be more cautious and prescribe antibiotics (without laboratory confirmation), because if medications are not prescribed, patients with a potentially serious, quickly developing infection may experience an adverse outcome.6 Additionally, there is the anticipation and pressure from patients to receive a medication. Although only 60 of the 1,174 prescriptions were antibiotics or antifungals, one could easily insert other indications into this rationale.
Related: Pharmacists in the Emergency Department: Feasibility and Cost
During the collection period, the problem of polypharmacy stemming from the emergency department (ED), independent of this QI project, was brought to the authors’ attention. Consequently, data were collected from patients who presented for what was perceived (by both the patient and the pharmacy) as a high number of prescriptions from the ED. The data were reviewed and analyzed to determine whether there were any correlations between perceived excessive prescribing and the patient medication return data.
This study found that of 54 patient visits, there were a total of 324 prescriptions with a median of 6 prescriptions per person. The majority (56%) of these prescriptions were for OTC medications. The top 5 medications prescribed were ibuprofen, acetaminophen, ondansetron, oxymetazoline, and pseudoephedrine; 4 of which are OTC medications. The top 5 classifications of medications were decongestants, nonsteroidal anti-inflammatory drugs, analgesics, antibiotics, and antiemetics.
In contrast to the patient return data with 5 of the 6 top medications prescribed for chronic conditions, it is no surprise that the top 5 ED medications were prescribed for acute conditions. Ondansetron, which costs up to $0.37 per tablet, was one of the top prescribed medications from the ED and one of the most frequently returned medications. One might question whether this was a misuse of ED resources, considering patients were seen in this costly setting and received OTC medications. Further study of misappropriation of resources in the ED and trends from other clinic areas are needed.
Dispensing Patterns
In addition, it was observed that the pharmacy was overfilling prescriptions. Inaccurate quantities dispensed may have been due to human error and also due to staff belief that it would cost more (in staff time) to count the exact quantity prescribed for medications supplied in a manufacturer bottle near the amount needed for the prescription. It has been noted by pharmacy staff that deviation from exact counts is only done with medications that do not have a significant cost per tablet or capsule. The cost of medications intentionally overfilled was $70.26—not an insignificant source of waste.
Related: Pharmacist-Managed Collaborative Practice for Chronic Stable Angina
Medications returned to stock (because patients never picked up the prescription) were not used for future prescriptions but rather placed in the patient return collection for destruction. After this practice was noted, these returned-to-stock products were segregated to evaluate the value of the medications that could have been used for future prescriptions. Seventy-six prescriptions could have been dispensed, and the value of these unused medications was $3,049. Whereas civilian retail settings would not allow the practice of destroying medications that can otherwise be dispensed, this practice was permitted at EACH.
Consumer Patterns
It was hypothesized in this study that patients were returning medications because the prescriber switched the medication, the patient ultimately did not need the medication because symptoms resolved on their own, the patient may have had an AE or tolerance issues, the patient died, the dose was adjusted, or the patient had duplicate prescriptions. Further exploration regarding patients’ perspectives should be considered.
Back Orders and Shortages
Similar to many other institutions across the country, EACH has been affected by drug product shortages. There are a number of contributing factors to these shortages, including raw and bulk material unavailability, manufacturer difficulties and regulatory issues, voluntary recalls, change in product formulation or manufacturer, unexpected increases in demand, and shifts in clinical practice.7
An example of a recently recalled medication is atorvastatin. Historical data indicate that EACH paid $0.08 per tablet ($6.77 for a 90-day supply). After the generic manufacturer recalled atorvastatin, the brand-name product needed to be ordered, which cost $1.93 per tablet (or $173.70 for a 90-day supply). During the study, 370 atorvastatin tablets were returned, 90 of which were the brand-name tablets. It was unfortunate that this quantity was dispensed, considering these tablets were destroyed. If it is possible to limit quantities dispensed on manufacturer recall/ back order products until the price is more reasonable, without a significant disruption in patient care, pharmacies may consider policy changes.
High-Dollar Medications
Although the cost of a number of generic medications may be negligible, a number of medications continue to have a significant associated cost. Of the prescriptions returned, 170 cost > $100. Of these, 16 prescriptions cost > $500, and the total was > $13,000.
The U.S. Air Force had a high dollar program, in which patients were limited to a 30-day supply if the 30-day supply cost > $500 for treatment of a chronic condition. The staff burden and difficulty of maintaining such a program is unknown; however, the program is thought-provoking. Specifically, instead of dispensing 90-day supplies, the facility might consider limiting expensive prescriptions to ≤ 30 days for medications with additional refills if needed. Quantity limitations are already implemented for medications such as sildenafil, migraine medications, and opioids.
There is clearly a financial burden that needs to be addressed, and as this study evaluated the waste involved in patient returns, additional sources of waste were illuminated. Lean Six Sigma highlights several forms of waste: transportation, inventory, motion, waiting, overprocessing, overproduction, and defects/errors.8,9 This study found that there were several forms of waste in the prescribing and dispensing processes. Specifically, the authors found inventory mismanagement, overprocessing (overprescribing), overproduction (dispensing more than prescribed), possible misuse of costly resources, and defects/errors.
Limitations
The results of this QI project were limited to unused medications that patients returned to the facility. Returning unused medications is neither requested nor mandatory. Therefore, it is estimated that the true amount of unused medications that could be returned for destruction is vastly greater than the brief collection obtained in this data set. Furthermore, this collection is only a snapshot at one military treatment facility. With multiple facilities within the DoD, the total amount and value of unused medications is likely to be immensely greater than the $63,000 collected in this study.
Additionally, the cost to discard hazardous waste medications was not quantified. Evans Army Community Hospital pays $1.95 per lb for disposal of hazardous waste medications (eg, fluticasone/salmeterol, albuterol, warfarin, insulins), but this financial burden was not addressed in this QI project.
Recommendations
There are a number of behaviors that could be addressed to reduce the waste observed in this study:
- Prescribers should reevaluate prescribing habits to assess whether they are overprescribing medications. They may consider asking the patient whether they plan to take the medication prior to writing the prescription. If the patient is not agreeable to the treatment plan, then the treatment plan may need to be reevaluated.
- Facilities may consider a policy that allows no more than a 30-day supply for new medication prescriptions. Patients should have a follow-up to determine whether the treatment is effective or whether there are AEs, and a new maintenance prescription may be written at that time.
- Pharmacies should ensure that pharmacists fill the quantity prescribed. Prescriptions that have overfills in quantities are considered misbranded.
- Pharmacies should enforce policies for returning to stock the prescriptions that were prepared but never dispensed to patients.
- For medications that are on back order or in short supply, prescribers should consider changing the quantity dispensed to a 30-day supply (or less as appropriate) with refills.
- Pharmacies should consider limiting quantities of high-dollar medications and adding refills for any additional therapy needed.
- Hospitals should evaluate patient use of emergency resources. Other local health treatment facilities outline clearly for patients what constitutes an emergency and what does not. A similar policy change should be considered at EACH.
Summary
Polypharmacy is an increasing problem in today’s medical field. Consequently, unwanted and unused medications accumulate in patients’ homes. In an attempt to keep patients and the environment safe, EACH takes back unused medications every day for destruction. During the collection period of patient returns from December 16, 2012, through April 5, 2013, > $63,000 of unused medications were returned for destruction, which did not include the cost of labor or additional supplies. These data illuminated possible prescribing and dispensing patterns contributing to this waste and inspired further exploration of additional sources of waste, such as overprocessing, overproduction, inventory mismanagement, misuse of resources, and defects/ errors. This study highlighted a number of strategies that, if implemented, may significantly reduce the deficit burden and reduce costs associated with polypharmacy.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Kaur G. Polypharmacy: The past, present and the future. J Adv Pharm Technol Res. 2013;4(4):224-225.
2. Calderón-Larrañaga A, Gimeno-Feliu LA, González-Rubio F, et al. Polypharmacy patterns: Unravelling systematic associations between prescribed medications. PLoS One. 2013;8(12):e84967.
3. Murray MD, Kroenke K. Polypharmacy and medication adherence: Small steps on a long road. J Gen Intern Med. 2001;16(2):137-139.
4. Wieczorkiewicz SM, Kassamali Z, Danziger LH. Behind closed doors: Medication storage and disposal in the home. Ann Pharmacother. 2013;47(4):482-489.
5. U.S. Food and Drug Administration. How to dispose of unused medicines. U.S. Department of Health and Human Services Website. http://www.fda.gov/forconsumers/consumerupdates/ucm101653.htm. Updated February 18, 2015. Accessed March 11, 2015.
6. Ruef C. Why do physicians prescribe antibiotics? Infect. 2011;39(4):287.
7. ASHP Expert Panel on Drug Product Shortages; Fox ER, Birt A, James KB, Kokko H, Salverson S, Soflin DL. ASHP Guidelines on Managing Drug Product Shortages in Hospitals and Health Systems. Am J Health Syst Pharm. 2009;66(15):1399-1406.
8. George M, Rowlands D, Kastle B. What is Lean Six Sigma? New York, NY: McGraw-Hill; 2004.
9. Womack JP, Jones DT. Lean Thinking: Banish Waste and Create Wealth in Your Corporation. New York, NY: Free Press; 2003.
1. Kaur G. Polypharmacy: The past, present and the future. J Adv Pharm Technol Res. 2013;4(4):224-225.
2. Calderón-Larrañaga A, Gimeno-Feliu LA, González-Rubio F, et al. Polypharmacy patterns: Unravelling systematic associations between prescribed medications. PLoS One. 2013;8(12):e84967.
3. Murray MD, Kroenke K. Polypharmacy and medication adherence: Small steps on a long road. J Gen Intern Med. 2001;16(2):137-139.
4. Wieczorkiewicz SM, Kassamali Z, Danziger LH. Behind closed doors: Medication storage and disposal in the home. Ann Pharmacother. 2013;47(4):482-489.
5. U.S. Food and Drug Administration. How to dispose of unused medicines. U.S. Department of Health and Human Services Website. http://www.fda.gov/forconsumers/consumerupdates/ucm101653.htm. Updated February 18, 2015. Accessed March 11, 2015.
6. Ruef C. Why do physicians prescribe antibiotics? Infect. 2011;39(4):287.
7. ASHP Expert Panel on Drug Product Shortages; Fox ER, Birt A, James KB, Kokko H, Salverson S, Soflin DL. ASHP Guidelines on Managing Drug Product Shortages in Hospitals and Health Systems. Am J Health Syst Pharm. 2009;66(15):1399-1406.
8. George M, Rowlands D, Kastle B. What is Lean Six Sigma? New York, NY: McGraw-Hill; 2004.
9. Womack JP, Jones DT. Lean Thinking: Banish Waste and Create Wealth in Your Corporation. New York, NY: Free Press; 2003.
