User login
Scenario
John is a 50-year-old man with treated hypertension; his blood pressure is 144/84 mm Hg. His lipid panel shows a total cholesterol level of 236 mg/dL, a low-density lipoprotein (LDL) level of 153 mg/dL, and high-density lipoprotein level of 48 mg/dL after therapeutic lifestyle changes. Should John be started on drug therapy to lower his lipid levels?
Solutions
John’s physician might decide whether to initiate drug therapy by “eyeballing” the lipids and making a clinical “guesstimate,” or by determining the Framingham 10-year risk. The Framingham 10-year risk determination is recommended by the Adult Treatment Panel (ATP III) of the National Institutes of Health.1 Although these calculations can be made using published charts,1 the charts are unwieldy and often not available at the point of care. Here are 3 electronic solutions that provide a better way to determine the ATP III-recommended strategy for your patients.
Atp III Cholesterol Management Guidelines
The first, downloadable free from the National Institutes of Health (Table 1), is entitled ATP III Cholesterol Management Guidelines (NIH-ATP3) and is available only for Palm operating system devices. The user enters the patient’s lipid values, age, and sex (Figure 1A). Known risk factors are checked via taps on the touch-sensitive palm-top device’s screen. If additional information is needed, such as the blood pressure, a second screen asks for those values. Then, the assessment is provided with options for additional information if desired (Figure 1B). The ATP III, or Framingham, risk percentage is for “hard” coronary heart disease (CHD) end points (myocardial infarction and cardiac death) during the next 10 years. NIH-ATP3 is not beamable from one handheld unit to another.
TABLE 1
Sources of programs
| Program | Source |
|---|---|
| NIH-ATP3 | http://hin.nhlbi.nih.gov/palmapps.htm |
| Stat Cholesterol | http://www.statcoder.com |
| Cholesterol 1.1 | http://www.ScyMed.com |
FIGURE 1
Sample screens from ATP III Cholesterol Management Guidelines (NIH-ATP3)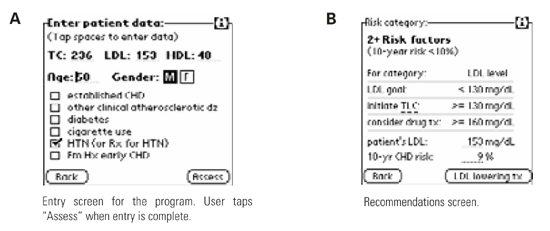
Another option for the Palm operating system is STAT Cholesterol, also downloadable. The price for it is banner advertising occupying about the bottom third of the screen (Figure 2A). STAT Cholesterol also uses ATP III treatment guidelines, but the presentation is different. Rather than numeric entry of lipid values, age, and blood pressure, these data are chosen from drop-down menus specifying ranges. Both ATP III CHD (hard end point) risk and total CHD risk are shown, along with the “average” risk and a “low” risk for age and sex (independent of other factors). As the user changes the values shown on the first screen (age, sex, blood pressure, lipids, and 3 check boxes), the 10-year ATP III risk and total CHD risk percentages change in real time, which is unique among these programs.
The therapeutic recommendations are not as clear on STAT Cholesterol as on the other programs. For example, when a patient is in the highest risk category, NIH-ATP3 clearly specifies that drug therapy is optional for LDL levels of 100 to 129 mg/dL and should be considered when LDL levels are ≥130 mg/dL. STAT Cholesterol lists drug treatment at an LDL level of ≥130 mg/dL but, in STAT Cholesterol, the user has to drill down into the details and scroll down to find that drug treatment is an option for LDL levels of 100 to 129 mg/dL (Figure 2B). However, STAT Cholesterol presents a check-box list for metabolic syndrome, with the appropriate boxes already checked from information previously entered. (Abdominal girth and, for nondiabetic individuals, assessment of fasting blood glucose, are additional user entries to complete this assessment.) This program is the only one of the 3 in this review that allows users (via Menu/options) to choose units of either mg/dL (United States) or mmol/L (the rest of the world). Stat Cholesterol is freely beamable among Palm operating system devices.
FIGURE 2
Sample screens from STAT Cholesterol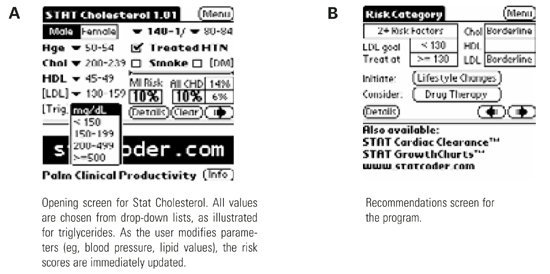
Cholesterol 1.1
The third program is Cholesterol 1.1 by ScyMed, and runs on desktop computers using the Windows operating system. It is available in a CD-only version ($49.95) or a Web-based version. The Web-based version also includes the other resources on ScyMed’s Web site (a medical calculator and history/physical examination templates; single user, $149 per year). Like the other 2 programs, users enter pertinent data, then click “Create Profile.” Appropriately, the program does not force the user to enter all data on the entry screen. A new page opens that contains a summary of the data, including a table explicitly listing Framingham points for each pertinent entry (eg, the points for the age-sex category), the 10-year Framingham CHD (ATP III) risk, and specific suggestions for ATP III-compliant therapy (Figure 3).
Obviously, a major advantage of a PC-based system is the ability to produce a printout for the patient and for the chart. Printouts can be personalized with physician and patient name if the user chooses to enter this information. For physicians who have PC or Internet access in examination rooms or who generally preview laboratory reports in an office with such access, the CD or Web-based system presents an interesting option. Both Cholesterol 1.1 incarnations (CD and Web) include the complete ATP III Executive Summary. The therapy recommendations are hyperlinked to the relevant sections of the ATP-III Summary for users who wish to review any specifics in the recommendations.
FIGURE 3
Sample screen from Cholesterol 1.1
Conclusion
In summary, all 3 options “work.” All are meant to facilitate implementation of the ATP III guidelines. For physicians who wish to use ATP III guidelines to support their therapeutic decisions, all of these options simplify calculation and are better than simply guessing about whether—and which—therapy is appropriate. Regarding the 2 applications for the Palm operating system, Stat Cholesterol has a few more screens than NIH-ATP3, but these serve as helpful reminders about metabolic syndrome and triglyceride levels. Stat Cholesterol’s unique features include choice of units (mmol/L, mg/dL) and “real time” changes in 10-year risk numbers as data are entered or modified. NIH-ATP3 is the “cleanest” and simplest in my opinion. For physicians who have the computer resources and most especially for those who want personalized, printed information for the patient or chart (and are willing to enter these additional data), Cholesterol 1.1 for desktop computers is the way to go.
It is important to remember that the Framingham model was developed in individuals without known established CHD, and consisted largely of non-Hispanic white patients; thus data may not be entirely generalizable to other groups. In 1997, the American Diabetes Association2 also lowered the fasting glucose levels defining diabetes from 140 to 126 mg/dL; thus, the “mildest” forms of diabetes may not have the same prognostic significance. Finally, just because a population with a total cholesterol level of 280 mg/dL has one risk and a population with a total cholesterol level of 220 mg/dL has a lower risk, does not automatically mean that lowering the 280 cholesterol group’s cholesterol to 220 reduces their risk to that of the group whose innate cholesterol level was 220. However, it is tempting to use these data that way.
Finally, the NCEP ATP III tables offer recommendations only through age 79. Cholesterol 1.1 handles ages 80 and above improperly, but provides no error message or explanation. Stat Cholesterol allows only fixed choices from its drop-down menus; for age, these stop at age 79. NIH-ATP III appears to apply the risk values for age 79 to older individuals without modification (or notification to the user), although the product information specifies an age range up to 99 years.
1. National Cholesterol Education Program. Third Report of the Expert Panel on Detection, Evaluation, and Treatment of high blood cholesterol in adults (Adult Treatment Panel III) Executive Summary. NIH publication 01-3670, May 2001. Available from: http://www.nhlbi.nih.gov/guidelines/cholesterol/atp_iii.htm.
2. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997;20:1183-97.
Scenario
John is a 50-year-old man with treated hypertension; his blood pressure is 144/84 mm Hg. His lipid panel shows a total cholesterol level of 236 mg/dL, a low-density lipoprotein (LDL) level of 153 mg/dL, and high-density lipoprotein level of 48 mg/dL after therapeutic lifestyle changes. Should John be started on drug therapy to lower his lipid levels?
Solutions
John’s physician might decide whether to initiate drug therapy by “eyeballing” the lipids and making a clinical “guesstimate,” or by determining the Framingham 10-year risk. The Framingham 10-year risk determination is recommended by the Adult Treatment Panel (ATP III) of the National Institutes of Health.1 Although these calculations can be made using published charts,1 the charts are unwieldy and often not available at the point of care. Here are 3 electronic solutions that provide a better way to determine the ATP III-recommended strategy for your patients.
Atp III Cholesterol Management Guidelines
The first, downloadable free from the National Institutes of Health (Table 1), is entitled ATP III Cholesterol Management Guidelines (NIH-ATP3) and is available only for Palm operating system devices. The user enters the patient’s lipid values, age, and sex (Figure 1A). Known risk factors are checked via taps on the touch-sensitive palm-top device’s screen. If additional information is needed, such as the blood pressure, a second screen asks for those values. Then, the assessment is provided with options for additional information if desired (Figure 1B). The ATP III, or Framingham, risk percentage is for “hard” coronary heart disease (CHD) end points (myocardial infarction and cardiac death) during the next 10 years. NIH-ATP3 is not beamable from one handheld unit to another.
TABLE 1
Sources of programs
| Program | Source |
|---|---|
| NIH-ATP3 | http://hin.nhlbi.nih.gov/palmapps.htm |
| Stat Cholesterol | http://www.statcoder.com |
| Cholesterol 1.1 | http://www.ScyMed.com |
FIGURE 1
Sample screens from ATP III Cholesterol Management Guidelines (NIH-ATP3)
Another option for the Palm operating system is STAT Cholesterol, also downloadable. The price for it is banner advertising occupying about the bottom third of the screen (Figure 2A). STAT Cholesterol also uses ATP III treatment guidelines, but the presentation is different. Rather than numeric entry of lipid values, age, and blood pressure, these data are chosen from drop-down menus specifying ranges. Both ATP III CHD (hard end point) risk and total CHD risk are shown, along with the “average” risk and a “low” risk for age and sex (independent of other factors). As the user changes the values shown on the first screen (age, sex, blood pressure, lipids, and 3 check boxes), the 10-year ATP III risk and total CHD risk percentages change in real time, which is unique among these programs.
The therapeutic recommendations are not as clear on STAT Cholesterol as on the other programs. For example, when a patient is in the highest risk category, NIH-ATP3 clearly specifies that drug therapy is optional for LDL levels of 100 to 129 mg/dL and should be considered when LDL levels are ≥130 mg/dL. STAT Cholesterol lists drug treatment at an LDL level of ≥130 mg/dL but, in STAT Cholesterol, the user has to drill down into the details and scroll down to find that drug treatment is an option for LDL levels of 100 to 129 mg/dL (Figure 2B). However, STAT Cholesterol presents a check-box list for metabolic syndrome, with the appropriate boxes already checked from information previously entered. (Abdominal girth and, for nondiabetic individuals, assessment of fasting blood glucose, are additional user entries to complete this assessment.) This program is the only one of the 3 in this review that allows users (via Menu/options) to choose units of either mg/dL (United States) or mmol/L (the rest of the world). Stat Cholesterol is freely beamable among Palm operating system devices.
FIGURE 2
Sample screens from STAT Cholesterol
Cholesterol 1.1
The third program is Cholesterol 1.1 by ScyMed, and runs on desktop computers using the Windows operating system. It is available in a CD-only version ($49.95) or a Web-based version. The Web-based version also includes the other resources on ScyMed’s Web site (a medical calculator and history/physical examination templates; single user, $149 per year). Like the other 2 programs, users enter pertinent data, then click “Create Profile.” Appropriately, the program does not force the user to enter all data on the entry screen. A new page opens that contains a summary of the data, including a table explicitly listing Framingham points for each pertinent entry (eg, the points for the age-sex category), the 10-year Framingham CHD (ATP III) risk, and specific suggestions for ATP III-compliant therapy (Figure 3).
Obviously, a major advantage of a PC-based system is the ability to produce a printout for the patient and for the chart. Printouts can be personalized with physician and patient name if the user chooses to enter this information. For physicians who have PC or Internet access in examination rooms or who generally preview laboratory reports in an office with such access, the CD or Web-based system presents an interesting option. Both Cholesterol 1.1 incarnations (CD and Web) include the complete ATP III Executive Summary. The therapy recommendations are hyperlinked to the relevant sections of the ATP-III Summary for users who wish to review any specifics in the recommendations.
FIGURE 3
Sample screen from Cholesterol 1.1
Conclusion
In summary, all 3 options “work.” All are meant to facilitate implementation of the ATP III guidelines. For physicians who wish to use ATP III guidelines to support their therapeutic decisions, all of these options simplify calculation and are better than simply guessing about whether—and which—therapy is appropriate. Regarding the 2 applications for the Palm operating system, Stat Cholesterol has a few more screens than NIH-ATP3, but these serve as helpful reminders about metabolic syndrome and triglyceride levels. Stat Cholesterol’s unique features include choice of units (mmol/L, mg/dL) and “real time” changes in 10-year risk numbers as data are entered or modified. NIH-ATP3 is the “cleanest” and simplest in my opinion. For physicians who have the computer resources and most especially for those who want personalized, printed information for the patient or chart (and are willing to enter these additional data), Cholesterol 1.1 for desktop computers is the way to go.
It is important to remember that the Framingham model was developed in individuals without known established CHD, and consisted largely of non-Hispanic white patients; thus data may not be entirely generalizable to other groups. In 1997, the American Diabetes Association2 also lowered the fasting glucose levels defining diabetes from 140 to 126 mg/dL; thus, the “mildest” forms of diabetes may not have the same prognostic significance. Finally, just because a population with a total cholesterol level of 280 mg/dL has one risk and a population with a total cholesterol level of 220 mg/dL has a lower risk, does not automatically mean that lowering the 280 cholesterol group’s cholesterol to 220 reduces their risk to that of the group whose innate cholesterol level was 220. However, it is tempting to use these data that way.
Finally, the NCEP ATP III tables offer recommendations only through age 79. Cholesterol 1.1 handles ages 80 and above improperly, but provides no error message or explanation. Stat Cholesterol allows only fixed choices from its drop-down menus; for age, these stop at age 79. NIH-ATP III appears to apply the risk values for age 79 to older individuals without modification (or notification to the user), although the product information specifies an age range up to 99 years.
Scenario
John is a 50-year-old man with treated hypertension; his blood pressure is 144/84 mm Hg. His lipid panel shows a total cholesterol level of 236 mg/dL, a low-density lipoprotein (LDL) level of 153 mg/dL, and high-density lipoprotein level of 48 mg/dL after therapeutic lifestyle changes. Should John be started on drug therapy to lower his lipid levels?
Solutions
John’s physician might decide whether to initiate drug therapy by “eyeballing” the lipids and making a clinical “guesstimate,” or by determining the Framingham 10-year risk. The Framingham 10-year risk determination is recommended by the Adult Treatment Panel (ATP III) of the National Institutes of Health.1 Although these calculations can be made using published charts,1 the charts are unwieldy and often not available at the point of care. Here are 3 electronic solutions that provide a better way to determine the ATP III-recommended strategy for your patients.
Atp III Cholesterol Management Guidelines
The first, downloadable free from the National Institutes of Health (Table 1), is entitled ATP III Cholesterol Management Guidelines (NIH-ATP3) and is available only for Palm operating system devices. The user enters the patient’s lipid values, age, and sex (Figure 1A). Known risk factors are checked via taps on the touch-sensitive palm-top device’s screen. If additional information is needed, such as the blood pressure, a second screen asks for those values. Then, the assessment is provided with options for additional information if desired (Figure 1B). The ATP III, or Framingham, risk percentage is for “hard” coronary heart disease (CHD) end points (myocardial infarction and cardiac death) during the next 10 years. NIH-ATP3 is not beamable from one handheld unit to another.
TABLE 1
Sources of programs
| Program | Source |
|---|---|
| NIH-ATP3 | http://hin.nhlbi.nih.gov/palmapps.htm |
| Stat Cholesterol | http://www.statcoder.com |
| Cholesterol 1.1 | http://www.ScyMed.com |
FIGURE 1
Sample screens from ATP III Cholesterol Management Guidelines (NIH-ATP3)
Another option for the Palm operating system is STAT Cholesterol, also downloadable. The price for it is banner advertising occupying about the bottom third of the screen (Figure 2A). STAT Cholesterol also uses ATP III treatment guidelines, but the presentation is different. Rather than numeric entry of lipid values, age, and blood pressure, these data are chosen from drop-down menus specifying ranges. Both ATP III CHD (hard end point) risk and total CHD risk are shown, along with the “average” risk and a “low” risk for age and sex (independent of other factors). As the user changes the values shown on the first screen (age, sex, blood pressure, lipids, and 3 check boxes), the 10-year ATP III risk and total CHD risk percentages change in real time, which is unique among these programs.
The therapeutic recommendations are not as clear on STAT Cholesterol as on the other programs. For example, when a patient is in the highest risk category, NIH-ATP3 clearly specifies that drug therapy is optional for LDL levels of 100 to 129 mg/dL and should be considered when LDL levels are ≥130 mg/dL. STAT Cholesterol lists drug treatment at an LDL level of ≥130 mg/dL but, in STAT Cholesterol, the user has to drill down into the details and scroll down to find that drug treatment is an option for LDL levels of 100 to 129 mg/dL (Figure 2B). However, STAT Cholesterol presents a check-box list for metabolic syndrome, with the appropriate boxes already checked from information previously entered. (Abdominal girth and, for nondiabetic individuals, assessment of fasting blood glucose, are additional user entries to complete this assessment.) This program is the only one of the 3 in this review that allows users (via Menu/options) to choose units of either mg/dL (United States) or mmol/L (the rest of the world). Stat Cholesterol is freely beamable among Palm operating system devices.
FIGURE 2
Sample screens from STAT Cholesterol
Cholesterol 1.1
The third program is Cholesterol 1.1 by ScyMed, and runs on desktop computers using the Windows operating system. It is available in a CD-only version ($49.95) or a Web-based version. The Web-based version also includes the other resources on ScyMed’s Web site (a medical calculator and history/physical examination templates; single user, $149 per year). Like the other 2 programs, users enter pertinent data, then click “Create Profile.” Appropriately, the program does not force the user to enter all data on the entry screen. A new page opens that contains a summary of the data, including a table explicitly listing Framingham points for each pertinent entry (eg, the points for the age-sex category), the 10-year Framingham CHD (ATP III) risk, and specific suggestions for ATP III-compliant therapy (Figure 3).
Obviously, a major advantage of a PC-based system is the ability to produce a printout for the patient and for the chart. Printouts can be personalized with physician and patient name if the user chooses to enter this information. For physicians who have PC or Internet access in examination rooms or who generally preview laboratory reports in an office with such access, the CD or Web-based system presents an interesting option. Both Cholesterol 1.1 incarnations (CD and Web) include the complete ATP III Executive Summary. The therapy recommendations are hyperlinked to the relevant sections of the ATP-III Summary for users who wish to review any specifics in the recommendations.
FIGURE 3
Sample screen from Cholesterol 1.1
Conclusion
In summary, all 3 options “work.” All are meant to facilitate implementation of the ATP III guidelines. For physicians who wish to use ATP III guidelines to support their therapeutic decisions, all of these options simplify calculation and are better than simply guessing about whether—and which—therapy is appropriate. Regarding the 2 applications for the Palm operating system, Stat Cholesterol has a few more screens than NIH-ATP3, but these serve as helpful reminders about metabolic syndrome and triglyceride levels. Stat Cholesterol’s unique features include choice of units (mmol/L, mg/dL) and “real time” changes in 10-year risk numbers as data are entered or modified. NIH-ATP3 is the “cleanest” and simplest in my opinion. For physicians who have the computer resources and most especially for those who want personalized, printed information for the patient or chart (and are willing to enter these additional data), Cholesterol 1.1 for desktop computers is the way to go.
It is important to remember that the Framingham model was developed in individuals without known established CHD, and consisted largely of non-Hispanic white patients; thus data may not be entirely generalizable to other groups. In 1997, the American Diabetes Association2 also lowered the fasting glucose levels defining diabetes from 140 to 126 mg/dL; thus, the “mildest” forms of diabetes may not have the same prognostic significance. Finally, just because a population with a total cholesterol level of 280 mg/dL has one risk and a population with a total cholesterol level of 220 mg/dL has a lower risk, does not automatically mean that lowering the 280 cholesterol group’s cholesterol to 220 reduces their risk to that of the group whose innate cholesterol level was 220. However, it is tempting to use these data that way.
Finally, the NCEP ATP III tables offer recommendations only through age 79. Cholesterol 1.1 handles ages 80 and above improperly, but provides no error message or explanation. Stat Cholesterol allows only fixed choices from its drop-down menus; for age, these stop at age 79. NIH-ATP III appears to apply the risk values for age 79 to older individuals without modification (or notification to the user), although the product information specifies an age range up to 99 years.
1. National Cholesterol Education Program. Third Report of the Expert Panel on Detection, Evaluation, and Treatment of high blood cholesterol in adults (Adult Treatment Panel III) Executive Summary. NIH publication 01-3670, May 2001. Available from: http://www.nhlbi.nih.gov/guidelines/cholesterol/atp_iii.htm.
2. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997;20:1183-97.
1. National Cholesterol Education Program. Third Report of the Expert Panel on Detection, Evaluation, and Treatment of high blood cholesterol in adults (Adult Treatment Panel III) Executive Summary. NIH publication 01-3670, May 2001. Available from: http://www.nhlbi.nih.gov/guidelines/cholesterol/atp_iii.htm.
2. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997;20:1183-97.