User login
- Shoulder pain is a common complaint seen in primary care.
- Subacromial impingement syndrome and rotator cuff tears are the most common disorders encountered.
- The history and physical examination are keys to most shoulder pain diagnoses, particularly when used in combination.
- Imaging studies are indicated for failed conservative therapy, severe shoulder pathology, or unclear diagnosis.
Shoulder pain is a common problem that can pose difficult diagnostic and therapeutic challenges for the family physician. It is the third most common musculoskeletal complaint in the general population, and accounts for 5% of all general practitioner musculoskeletal consults.1,2 The incidence of shoulder pain is 6.6 to 25 cases per 1000 patients, with a peak incidence in the fourth through sixth decades.3-6 Shoulder pain is second only to knee pain for referrals to orthopedic surgery or primary care sports medicine clinics.7,8 Furthermore, 8% to 13% of athletic injuries involve the shoulder and account for up to 3.9% of new emergency department visits.9,10
Differential diagnosis
The challenge for the physician evaluating shoulder pain is the myriad of etiologies and the potential for multiple disorders. Compounding the challenge is a lack of uniformity in the literature regarding diagnostic classification.11 As Table 1 shows, the age of the patient will help focus the differential diagnosis. Patients younger than 30 years old tend to have biomechanical or mild inflammatory etiologies for their pain such as atraumatic instability, tendinosis, and arthropathies. Less than 1% of shoulder injuries in persons younger than 30 years are complete rotator cuff tears, which occur in 35% of patients older than 45 years with shoulder pain.12,13
The rotator cuff is the most commonly affected structure in the shoulder, and subacromial impingement syndrome is the leading cause of rotator cuff injury.4,12,14-16 Neer14 described 3 stages of shoulder impingement that he estimated lead to 95% of rotator cuff tears. Impingement can be caused by repetitive overhead activities, acute trauma, or subtle instability (atraumatic instability). The current theory is that inflammation of the rotator cuff tendons and/or bursa, caused by irritation against the coracoacromial arch, can progress to a complete rotator cuff tear over time.
Referred sources of shoulder pain should be included in the differential diagnosis of shoulder pain. Potential sources include cervical spondylolysis, cervical arthritis, cervical disc disease, myocardial ischemia, reflex sympathetic dystrophy, diaphragmatic irritation, thoracic outlet syndrome, and gallbladder disease.
TABLE 1
Differential diagnosis of shoulder pain
| Diagnosis | Primary care setting4-15(%) | Age (y) of presentation, Mean (SD)14 |
|---|---|---|
| Subacromial impingement syndrome | 48–72 | |
| Stage I (edema and hemorrhage) | 16 | 23 (7) |
| Stage II (cuff fibrosis and partial tear) | 42 | 41 (11) |
| Stage III (full-thickness tear) | 15 | 62 (12) |
| Adhesive capsulitis | 16–22 | 53 (10) |
| Acute bursitis | 17 | |
| Calcific tendonitis | 6 | |
| Myofascial pain syndrome | 5 | |
| Glenohumeral joint arthrosis | 2.5 | 64 (10) |
| Thoracic outlet syndrome | 2 | |
| Biceps tendonitis | 0.8 |
Using the history and physical examination
As noted above, the likelihood of specific conditions such as a complete rotator cuff tear varies with the setting, age of the patient, and specialty of the physi-cian.4,13,17,18 It is important to keep this pretest probability in mind while interpreting the history and physical examination. For example, a positive empty can test in a 50-year-old patient almost certainly represents a rotator cuff tear, whereas many younger patients with this finding will not have a tear. Moreover, certain components of the history and physical examination are more indicative of disorders while others are better at ruling them out. This concept is represented by the positive and negative likelihood ratios listed in Table 2.
The clinical evaluation begins with identification of the chief complaint and a thorough history. Common complaints include pain, weakness, stiffness, instability, locking, catching, and deformity.26 Determining the duration of symptoms and mechanism of injury will narrow the differential diagnosis. If trauma occurred, the mechanism can determine radiological needs. Aggravating and alleviating factors should be reviewed, including work, recreation, sports, or hobbies. Night pain when lying on the affected side and a history of trauma in a patient older than 65 years both suggest a rotator cuff tear, but no individual symptom is definitive for the diagnosis (Table 2).19 Pain with overhead work may indicate impingement syndrome, especially if the patient is symptomatic through the arc of 60 to 120 degrees.
The physical examination should include observation, palpation, range of motion (ROM), and provocative testing. Observation requires adequate exposure of the shoulders bilaterally to identify any gross deformities or abnormalities, including muscle atrophy, acromioclavicular joint disparity, or evidence of trauma. Muscle atrophy of either the supraspinatus or infraspinatus muscles is moderately predictive of rotator cuff tears in the elderly population, with a positive predictive value of 81%. However, this sign is not useful if absent, with a negative predictive value of only 43%.19 No studies have assessed the role of palpation in the evaluation of shoulder pain. Nevertheless, the role of palpation in discerning acromioclavicular joint pathology from shoulder and neck makes it a useful part of the examination.
The shoulder’s ROM should be evaluated both actively and passively. The shoulder is a mobile joint with a complexity of movements. These include flexion to 180 degrees, extension to 40 degrees, abduction to 120 degrees with palms down and 180 degrees with palms up, internal rotation to 55 degrees, and external rotation to 45 degrees with arms at the side. Although determining abduction ROM is consistent among examiners,27 interrater reliability is poor for assessment of external rotation ROM. Lack of full ROM that is equally limited with both passive and active examination is found in arthropathies and adhesive capsulitis.
Pain between 60 and 120 degrees of abduction “the painful arc”) is associated with subacromial impingement, whereas pain after 120 degrees is an indication of acromioclavicular joint origin. However, Calis and coworkers17 found that the presence of subacromial impingement has a positive likelihood ratio of only 1.7.
After assessing the ROM, the next steps are to evaluate the rotator cuff and biceps tendon, perform impingement testing, check for instability, and finally assess the acromioclavicular joint. The tests are listed in Table 2 in our preferred order of examination and represent the tests best supported by the evidence; the results are based on a literature search of Medline, PubMed, DARE, and Sports Discuss. The technique of each examination maneuver has been published elsewhere and is not described in detail here. Figure 1 through 4 illustrate several common examination maneuvers described below. A Web site that demonstrates the physical examination more thoroughly can be found at http://www.nismat.org/orthocor/exam/shoulder.html#Evaluation.
TABLE 2
Use of history and physical examination to diagnose shoulder pain
| History or maneuver | Study quality (1A–5)* | Sensitivity | Specificity | LR+ | LR− | PV+ | PV− |
|---|---|---|---|---|---|---|---|
| Rotator cuff tear | |||||||
| History of trauma19 | 2B | 36 | 73 | 1.3 | 0.88 | 72 | 37 |
| Night pain19 | 2B | 88 | 20 | 1.1 | 0.6 | 70 | 43 |
| Painful arc17 | 2B | 33 | 81 | 1.7 | 0.83 | 81 | 33 |
| Empty can test18,20,21 | 1B | 84–89 | 50–58 | 1.7–2 | 0.22–0.28 | 36–98 | 22–93 |
| Drop sign21 | 1B | 21 | 100 | >25 | 0.79 | 100 | 32 |
| Lift off test (for subscapularis tears)21 | 1B | 62 | 100 | >25 | 0.38 | 100 | 69 |
| Impingement | |||||||
| Hawkin’s test20,22 | 1B | 87–89 | 60 | 2.2 | 0.18 | 71 | 83 |
| Instability | |||||||
| Relocation test23 | 2B | 57 | 100 | >25 | 0.43 | 100 | 73 |
| Augmented apprehension23 | 2B | 68 | 100 | >25 | 0.32 | 100 | 78 |
| Labral tear | |||||||
| Crank test24 | 2B | 91 | 93 | 13 | 0.10 | 94 | 90 |
| Active compression test25 | 1B | 100 | 99 | >25 | 0.01 | 95 | 100 |
| Acromioclavicular joint | |||||||
| Active compression test25 | 1B | 100 | 97 | >25 | 0.01 | 89 | 100 |
| *Based on the guidelines for evidence quality outlined by the Center for Evidence-Based Medicine (http://163.1.96.10/docs/levels.html). | |||||||
| LR+ = positive likelihood ratio; LR− = negative likelihood ratio; PV+ = positive predictive value; PV− = negative predictive value. | |||||||
Figure 1
The empty can test
Rotator cuff tests
The drop arm test assesses the integrity of the rotator cuff, predominantly the supraspinatus muscle. The empty can test (Figure 1) isolates the supraspinatus against resistance. The lift off test (Figure 2) assesses the subscapularis integrity.
Figure 2
The lift off test
Impingement syndrome
Hawkin’s sign (Figure 3) is a test for evidence of impingement by re-creation of its symptoms.
Figures 3A & 3B
Hawkin’s sign
Glenohumeral joint stability
The augmented anterior apprehension test evaluates anterior shoulder instability. The relocation test, which helps confirm anterior instability, is carried out immediately after a positive anterior apprehension test.
Labral tears
The crank test is used to identify chronic labral injury, whereas the active compression test25 (Figure 4) indicates labral injury if pain is deep in the shoulder.
Figure 4
The active compression test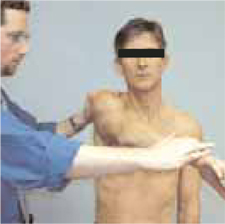
Acromioclavicular joint
The active compression test25 (Figure 4) indicates acromioclavicular joint inflammation, arthritis, or injury if pain is localized to the top of the shoulder.
Diagnostic tests
Imaging studies used in the evaluation of shoulder pain include plain radiographs, arthrography, computed tomography (CT), ultrasound (US), and magnetic resonance imaging (MRI). Often no imaging is required, or plain radiographs are the sole imaging study needed. Soft tissue injuries are best identified by MRI or US, whereas bony pathology is seen best with plain radiographs or CT. Indications for imaging include severe injury, uncontrolled pain, failure of conservative therapy, return to play considerations, and examiner discretion. Table 3 outlines the accuracy of imaging modalities organized by diagnosis.
TABLE 3
Imaging tests to diagnose shoulder pain
| Diagnostic test | Study quality (1A–5)* | Sensitivity | Specificity | LR+ | LR− | PV+ | PV− |
|---|---|---|---|---|---|---|---|
| MRI | |||||||
| Rotator cuff tears | |||||||
| Partial28 | 2B | 82 | 85 | 5.5 | 0.21 | 82 | 85 |
| Complete15 | 1B | 81 | 78 | 3.7 | 0.24 | — | — |
| Overall16,29,30 | 2B | 89–96 | 49–100 | 1.9 to >25 | 0.08 | 58 | 94 |
| Impingement28 | 2B | 93 | 87 | 7.2 | 0.08 | 93 | 87 |
| Labral tears31-32 | 1B | 75–89 | 97–100 | >25 | 0.11–0.25 | 100 | 41 |
| Plain arthrogram | |||||||
| Rotator cuff tears | |||||||
| Partial33 | 1B | 70 | — | — | — | — | — |
| Complete15 | 1A | 50 | 96 | 13 | 0.52 | — | — |
| CT arthrogram | |||||||
| Rotator cuff tears | |||||||
| Partial33 | 1B | 70 | — | — | — | — | — |
| Complete33 | 1B | 95 | — | — | — | — | — |
| Overall33 | 1B | 86 | 98 | >25 | 0.14 | 96 | 93 |
| Ultrasound | |||||||
| Rotator cuff tears | |||||||
| Partial33 | 1B | 80 | — | — | — | — | — |
| Complete33 | 1B | 90 | — | — | — | — | — |
| Overall33,34 | 1B | 86 | 91 | 9.6 | 0.15 | 96 | 73 |
| *Based on the guidelines for evidence quality outlined by the Center for Evidence-Based Medicine (http://163.1.96.10/docs/levels.html). | |||||||
| CT, computed tomography; LR+ = positive likelihood ratio; LR− = negative likelihood ratio; MRI, magnetic resonance imaging; PV+ = positive predictive value; PV− = negative predictive value. | |||||||
Plain radiographs
Plain radiographs are the first step in diagnostic imaging. They can reveal fractures, dislocation, subluxation, bony lesions, outlet obstruction, acromioclavicular joint pathology, and arthritic changes. No definitive clinical studies on the needs of radiographs have been done. Plain radiographs should be taken when ROM is lost, especially when there is abduction of less than 90 degrees, severe pain, and after trauma. Our preferred x-rays include a glenohumeral anteroposterior (AP) view, a supraspinatus outlet view, and an axillary view. Anteroposterior views with internal and external rotation are added in cases of trauma to help rule out fracture. Positive acromioclavicular joint tests (crossover or palpation) should be followed by acromioclavicular joint radiographs because a shoulder series does not give a clear view of this joint. Additional views of the neck as well as a chest x-ray or abdominal imaging should be considered if a referred source of shoulder pain remains a possibility.
Arthrography
Arthrography was the diagnostic test of choice before MRI. It is specific for rotator cuff tears but lacks sensitivity15 because it cannot detect partial-thickness or associated soft tissue injuries of the shoulder. Arthrography still has a role in evaluating adhesive capsulitis by demonstrating decreased intracapsular volume.26 The test can be therapeutic if the capsule is dilated during the procedure. Additionally, patients with claustrophobia may be good candidates for arthrography if a full-thickness tear is suspected and MRI is not possible.
Computed tomography
Computed tomography may be used to evaluate bony lesions, including glenoid rim fractures, humoral fractures, and acromioclavicular joint disease. Computed tomography arthrograms may have a role in assessing labral tears and full-thickness rotator cuff tears.35 The use of CT arthrography has fallen into disfavor compared with MRI because of the risks associated with contrast exposure and poor sensitivity for partial-thickness rotator cuff tears or associated soft tissue injury.
Ultrasound
Ultrasound has been used in the evaluation of rotator cuff tears with varying degrees of sensitivity and specificity.12,29,34 This inconsistency may be related to variation in operator skill. Advantages of US include relatively low cost, speed, and noninvasiveness.
Magnetic resonance imaging
Magnetic resonance imaging has become the gold standard for diagnostic imaging of the shoulder related to soft tissue injury. The advantages include its noninvasive nature, lack of contrast exposure, nonionizing radiation, high degree of resolution, and the ability to evaluate multiple potential pathologic processes.36 Magnetic resonance imaging is the preferred test for evaluating impingement syndrome and rotator cuff pathology. A normal MRI greatly reduces the chances of a rotator cuff tear, with a negative likelihood ratio of 0.08.16,29,30 Magnetic resonance imaging is also useful in the evaluation of avascular necrosis, biceps tendon disorders, inflammatory processes, and tumors.13 The diagnosis of labral lesions can be challenging given the relatively low sensitivity and negative predictive value noted in several trials.16,28,31 Finally, it is important to note that up to one third of all asymptomatic patients and more than half of those older than 60 years demonstrate asymptomatic rotator cuff tears on MRI.37
Approach to the patient
A general approach to the patient with shoulder pain is summarized in Figure 5. Pre- and posttest probabilities are included to give an understanding of how tests may help diagnose or rule out a complete rotator cuff tear. A recent prospective study combining multiple examination maneuvers demonstrated that a combination of 3 physical examination findings (supraspinatus weakness, weakness in external rotation, and impingement) along with the patient’s age can often diagnose or rule out a rotator cuff tear.38 This group of tests did not distinguish full versus partial thickness tears. This approach is summarized in Figure 6.
Figure 5
Basic approach to assess for complete rotator cuff tear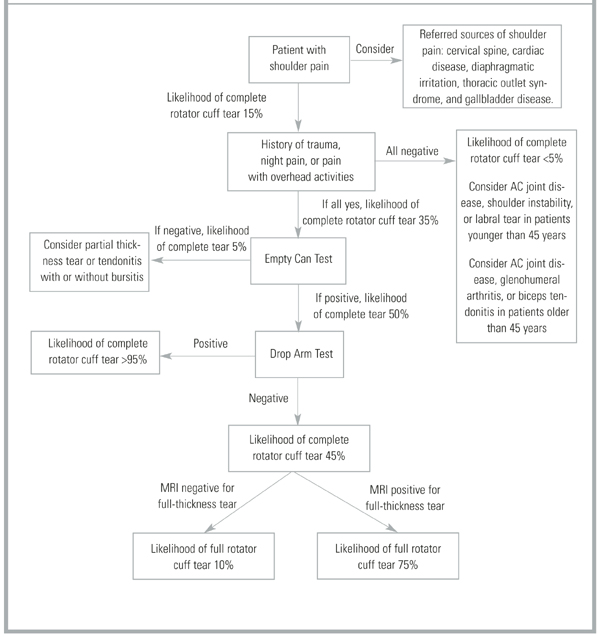
Figure 6
Alternative approach to a suspected rotator cuff tear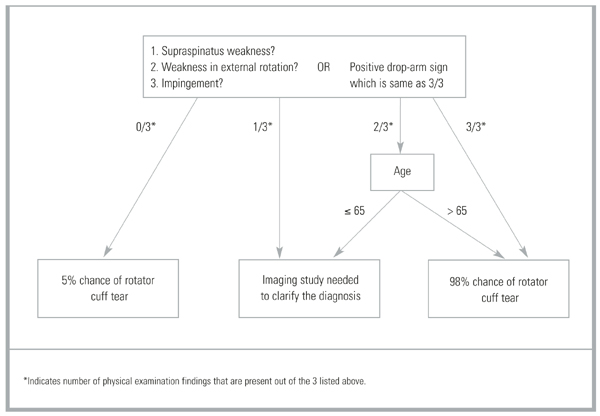
1. Urwin M, Symmons D, Allison T, et al. Estimating the burden of musculoskeletal disorders in the community: the comparative prevalence of symptoms at different anatomical sites, and the relation to social deprivation. Ann Rheum Dis 1998;57:649-55.
2. Peters D, Davies P, Pietroni P. Musculoskeletal clinic in general practice: study of one year’s referrals. Br J Gen Pract 1994;44:25-9.
3. Croft P. Soft-tissue rheumatism. In: Sillman AJ, Hochberg MC, Eds. Epidemiology of the Rheumatic Disease. Oxford, England: Oxford University Press; 1993;375-421.
4. Van der Windt DA, Koes BW, De Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis 1995;54:959-64.
5. Bjelle A. Epidemiology of shoulder problems. Baillieres Clin Rheumatol 1989;3:437-51.
6. Lamberts H, Brouwer HJ, Mohrs J. Reason for Encounter-, Episode-and Process-Oriented Standard Output From Transition Project. Part I. Amsterdam: Department of General Practice/Family Medicine. University of Amsterdam; 1991.
7. Glockner SM. Shoulder pain: a diagnostic dilemma. Am Fam Physician 1995;51:1677-87-1690-2.
8. Butcher JD. Patient profile, referral sources, and consultant utilization in a primary care sports medicine clinic. J Fam Pract 1996;43:556-60.
9. Hill JA. Epidemiological perspective on shoulder injuries. Clin Sports Med 1983;2:241-6.
10. Watters DA, Brooks S, Elton RA, Little K. Sports injuries in an accident and emergency department. Arch Emerg Med 1984;1:105-11.
11. Croft P. Measuring up to shoulder pain. Ann Rheum Dis 1998;57:65-6.
12. Teefey SA, Hasan SA, Middleton WD, Patel M, Wright RW, Yamaguchi K. Ultrasonography of the rotator cuff. A comparison of ultrasonographic and arthroscopic findings in one hundred consecutive cases. J Bone Joint Surg Am 2000;82:498-504.
13. Matsen FA, Lippitt SB, Sidles JA, Harryman DT. Practical Evaluation and Management of the Shoulder. Philadelphia: W.B. Saunders; 1994.
14. Neer CS. Anterior acromioplasty for chronic impingement syndrome of shoulder. J Bone Joint Surg 1972;54A:41-50.
15. Blanchard TK, Bearcroft PW, Constant CR, Griffin DR, Dixon AK. Diagnostic and therapeutic impact of MRI and arthrography in the investigation of full-thickness rotator cuff tears. Eur Radiol 1999;9:638-42.
16. Torstensen ET, Hollinshead RM. Comparison of magnetic resonance imaging and arthroscopy in the evaluation of shoulder pathology. J Shoulder Elbow Surg 1999;8:42-5.
17. Calis M, Akgun K, Birtane M, Karacan I, Calis H, Tuzun F. Diagnostic values of clinical diagnostic tests in subacromial impingement syndrome. Ann Rheum Dis 2000;59:44-7.
18. Itoi E, Kido T, Samo A, Urayama M, Sato K. Which is more useful, the “full can test” or the “empty can test,” in detecting the torn supraspinatus tendon? Am J Sports Med 1999;27:65-8.
19. Litaker D, Pioro M, El Bilbeisi H, Brems J. Returning to the bedside: using the history and physical exam to identify rotator cuff tears. J Am Geriatr Soc 2000;48:1633-7.
20. Leroux JL, Thomas E, Bonnel F, Blotman F. Diagnostic value of clinical tests for shoulder impingement syndrome. Rev Rhum Engl Ed 1995;62:423-8.
21. Hertel R, Ballmer RT, Lombert SM, Gerber C. Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-13.
22. MacDonald PB, Clark P, Sutherland K. An analysis of the diagnostic accuracy of the Hawkins and Neer subacromial impingement signs. J Shoulder Elbow Surg 2000;9:299-301.
23. Speer KP, Hannafin JA, Altchek DW, Warren RF. An evaluation of shoulder relocation test. Am J Sports Med 1994;22:177-83.
24. Liu SH, Henry MH, Nuccion SL. A prospective evaluation of a new physical examination in predicting glenoid labral tears. Am J Sports Med 1996;24:721-5.
25. O’Brien SJ, Pagnani MJ, Fealy S, McGlynn SR, Wilson JB. The active compression test: a new and effective test for diagnosing labral tears and acromioclavicular joint abnormality. Am J Sports Med 1998;26:610-3.
26. Howard T, O’Connor FG. The injured shoulder: primary care assessment. Arch Fam Med 1997;6:376-84.
27. Croft P, Pope D, Boswell R, Rigby A, Silman A. Observer variability in measuring elevation and external rotation of the shoulder. Primary Care Rheumatology Society Shoulder Study Group. Br J Rheumatol 1994;3 3:942-6.
28. Iannotti JP, Zlatkin MB, Esterhai JL, Kressel HY, Dalinka MK, Spindler KP. Magnetic resonance imaging of the shoulder. Sensitivity, specificity, and predictive value. J Bone Joint Surg 1991;73:17-29.
29. Burk DL, Jr, Karasick D, Kurtz AB, et al. Rotator cuff tears: prospective comparison of MR imaging with arthrography, sonography, and surgery. AJR Am J Roentgenol 1989;153:87-92.
30. Yeu K, Jiang CC, Shih TT. Correlation between MRI and operative findings of the rotator cuff tear. J Formos Med Assoc 1994;93:134-9.
31. Green MR, Christensen KP. Magnetic resonance imaging of the glenoid labrum in anterior shoulder instability. Am J Sports Med 1994;22:493-8.
32. Gusmer PB, Potter HG, Schaltz JA, et al. Labral injuries: accuracy of detection with unenhanced MR imaging of the shoulder. Radiology 1996;200:519-24.
33. Farin PU, Kaukanen E, Jaroma H, Vaatainen U, Miettinen H, Soimakallio S. Site and size of rotator-cuff tear. Findings at ultrasound, double-contrast arthrography, and computed tomography arthrography with surgical correlation. Invest Radiol 1996;31:387-94.
34. Van Moppes FI, Veldkam O, Roorda J. Role of shoulder ultrasonography in the evaluation of the painful shoulder. Eur J Radiol 1995;19:142-6.
35. Wilson AJ, Totty WG, Murphy WA, Hardy DC. Shoulder joint: arthrographic CT and long term follow-up, with surgical correlation. Radiology 1989;173:329-33.
36. Meyer SJ, Dalinka MK. Magnetic resonance imaging of the shoulder. Orthop Clin North Am 1990;21:497-513.
37. Sher JS, Uribe JW, Posada A, Murphy B, Zlatkin MB. Abnormal findings on magnetic resonance images of asymptomatic shoulders. J Bone Joint Surg Am 1995;77-A:10-5.
38. Murrell G, Walton J. Diagnosis of rotator cuff tears. Lancet 2001;357:769-70.
- Shoulder pain is a common complaint seen in primary care.
- Subacromial impingement syndrome and rotator cuff tears are the most common disorders encountered.
- The history and physical examination are keys to most shoulder pain diagnoses, particularly when used in combination.
- Imaging studies are indicated for failed conservative therapy, severe shoulder pathology, or unclear diagnosis.
Shoulder pain is a common problem that can pose difficult diagnostic and therapeutic challenges for the family physician. It is the third most common musculoskeletal complaint in the general population, and accounts for 5% of all general practitioner musculoskeletal consults.1,2 The incidence of shoulder pain is 6.6 to 25 cases per 1000 patients, with a peak incidence in the fourth through sixth decades.3-6 Shoulder pain is second only to knee pain for referrals to orthopedic surgery or primary care sports medicine clinics.7,8 Furthermore, 8% to 13% of athletic injuries involve the shoulder and account for up to 3.9% of new emergency department visits.9,10
Differential diagnosis
The challenge for the physician evaluating shoulder pain is the myriad of etiologies and the potential for multiple disorders. Compounding the challenge is a lack of uniformity in the literature regarding diagnostic classification.11 As Table 1 shows, the age of the patient will help focus the differential diagnosis. Patients younger than 30 years old tend to have biomechanical or mild inflammatory etiologies for their pain such as atraumatic instability, tendinosis, and arthropathies. Less than 1% of shoulder injuries in persons younger than 30 years are complete rotator cuff tears, which occur in 35% of patients older than 45 years with shoulder pain.12,13
The rotator cuff is the most commonly affected structure in the shoulder, and subacromial impingement syndrome is the leading cause of rotator cuff injury.4,12,14-16 Neer14 described 3 stages of shoulder impingement that he estimated lead to 95% of rotator cuff tears. Impingement can be caused by repetitive overhead activities, acute trauma, or subtle instability (atraumatic instability). The current theory is that inflammation of the rotator cuff tendons and/or bursa, caused by irritation against the coracoacromial arch, can progress to a complete rotator cuff tear over time.
Referred sources of shoulder pain should be included in the differential diagnosis of shoulder pain. Potential sources include cervical spondylolysis, cervical arthritis, cervical disc disease, myocardial ischemia, reflex sympathetic dystrophy, diaphragmatic irritation, thoracic outlet syndrome, and gallbladder disease.
TABLE 1
Differential diagnosis of shoulder pain
| Diagnosis | Primary care setting4-15(%) | Age (y) of presentation, Mean (SD)14 |
|---|---|---|
| Subacromial impingement syndrome | 48–72 | |
| Stage I (edema and hemorrhage) | 16 | 23 (7) |
| Stage II (cuff fibrosis and partial tear) | 42 | 41 (11) |
| Stage III (full-thickness tear) | 15 | 62 (12) |
| Adhesive capsulitis | 16–22 | 53 (10) |
| Acute bursitis | 17 | |
| Calcific tendonitis | 6 | |
| Myofascial pain syndrome | 5 | |
| Glenohumeral joint arthrosis | 2.5 | 64 (10) |
| Thoracic outlet syndrome | 2 | |
| Biceps tendonitis | 0.8 |
Using the history and physical examination
As noted above, the likelihood of specific conditions such as a complete rotator cuff tear varies with the setting, age of the patient, and specialty of the physi-cian.4,13,17,18 It is important to keep this pretest probability in mind while interpreting the history and physical examination. For example, a positive empty can test in a 50-year-old patient almost certainly represents a rotator cuff tear, whereas many younger patients with this finding will not have a tear. Moreover, certain components of the history and physical examination are more indicative of disorders while others are better at ruling them out. This concept is represented by the positive and negative likelihood ratios listed in Table 2.
The clinical evaluation begins with identification of the chief complaint and a thorough history. Common complaints include pain, weakness, stiffness, instability, locking, catching, and deformity.26 Determining the duration of symptoms and mechanism of injury will narrow the differential diagnosis. If trauma occurred, the mechanism can determine radiological needs. Aggravating and alleviating factors should be reviewed, including work, recreation, sports, or hobbies. Night pain when lying on the affected side and a history of trauma in a patient older than 65 years both suggest a rotator cuff tear, but no individual symptom is definitive for the diagnosis (Table 2).19 Pain with overhead work may indicate impingement syndrome, especially if the patient is symptomatic through the arc of 60 to 120 degrees.
The physical examination should include observation, palpation, range of motion (ROM), and provocative testing. Observation requires adequate exposure of the shoulders bilaterally to identify any gross deformities or abnormalities, including muscle atrophy, acromioclavicular joint disparity, or evidence of trauma. Muscle atrophy of either the supraspinatus or infraspinatus muscles is moderately predictive of rotator cuff tears in the elderly population, with a positive predictive value of 81%. However, this sign is not useful if absent, with a negative predictive value of only 43%.19 No studies have assessed the role of palpation in the evaluation of shoulder pain. Nevertheless, the role of palpation in discerning acromioclavicular joint pathology from shoulder and neck makes it a useful part of the examination.
The shoulder’s ROM should be evaluated both actively and passively. The shoulder is a mobile joint with a complexity of movements. These include flexion to 180 degrees, extension to 40 degrees, abduction to 120 degrees with palms down and 180 degrees with palms up, internal rotation to 55 degrees, and external rotation to 45 degrees with arms at the side. Although determining abduction ROM is consistent among examiners,27 interrater reliability is poor for assessment of external rotation ROM. Lack of full ROM that is equally limited with both passive and active examination is found in arthropathies and adhesive capsulitis.
Pain between 60 and 120 degrees of abduction “the painful arc”) is associated with subacromial impingement, whereas pain after 120 degrees is an indication of acromioclavicular joint origin. However, Calis and coworkers17 found that the presence of subacromial impingement has a positive likelihood ratio of only 1.7.
After assessing the ROM, the next steps are to evaluate the rotator cuff and biceps tendon, perform impingement testing, check for instability, and finally assess the acromioclavicular joint. The tests are listed in Table 2 in our preferred order of examination and represent the tests best supported by the evidence; the results are based on a literature search of Medline, PubMed, DARE, and Sports Discuss. The technique of each examination maneuver has been published elsewhere and is not described in detail here. Figure 1 through 4 illustrate several common examination maneuvers described below. A Web site that demonstrates the physical examination more thoroughly can be found at http://www.nismat.org/orthocor/exam/shoulder.html#Evaluation.
TABLE 2
Use of history and physical examination to diagnose shoulder pain
| History or maneuver | Study quality (1A–5)* | Sensitivity | Specificity | LR+ | LR− | PV+ | PV− |
|---|---|---|---|---|---|---|---|
| Rotator cuff tear | |||||||
| History of trauma19 | 2B | 36 | 73 | 1.3 | 0.88 | 72 | 37 |
| Night pain19 | 2B | 88 | 20 | 1.1 | 0.6 | 70 | 43 |
| Painful arc17 | 2B | 33 | 81 | 1.7 | 0.83 | 81 | 33 |
| Empty can test18,20,21 | 1B | 84–89 | 50–58 | 1.7–2 | 0.22–0.28 | 36–98 | 22–93 |
| Drop sign21 | 1B | 21 | 100 | >25 | 0.79 | 100 | 32 |
| Lift off test (for subscapularis tears)21 | 1B | 62 | 100 | >25 | 0.38 | 100 | 69 |
| Impingement | |||||||
| Hawkin’s test20,22 | 1B | 87–89 | 60 | 2.2 | 0.18 | 71 | 83 |
| Instability | |||||||
| Relocation test23 | 2B | 57 | 100 | >25 | 0.43 | 100 | 73 |
| Augmented apprehension23 | 2B | 68 | 100 | >25 | 0.32 | 100 | 78 |
| Labral tear | |||||||
| Crank test24 | 2B | 91 | 93 | 13 | 0.10 | 94 | 90 |
| Active compression test25 | 1B | 100 | 99 | >25 | 0.01 | 95 | 100 |
| Acromioclavicular joint | |||||||
| Active compression test25 | 1B | 100 | 97 | >25 | 0.01 | 89 | 100 |
| *Based on the guidelines for evidence quality outlined by the Center for Evidence-Based Medicine (http://163.1.96.10/docs/levels.html). | |||||||
| LR+ = positive likelihood ratio; LR− = negative likelihood ratio; PV+ = positive predictive value; PV− = negative predictive value. | |||||||
Figure 1
The empty can test
Rotator cuff tests
The drop arm test assesses the integrity of the rotator cuff, predominantly the supraspinatus muscle. The empty can test (Figure 1) isolates the supraspinatus against resistance. The lift off test (Figure 2) assesses the subscapularis integrity.
Figure 2
The lift off test
Impingement syndrome
Hawkin’s sign (Figure 3) is a test for evidence of impingement by re-creation of its symptoms.
Figures 3A & 3B
Hawkin’s sign
Glenohumeral joint stability
The augmented anterior apprehension test evaluates anterior shoulder instability. The relocation test, which helps confirm anterior instability, is carried out immediately after a positive anterior apprehension test.
Labral tears
The crank test is used to identify chronic labral injury, whereas the active compression test25 (Figure 4) indicates labral injury if pain is deep in the shoulder.
Figure 4
The active compression test
Acromioclavicular joint
The active compression test25 (Figure 4) indicates acromioclavicular joint inflammation, arthritis, or injury if pain is localized to the top of the shoulder.
Diagnostic tests
Imaging studies used in the evaluation of shoulder pain include plain radiographs, arthrography, computed tomography (CT), ultrasound (US), and magnetic resonance imaging (MRI). Often no imaging is required, or plain radiographs are the sole imaging study needed. Soft tissue injuries are best identified by MRI or US, whereas bony pathology is seen best with plain radiographs or CT. Indications for imaging include severe injury, uncontrolled pain, failure of conservative therapy, return to play considerations, and examiner discretion. Table 3 outlines the accuracy of imaging modalities organized by diagnosis.
TABLE 3
Imaging tests to diagnose shoulder pain
| Diagnostic test | Study quality (1A–5)* | Sensitivity | Specificity | LR+ | LR− | PV+ | PV− |
|---|---|---|---|---|---|---|---|
| MRI | |||||||
| Rotator cuff tears | |||||||
| Partial28 | 2B | 82 | 85 | 5.5 | 0.21 | 82 | 85 |
| Complete15 | 1B | 81 | 78 | 3.7 | 0.24 | — | — |
| Overall16,29,30 | 2B | 89–96 | 49–100 | 1.9 to >25 | 0.08 | 58 | 94 |
| Impingement28 | 2B | 93 | 87 | 7.2 | 0.08 | 93 | 87 |
| Labral tears31-32 | 1B | 75–89 | 97–100 | >25 | 0.11–0.25 | 100 | 41 |
| Plain arthrogram | |||||||
| Rotator cuff tears | |||||||
| Partial33 | 1B | 70 | — | — | — | — | — |
| Complete15 | 1A | 50 | 96 | 13 | 0.52 | — | — |
| CT arthrogram | |||||||
| Rotator cuff tears | |||||||
| Partial33 | 1B | 70 | — | — | — | — | — |
| Complete33 | 1B | 95 | — | — | — | — | — |
| Overall33 | 1B | 86 | 98 | >25 | 0.14 | 96 | 93 |
| Ultrasound | |||||||
| Rotator cuff tears | |||||||
| Partial33 | 1B | 80 | — | — | — | — | — |
| Complete33 | 1B | 90 | — | — | — | — | — |
| Overall33,34 | 1B | 86 | 91 | 9.6 | 0.15 | 96 | 73 |
| *Based on the guidelines for evidence quality outlined by the Center for Evidence-Based Medicine (http://163.1.96.10/docs/levels.html). | |||||||
| CT, computed tomography; LR+ = positive likelihood ratio; LR− = negative likelihood ratio; MRI, magnetic resonance imaging; PV+ = positive predictive value; PV− = negative predictive value. | |||||||
Plain radiographs
Plain radiographs are the first step in diagnostic imaging. They can reveal fractures, dislocation, subluxation, bony lesions, outlet obstruction, acromioclavicular joint pathology, and arthritic changes. No definitive clinical studies on the needs of radiographs have been done. Plain radiographs should be taken when ROM is lost, especially when there is abduction of less than 90 degrees, severe pain, and after trauma. Our preferred x-rays include a glenohumeral anteroposterior (AP) view, a supraspinatus outlet view, and an axillary view. Anteroposterior views with internal and external rotation are added in cases of trauma to help rule out fracture. Positive acromioclavicular joint tests (crossover or palpation) should be followed by acromioclavicular joint radiographs because a shoulder series does not give a clear view of this joint. Additional views of the neck as well as a chest x-ray or abdominal imaging should be considered if a referred source of shoulder pain remains a possibility.
Arthrography
Arthrography was the diagnostic test of choice before MRI. It is specific for rotator cuff tears but lacks sensitivity15 because it cannot detect partial-thickness or associated soft tissue injuries of the shoulder. Arthrography still has a role in evaluating adhesive capsulitis by demonstrating decreased intracapsular volume.26 The test can be therapeutic if the capsule is dilated during the procedure. Additionally, patients with claustrophobia may be good candidates for arthrography if a full-thickness tear is suspected and MRI is not possible.
Computed tomography
Computed tomography may be used to evaluate bony lesions, including glenoid rim fractures, humoral fractures, and acromioclavicular joint disease. Computed tomography arthrograms may have a role in assessing labral tears and full-thickness rotator cuff tears.35 The use of CT arthrography has fallen into disfavor compared with MRI because of the risks associated with contrast exposure and poor sensitivity for partial-thickness rotator cuff tears or associated soft tissue injury.
Ultrasound
Ultrasound has been used in the evaluation of rotator cuff tears with varying degrees of sensitivity and specificity.12,29,34 This inconsistency may be related to variation in operator skill. Advantages of US include relatively low cost, speed, and noninvasiveness.
Magnetic resonance imaging
Magnetic resonance imaging has become the gold standard for diagnostic imaging of the shoulder related to soft tissue injury. The advantages include its noninvasive nature, lack of contrast exposure, nonionizing radiation, high degree of resolution, and the ability to evaluate multiple potential pathologic processes.36 Magnetic resonance imaging is the preferred test for evaluating impingement syndrome and rotator cuff pathology. A normal MRI greatly reduces the chances of a rotator cuff tear, with a negative likelihood ratio of 0.08.16,29,30 Magnetic resonance imaging is also useful in the evaluation of avascular necrosis, biceps tendon disorders, inflammatory processes, and tumors.13 The diagnosis of labral lesions can be challenging given the relatively low sensitivity and negative predictive value noted in several trials.16,28,31 Finally, it is important to note that up to one third of all asymptomatic patients and more than half of those older than 60 years demonstrate asymptomatic rotator cuff tears on MRI.37
Approach to the patient
A general approach to the patient with shoulder pain is summarized in Figure 5. Pre- and posttest probabilities are included to give an understanding of how tests may help diagnose or rule out a complete rotator cuff tear. A recent prospective study combining multiple examination maneuvers demonstrated that a combination of 3 physical examination findings (supraspinatus weakness, weakness in external rotation, and impingement) along with the patient’s age can often diagnose or rule out a rotator cuff tear.38 This group of tests did not distinguish full versus partial thickness tears. This approach is summarized in Figure 6.
Figure 5
Basic approach to assess for complete rotator cuff tear
Figure 6
Alternative approach to a suspected rotator cuff tear
- Shoulder pain is a common complaint seen in primary care.
- Subacromial impingement syndrome and rotator cuff tears are the most common disorders encountered.
- The history and physical examination are keys to most shoulder pain diagnoses, particularly when used in combination.
- Imaging studies are indicated for failed conservative therapy, severe shoulder pathology, or unclear diagnosis.
Shoulder pain is a common problem that can pose difficult diagnostic and therapeutic challenges for the family physician. It is the third most common musculoskeletal complaint in the general population, and accounts for 5% of all general practitioner musculoskeletal consults.1,2 The incidence of shoulder pain is 6.6 to 25 cases per 1000 patients, with a peak incidence in the fourth through sixth decades.3-6 Shoulder pain is second only to knee pain for referrals to orthopedic surgery or primary care sports medicine clinics.7,8 Furthermore, 8% to 13% of athletic injuries involve the shoulder and account for up to 3.9% of new emergency department visits.9,10
Differential diagnosis
The challenge for the physician evaluating shoulder pain is the myriad of etiologies and the potential for multiple disorders. Compounding the challenge is a lack of uniformity in the literature regarding diagnostic classification.11 As Table 1 shows, the age of the patient will help focus the differential diagnosis. Patients younger than 30 years old tend to have biomechanical or mild inflammatory etiologies for their pain such as atraumatic instability, tendinosis, and arthropathies. Less than 1% of shoulder injuries in persons younger than 30 years are complete rotator cuff tears, which occur in 35% of patients older than 45 years with shoulder pain.12,13
The rotator cuff is the most commonly affected structure in the shoulder, and subacromial impingement syndrome is the leading cause of rotator cuff injury.4,12,14-16 Neer14 described 3 stages of shoulder impingement that he estimated lead to 95% of rotator cuff tears. Impingement can be caused by repetitive overhead activities, acute trauma, or subtle instability (atraumatic instability). The current theory is that inflammation of the rotator cuff tendons and/or bursa, caused by irritation against the coracoacromial arch, can progress to a complete rotator cuff tear over time.
Referred sources of shoulder pain should be included in the differential diagnosis of shoulder pain. Potential sources include cervical spondylolysis, cervical arthritis, cervical disc disease, myocardial ischemia, reflex sympathetic dystrophy, diaphragmatic irritation, thoracic outlet syndrome, and gallbladder disease.
TABLE 1
Differential diagnosis of shoulder pain
| Diagnosis | Primary care setting4-15(%) | Age (y) of presentation, Mean (SD)14 |
|---|---|---|
| Subacromial impingement syndrome | 48–72 | |
| Stage I (edema and hemorrhage) | 16 | 23 (7) |
| Stage II (cuff fibrosis and partial tear) | 42 | 41 (11) |
| Stage III (full-thickness tear) | 15 | 62 (12) |
| Adhesive capsulitis | 16–22 | 53 (10) |
| Acute bursitis | 17 | |
| Calcific tendonitis | 6 | |
| Myofascial pain syndrome | 5 | |
| Glenohumeral joint arthrosis | 2.5 | 64 (10) |
| Thoracic outlet syndrome | 2 | |
| Biceps tendonitis | 0.8 |
Using the history and physical examination
As noted above, the likelihood of specific conditions such as a complete rotator cuff tear varies with the setting, age of the patient, and specialty of the physi-cian.4,13,17,18 It is important to keep this pretest probability in mind while interpreting the history and physical examination. For example, a positive empty can test in a 50-year-old patient almost certainly represents a rotator cuff tear, whereas many younger patients with this finding will not have a tear. Moreover, certain components of the history and physical examination are more indicative of disorders while others are better at ruling them out. This concept is represented by the positive and negative likelihood ratios listed in Table 2.
The clinical evaluation begins with identification of the chief complaint and a thorough history. Common complaints include pain, weakness, stiffness, instability, locking, catching, and deformity.26 Determining the duration of symptoms and mechanism of injury will narrow the differential diagnosis. If trauma occurred, the mechanism can determine radiological needs. Aggravating and alleviating factors should be reviewed, including work, recreation, sports, or hobbies. Night pain when lying on the affected side and a history of trauma in a patient older than 65 years both suggest a rotator cuff tear, but no individual symptom is definitive for the diagnosis (Table 2).19 Pain with overhead work may indicate impingement syndrome, especially if the patient is symptomatic through the arc of 60 to 120 degrees.
The physical examination should include observation, palpation, range of motion (ROM), and provocative testing. Observation requires adequate exposure of the shoulders bilaterally to identify any gross deformities or abnormalities, including muscle atrophy, acromioclavicular joint disparity, or evidence of trauma. Muscle atrophy of either the supraspinatus or infraspinatus muscles is moderately predictive of rotator cuff tears in the elderly population, with a positive predictive value of 81%. However, this sign is not useful if absent, with a negative predictive value of only 43%.19 No studies have assessed the role of palpation in the evaluation of shoulder pain. Nevertheless, the role of palpation in discerning acromioclavicular joint pathology from shoulder and neck makes it a useful part of the examination.
The shoulder’s ROM should be evaluated both actively and passively. The shoulder is a mobile joint with a complexity of movements. These include flexion to 180 degrees, extension to 40 degrees, abduction to 120 degrees with palms down and 180 degrees with palms up, internal rotation to 55 degrees, and external rotation to 45 degrees with arms at the side. Although determining abduction ROM is consistent among examiners,27 interrater reliability is poor for assessment of external rotation ROM. Lack of full ROM that is equally limited with both passive and active examination is found in arthropathies and adhesive capsulitis.
Pain between 60 and 120 degrees of abduction “the painful arc”) is associated with subacromial impingement, whereas pain after 120 degrees is an indication of acromioclavicular joint origin. However, Calis and coworkers17 found that the presence of subacromial impingement has a positive likelihood ratio of only 1.7.
After assessing the ROM, the next steps are to evaluate the rotator cuff and biceps tendon, perform impingement testing, check for instability, and finally assess the acromioclavicular joint. The tests are listed in Table 2 in our preferred order of examination and represent the tests best supported by the evidence; the results are based on a literature search of Medline, PubMed, DARE, and Sports Discuss. The technique of each examination maneuver has been published elsewhere and is not described in detail here. Figure 1 through 4 illustrate several common examination maneuvers described below. A Web site that demonstrates the physical examination more thoroughly can be found at http://www.nismat.org/orthocor/exam/shoulder.html#Evaluation.
TABLE 2
Use of history and physical examination to diagnose shoulder pain
| History or maneuver | Study quality (1A–5)* | Sensitivity | Specificity | LR+ | LR− | PV+ | PV− |
|---|---|---|---|---|---|---|---|
| Rotator cuff tear | |||||||
| History of trauma19 | 2B | 36 | 73 | 1.3 | 0.88 | 72 | 37 |
| Night pain19 | 2B | 88 | 20 | 1.1 | 0.6 | 70 | 43 |
| Painful arc17 | 2B | 33 | 81 | 1.7 | 0.83 | 81 | 33 |
| Empty can test18,20,21 | 1B | 84–89 | 50–58 | 1.7–2 | 0.22–0.28 | 36–98 | 22–93 |
| Drop sign21 | 1B | 21 | 100 | >25 | 0.79 | 100 | 32 |
| Lift off test (for subscapularis tears)21 | 1B | 62 | 100 | >25 | 0.38 | 100 | 69 |
| Impingement | |||||||
| Hawkin’s test20,22 | 1B | 87–89 | 60 | 2.2 | 0.18 | 71 | 83 |
| Instability | |||||||
| Relocation test23 | 2B | 57 | 100 | >25 | 0.43 | 100 | 73 |
| Augmented apprehension23 | 2B | 68 | 100 | >25 | 0.32 | 100 | 78 |
| Labral tear | |||||||
| Crank test24 | 2B | 91 | 93 | 13 | 0.10 | 94 | 90 |
| Active compression test25 | 1B | 100 | 99 | >25 | 0.01 | 95 | 100 |
| Acromioclavicular joint | |||||||
| Active compression test25 | 1B | 100 | 97 | >25 | 0.01 | 89 | 100 |
| *Based on the guidelines for evidence quality outlined by the Center for Evidence-Based Medicine (http://163.1.96.10/docs/levels.html). | |||||||
| LR+ = positive likelihood ratio; LR− = negative likelihood ratio; PV+ = positive predictive value; PV− = negative predictive value. | |||||||
Figure 1
The empty can test
Rotator cuff tests
The drop arm test assesses the integrity of the rotator cuff, predominantly the supraspinatus muscle. The empty can test (Figure 1) isolates the supraspinatus against resistance. The lift off test (Figure 2) assesses the subscapularis integrity.
Figure 2
The lift off test
Impingement syndrome
Hawkin’s sign (Figure 3) is a test for evidence of impingement by re-creation of its symptoms.
Figures 3A & 3B
Hawkin’s sign
Glenohumeral joint stability
The augmented anterior apprehension test evaluates anterior shoulder instability. The relocation test, which helps confirm anterior instability, is carried out immediately after a positive anterior apprehension test.
Labral tears
The crank test is used to identify chronic labral injury, whereas the active compression test25 (Figure 4) indicates labral injury if pain is deep in the shoulder.
Figure 4
The active compression test
Acromioclavicular joint
The active compression test25 (Figure 4) indicates acromioclavicular joint inflammation, arthritis, or injury if pain is localized to the top of the shoulder.
Diagnostic tests
Imaging studies used in the evaluation of shoulder pain include plain radiographs, arthrography, computed tomography (CT), ultrasound (US), and magnetic resonance imaging (MRI). Often no imaging is required, or plain radiographs are the sole imaging study needed. Soft tissue injuries are best identified by MRI or US, whereas bony pathology is seen best with plain radiographs or CT. Indications for imaging include severe injury, uncontrolled pain, failure of conservative therapy, return to play considerations, and examiner discretion. Table 3 outlines the accuracy of imaging modalities organized by diagnosis.
TABLE 3
Imaging tests to diagnose shoulder pain
| Diagnostic test | Study quality (1A–5)* | Sensitivity | Specificity | LR+ | LR− | PV+ | PV− |
|---|---|---|---|---|---|---|---|
| MRI | |||||||
| Rotator cuff tears | |||||||
| Partial28 | 2B | 82 | 85 | 5.5 | 0.21 | 82 | 85 |
| Complete15 | 1B | 81 | 78 | 3.7 | 0.24 | — | — |
| Overall16,29,30 | 2B | 89–96 | 49–100 | 1.9 to >25 | 0.08 | 58 | 94 |
| Impingement28 | 2B | 93 | 87 | 7.2 | 0.08 | 93 | 87 |
| Labral tears31-32 | 1B | 75–89 | 97–100 | >25 | 0.11–0.25 | 100 | 41 |
| Plain arthrogram | |||||||
| Rotator cuff tears | |||||||
| Partial33 | 1B | 70 | — | — | — | — | — |
| Complete15 | 1A | 50 | 96 | 13 | 0.52 | — | — |
| CT arthrogram | |||||||
| Rotator cuff tears | |||||||
| Partial33 | 1B | 70 | — | — | — | — | — |
| Complete33 | 1B | 95 | — | — | — | — | — |
| Overall33 | 1B | 86 | 98 | >25 | 0.14 | 96 | 93 |
| Ultrasound | |||||||
| Rotator cuff tears | |||||||
| Partial33 | 1B | 80 | — | — | — | — | — |
| Complete33 | 1B | 90 | — | — | — | — | — |
| Overall33,34 | 1B | 86 | 91 | 9.6 | 0.15 | 96 | 73 |
| *Based on the guidelines for evidence quality outlined by the Center for Evidence-Based Medicine (http://163.1.96.10/docs/levels.html). | |||||||
| CT, computed tomography; LR+ = positive likelihood ratio; LR− = negative likelihood ratio; MRI, magnetic resonance imaging; PV+ = positive predictive value; PV− = negative predictive value. | |||||||
Plain radiographs
Plain radiographs are the first step in diagnostic imaging. They can reveal fractures, dislocation, subluxation, bony lesions, outlet obstruction, acromioclavicular joint pathology, and arthritic changes. No definitive clinical studies on the needs of radiographs have been done. Plain radiographs should be taken when ROM is lost, especially when there is abduction of less than 90 degrees, severe pain, and after trauma. Our preferred x-rays include a glenohumeral anteroposterior (AP) view, a supraspinatus outlet view, and an axillary view. Anteroposterior views with internal and external rotation are added in cases of trauma to help rule out fracture. Positive acromioclavicular joint tests (crossover or palpation) should be followed by acromioclavicular joint radiographs because a shoulder series does not give a clear view of this joint. Additional views of the neck as well as a chest x-ray or abdominal imaging should be considered if a referred source of shoulder pain remains a possibility.
Arthrography
Arthrography was the diagnostic test of choice before MRI. It is specific for rotator cuff tears but lacks sensitivity15 because it cannot detect partial-thickness or associated soft tissue injuries of the shoulder. Arthrography still has a role in evaluating adhesive capsulitis by demonstrating decreased intracapsular volume.26 The test can be therapeutic if the capsule is dilated during the procedure. Additionally, patients with claustrophobia may be good candidates for arthrography if a full-thickness tear is suspected and MRI is not possible.
Computed tomography
Computed tomography may be used to evaluate bony lesions, including glenoid rim fractures, humoral fractures, and acromioclavicular joint disease. Computed tomography arthrograms may have a role in assessing labral tears and full-thickness rotator cuff tears.35 The use of CT arthrography has fallen into disfavor compared with MRI because of the risks associated with contrast exposure and poor sensitivity for partial-thickness rotator cuff tears or associated soft tissue injury.
Ultrasound
Ultrasound has been used in the evaluation of rotator cuff tears with varying degrees of sensitivity and specificity.12,29,34 This inconsistency may be related to variation in operator skill. Advantages of US include relatively low cost, speed, and noninvasiveness.
Magnetic resonance imaging
Magnetic resonance imaging has become the gold standard for diagnostic imaging of the shoulder related to soft tissue injury. The advantages include its noninvasive nature, lack of contrast exposure, nonionizing radiation, high degree of resolution, and the ability to evaluate multiple potential pathologic processes.36 Magnetic resonance imaging is the preferred test for evaluating impingement syndrome and rotator cuff pathology. A normal MRI greatly reduces the chances of a rotator cuff tear, with a negative likelihood ratio of 0.08.16,29,30 Magnetic resonance imaging is also useful in the evaluation of avascular necrosis, biceps tendon disorders, inflammatory processes, and tumors.13 The diagnosis of labral lesions can be challenging given the relatively low sensitivity and negative predictive value noted in several trials.16,28,31 Finally, it is important to note that up to one third of all asymptomatic patients and more than half of those older than 60 years demonstrate asymptomatic rotator cuff tears on MRI.37
Approach to the patient
A general approach to the patient with shoulder pain is summarized in Figure 5. Pre- and posttest probabilities are included to give an understanding of how tests may help diagnose or rule out a complete rotator cuff tear. A recent prospective study combining multiple examination maneuvers demonstrated that a combination of 3 physical examination findings (supraspinatus weakness, weakness in external rotation, and impingement) along with the patient’s age can often diagnose or rule out a rotator cuff tear.38 This group of tests did not distinguish full versus partial thickness tears. This approach is summarized in Figure 6.
Figure 5
Basic approach to assess for complete rotator cuff tear
Figure 6
Alternative approach to a suspected rotator cuff tear
1. Urwin M, Symmons D, Allison T, et al. Estimating the burden of musculoskeletal disorders in the community: the comparative prevalence of symptoms at different anatomical sites, and the relation to social deprivation. Ann Rheum Dis 1998;57:649-55.
2. Peters D, Davies P, Pietroni P. Musculoskeletal clinic in general practice: study of one year’s referrals. Br J Gen Pract 1994;44:25-9.
3. Croft P. Soft-tissue rheumatism. In: Sillman AJ, Hochberg MC, Eds. Epidemiology of the Rheumatic Disease. Oxford, England: Oxford University Press; 1993;375-421.
4. Van der Windt DA, Koes BW, De Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis 1995;54:959-64.
5. Bjelle A. Epidemiology of shoulder problems. Baillieres Clin Rheumatol 1989;3:437-51.
6. Lamberts H, Brouwer HJ, Mohrs J. Reason for Encounter-, Episode-and Process-Oriented Standard Output From Transition Project. Part I. Amsterdam: Department of General Practice/Family Medicine. University of Amsterdam; 1991.
7. Glockner SM. Shoulder pain: a diagnostic dilemma. Am Fam Physician 1995;51:1677-87-1690-2.
8. Butcher JD. Patient profile, referral sources, and consultant utilization in a primary care sports medicine clinic. J Fam Pract 1996;43:556-60.
9. Hill JA. Epidemiological perspective on shoulder injuries. Clin Sports Med 1983;2:241-6.
10. Watters DA, Brooks S, Elton RA, Little K. Sports injuries in an accident and emergency department. Arch Emerg Med 1984;1:105-11.
11. Croft P. Measuring up to shoulder pain. Ann Rheum Dis 1998;57:65-6.
12. Teefey SA, Hasan SA, Middleton WD, Patel M, Wright RW, Yamaguchi K. Ultrasonography of the rotator cuff. A comparison of ultrasonographic and arthroscopic findings in one hundred consecutive cases. J Bone Joint Surg Am 2000;82:498-504.
13. Matsen FA, Lippitt SB, Sidles JA, Harryman DT. Practical Evaluation and Management of the Shoulder. Philadelphia: W.B. Saunders; 1994.
14. Neer CS. Anterior acromioplasty for chronic impingement syndrome of shoulder. J Bone Joint Surg 1972;54A:41-50.
15. Blanchard TK, Bearcroft PW, Constant CR, Griffin DR, Dixon AK. Diagnostic and therapeutic impact of MRI and arthrography in the investigation of full-thickness rotator cuff tears. Eur Radiol 1999;9:638-42.
16. Torstensen ET, Hollinshead RM. Comparison of magnetic resonance imaging and arthroscopy in the evaluation of shoulder pathology. J Shoulder Elbow Surg 1999;8:42-5.
17. Calis M, Akgun K, Birtane M, Karacan I, Calis H, Tuzun F. Diagnostic values of clinical diagnostic tests in subacromial impingement syndrome. Ann Rheum Dis 2000;59:44-7.
18. Itoi E, Kido T, Samo A, Urayama M, Sato K. Which is more useful, the “full can test” or the “empty can test,” in detecting the torn supraspinatus tendon? Am J Sports Med 1999;27:65-8.
19. Litaker D, Pioro M, El Bilbeisi H, Brems J. Returning to the bedside: using the history and physical exam to identify rotator cuff tears. J Am Geriatr Soc 2000;48:1633-7.
20. Leroux JL, Thomas E, Bonnel F, Blotman F. Diagnostic value of clinical tests for shoulder impingement syndrome. Rev Rhum Engl Ed 1995;62:423-8.
21. Hertel R, Ballmer RT, Lombert SM, Gerber C. Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-13.
22. MacDonald PB, Clark P, Sutherland K. An analysis of the diagnostic accuracy of the Hawkins and Neer subacromial impingement signs. J Shoulder Elbow Surg 2000;9:299-301.
23. Speer KP, Hannafin JA, Altchek DW, Warren RF. An evaluation of shoulder relocation test. Am J Sports Med 1994;22:177-83.
24. Liu SH, Henry MH, Nuccion SL. A prospective evaluation of a new physical examination in predicting glenoid labral tears. Am J Sports Med 1996;24:721-5.
25. O’Brien SJ, Pagnani MJ, Fealy S, McGlynn SR, Wilson JB. The active compression test: a new and effective test for diagnosing labral tears and acromioclavicular joint abnormality. Am J Sports Med 1998;26:610-3.
26. Howard T, O’Connor FG. The injured shoulder: primary care assessment. Arch Fam Med 1997;6:376-84.
27. Croft P, Pope D, Boswell R, Rigby A, Silman A. Observer variability in measuring elevation and external rotation of the shoulder. Primary Care Rheumatology Society Shoulder Study Group. Br J Rheumatol 1994;3 3:942-6.
28. Iannotti JP, Zlatkin MB, Esterhai JL, Kressel HY, Dalinka MK, Spindler KP. Magnetic resonance imaging of the shoulder. Sensitivity, specificity, and predictive value. J Bone Joint Surg 1991;73:17-29.
29. Burk DL, Jr, Karasick D, Kurtz AB, et al. Rotator cuff tears: prospective comparison of MR imaging with arthrography, sonography, and surgery. AJR Am J Roentgenol 1989;153:87-92.
30. Yeu K, Jiang CC, Shih TT. Correlation between MRI and operative findings of the rotator cuff tear. J Formos Med Assoc 1994;93:134-9.
31. Green MR, Christensen KP. Magnetic resonance imaging of the glenoid labrum in anterior shoulder instability. Am J Sports Med 1994;22:493-8.
32. Gusmer PB, Potter HG, Schaltz JA, et al. Labral injuries: accuracy of detection with unenhanced MR imaging of the shoulder. Radiology 1996;200:519-24.
33. Farin PU, Kaukanen E, Jaroma H, Vaatainen U, Miettinen H, Soimakallio S. Site and size of rotator-cuff tear. Findings at ultrasound, double-contrast arthrography, and computed tomography arthrography with surgical correlation. Invest Radiol 1996;31:387-94.
34. Van Moppes FI, Veldkam O, Roorda J. Role of shoulder ultrasonography in the evaluation of the painful shoulder. Eur J Radiol 1995;19:142-6.
35. Wilson AJ, Totty WG, Murphy WA, Hardy DC. Shoulder joint: arthrographic CT and long term follow-up, with surgical correlation. Radiology 1989;173:329-33.
36. Meyer SJ, Dalinka MK. Magnetic resonance imaging of the shoulder. Orthop Clin North Am 1990;21:497-513.
37. Sher JS, Uribe JW, Posada A, Murphy B, Zlatkin MB. Abnormal findings on magnetic resonance images of asymptomatic shoulders. J Bone Joint Surg Am 1995;77-A:10-5.
38. Murrell G, Walton J. Diagnosis of rotator cuff tears. Lancet 2001;357:769-70.
1. Urwin M, Symmons D, Allison T, et al. Estimating the burden of musculoskeletal disorders in the community: the comparative prevalence of symptoms at different anatomical sites, and the relation to social deprivation. Ann Rheum Dis 1998;57:649-55.
2. Peters D, Davies P, Pietroni P. Musculoskeletal clinic in general practice: study of one year’s referrals. Br J Gen Pract 1994;44:25-9.
3. Croft P. Soft-tissue rheumatism. In: Sillman AJ, Hochberg MC, Eds. Epidemiology of the Rheumatic Disease. Oxford, England: Oxford University Press; 1993;375-421.
4. Van der Windt DA, Koes BW, De Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis 1995;54:959-64.
5. Bjelle A. Epidemiology of shoulder problems. Baillieres Clin Rheumatol 1989;3:437-51.
6. Lamberts H, Brouwer HJ, Mohrs J. Reason for Encounter-, Episode-and Process-Oriented Standard Output From Transition Project. Part I. Amsterdam: Department of General Practice/Family Medicine. University of Amsterdam; 1991.
7. Glockner SM. Shoulder pain: a diagnostic dilemma. Am Fam Physician 1995;51:1677-87-1690-2.
8. Butcher JD. Patient profile, referral sources, and consultant utilization in a primary care sports medicine clinic. J Fam Pract 1996;43:556-60.
9. Hill JA. Epidemiological perspective on shoulder injuries. Clin Sports Med 1983;2:241-6.
10. Watters DA, Brooks S, Elton RA, Little K. Sports injuries in an accident and emergency department. Arch Emerg Med 1984;1:105-11.
11. Croft P. Measuring up to shoulder pain. Ann Rheum Dis 1998;57:65-6.
12. Teefey SA, Hasan SA, Middleton WD, Patel M, Wright RW, Yamaguchi K. Ultrasonography of the rotator cuff. A comparison of ultrasonographic and arthroscopic findings in one hundred consecutive cases. J Bone Joint Surg Am 2000;82:498-504.
13. Matsen FA, Lippitt SB, Sidles JA, Harryman DT. Practical Evaluation and Management of the Shoulder. Philadelphia: W.B. Saunders; 1994.
14. Neer CS. Anterior acromioplasty for chronic impingement syndrome of shoulder. J Bone Joint Surg 1972;54A:41-50.
15. Blanchard TK, Bearcroft PW, Constant CR, Griffin DR, Dixon AK. Diagnostic and therapeutic impact of MRI and arthrography in the investigation of full-thickness rotator cuff tears. Eur Radiol 1999;9:638-42.
16. Torstensen ET, Hollinshead RM. Comparison of magnetic resonance imaging and arthroscopy in the evaluation of shoulder pathology. J Shoulder Elbow Surg 1999;8:42-5.
17. Calis M, Akgun K, Birtane M, Karacan I, Calis H, Tuzun F. Diagnostic values of clinical diagnostic tests in subacromial impingement syndrome. Ann Rheum Dis 2000;59:44-7.
18. Itoi E, Kido T, Samo A, Urayama M, Sato K. Which is more useful, the “full can test” or the “empty can test,” in detecting the torn supraspinatus tendon? Am J Sports Med 1999;27:65-8.
19. Litaker D, Pioro M, El Bilbeisi H, Brems J. Returning to the bedside: using the history and physical exam to identify rotator cuff tears. J Am Geriatr Soc 2000;48:1633-7.
20. Leroux JL, Thomas E, Bonnel F, Blotman F. Diagnostic value of clinical tests for shoulder impingement syndrome. Rev Rhum Engl Ed 1995;62:423-8.
21. Hertel R, Ballmer RT, Lombert SM, Gerber C. Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-13.
22. MacDonald PB, Clark P, Sutherland K. An analysis of the diagnostic accuracy of the Hawkins and Neer subacromial impingement signs. J Shoulder Elbow Surg 2000;9:299-301.
23. Speer KP, Hannafin JA, Altchek DW, Warren RF. An evaluation of shoulder relocation test. Am J Sports Med 1994;22:177-83.
24. Liu SH, Henry MH, Nuccion SL. A prospective evaluation of a new physical examination in predicting glenoid labral tears. Am J Sports Med 1996;24:721-5.
25. O’Brien SJ, Pagnani MJ, Fealy S, McGlynn SR, Wilson JB. The active compression test: a new and effective test for diagnosing labral tears and acromioclavicular joint abnormality. Am J Sports Med 1998;26:610-3.
26. Howard T, O’Connor FG. The injured shoulder: primary care assessment. Arch Fam Med 1997;6:376-84.
27. Croft P, Pope D, Boswell R, Rigby A, Silman A. Observer variability in measuring elevation and external rotation of the shoulder. Primary Care Rheumatology Society Shoulder Study Group. Br J Rheumatol 1994;3 3:942-6.
28. Iannotti JP, Zlatkin MB, Esterhai JL, Kressel HY, Dalinka MK, Spindler KP. Magnetic resonance imaging of the shoulder. Sensitivity, specificity, and predictive value. J Bone Joint Surg 1991;73:17-29.
29. Burk DL, Jr, Karasick D, Kurtz AB, et al. Rotator cuff tears: prospective comparison of MR imaging with arthrography, sonography, and surgery. AJR Am J Roentgenol 1989;153:87-92.
30. Yeu K, Jiang CC, Shih TT. Correlation between MRI and operative findings of the rotator cuff tear. J Formos Med Assoc 1994;93:134-9.
31. Green MR, Christensen KP. Magnetic resonance imaging of the glenoid labrum in anterior shoulder instability. Am J Sports Med 1994;22:493-8.
32. Gusmer PB, Potter HG, Schaltz JA, et al. Labral injuries: accuracy of detection with unenhanced MR imaging of the shoulder. Radiology 1996;200:519-24.
33. Farin PU, Kaukanen E, Jaroma H, Vaatainen U, Miettinen H, Soimakallio S. Site and size of rotator-cuff tear. Findings at ultrasound, double-contrast arthrography, and computed tomography arthrography with surgical correlation. Invest Radiol 1996;31:387-94.
34. Van Moppes FI, Veldkam O, Roorda J. Role of shoulder ultrasonography in the evaluation of the painful shoulder. Eur J Radiol 1995;19:142-6.
35. Wilson AJ, Totty WG, Murphy WA, Hardy DC. Shoulder joint: arthrographic CT and long term follow-up, with surgical correlation. Radiology 1989;173:329-33.
36. Meyer SJ, Dalinka MK. Magnetic resonance imaging of the shoulder. Orthop Clin North Am 1990;21:497-513.
37. Sher JS, Uribe JW, Posada A, Murphy B, Zlatkin MB. Abnormal findings on magnetic resonance images of asymptomatic shoulders. J Bone Joint Surg Am 1995;77-A:10-5.
38. Murrell G, Walton J. Diagnosis of rotator cuff tears. Lancet 2001;357:769-70.