User login
The sesamoid bones are a major contributor to normal gait, with more than 50% of body weight transmitted through the hallux metatarsophalangeal joint (MTPJ) complex. There are varying amounts of stress on the sesamoids, dependent on the gait cycle.1,2 The sesamoids act as a fulcrum to increase the mechanical force of the flexor hallucis brevis tendon.3 Sesamoid pathology can be a source of significant morbidity in patients, especially young athletes or laborers who spend long hours on their feet. More common causes of isolated sesamoid discomfort include sesamoiditis, fracture, and avascular necrosis, with neoplastic, infectious, and inflammatory conditions rarely isolated to the sesamoid.
Gout is a systemic disorder of uric acid metabolism characterized by deposition of monosodium urate crystals in soft tissues and joints.1 This deposition leads to tophus formation with an accompanying inflammatory response. Gout progresses through 3 stages, beginning with acute gout, which may end with chronic, recurrent, and tophaceous gouty arthritis. The hallux MTPJ is the most common joint affected by gout, with few case reports of primary sesamoid gout.1-2,4 We present a case of gout, with radiographic findings isolated to the medial sesamoid, that mimicked a neoplastic process in a patient with no known history of gout. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 37-year-old laborer presented for evaluation of a right sesamoid injury he sustained 4 months earlier when he fell off a ladder and had acute onset plantar hallux MTPJ pain and swelling. He was treated by an outside physician for a presumptive diagnosis of a medial sesamoid fracture with rest and controlled ankle movement (CAM) boot immobilization that resulted in slowly improving symptoms. In discussion of the patient’s history, he reported that 1 year earlier he had a traumatic event with similar symptoms of MTPJ pain and swelling. At that time, treatment with a CAM boot resulted in complete resolution of pain. His outside physician performed a hematologic workup for gout, which showed a normal uric acid level.
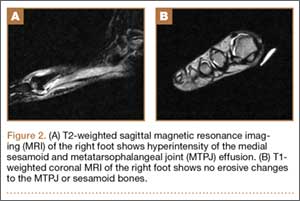
On examination, the patient presented with edema to the right hallux MTPJ and mild tenderness to palpation of the medial sesamoid. He had no pain with motion of the hallux MTPJ or with palpation of the lateral sesamoid. His radiographs showed a bipartite versus fractured sesamoid (Figures 1A, 1B) and serial magnetic resonance imaging (MRI) showed an MTPJ effusion and hyperintense signal in the medial sesamoid, but no erosive findings or soft-tissue masses (Figures 2A, 2B).

The patient was treated with wedge-sandal forefoot offloading, leading to resolution of symptoms over 6 weeks, at which point he was transitioned to normal shoe wear and allowed to progress in his activity as dictated by his symptoms. He presented for reevaluation approximately 2 weeks later with acute, atraumatic onset of plantar left hallux pain and swelling. His examination showed diffuse hallux MTPJ swelling and tenderness isolated to the medial sesamoid. An attempt at aspiration of the MTPJ yielded no fluid, and the patient again was placed in a forefoot-offloading sandal.
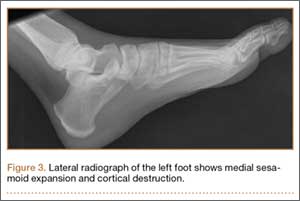
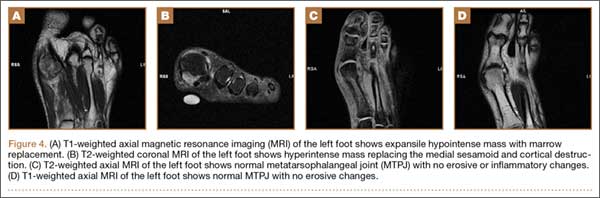
Radiographs of the left foot showed an expansile destructive lesion of the medial sesamoid with interval change from his previous imaging approximately 3 months earlier, obtained as part of his contralateral foot evaluation (Figure 3). MRI with and without contrast showed an expansile process isolated to the medial sesamoid with cortical thinning and marrow replacement (Figures 4A-4D).
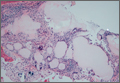
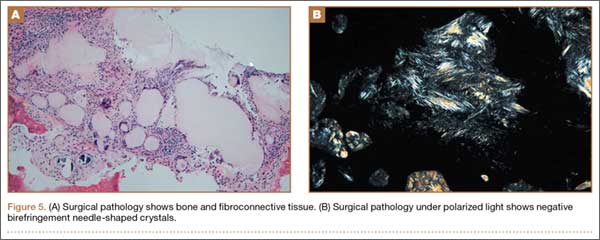
Because of continued discomfort and lack of a definitive diagnosis, an excisional biopsy of the sesamoid was performed. Intraoperatively, the sesamoid was extensively fragmented with near complete replacement by a chalky tophus, as well as chalky deposition throughout the hallux MTPJ. No significant degenerative changes were observed. Surgical pathology showed bone and fibroconnective tissue with deposits of negative birefringement needle-shaped crystals consistent with monosodium urate deposition and foreign body histocytic reaction, as well as repair reaction of bone (Figures 5A, 5B).
Postoperatively, the patient was again placed in a forefoot-offloading wedge sandal for 6 weeks, followed by progression of activity as dictated by his symptoms. He was also evaluated by a rheumatologist and started on medical treatment for gout, with complete resolution of his bilateral hallux pain. He has been able to return to his previous employment.
Discussion
The sesamoid bones are an important component of the hallux MTPJ complex, giving a mechanical advantage to the flexor hallucis brevis tendons in plantar flexion of the hallux.5 Many pathologic conditions have been well described in the literature, including fracture, sesamoiditis, nonunion, avascular necrosis, and plantar keratosis. There is also a 10% incidence of bipartite sesamoids, most commonly isolated to the medial sesamoid, with up to 25% of patients presenting with bilateral bipartite sesamoids.5 Neoplastic processes of the sesamoid are rare, with a paucity of reports in the literature.6,7 Gout is a condition in which hyperuricemia, due to an imbalance in uric acid production and excretion, leads to deposition of monosodium urate crystals in joints, bones, and soft tissues, causing an inflammatory reaction. Risk factors for gout are male sex, advanced age, and ethnicity, as well as obesity, high protein diet, alcohol use, hypertension, and certain medications. Precipitation of acute attacks has been associated with acute trauma, and the first MTPJ is the most common location for an acute attack.8
Isolated sesamoid lesions are rare, with few isolated case reports in the literature. Benign and malignant lesions appear most often in the metatarsals, with the calcaneus being the second most commonly afflicted site.9 The typical differential diagnosis for isolated lytic bone lesions includes fibrous dysplasia, osteoblastoma, giant cell tumor, metastatic lesion, multiple myeloma, aneurysmal bone cyst, chondroblastoma, brown tumor, infection, eosinophilic granuloma, enchondroma, and bone cyst, with no reports in the literature to our knowledge of these entities presenting in the hallux MTPJ sesamoid. In contrast, gout typically begins with normal radiographic findings, and later leads to erosive, “punched out” lesions on either side of the MTPJ.2
Hyperuricemia is an essential part of the pathophysiology of gout, but not all patients with an acute gouty attack have elevated uric acid levels and, in contrast, may actually have normal or low levels in 12% to 43% of cases.8 The most accurate time frame for assessment of serum uric acid levels is 2 weeks or more after subsidence of an acute event.8 The normal uric acid levels seen in our patient were most likely due to the fact that the workup was undertaken during an acute attack. The difficulty with establishing the diagnosis was compounded by bilateral involvement, history of trauma, negative joint aspiration, and atypical radiographic findings. A number of reports have described patients with tophus deposits prior to or in the absence of gouty arthritis or a gouty attack.10 Risk factors for this presentation include female sex, the predominant or exclusive involvement of fingers, chronic kidney disease, and treatment with a diuretic or anti-inflammatory drug.10
Conclusion
Our case report illustrates the difficulty in diagnosing an acute gouty attack in a patient with a history of trauma and atypical radiographic findings. The hallux MTPJ is the most common location of acute gouty attacks, but the medial sesamoid as an isolated location is a rare site of presentation. The combination of pain isolated to palpation of the sesamoid and radiographs that showed an aggressive and rapidly expansile lesion of the medial sesamoid raised concerns about a neoplastic lesion. Practitioners should consider acute gout in patients with sesamoid pain and with radiographs showing an expansile sesamoid lesion.
1. Mair SD, Coogan AC, Speer KP, Hall RL. Gout as a source of sesamoid pain. Foot Ankle Int. 1995;16(10):613-616.
2. Reber PU, Patel AG, Noesberger B. Gout: rare cause of hallucal sesamoid pain: a case report. Foot Ankle Int. 1997;12(18):818-820.
3. Van Hal ME, Kenne JS, Lange TA, Clancy WG Jr. Stress fractures of the great toe sesamoids. Am J Sports Med. 1982;10(2):122-128.
4. Liu S-Z, Yeh L, Chou Y, Chen CK, Pan HB. Isolated intraosseous gout in hallux sesamoid mimicking a bone tumor in a teenaged patient. Skeletal Radiol. 2003;32(11):647-650.
5. Cohen BE. Hallux sesamoid disorders. Foot Ankle Clin. 2009;14(1):91-104.
6. Harty JA, Kelly P, Niall D, O’Keane JC, Stephens MM. Bizarre parosteal osteochondromatous proliferation (Nora’s lesion) of the sesamoid: a case report. Foot Ankle Int. 2000;21(5):408-412.
7. Noguchi M, Ikoma K, Matsumoto N, Nagasawa K. Bizarre parosteal osteochondromatous proliferation of the sesamoid: an unusual hallux valgus deformity. Foot Ankle Int. 2004;25(7):503-506.
8. Becker MA. Clinical manifestations and diagnosis of gout. Up to Date website. http://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-gout. Updated June 20, 2015. Accessed August 19, 2015.
9. Bos GD, Esther RJ, Woll TS. Foot tumors: diagnosis and treatment. J Am Acad Orthop Surg. 2002;10(4):259-270.
10. Wernick R, Winkler C, Campbell S. Tophi as the initial manifestation of gout. Report of six cases and review of the literature. Arch Intern Med. 1992;152(4):873-876.
The sesamoid bones are a major contributor to normal gait, with more than 50% of body weight transmitted through the hallux metatarsophalangeal joint (MTPJ) complex. There are varying amounts of stress on the sesamoids, dependent on the gait cycle.1,2 The sesamoids act as a fulcrum to increase the mechanical force of the flexor hallucis brevis tendon.3 Sesamoid pathology can be a source of significant morbidity in patients, especially young athletes or laborers who spend long hours on their feet. More common causes of isolated sesamoid discomfort include sesamoiditis, fracture, and avascular necrosis, with neoplastic, infectious, and inflammatory conditions rarely isolated to the sesamoid.
Gout is a systemic disorder of uric acid metabolism characterized by deposition of monosodium urate crystals in soft tissues and joints.1 This deposition leads to tophus formation with an accompanying inflammatory response. Gout progresses through 3 stages, beginning with acute gout, which may end with chronic, recurrent, and tophaceous gouty arthritis. The hallux MTPJ is the most common joint affected by gout, with few case reports of primary sesamoid gout.1-2,4 We present a case of gout, with radiographic findings isolated to the medial sesamoid, that mimicked a neoplastic process in a patient with no known history of gout. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 37-year-old laborer presented for evaluation of a right sesamoid injury he sustained 4 months earlier when he fell off a ladder and had acute onset plantar hallux MTPJ pain and swelling. He was treated by an outside physician for a presumptive diagnosis of a medial sesamoid fracture with rest and controlled ankle movement (CAM) boot immobilization that resulted in slowly improving symptoms. In discussion of the patient’s history, he reported that 1 year earlier he had a traumatic event with similar symptoms of MTPJ pain and swelling. At that time, treatment with a CAM boot resulted in complete resolution of pain. His outside physician performed a hematologic workup for gout, which showed a normal uric acid level.
On examination, the patient presented with edema to the right hallux MTPJ and mild tenderness to palpation of the medial sesamoid. He had no pain with motion of the hallux MTPJ or with palpation of the lateral sesamoid. His radiographs showed a bipartite versus fractured sesamoid (Figures 1A, 1B) and serial magnetic resonance imaging (MRI) showed an MTPJ effusion and hyperintense signal in the medial sesamoid, but no erosive findings or soft-tissue masses (Figures 2A, 2B).
The patient was treated with wedge-sandal forefoot offloading, leading to resolution of symptoms over 6 weeks, at which point he was transitioned to normal shoe wear and allowed to progress in his activity as dictated by his symptoms. He presented for reevaluation approximately 2 weeks later with acute, atraumatic onset of plantar left hallux pain and swelling. His examination showed diffuse hallux MTPJ swelling and tenderness isolated to the medial sesamoid. An attempt at aspiration of the MTPJ yielded no fluid, and the patient again was placed in a forefoot-offloading sandal.
Radiographs of the left foot showed an expansile destructive lesion of the medial sesamoid with interval change from his previous imaging approximately 3 months earlier, obtained as part of his contralateral foot evaluation (Figure 3). MRI with and without contrast showed an expansile process isolated to the medial sesamoid with cortical thinning and marrow replacement (Figures 4A-4D).
Because of continued discomfort and lack of a definitive diagnosis, an excisional biopsy of the sesamoid was performed. Intraoperatively, the sesamoid was extensively fragmented with near complete replacement by a chalky tophus, as well as chalky deposition throughout the hallux MTPJ. No significant degenerative changes were observed. Surgical pathology showed bone and fibroconnective tissue with deposits of negative birefringement needle-shaped crystals consistent with monosodium urate deposition and foreign body histocytic reaction, as well as repair reaction of bone (Figures 5A, 5B).
Postoperatively, the patient was again placed in a forefoot-offloading wedge sandal for 6 weeks, followed by progression of activity as dictated by his symptoms. He was also evaluated by a rheumatologist and started on medical treatment for gout, with complete resolution of his bilateral hallux pain. He has been able to return to his previous employment.
Discussion
The sesamoid bones are an important component of the hallux MTPJ complex, giving a mechanical advantage to the flexor hallucis brevis tendons in plantar flexion of the hallux.5 Many pathologic conditions have been well described in the literature, including fracture, sesamoiditis, nonunion, avascular necrosis, and plantar keratosis. There is also a 10% incidence of bipartite sesamoids, most commonly isolated to the medial sesamoid, with up to 25% of patients presenting with bilateral bipartite sesamoids.5 Neoplastic processes of the sesamoid are rare, with a paucity of reports in the literature.6,7 Gout is a condition in which hyperuricemia, due to an imbalance in uric acid production and excretion, leads to deposition of monosodium urate crystals in joints, bones, and soft tissues, causing an inflammatory reaction. Risk factors for gout are male sex, advanced age, and ethnicity, as well as obesity, high protein diet, alcohol use, hypertension, and certain medications. Precipitation of acute attacks has been associated with acute trauma, and the first MTPJ is the most common location for an acute attack.8
Isolated sesamoid lesions are rare, with few isolated case reports in the literature. Benign and malignant lesions appear most often in the metatarsals, with the calcaneus being the second most commonly afflicted site.9 The typical differential diagnosis for isolated lytic bone lesions includes fibrous dysplasia, osteoblastoma, giant cell tumor, metastatic lesion, multiple myeloma, aneurysmal bone cyst, chondroblastoma, brown tumor, infection, eosinophilic granuloma, enchondroma, and bone cyst, with no reports in the literature to our knowledge of these entities presenting in the hallux MTPJ sesamoid. In contrast, gout typically begins with normal radiographic findings, and later leads to erosive, “punched out” lesions on either side of the MTPJ.2
Hyperuricemia is an essential part of the pathophysiology of gout, but not all patients with an acute gouty attack have elevated uric acid levels and, in contrast, may actually have normal or low levels in 12% to 43% of cases.8 The most accurate time frame for assessment of serum uric acid levels is 2 weeks or more after subsidence of an acute event.8 The normal uric acid levels seen in our patient were most likely due to the fact that the workup was undertaken during an acute attack. The difficulty with establishing the diagnosis was compounded by bilateral involvement, history of trauma, negative joint aspiration, and atypical radiographic findings. A number of reports have described patients with tophus deposits prior to or in the absence of gouty arthritis or a gouty attack.10 Risk factors for this presentation include female sex, the predominant or exclusive involvement of fingers, chronic kidney disease, and treatment with a diuretic or anti-inflammatory drug.10
Conclusion
Our case report illustrates the difficulty in diagnosing an acute gouty attack in a patient with a history of trauma and atypical radiographic findings. The hallux MTPJ is the most common location of acute gouty attacks, but the medial sesamoid as an isolated location is a rare site of presentation. The combination of pain isolated to palpation of the sesamoid and radiographs that showed an aggressive and rapidly expansile lesion of the medial sesamoid raised concerns about a neoplastic lesion. Practitioners should consider acute gout in patients with sesamoid pain and with radiographs showing an expansile sesamoid lesion.
The sesamoid bones are a major contributor to normal gait, with more than 50% of body weight transmitted through the hallux metatarsophalangeal joint (MTPJ) complex. There are varying amounts of stress on the sesamoids, dependent on the gait cycle.1,2 The sesamoids act as a fulcrum to increase the mechanical force of the flexor hallucis brevis tendon.3 Sesamoid pathology can be a source of significant morbidity in patients, especially young athletes or laborers who spend long hours on their feet. More common causes of isolated sesamoid discomfort include sesamoiditis, fracture, and avascular necrosis, with neoplastic, infectious, and inflammatory conditions rarely isolated to the sesamoid.
Gout is a systemic disorder of uric acid metabolism characterized by deposition of monosodium urate crystals in soft tissues and joints.1 This deposition leads to tophus formation with an accompanying inflammatory response. Gout progresses through 3 stages, beginning with acute gout, which may end with chronic, recurrent, and tophaceous gouty arthritis. The hallux MTPJ is the most common joint affected by gout, with few case reports of primary sesamoid gout.1-2,4 We present a case of gout, with radiographic findings isolated to the medial sesamoid, that mimicked a neoplastic process in a patient with no known history of gout. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 37-year-old laborer presented for evaluation of a right sesamoid injury he sustained 4 months earlier when he fell off a ladder and had acute onset plantar hallux MTPJ pain and swelling. He was treated by an outside physician for a presumptive diagnosis of a medial sesamoid fracture with rest and controlled ankle movement (CAM) boot immobilization that resulted in slowly improving symptoms. In discussion of the patient’s history, he reported that 1 year earlier he had a traumatic event with similar symptoms of MTPJ pain and swelling. At that time, treatment with a CAM boot resulted in complete resolution of pain. His outside physician performed a hematologic workup for gout, which showed a normal uric acid level.
On examination, the patient presented with edema to the right hallux MTPJ and mild tenderness to palpation of the medial sesamoid. He had no pain with motion of the hallux MTPJ or with palpation of the lateral sesamoid. His radiographs showed a bipartite versus fractured sesamoid (Figures 1A, 1B) and serial magnetic resonance imaging (MRI) showed an MTPJ effusion and hyperintense signal in the medial sesamoid, but no erosive findings or soft-tissue masses (Figures 2A, 2B).
The patient was treated with wedge-sandal forefoot offloading, leading to resolution of symptoms over 6 weeks, at which point he was transitioned to normal shoe wear and allowed to progress in his activity as dictated by his symptoms. He presented for reevaluation approximately 2 weeks later with acute, atraumatic onset of plantar left hallux pain and swelling. His examination showed diffuse hallux MTPJ swelling and tenderness isolated to the medial sesamoid. An attempt at aspiration of the MTPJ yielded no fluid, and the patient again was placed in a forefoot-offloading sandal.
Radiographs of the left foot showed an expansile destructive lesion of the medial sesamoid with interval change from his previous imaging approximately 3 months earlier, obtained as part of his contralateral foot evaluation (Figure 3). MRI with and without contrast showed an expansile process isolated to the medial sesamoid with cortical thinning and marrow replacement (Figures 4A-4D).
Because of continued discomfort and lack of a definitive diagnosis, an excisional biopsy of the sesamoid was performed. Intraoperatively, the sesamoid was extensively fragmented with near complete replacement by a chalky tophus, as well as chalky deposition throughout the hallux MTPJ. No significant degenerative changes were observed. Surgical pathology showed bone and fibroconnective tissue with deposits of negative birefringement needle-shaped crystals consistent with monosodium urate deposition and foreign body histocytic reaction, as well as repair reaction of bone (Figures 5A, 5B).
Postoperatively, the patient was again placed in a forefoot-offloading wedge sandal for 6 weeks, followed by progression of activity as dictated by his symptoms. He was also evaluated by a rheumatologist and started on medical treatment for gout, with complete resolution of his bilateral hallux pain. He has been able to return to his previous employment.
Discussion
The sesamoid bones are an important component of the hallux MTPJ complex, giving a mechanical advantage to the flexor hallucis brevis tendons in plantar flexion of the hallux.5 Many pathologic conditions have been well described in the literature, including fracture, sesamoiditis, nonunion, avascular necrosis, and plantar keratosis. There is also a 10% incidence of bipartite sesamoids, most commonly isolated to the medial sesamoid, with up to 25% of patients presenting with bilateral bipartite sesamoids.5 Neoplastic processes of the sesamoid are rare, with a paucity of reports in the literature.6,7 Gout is a condition in which hyperuricemia, due to an imbalance in uric acid production and excretion, leads to deposition of monosodium urate crystals in joints, bones, and soft tissues, causing an inflammatory reaction. Risk factors for gout are male sex, advanced age, and ethnicity, as well as obesity, high protein diet, alcohol use, hypertension, and certain medications. Precipitation of acute attacks has been associated with acute trauma, and the first MTPJ is the most common location for an acute attack.8
Isolated sesamoid lesions are rare, with few isolated case reports in the literature. Benign and malignant lesions appear most often in the metatarsals, with the calcaneus being the second most commonly afflicted site.9 The typical differential diagnosis for isolated lytic bone lesions includes fibrous dysplasia, osteoblastoma, giant cell tumor, metastatic lesion, multiple myeloma, aneurysmal bone cyst, chondroblastoma, brown tumor, infection, eosinophilic granuloma, enchondroma, and bone cyst, with no reports in the literature to our knowledge of these entities presenting in the hallux MTPJ sesamoid. In contrast, gout typically begins with normal radiographic findings, and later leads to erosive, “punched out” lesions on either side of the MTPJ.2
Hyperuricemia is an essential part of the pathophysiology of gout, but not all patients with an acute gouty attack have elevated uric acid levels and, in contrast, may actually have normal or low levels in 12% to 43% of cases.8 The most accurate time frame for assessment of serum uric acid levels is 2 weeks or more after subsidence of an acute event.8 The normal uric acid levels seen in our patient were most likely due to the fact that the workup was undertaken during an acute attack. The difficulty with establishing the diagnosis was compounded by bilateral involvement, history of trauma, negative joint aspiration, and atypical radiographic findings. A number of reports have described patients with tophus deposits prior to or in the absence of gouty arthritis or a gouty attack.10 Risk factors for this presentation include female sex, the predominant or exclusive involvement of fingers, chronic kidney disease, and treatment with a diuretic or anti-inflammatory drug.10
Conclusion
Our case report illustrates the difficulty in diagnosing an acute gouty attack in a patient with a history of trauma and atypical radiographic findings. The hallux MTPJ is the most common location of acute gouty attacks, but the medial sesamoid as an isolated location is a rare site of presentation. The combination of pain isolated to palpation of the sesamoid and radiographs that showed an aggressive and rapidly expansile lesion of the medial sesamoid raised concerns about a neoplastic lesion. Practitioners should consider acute gout in patients with sesamoid pain and with radiographs showing an expansile sesamoid lesion.
1. Mair SD, Coogan AC, Speer KP, Hall RL. Gout as a source of sesamoid pain. Foot Ankle Int. 1995;16(10):613-616.
2. Reber PU, Patel AG, Noesberger B. Gout: rare cause of hallucal sesamoid pain: a case report. Foot Ankle Int. 1997;12(18):818-820.
3. Van Hal ME, Kenne JS, Lange TA, Clancy WG Jr. Stress fractures of the great toe sesamoids. Am J Sports Med. 1982;10(2):122-128.
4. Liu S-Z, Yeh L, Chou Y, Chen CK, Pan HB. Isolated intraosseous gout in hallux sesamoid mimicking a bone tumor in a teenaged patient. Skeletal Radiol. 2003;32(11):647-650.
5. Cohen BE. Hallux sesamoid disorders. Foot Ankle Clin. 2009;14(1):91-104.
6. Harty JA, Kelly P, Niall D, O’Keane JC, Stephens MM. Bizarre parosteal osteochondromatous proliferation (Nora’s lesion) of the sesamoid: a case report. Foot Ankle Int. 2000;21(5):408-412.
7. Noguchi M, Ikoma K, Matsumoto N, Nagasawa K. Bizarre parosteal osteochondromatous proliferation of the sesamoid: an unusual hallux valgus deformity. Foot Ankle Int. 2004;25(7):503-506.
8. Becker MA. Clinical manifestations and diagnosis of gout. Up to Date website. http://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-gout. Updated June 20, 2015. Accessed August 19, 2015.
9. Bos GD, Esther RJ, Woll TS. Foot tumors: diagnosis and treatment. J Am Acad Orthop Surg. 2002;10(4):259-270.
10. Wernick R, Winkler C, Campbell S. Tophi as the initial manifestation of gout. Report of six cases and review of the literature. Arch Intern Med. 1992;152(4):873-876.
1. Mair SD, Coogan AC, Speer KP, Hall RL. Gout as a source of sesamoid pain. Foot Ankle Int. 1995;16(10):613-616.
2. Reber PU, Patel AG, Noesberger B. Gout: rare cause of hallucal sesamoid pain: a case report. Foot Ankle Int. 1997;12(18):818-820.
3. Van Hal ME, Kenne JS, Lange TA, Clancy WG Jr. Stress fractures of the great toe sesamoids. Am J Sports Med. 1982;10(2):122-128.
4. Liu S-Z, Yeh L, Chou Y, Chen CK, Pan HB. Isolated intraosseous gout in hallux sesamoid mimicking a bone tumor in a teenaged patient. Skeletal Radiol. 2003;32(11):647-650.
5. Cohen BE. Hallux sesamoid disorders. Foot Ankle Clin. 2009;14(1):91-104.
6. Harty JA, Kelly P, Niall D, O’Keane JC, Stephens MM. Bizarre parosteal osteochondromatous proliferation (Nora’s lesion) of the sesamoid: a case report. Foot Ankle Int. 2000;21(5):408-412.
7. Noguchi M, Ikoma K, Matsumoto N, Nagasawa K. Bizarre parosteal osteochondromatous proliferation of the sesamoid: an unusual hallux valgus deformity. Foot Ankle Int. 2004;25(7):503-506.
8. Becker MA. Clinical manifestations and diagnosis of gout. Up to Date website. http://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-gout. Updated June 20, 2015. Accessed August 19, 2015.
9. Bos GD, Esther RJ, Woll TS. Foot tumors: diagnosis and treatment. J Am Acad Orthop Surg. 2002;10(4):259-270.
10. Wernick R, Winkler C, Campbell S. Tophi as the initial manifestation of gout. Report of six cases and review of the literature. Arch Intern Med. 1992;152(4):873-876.