User login
Mr. R., 37, started gambling during college. He often bet on sporting events with friends. The gambling was sporadic and apparently did not cause any problems in his life.
Over the next 3 or 4 years, he started visiting the local casino every couple of months with friends and playing blackjack. He occasionally won, but even if he lost he was able to return home without being preoccupied by the experience.
During the past year the frequency with which he gambled had increased. Prior to treatment, he was going to the casino 2 or 3 nights per week. Although he intended to gamble only for a few hours and spend no more than $100 each visit, Mr. R. usually spent most of the evening at the casino and squandered $500 to $1,000 per night. Mr. R. reported daily—and severe—urges to gamble. He would often see a billboard for the casino while driving home from his job as an accountant. The advertisement triggered his urges; instead of going home, he would drive to the casino.
While at work, Mr. R. spent so much time thinking of ways to win at gambling—which tables to play, how to lay the bets, which “lucky” shirt to wear—that he could not complete his assignments in a timely manner. He found it difficult to stay at work, even when he had meetings. Instead, when he felt urges to gamble, he would leave early.
Mr. R. felt ashamed of his gambling and kept it a secret from his wife. If unable to gamble when he had urges, he felt anxious and irritable. Because of his gambling, he missed family functions and lied to his wife and family.
Although married for only 3 years, his wife had already talked about divorce. Mr. R. had significant credit card debt and had to file for bankruptcy. Only then did he tell his wife about his gambling problem.
After telling his primary physician he was depressed, Mr. R. was treated with citalopram 20mg/d. The medication helped his mood but did not decrease his urges to gamble or alter his gambling behavior.
When he presented to our clinic, Mr. R. was off medication and still gambling 2 or 3 times per week. He was then treated with naltrexone 25mg/d for 2 days, then 50mg/d. Because of a possible drug-drug interaction with naltrexone, he agreed to stop taking over-the-counter nonsteroidal analgesics. After 2 weeks, the dosage was increased to 100mg/d taken in the morning with food. Mr. R. reported that his urges to gamble, although still present, were significantly reduced.
After another 2 weeks, the dosage was increased to 150mg/d. Mr. R. reported that his urges to gamble were gone. Without the urges, he was able to stop gambling. Liver function tests were performed every 2 weeks for the first 2 months of treatment and every month thereafter for 3 months.
This case illustrates many of the clinical features of pathological gambling, defined by persistent and recurrent maladaptive patterns of gambling behavior. The disorder often goes undiagnosed and untreated, though preliminary data suggest that it may be relatively common. The lifetime prevalence of pathological gambling is 1.6% among adults, and 3.9% among those younger than 18.1 Pathological gamblers usually experience painful financial losses and perhaps as a consequence have high rates of bankruptcy, divorce, and criminal behavior.2 They also often suffer from comorbid mood, anxiety, and alcohol use disorders.3 In fact, the suicide rate in cities with established, legal casinos is 2 to 4 times higher than in cities without.4
How to identify the pathological gambler
Pathological gambling is often a secret disorder. If left untreated, it frequently becomes a chronic condition. To make the diagnosis, use the simple screening instrument shown in (Table 1).5 The patient is likely to be suffering from pathological gambling disorder if he or she answered five or more of the questions “yes.” The last two questions are useful when trying to determine if someone has a gambling problem that is not readily apparent. Some people gamble in binges—for example, they may only gamble when they have available funds. These people may, however, be significantly impaired by the cravings or urges to gamble even though they may not have gambled for weeks.
Data suggest that the male-to-female ratio in pathological gambling is approximately 2:1. Gambling usually begins in early adulthood, with males tending to start at an earlier age. Although many pathological gamblers take several years to develop a problem, almost one-half report feeling “addicted” within a year after starting to gamble.2 Females appear to develop pathological gambling disorder in a shorter time.
Most pathological gamblers are fairly specific about their choice of gambling activity. Women tend to play slot machines and bingo, whereas men choose sporting events, blackjack, and cards. Both cite advertisements as a common trigger of their urges to gamble, although females are more likely to report that feeling bored or lonely may also trigger these urges.
Despite their preoccupation with gambling, many pathological gamblers function quite well, although often below their capacity. But others are severely debilitated—unable to function socially or occupationally.
In a series of 131 patients with pathological gambling disorder, 44% had lost all their savings, 24% had filed for bankruptcy, 23% had lost their homes or cars, and 15% had significant marital problems because of their gambling.2 Financial concerns may become so distressing that many pathological gamblers engage in illegal behavior, such as stealing, embezzlement, and writing bad checks.2
Table 1
Questions that can help diagnose pathological gambling
| Yes | No | Questions | |
|---|---|---|---|
| ○ | ○ | 1. Are you preoccupied with previous or future gambling experiences? That is, do you think about them a lot and wish you could think about them less? | |
| ○ | ○ | 2. Have you been unable to stop gambling or decrease the amount you gamble? | |
| ○ | ○ | 3. When you tried to stop or cut down, did you feel more irritable or anxious? | |
| ○ | ○ | 4. Has the amount you gamble increased to get the same sort of “high” or excitement? | |
| ○ | ○ | 5. Do you gamble as a way of escaping feelings of depression? | |
| ○ | ○ | 6. After you lose, do you go back in the next couple of days to try and win back the money? | |
| What effect has your gambling had on your life? | |||
| ○ | ○ | 7. Have you lied to others about your gambling? | |
| ○ | ○ | 8. Have you committed illegal acts as a result of gambling or lack of money? | |
| ○ | ○ | 9. Has gambling significantly interfered with school, job, or relationships? | |
| ○ | ○ | 10. Have you needed to borrow money because of gambling? | |
| ○ | ○ | 11. When you aren’t gambling, do you have urges to gamble? | |
| ○ | ○ | 12. If you have urges to gamble, do they preoccupy you or interfere with school, job, or relationships? | |
| adapted from DSM-IV criteria5 | |||
Table 2 Medical options for pathological gambling
Treatment response findings appear promising
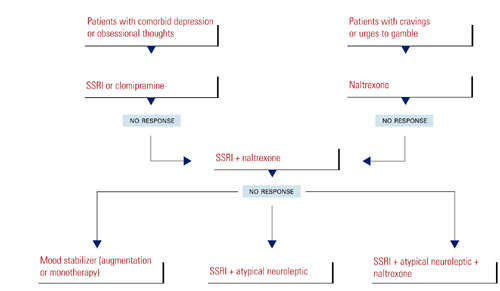
Only a few controlled treatment studies of pathological gambling have been done, but the findings on the response to treatment appear promising. Thus far, the uses of serotonin reuptake inhibitors (SRIs), either clomipramine or selective serotonin reuptake inhibitors (SSRIs), the opioid antagonist naltrexone, mood stabilizers, and atypical neuroleptics have met with varying degrees of success. Additional strategies targeting urge and behavior reduction and mechanisms for coping with urges and behavior (e.g., cognitive behavioral therapies) may represent important adjunctive components.6
Because no medication is currently approved by the Food and Drug Administration (FDA) for treating pathological gambling, it is important to inform your patients of any “off-label” use of medications for this disorder, as well as the empirical basis for considering the medication.
The role of SRIs Response to SRIs usually means decreased thoughts about gambling, decreased gambling behavior, and improved social and occupational functioning. Patients may initially report feeling both less preoccupied with gambling and less anxious about having thoughts of gambling. For people who gamble because they are depressed and trying to escape loneliness or depressed feelings, SRIs are a reasonable first-line medication (Table 2).
As in the treatment of obsessive-compulsive disorder (OCD), dosages of SRIs required to treat pathological gambling symptoms appear to be higher than the average dosages required to treat depressive disorders. Some studies suggest that a significant initial response may be largely placebo. This means that improvement should be monitored for several months and that patients and clinicians need to be cautious about early improvement. An SRI should not be considered ineffective unless it has been tried for at least 10 to 12 weeks and the highest dose tolerated or recommended by the manufacturer has been reached.
The following SRIs have been used with varying degrees of success:
- Clomipramine has been shown effective in reducing gambling behavior with dosages between 125mg/d to 175mg/d.7
- Fluvoxamine has demonstrated mixed results in 3 studies of pathological gambling. Two studies supported its efficacy at an average dosage of 195mg/d to 207mg/d,8-9 but a third found that time spent gambling did not decrease when subjects took 200mg/d.10
- Citalopram has also shown some benefit as a possible treatment option in a single study.11
- Paroxetine, at dosages between 20mg/d and 60mg/d, was found to decrease thoughts of gambling and gambling behavior after approximately 6 to 8 weeks of treatment.12
- Fluoxetine (20mg/d) plus monthly supportive psychotherapy was found to improve gambling symptoms more than did supportive therapy alone.13
When naltrexone is indicated Naltrexone appears to be a reasonable first-line agent for patients who report intense urges to gamble (Table 2). Many patients who report “obsessions” with gambling may suffer from uncontrollable urges that interfere with daily functioning. By eliminating or reducing the urges, the preoccupation often disappears. Patients taking naltrexone often report less-intense urges. The urges may not go away completely; instead, they are often reduced enough for the patient to resist them more easily. Patients also report enjoying the gambling experience less when taking naltrexone; the “high” associated with gambling is reduced.
Naltrexone has been tested in psychiatric conditions in which urges are a dominant symptom.14 The greatest amount of evidence supports the agent’s use in treating alcohol dependence (see related article on page 55) and opiate dependence, both of which are FDA-approved indications.
In the case of pathological gambling, a small body of literature suggests that naltrexone is effective. One case report describes a patient suffering from both pathological gambling and alcohol dependence who responded to naltrexone 50mg/d.15 The first study using naltrexone in pathological gambling showed a significant decline in the intensity of urges to gamble, gambling thoughts, and gambling behavior when using 157 mg/d on average.16 This was followed by a larger study in which an average naltrexone dosage of 188mg/d resulted in improvement in gambling urges, thoughts, and behavior.14
Clinically, a patient will usually respond to a particular dose of naltrexone within 2 weeks. After that, an adjustment in dose is usually necessary. Patients often report nausea and diarrhea. Dizziness, sedation, and headaches occur less commonly. The side effects are usually mild and go away within the first week. Nausea, however, may be moderate to severe in some patients, so patients should be started on 25mg/d for the first 3 or 4 days to reduce that possibility. Ondansetron 4 mg/d is often given adjunctively for the same period to prevent the nausea.
Given the risk of associated hepatic transaminase elevations, liver function tests should be monitored in all patients taking naltrexone.14,16 A boxed warning refers to the potential hepatotoxicity of naltrexone at 50 mg/d, the dosage recommended for treating alcohol or opioid dependence. The warning also states that naltrexone use is contraindicated in acute hepatitis or liver failure, and its use in individuals with active liver disease must be carefully considered.
Initial liver function tests should be evaluated prior to naltrexone administration and again 3 to 4 weeks after starting the drug. Repeat testing should be performed at 2- to 4-week intervals for the next 2 months, a potential high-risk period. Thereafter, tests should be done approximately once a month for the following 3 months. After 6 months, liver enzyme elevations appear to occur rarely and testing 3 to 4 times a year should suffice unless an undue risk arises, e.g., excessive alcohol consumption. If elevated, the enzymes return to normal levels after discontinuing the naltrexone.
Research in this area is still in an early stage and clinicians prescribing the drug for pathological gambling should take extra caution in administering naltrexone at high doses and monitor for potential adverse consequences. Nonsteroidal analgesics should not be used in conjunction with high-dose naltrexone,14 as their concurrent use seems to cause a higher risk of hepatic transaminase elevation.
Mood stabilizers Successful responses to lithium and carbamazepine were described in 2 early case reports. Three subjects who were treated with lithium 1,800mg/d reported cessation of gambling.17 An early case report also found that carbamazepine resulted in improvement in pathological gambling disorder.18 Preliminary studies of lithium and valproate further support the notion that mood stabilizers may be useful. The benefit from carbamazepine, lithium, and valproate may be attributed to their efficacy in treating bipolar disorder and to the existence of features shared by pathological gambling and bipolar disorder (e.g., impulsivity).
Atypical antipsychotics Although there is little evidence that atypical antipsychotics work against pathological gambling when used alone, clinically atypical neuroleptic augmentation of SSRIs may be beneficial.
Atypical antipsychotics have been explored as augmenting agents in the treatment of nonpsychotic disorders and behaviors, including OCD. A recent trial of olanzapine in the treatment of pathological video poker gamblers showed no difference in outcomes between the patients on medication and those on placebo.19
Cognitive behavioral therapy There is also mounting evidence that cognitive behavioral treatments are effective for pathological gambling.6,20-21 Combined pharmacological and behavioral therapy is considered the optimal treatment strategy for many psychiatric disorders, including substance dependence.
In our clinical experience, patients who only partially respond or fail to respond to pharmacotherapy alone are more likely to find relief with a combination of drug and cognitive behavioral therapies. Future studies should explore directly how pharmacological and behavioral therapy contribute to clinical improvement as part of combination treatment strategies for pathological gambling.
Ways to enhance compliance
Pathological gamblers, like those with bipolar disorder or substance dependence, often fail to comply with treatment.
Patients suffering from mania may not adhere to treatment with mood stabilizers in part because drug treatment may reduce positive or euphoric experiences. Similarly, the “high” associated with drug use often makes patients ambivalent about taking medications to remain abstinent.
In treating opioid dependence with naltrexone, a reward system has been incorporated in a contingency management fashion to substitute for drug-related reward and to enhance compliance with the medication.22 Recruitment of friends or family has also been used to enhance compliance with naltrexone in treating opioid dependence.22
In the case of pathological gamblers, a self-rewarding system for each day of nongambling can be used (e.g., a favorite meal or a movie).6 Family members can help by increasing social or other activities that can take the patient’s mind off gambling, particularly at high-risk times (weekends and payday).6
How long should you treat?
No guidelines exist for recommended adequate treatment trials for pathological gambling. Available data, however, suggest that an adequate medication trial may require a relatively long duration (4 months or longer).
Many pathological gamblers have never discussed their difficulties, and this unquantifiable therapeutic response may resemble a medication response. Clinicians must monitor symptoms long enough to assess the difference between response to placebo and to medication.
The optimal duration of treatment and rates of relapse associated with discontinuation are not known. Many patients relapse upon discontinuation of medication, and long-term treatment, perhaps 2 to 3 years, may be warranted.
Treatment-resistant pathological gambling
It is not unusual to encounter patients who have had no response or only a partial response to treatment. Several approaches appear promising (Table 2):
- If a patient has had an adequate trial of either an SRI or naltrexone as monotherapy, adding another agent appears to result in additional clinical improvement.
- A patient who has failed to respond to either an SRI or naltrexone may be effectively treated with a mood stabilizer, either as monotherapy or as augmentation. Some patients with pathological gambling disorder, although not screening positive for a manic episode, exhibit symptoms consistent with cyclothymia or other subclinical cycling mood disorder. For such patients lithium, valproate, or another drug with putative mood stabilizing properties may represent an appropriate option.
- The possibility of adding atypical antipsychotics to SRIs in the SRI-refractory pathological gambler warrants consideration.
- Patients who only partially respond or fail to respond to medication alone are more likely to find relief with a combination of drug and cognitive-behavioral therapies, since this is considered the optimal treatment strategy for many psychiatric disorders.
Related resources
- Gamblers Anonymous International Service Office. Los Angeles, Calif. http://www.gamblersanonymous.org.
- National Research Council. Pathological Gambling: A Critical Review. Washington, DC: National Academy Press, 1990.
- James K. National Gambling Impact Study Commission: Final Report to Congress 1999. http://www.ngisc.gov/reports/finrpt.html
Drug brand names
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clomipramine • Anafranil
- Fluoxetine• Prozac, Prozac Weekly
- Fluvoxamine • Luvox
- Naltrexone • ReVia
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Valproic acid •Depakote
Disclosure
The authors report no affiliation or financial arrangement with any of the companies whose products are mentioned in this article.
1. Shaffer HJ, Hall MN, Vander Bilt J. Estimating the prevalence of disordered gambling behavior in the United States and Canada: a research synthesis. Am J Public Health. 1999;89(9):1369-1376.
2. Grant JE, Kim SW. Demographic and clinical features of 131 adult pathological gamblers. J Clin Psychiatry. 2001;62(12):957-962.
3. Black DW, Moyer TM. Clinical features and psychiatric comorbidity of subjects with pathological gambling behavior. Psychiatric Serv. 1998;49(11):1434-1439.
4. Phillips DP, Welty WR, Smith MM. Elevated suicide levels associated with legalized gambling. Suicide Life Threat Behav. 1997;27(4):373-378.
5. American Psychiatric Association Committee on Nomenclature and Statistics. Diagnostic and Statistical Manual of Mental Disorders. 4th ed., text revision. Washington, DC: American Psychiatric Association, 2000.
6. Petry NM, Roll JM. A behavioral approach to understanding and treating pathological gambling. Semin Clin Neuropsychiatry. 2001;6(3):177-183.
7. Hollander E, Frenkel M, DeCaria C, et al. Treatment of pathological gambling with clomipramine. Am J Psychiatry. 1992;149(5):710-711.
8. Hollander E, DeCaria CM, Mari E, et al. Short-term single-blind fluvoxamine treatment of pathological gambling. Am J Psychiatry. 1998;155(12):1781-1783.
9. Hollander E, DeCaria CM, et al. A randomized double-blind fluvoxamine/placebo crossover trial in pathological gambling. Biol Psychiatry. 2000;47(9):813-817.
10. Blanco-Jerez C. A long-term, double-blind, placebo-controlled study of fluvoxamine for pathological gambling. Presented at the 152nd Annual Meeting of the American Psychiatric Association, Washington, DC, May 16-21, 1999 [abstract].
11. Zimmerman M, Breen R. An open-label study of citalopram in the treatment of pathological gambling. Presented at the 11th International Conference on Gambling and Risk Taking, Las Vegas, Nev, June 17-21, 2000 [abstract].
12. Kim SW, Grant JE, Shin YC, Toth JA, et al. A double-blind, placebo-controlled study of the efficacy and safety of paroxetine in the treatment of pathological gambling disorder. J Clin Psychiatry. 2002 (in press).
13. De la Gandara JJ. Fluoxetine: open-trial in pathological gambling. Presented at the 152 Annual Meeting of the American Psychiatric Association, Washington, DC, May 16-21, 1999 [abstract].
14. Kim SW, Grant JE, et al. Double-blind naltrexone and placebo comparison study in the treatment of pathological gambling. Biol Psychiatry. 2001;49(11):914-921.
15. Crockford DN, el-Guebaly N. Naltrexone in the treatment of pathological gambling and alcohol dependence. Can J Psychiatry. 1998;43(1):86.-
16. Kim SW, Grant JE. An open naltrexone treatment study of pathological gambling disorder. Int Clin Psychopharmacol. 2001;16(5):285-289.
17. Moskowitz JA. Lithium and lady luck: use of lithium carbonate in compulsive gambling. NY State J Med. 1980;80(5):785-788.
18. Haller R, Hinterhuber H. Treatment of pathological gambling with carbamazepine. Pharmacopsychiatry. 1994;27:129.-
19. Rugle L. The use of olanzapine in the treatment of video poker pathological gamblers. Presented at the conference titled, “The Comorbidity of Pathological Gambling: A Current Research Synthesis,” Dec 3 5, 2000, Las Vegas, Nev [abstract].
20. Ladoceur R, Sylvain C, Boutin C, et al. Cognitive treatment of pathological gambling. J Nerv Ment Dis. 2001;189(11):774-780.
21. Sylvain C, Ladouceur R, Boisvert JM. Cognitive and behavioral treatment of pathological gambling: a controlled study. J Consult Clin Psychol. 1997;65(5):727-732.
22. Carroll KM, Ball SA, Nich C, et al. Targeting behavioral therapies to enhance naltrexone treatment of opioid dependence. Arch Gen Psychiatry. 2001;58(8):755-761.
Mr. R., 37, started gambling during college. He often bet on sporting events with friends. The gambling was sporadic and apparently did not cause any problems in his life.
Over the next 3 or 4 years, he started visiting the local casino every couple of months with friends and playing blackjack. He occasionally won, but even if he lost he was able to return home without being preoccupied by the experience.
During the past year the frequency with which he gambled had increased. Prior to treatment, he was going to the casino 2 or 3 nights per week. Although he intended to gamble only for a few hours and spend no more than $100 each visit, Mr. R. usually spent most of the evening at the casino and squandered $500 to $1,000 per night. Mr. R. reported daily—and severe—urges to gamble. He would often see a billboard for the casino while driving home from his job as an accountant. The advertisement triggered his urges; instead of going home, he would drive to the casino.
While at work, Mr. R. spent so much time thinking of ways to win at gambling—which tables to play, how to lay the bets, which “lucky” shirt to wear—that he could not complete his assignments in a timely manner. He found it difficult to stay at work, even when he had meetings. Instead, when he felt urges to gamble, he would leave early.
Mr. R. felt ashamed of his gambling and kept it a secret from his wife. If unable to gamble when he had urges, he felt anxious and irritable. Because of his gambling, he missed family functions and lied to his wife and family.
Although married for only 3 years, his wife had already talked about divorce. Mr. R. had significant credit card debt and had to file for bankruptcy. Only then did he tell his wife about his gambling problem.
After telling his primary physician he was depressed, Mr. R. was treated with citalopram 20mg/d. The medication helped his mood but did not decrease his urges to gamble or alter his gambling behavior.
When he presented to our clinic, Mr. R. was off medication and still gambling 2 or 3 times per week. He was then treated with naltrexone 25mg/d for 2 days, then 50mg/d. Because of a possible drug-drug interaction with naltrexone, he agreed to stop taking over-the-counter nonsteroidal analgesics. After 2 weeks, the dosage was increased to 100mg/d taken in the morning with food. Mr. R. reported that his urges to gamble, although still present, were significantly reduced.
After another 2 weeks, the dosage was increased to 150mg/d. Mr. R. reported that his urges to gamble were gone. Without the urges, he was able to stop gambling. Liver function tests were performed every 2 weeks for the first 2 months of treatment and every month thereafter for 3 months.
This case illustrates many of the clinical features of pathological gambling, defined by persistent and recurrent maladaptive patterns of gambling behavior. The disorder often goes undiagnosed and untreated, though preliminary data suggest that it may be relatively common. The lifetime prevalence of pathological gambling is 1.6% among adults, and 3.9% among those younger than 18.1 Pathological gamblers usually experience painful financial losses and perhaps as a consequence have high rates of bankruptcy, divorce, and criminal behavior.2 They also often suffer from comorbid mood, anxiety, and alcohol use disorders.3 In fact, the suicide rate in cities with established, legal casinos is 2 to 4 times higher than in cities without.4
How to identify the pathological gambler
Pathological gambling is often a secret disorder. If left untreated, it frequently becomes a chronic condition. To make the diagnosis, use the simple screening instrument shown in (Table 1).5 The patient is likely to be suffering from pathological gambling disorder if he or she answered five or more of the questions “yes.” The last two questions are useful when trying to determine if someone has a gambling problem that is not readily apparent. Some people gamble in binges—for example, they may only gamble when they have available funds. These people may, however, be significantly impaired by the cravings or urges to gamble even though they may not have gambled for weeks.
Data suggest that the male-to-female ratio in pathological gambling is approximately 2:1. Gambling usually begins in early adulthood, with males tending to start at an earlier age. Although many pathological gamblers take several years to develop a problem, almost one-half report feeling “addicted” within a year after starting to gamble.2 Females appear to develop pathological gambling disorder in a shorter time.
Most pathological gamblers are fairly specific about their choice of gambling activity. Women tend to play slot machines and bingo, whereas men choose sporting events, blackjack, and cards. Both cite advertisements as a common trigger of their urges to gamble, although females are more likely to report that feeling bored or lonely may also trigger these urges.
Despite their preoccupation with gambling, many pathological gamblers function quite well, although often below their capacity. But others are severely debilitated—unable to function socially or occupationally.
In a series of 131 patients with pathological gambling disorder, 44% had lost all their savings, 24% had filed for bankruptcy, 23% had lost their homes or cars, and 15% had significant marital problems because of their gambling.2 Financial concerns may become so distressing that many pathological gamblers engage in illegal behavior, such as stealing, embezzlement, and writing bad checks.2
Table 1
Questions that can help diagnose pathological gambling
| Yes | No | Questions | |
|---|---|---|---|
| ○ | ○ | 1. Are you preoccupied with previous or future gambling experiences? That is, do you think about them a lot and wish you could think about them less? | |
| ○ | ○ | 2. Have you been unable to stop gambling or decrease the amount you gamble? | |
| ○ | ○ | 3. When you tried to stop or cut down, did you feel more irritable or anxious? | |
| ○ | ○ | 4. Has the amount you gamble increased to get the same sort of “high” or excitement? | |
| ○ | ○ | 5. Do you gamble as a way of escaping feelings of depression? | |
| ○ | ○ | 6. After you lose, do you go back in the next couple of days to try and win back the money? | |
| What effect has your gambling had on your life? | |||
| ○ | ○ | 7. Have you lied to others about your gambling? | |
| ○ | ○ | 8. Have you committed illegal acts as a result of gambling or lack of money? | |
| ○ | ○ | 9. Has gambling significantly interfered with school, job, or relationships? | |
| ○ | ○ | 10. Have you needed to borrow money because of gambling? | |
| ○ | ○ | 11. When you aren’t gambling, do you have urges to gamble? | |
| ○ | ○ | 12. If you have urges to gamble, do they preoccupy you or interfere with school, job, or relationships? | |
| adapted from DSM-IV criteria5 | |||
Table 2 Medical options for pathological gambling
Treatment response findings appear promising
Only a few controlled treatment studies of pathological gambling have been done, but the findings on the response to treatment appear promising. Thus far, the uses of serotonin reuptake inhibitors (SRIs), either clomipramine or selective serotonin reuptake inhibitors (SSRIs), the opioid antagonist naltrexone, mood stabilizers, and atypical neuroleptics have met with varying degrees of success. Additional strategies targeting urge and behavior reduction and mechanisms for coping with urges and behavior (e.g., cognitive behavioral therapies) may represent important adjunctive components.6
Because no medication is currently approved by the Food and Drug Administration (FDA) for treating pathological gambling, it is important to inform your patients of any “off-label” use of medications for this disorder, as well as the empirical basis for considering the medication.
The role of SRIs Response to SRIs usually means decreased thoughts about gambling, decreased gambling behavior, and improved social and occupational functioning. Patients may initially report feeling both less preoccupied with gambling and less anxious about having thoughts of gambling. For people who gamble because they are depressed and trying to escape loneliness or depressed feelings, SRIs are a reasonable first-line medication (Table 2).
As in the treatment of obsessive-compulsive disorder (OCD), dosages of SRIs required to treat pathological gambling symptoms appear to be higher than the average dosages required to treat depressive disorders. Some studies suggest that a significant initial response may be largely placebo. This means that improvement should be monitored for several months and that patients and clinicians need to be cautious about early improvement. An SRI should not be considered ineffective unless it has been tried for at least 10 to 12 weeks and the highest dose tolerated or recommended by the manufacturer has been reached.
The following SRIs have been used with varying degrees of success:
- Clomipramine has been shown effective in reducing gambling behavior with dosages between 125mg/d to 175mg/d.7
- Fluvoxamine has demonstrated mixed results in 3 studies of pathological gambling. Two studies supported its efficacy at an average dosage of 195mg/d to 207mg/d,8-9 but a third found that time spent gambling did not decrease when subjects took 200mg/d.10
- Citalopram has also shown some benefit as a possible treatment option in a single study.11
- Paroxetine, at dosages between 20mg/d and 60mg/d, was found to decrease thoughts of gambling and gambling behavior after approximately 6 to 8 weeks of treatment.12
- Fluoxetine (20mg/d) plus monthly supportive psychotherapy was found to improve gambling symptoms more than did supportive therapy alone.13
When naltrexone is indicated Naltrexone appears to be a reasonable first-line agent for patients who report intense urges to gamble (Table 2). Many patients who report “obsessions” with gambling may suffer from uncontrollable urges that interfere with daily functioning. By eliminating or reducing the urges, the preoccupation often disappears. Patients taking naltrexone often report less-intense urges. The urges may not go away completely; instead, they are often reduced enough for the patient to resist them more easily. Patients also report enjoying the gambling experience less when taking naltrexone; the “high” associated with gambling is reduced.
Naltrexone has been tested in psychiatric conditions in which urges are a dominant symptom.14 The greatest amount of evidence supports the agent’s use in treating alcohol dependence (see related article on page 55) and opiate dependence, both of which are FDA-approved indications.
In the case of pathological gambling, a small body of literature suggests that naltrexone is effective. One case report describes a patient suffering from both pathological gambling and alcohol dependence who responded to naltrexone 50mg/d.15 The first study using naltrexone in pathological gambling showed a significant decline in the intensity of urges to gamble, gambling thoughts, and gambling behavior when using 157 mg/d on average.16 This was followed by a larger study in which an average naltrexone dosage of 188mg/d resulted in improvement in gambling urges, thoughts, and behavior.14
Clinically, a patient will usually respond to a particular dose of naltrexone within 2 weeks. After that, an adjustment in dose is usually necessary. Patients often report nausea and diarrhea. Dizziness, sedation, and headaches occur less commonly. The side effects are usually mild and go away within the first week. Nausea, however, may be moderate to severe in some patients, so patients should be started on 25mg/d for the first 3 or 4 days to reduce that possibility. Ondansetron 4 mg/d is often given adjunctively for the same period to prevent the nausea.
Given the risk of associated hepatic transaminase elevations, liver function tests should be monitored in all patients taking naltrexone.14,16 A boxed warning refers to the potential hepatotoxicity of naltrexone at 50 mg/d, the dosage recommended for treating alcohol or opioid dependence. The warning also states that naltrexone use is contraindicated in acute hepatitis or liver failure, and its use in individuals with active liver disease must be carefully considered.
Initial liver function tests should be evaluated prior to naltrexone administration and again 3 to 4 weeks after starting the drug. Repeat testing should be performed at 2- to 4-week intervals for the next 2 months, a potential high-risk period. Thereafter, tests should be done approximately once a month for the following 3 months. After 6 months, liver enzyme elevations appear to occur rarely and testing 3 to 4 times a year should suffice unless an undue risk arises, e.g., excessive alcohol consumption. If elevated, the enzymes return to normal levels after discontinuing the naltrexone.
Research in this area is still in an early stage and clinicians prescribing the drug for pathological gambling should take extra caution in administering naltrexone at high doses and monitor for potential adverse consequences. Nonsteroidal analgesics should not be used in conjunction with high-dose naltrexone,14 as their concurrent use seems to cause a higher risk of hepatic transaminase elevation.
Mood stabilizers Successful responses to lithium and carbamazepine were described in 2 early case reports. Three subjects who were treated with lithium 1,800mg/d reported cessation of gambling.17 An early case report also found that carbamazepine resulted in improvement in pathological gambling disorder.18 Preliminary studies of lithium and valproate further support the notion that mood stabilizers may be useful. The benefit from carbamazepine, lithium, and valproate may be attributed to their efficacy in treating bipolar disorder and to the existence of features shared by pathological gambling and bipolar disorder (e.g., impulsivity).
Atypical antipsychotics Although there is little evidence that atypical antipsychotics work against pathological gambling when used alone, clinically atypical neuroleptic augmentation of SSRIs may be beneficial.
Atypical antipsychotics have been explored as augmenting agents in the treatment of nonpsychotic disorders and behaviors, including OCD. A recent trial of olanzapine in the treatment of pathological video poker gamblers showed no difference in outcomes between the patients on medication and those on placebo.19
Cognitive behavioral therapy There is also mounting evidence that cognitive behavioral treatments are effective for pathological gambling.6,20-21 Combined pharmacological and behavioral therapy is considered the optimal treatment strategy for many psychiatric disorders, including substance dependence.
In our clinical experience, patients who only partially respond or fail to respond to pharmacotherapy alone are more likely to find relief with a combination of drug and cognitive behavioral therapies. Future studies should explore directly how pharmacological and behavioral therapy contribute to clinical improvement as part of combination treatment strategies for pathological gambling.
Ways to enhance compliance
Pathological gamblers, like those with bipolar disorder or substance dependence, often fail to comply with treatment.
Patients suffering from mania may not adhere to treatment with mood stabilizers in part because drug treatment may reduce positive or euphoric experiences. Similarly, the “high” associated with drug use often makes patients ambivalent about taking medications to remain abstinent.
In treating opioid dependence with naltrexone, a reward system has been incorporated in a contingency management fashion to substitute for drug-related reward and to enhance compliance with the medication.22 Recruitment of friends or family has also been used to enhance compliance with naltrexone in treating opioid dependence.22
In the case of pathological gamblers, a self-rewarding system for each day of nongambling can be used (e.g., a favorite meal or a movie).6 Family members can help by increasing social or other activities that can take the patient’s mind off gambling, particularly at high-risk times (weekends and payday).6
How long should you treat?
No guidelines exist for recommended adequate treatment trials for pathological gambling. Available data, however, suggest that an adequate medication trial may require a relatively long duration (4 months or longer).
Many pathological gamblers have never discussed their difficulties, and this unquantifiable therapeutic response may resemble a medication response. Clinicians must monitor symptoms long enough to assess the difference between response to placebo and to medication.
The optimal duration of treatment and rates of relapse associated with discontinuation are not known. Many patients relapse upon discontinuation of medication, and long-term treatment, perhaps 2 to 3 years, may be warranted.
Treatment-resistant pathological gambling
It is not unusual to encounter patients who have had no response or only a partial response to treatment. Several approaches appear promising (Table 2):
- If a patient has had an adequate trial of either an SRI or naltrexone as monotherapy, adding another agent appears to result in additional clinical improvement.
- A patient who has failed to respond to either an SRI or naltrexone may be effectively treated with a mood stabilizer, either as monotherapy or as augmentation. Some patients with pathological gambling disorder, although not screening positive for a manic episode, exhibit symptoms consistent with cyclothymia or other subclinical cycling mood disorder. For such patients lithium, valproate, or another drug with putative mood stabilizing properties may represent an appropriate option.
- The possibility of adding atypical antipsychotics to SRIs in the SRI-refractory pathological gambler warrants consideration.
- Patients who only partially respond or fail to respond to medication alone are more likely to find relief with a combination of drug and cognitive-behavioral therapies, since this is considered the optimal treatment strategy for many psychiatric disorders.
Related resources
- Gamblers Anonymous International Service Office. Los Angeles, Calif. http://www.gamblersanonymous.org.
- National Research Council. Pathological Gambling: A Critical Review. Washington, DC: National Academy Press, 1990.
- James K. National Gambling Impact Study Commission: Final Report to Congress 1999. http://www.ngisc.gov/reports/finrpt.html
Drug brand names
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clomipramine • Anafranil
- Fluoxetine• Prozac, Prozac Weekly
- Fluvoxamine • Luvox
- Naltrexone • ReVia
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Valproic acid •Depakote
Disclosure
The authors report no affiliation or financial arrangement with any of the companies whose products are mentioned in this article.
Mr. R., 37, started gambling during college. He often bet on sporting events with friends. The gambling was sporadic and apparently did not cause any problems in his life.
Over the next 3 or 4 years, he started visiting the local casino every couple of months with friends and playing blackjack. He occasionally won, but even if he lost he was able to return home without being preoccupied by the experience.
During the past year the frequency with which he gambled had increased. Prior to treatment, he was going to the casino 2 or 3 nights per week. Although he intended to gamble only for a few hours and spend no more than $100 each visit, Mr. R. usually spent most of the evening at the casino and squandered $500 to $1,000 per night. Mr. R. reported daily—and severe—urges to gamble. He would often see a billboard for the casino while driving home from his job as an accountant. The advertisement triggered his urges; instead of going home, he would drive to the casino.
While at work, Mr. R. spent so much time thinking of ways to win at gambling—which tables to play, how to lay the bets, which “lucky” shirt to wear—that he could not complete his assignments in a timely manner. He found it difficult to stay at work, even when he had meetings. Instead, when he felt urges to gamble, he would leave early.
Mr. R. felt ashamed of his gambling and kept it a secret from his wife. If unable to gamble when he had urges, he felt anxious and irritable. Because of his gambling, he missed family functions and lied to his wife and family.
Although married for only 3 years, his wife had already talked about divorce. Mr. R. had significant credit card debt and had to file for bankruptcy. Only then did he tell his wife about his gambling problem.
After telling his primary physician he was depressed, Mr. R. was treated with citalopram 20mg/d. The medication helped his mood but did not decrease his urges to gamble or alter his gambling behavior.
When he presented to our clinic, Mr. R. was off medication and still gambling 2 or 3 times per week. He was then treated with naltrexone 25mg/d for 2 days, then 50mg/d. Because of a possible drug-drug interaction with naltrexone, he agreed to stop taking over-the-counter nonsteroidal analgesics. After 2 weeks, the dosage was increased to 100mg/d taken in the morning with food. Mr. R. reported that his urges to gamble, although still present, were significantly reduced.
After another 2 weeks, the dosage was increased to 150mg/d. Mr. R. reported that his urges to gamble were gone. Without the urges, he was able to stop gambling. Liver function tests were performed every 2 weeks for the first 2 months of treatment and every month thereafter for 3 months.
This case illustrates many of the clinical features of pathological gambling, defined by persistent and recurrent maladaptive patterns of gambling behavior. The disorder often goes undiagnosed and untreated, though preliminary data suggest that it may be relatively common. The lifetime prevalence of pathological gambling is 1.6% among adults, and 3.9% among those younger than 18.1 Pathological gamblers usually experience painful financial losses and perhaps as a consequence have high rates of bankruptcy, divorce, and criminal behavior.2 They also often suffer from comorbid mood, anxiety, and alcohol use disorders.3 In fact, the suicide rate in cities with established, legal casinos is 2 to 4 times higher than in cities without.4
How to identify the pathological gambler
Pathological gambling is often a secret disorder. If left untreated, it frequently becomes a chronic condition. To make the diagnosis, use the simple screening instrument shown in (Table 1).5 The patient is likely to be suffering from pathological gambling disorder if he or she answered five or more of the questions “yes.” The last two questions are useful when trying to determine if someone has a gambling problem that is not readily apparent. Some people gamble in binges—for example, they may only gamble when they have available funds. These people may, however, be significantly impaired by the cravings or urges to gamble even though they may not have gambled for weeks.
Data suggest that the male-to-female ratio in pathological gambling is approximately 2:1. Gambling usually begins in early adulthood, with males tending to start at an earlier age. Although many pathological gamblers take several years to develop a problem, almost one-half report feeling “addicted” within a year after starting to gamble.2 Females appear to develop pathological gambling disorder in a shorter time.
Most pathological gamblers are fairly specific about their choice of gambling activity. Women tend to play slot machines and bingo, whereas men choose sporting events, blackjack, and cards. Both cite advertisements as a common trigger of their urges to gamble, although females are more likely to report that feeling bored or lonely may also trigger these urges.
Despite their preoccupation with gambling, many pathological gamblers function quite well, although often below their capacity. But others are severely debilitated—unable to function socially or occupationally.
In a series of 131 patients with pathological gambling disorder, 44% had lost all their savings, 24% had filed for bankruptcy, 23% had lost their homes or cars, and 15% had significant marital problems because of their gambling.2 Financial concerns may become so distressing that many pathological gamblers engage in illegal behavior, such as stealing, embezzlement, and writing bad checks.2
Table 1
Questions that can help diagnose pathological gambling
| Yes | No | Questions | |
|---|---|---|---|
| ○ | ○ | 1. Are you preoccupied with previous or future gambling experiences? That is, do you think about them a lot and wish you could think about them less? | |
| ○ | ○ | 2. Have you been unable to stop gambling or decrease the amount you gamble? | |
| ○ | ○ | 3. When you tried to stop or cut down, did you feel more irritable or anxious? | |
| ○ | ○ | 4. Has the amount you gamble increased to get the same sort of “high” or excitement? | |
| ○ | ○ | 5. Do you gamble as a way of escaping feelings of depression? | |
| ○ | ○ | 6. After you lose, do you go back in the next couple of days to try and win back the money? | |
| What effect has your gambling had on your life? | |||
| ○ | ○ | 7. Have you lied to others about your gambling? | |
| ○ | ○ | 8. Have you committed illegal acts as a result of gambling or lack of money? | |
| ○ | ○ | 9. Has gambling significantly interfered with school, job, or relationships? | |
| ○ | ○ | 10. Have you needed to borrow money because of gambling? | |
| ○ | ○ | 11. When you aren’t gambling, do you have urges to gamble? | |
| ○ | ○ | 12. If you have urges to gamble, do they preoccupy you or interfere with school, job, or relationships? | |
| adapted from DSM-IV criteria5 | |||
Table 2 Medical options for pathological gambling
Treatment response findings appear promising
Only a few controlled treatment studies of pathological gambling have been done, but the findings on the response to treatment appear promising. Thus far, the uses of serotonin reuptake inhibitors (SRIs), either clomipramine or selective serotonin reuptake inhibitors (SSRIs), the opioid antagonist naltrexone, mood stabilizers, and atypical neuroleptics have met with varying degrees of success. Additional strategies targeting urge and behavior reduction and mechanisms for coping with urges and behavior (e.g., cognitive behavioral therapies) may represent important adjunctive components.6
Because no medication is currently approved by the Food and Drug Administration (FDA) for treating pathological gambling, it is important to inform your patients of any “off-label” use of medications for this disorder, as well as the empirical basis for considering the medication.
The role of SRIs Response to SRIs usually means decreased thoughts about gambling, decreased gambling behavior, and improved social and occupational functioning. Patients may initially report feeling both less preoccupied with gambling and less anxious about having thoughts of gambling. For people who gamble because they are depressed and trying to escape loneliness or depressed feelings, SRIs are a reasonable first-line medication (Table 2).
As in the treatment of obsessive-compulsive disorder (OCD), dosages of SRIs required to treat pathological gambling symptoms appear to be higher than the average dosages required to treat depressive disorders. Some studies suggest that a significant initial response may be largely placebo. This means that improvement should be monitored for several months and that patients and clinicians need to be cautious about early improvement. An SRI should not be considered ineffective unless it has been tried for at least 10 to 12 weeks and the highest dose tolerated or recommended by the manufacturer has been reached.
The following SRIs have been used with varying degrees of success:
- Clomipramine has been shown effective in reducing gambling behavior with dosages between 125mg/d to 175mg/d.7
- Fluvoxamine has demonstrated mixed results in 3 studies of pathological gambling. Two studies supported its efficacy at an average dosage of 195mg/d to 207mg/d,8-9 but a third found that time spent gambling did not decrease when subjects took 200mg/d.10
- Citalopram has also shown some benefit as a possible treatment option in a single study.11
- Paroxetine, at dosages between 20mg/d and 60mg/d, was found to decrease thoughts of gambling and gambling behavior after approximately 6 to 8 weeks of treatment.12
- Fluoxetine (20mg/d) plus monthly supportive psychotherapy was found to improve gambling symptoms more than did supportive therapy alone.13
When naltrexone is indicated Naltrexone appears to be a reasonable first-line agent for patients who report intense urges to gamble (Table 2). Many patients who report “obsessions” with gambling may suffer from uncontrollable urges that interfere with daily functioning. By eliminating or reducing the urges, the preoccupation often disappears. Patients taking naltrexone often report less-intense urges. The urges may not go away completely; instead, they are often reduced enough for the patient to resist them more easily. Patients also report enjoying the gambling experience less when taking naltrexone; the “high” associated with gambling is reduced.
Naltrexone has been tested in psychiatric conditions in which urges are a dominant symptom.14 The greatest amount of evidence supports the agent’s use in treating alcohol dependence (see related article on page 55) and opiate dependence, both of which are FDA-approved indications.
In the case of pathological gambling, a small body of literature suggests that naltrexone is effective. One case report describes a patient suffering from both pathological gambling and alcohol dependence who responded to naltrexone 50mg/d.15 The first study using naltrexone in pathological gambling showed a significant decline in the intensity of urges to gamble, gambling thoughts, and gambling behavior when using 157 mg/d on average.16 This was followed by a larger study in which an average naltrexone dosage of 188mg/d resulted in improvement in gambling urges, thoughts, and behavior.14
Clinically, a patient will usually respond to a particular dose of naltrexone within 2 weeks. After that, an adjustment in dose is usually necessary. Patients often report nausea and diarrhea. Dizziness, sedation, and headaches occur less commonly. The side effects are usually mild and go away within the first week. Nausea, however, may be moderate to severe in some patients, so patients should be started on 25mg/d for the first 3 or 4 days to reduce that possibility. Ondansetron 4 mg/d is often given adjunctively for the same period to prevent the nausea.
Given the risk of associated hepatic transaminase elevations, liver function tests should be monitored in all patients taking naltrexone.14,16 A boxed warning refers to the potential hepatotoxicity of naltrexone at 50 mg/d, the dosage recommended for treating alcohol or opioid dependence. The warning also states that naltrexone use is contraindicated in acute hepatitis or liver failure, and its use in individuals with active liver disease must be carefully considered.
Initial liver function tests should be evaluated prior to naltrexone administration and again 3 to 4 weeks after starting the drug. Repeat testing should be performed at 2- to 4-week intervals for the next 2 months, a potential high-risk period. Thereafter, tests should be done approximately once a month for the following 3 months. After 6 months, liver enzyme elevations appear to occur rarely and testing 3 to 4 times a year should suffice unless an undue risk arises, e.g., excessive alcohol consumption. If elevated, the enzymes return to normal levels after discontinuing the naltrexone.
Research in this area is still in an early stage and clinicians prescribing the drug for pathological gambling should take extra caution in administering naltrexone at high doses and monitor for potential adverse consequences. Nonsteroidal analgesics should not be used in conjunction with high-dose naltrexone,14 as their concurrent use seems to cause a higher risk of hepatic transaminase elevation.
Mood stabilizers Successful responses to lithium and carbamazepine were described in 2 early case reports. Three subjects who were treated with lithium 1,800mg/d reported cessation of gambling.17 An early case report also found that carbamazepine resulted in improvement in pathological gambling disorder.18 Preliminary studies of lithium and valproate further support the notion that mood stabilizers may be useful. The benefit from carbamazepine, lithium, and valproate may be attributed to their efficacy in treating bipolar disorder and to the existence of features shared by pathological gambling and bipolar disorder (e.g., impulsivity).
Atypical antipsychotics Although there is little evidence that atypical antipsychotics work against pathological gambling when used alone, clinically atypical neuroleptic augmentation of SSRIs may be beneficial.
Atypical antipsychotics have been explored as augmenting agents in the treatment of nonpsychotic disorders and behaviors, including OCD. A recent trial of olanzapine in the treatment of pathological video poker gamblers showed no difference in outcomes between the patients on medication and those on placebo.19
Cognitive behavioral therapy There is also mounting evidence that cognitive behavioral treatments are effective for pathological gambling.6,20-21 Combined pharmacological and behavioral therapy is considered the optimal treatment strategy for many psychiatric disorders, including substance dependence.
In our clinical experience, patients who only partially respond or fail to respond to pharmacotherapy alone are more likely to find relief with a combination of drug and cognitive behavioral therapies. Future studies should explore directly how pharmacological and behavioral therapy contribute to clinical improvement as part of combination treatment strategies for pathological gambling.
Ways to enhance compliance
Pathological gamblers, like those with bipolar disorder or substance dependence, often fail to comply with treatment.
Patients suffering from mania may not adhere to treatment with mood stabilizers in part because drug treatment may reduce positive or euphoric experiences. Similarly, the “high” associated with drug use often makes patients ambivalent about taking medications to remain abstinent.
In treating opioid dependence with naltrexone, a reward system has been incorporated in a contingency management fashion to substitute for drug-related reward and to enhance compliance with the medication.22 Recruitment of friends or family has also been used to enhance compliance with naltrexone in treating opioid dependence.22
In the case of pathological gamblers, a self-rewarding system for each day of nongambling can be used (e.g., a favorite meal or a movie).6 Family members can help by increasing social or other activities that can take the patient’s mind off gambling, particularly at high-risk times (weekends and payday).6
How long should you treat?
No guidelines exist for recommended adequate treatment trials for pathological gambling. Available data, however, suggest that an adequate medication trial may require a relatively long duration (4 months or longer).
Many pathological gamblers have never discussed their difficulties, and this unquantifiable therapeutic response may resemble a medication response. Clinicians must monitor symptoms long enough to assess the difference between response to placebo and to medication.
The optimal duration of treatment and rates of relapse associated with discontinuation are not known. Many patients relapse upon discontinuation of medication, and long-term treatment, perhaps 2 to 3 years, may be warranted.
Treatment-resistant pathological gambling
It is not unusual to encounter patients who have had no response or only a partial response to treatment. Several approaches appear promising (Table 2):
- If a patient has had an adequate trial of either an SRI or naltrexone as monotherapy, adding another agent appears to result in additional clinical improvement.
- A patient who has failed to respond to either an SRI or naltrexone may be effectively treated with a mood stabilizer, either as monotherapy or as augmentation. Some patients with pathological gambling disorder, although not screening positive for a manic episode, exhibit symptoms consistent with cyclothymia or other subclinical cycling mood disorder. For such patients lithium, valproate, or another drug with putative mood stabilizing properties may represent an appropriate option.
- The possibility of adding atypical antipsychotics to SRIs in the SRI-refractory pathological gambler warrants consideration.
- Patients who only partially respond or fail to respond to medication alone are more likely to find relief with a combination of drug and cognitive-behavioral therapies, since this is considered the optimal treatment strategy for many psychiatric disorders.
Related resources
- Gamblers Anonymous International Service Office. Los Angeles, Calif. http://www.gamblersanonymous.org.
- National Research Council. Pathological Gambling: A Critical Review. Washington, DC: National Academy Press, 1990.
- James K. National Gambling Impact Study Commission: Final Report to Congress 1999. http://www.ngisc.gov/reports/finrpt.html
Drug brand names
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clomipramine • Anafranil
- Fluoxetine• Prozac, Prozac Weekly
- Fluvoxamine • Luvox
- Naltrexone • ReVia
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Valproic acid •Depakote
Disclosure
The authors report no affiliation or financial arrangement with any of the companies whose products are mentioned in this article.
1. Shaffer HJ, Hall MN, Vander Bilt J. Estimating the prevalence of disordered gambling behavior in the United States and Canada: a research synthesis. Am J Public Health. 1999;89(9):1369-1376.
2. Grant JE, Kim SW. Demographic and clinical features of 131 adult pathological gamblers. J Clin Psychiatry. 2001;62(12):957-962.
3. Black DW, Moyer TM. Clinical features and psychiatric comorbidity of subjects with pathological gambling behavior. Psychiatric Serv. 1998;49(11):1434-1439.
4. Phillips DP, Welty WR, Smith MM. Elevated suicide levels associated with legalized gambling. Suicide Life Threat Behav. 1997;27(4):373-378.
5. American Psychiatric Association Committee on Nomenclature and Statistics. Diagnostic and Statistical Manual of Mental Disorders. 4th ed., text revision. Washington, DC: American Psychiatric Association, 2000.
6. Petry NM, Roll JM. A behavioral approach to understanding and treating pathological gambling. Semin Clin Neuropsychiatry. 2001;6(3):177-183.
7. Hollander E, Frenkel M, DeCaria C, et al. Treatment of pathological gambling with clomipramine. Am J Psychiatry. 1992;149(5):710-711.
8. Hollander E, DeCaria CM, Mari E, et al. Short-term single-blind fluvoxamine treatment of pathological gambling. Am J Psychiatry. 1998;155(12):1781-1783.
9. Hollander E, DeCaria CM, et al. A randomized double-blind fluvoxamine/placebo crossover trial in pathological gambling. Biol Psychiatry. 2000;47(9):813-817.
10. Blanco-Jerez C. A long-term, double-blind, placebo-controlled study of fluvoxamine for pathological gambling. Presented at the 152nd Annual Meeting of the American Psychiatric Association, Washington, DC, May 16-21, 1999 [abstract].
11. Zimmerman M, Breen R. An open-label study of citalopram in the treatment of pathological gambling. Presented at the 11th International Conference on Gambling and Risk Taking, Las Vegas, Nev, June 17-21, 2000 [abstract].
12. Kim SW, Grant JE, Shin YC, Toth JA, et al. A double-blind, placebo-controlled study of the efficacy and safety of paroxetine in the treatment of pathological gambling disorder. J Clin Psychiatry. 2002 (in press).
13. De la Gandara JJ. Fluoxetine: open-trial in pathological gambling. Presented at the 152 Annual Meeting of the American Psychiatric Association, Washington, DC, May 16-21, 1999 [abstract].
14. Kim SW, Grant JE, et al. Double-blind naltrexone and placebo comparison study in the treatment of pathological gambling. Biol Psychiatry. 2001;49(11):914-921.
15. Crockford DN, el-Guebaly N. Naltrexone in the treatment of pathological gambling and alcohol dependence. Can J Psychiatry. 1998;43(1):86.-
16. Kim SW, Grant JE. An open naltrexone treatment study of pathological gambling disorder. Int Clin Psychopharmacol. 2001;16(5):285-289.
17. Moskowitz JA. Lithium and lady luck: use of lithium carbonate in compulsive gambling. NY State J Med. 1980;80(5):785-788.
18. Haller R, Hinterhuber H. Treatment of pathological gambling with carbamazepine. Pharmacopsychiatry. 1994;27:129.-
19. Rugle L. The use of olanzapine in the treatment of video poker pathological gamblers. Presented at the conference titled, “The Comorbidity of Pathological Gambling: A Current Research Synthesis,” Dec 3 5, 2000, Las Vegas, Nev [abstract].
20. Ladoceur R, Sylvain C, Boutin C, et al. Cognitive treatment of pathological gambling. J Nerv Ment Dis. 2001;189(11):774-780.
21. Sylvain C, Ladouceur R, Boisvert JM. Cognitive and behavioral treatment of pathological gambling: a controlled study. J Consult Clin Psychol. 1997;65(5):727-732.
22. Carroll KM, Ball SA, Nich C, et al. Targeting behavioral therapies to enhance naltrexone treatment of opioid dependence. Arch Gen Psychiatry. 2001;58(8):755-761.
1. Shaffer HJ, Hall MN, Vander Bilt J. Estimating the prevalence of disordered gambling behavior in the United States and Canada: a research synthesis. Am J Public Health. 1999;89(9):1369-1376.
2. Grant JE, Kim SW. Demographic and clinical features of 131 adult pathological gamblers. J Clin Psychiatry. 2001;62(12):957-962.
3. Black DW, Moyer TM. Clinical features and psychiatric comorbidity of subjects with pathological gambling behavior. Psychiatric Serv. 1998;49(11):1434-1439.
4. Phillips DP, Welty WR, Smith MM. Elevated suicide levels associated with legalized gambling. Suicide Life Threat Behav. 1997;27(4):373-378.
5. American Psychiatric Association Committee on Nomenclature and Statistics. Diagnostic and Statistical Manual of Mental Disorders. 4th ed., text revision. Washington, DC: American Psychiatric Association, 2000.
6. Petry NM, Roll JM. A behavioral approach to understanding and treating pathological gambling. Semin Clin Neuropsychiatry. 2001;6(3):177-183.
7. Hollander E, Frenkel M, DeCaria C, et al. Treatment of pathological gambling with clomipramine. Am J Psychiatry. 1992;149(5):710-711.
8. Hollander E, DeCaria CM, Mari E, et al. Short-term single-blind fluvoxamine treatment of pathological gambling. Am J Psychiatry. 1998;155(12):1781-1783.
9. Hollander E, DeCaria CM, et al. A randomized double-blind fluvoxamine/placebo crossover trial in pathological gambling. Biol Psychiatry. 2000;47(9):813-817.
10. Blanco-Jerez C. A long-term, double-blind, placebo-controlled study of fluvoxamine for pathological gambling. Presented at the 152nd Annual Meeting of the American Psychiatric Association, Washington, DC, May 16-21, 1999 [abstract].
11. Zimmerman M, Breen R. An open-label study of citalopram in the treatment of pathological gambling. Presented at the 11th International Conference on Gambling and Risk Taking, Las Vegas, Nev, June 17-21, 2000 [abstract].
12. Kim SW, Grant JE, Shin YC, Toth JA, et al. A double-blind, placebo-controlled study of the efficacy and safety of paroxetine in the treatment of pathological gambling disorder. J Clin Psychiatry. 2002 (in press).
13. De la Gandara JJ. Fluoxetine: open-trial in pathological gambling. Presented at the 152 Annual Meeting of the American Psychiatric Association, Washington, DC, May 16-21, 1999 [abstract].
14. Kim SW, Grant JE, et al. Double-blind naltrexone and placebo comparison study in the treatment of pathological gambling. Biol Psychiatry. 2001;49(11):914-921.
15. Crockford DN, el-Guebaly N. Naltrexone in the treatment of pathological gambling and alcohol dependence. Can J Psychiatry. 1998;43(1):86.-
16. Kim SW, Grant JE. An open naltrexone treatment study of pathological gambling disorder. Int Clin Psychopharmacol. 2001;16(5):285-289.
17. Moskowitz JA. Lithium and lady luck: use of lithium carbonate in compulsive gambling. NY State J Med. 1980;80(5):785-788.
18. Haller R, Hinterhuber H. Treatment of pathological gambling with carbamazepine. Pharmacopsychiatry. 1994;27:129.-
19. Rugle L. The use of olanzapine in the treatment of video poker pathological gamblers. Presented at the conference titled, “The Comorbidity of Pathological Gambling: A Current Research Synthesis,” Dec 3 5, 2000, Las Vegas, Nev [abstract].
20. Ladoceur R, Sylvain C, Boutin C, et al. Cognitive treatment of pathological gambling. J Nerv Ment Dis. 2001;189(11):774-780.
21. Sylvain C, Ladouceur R, Boisvert JM. Cognitive and behavioral treatment of pathological gambling: a controlled study. J Consult Clin Psychol. 1997;65(5):727-732.
22. Carroll KM, Ball SA, Nich C, et al. Targeting behavioral therapies to enhance naltrexone treatment of opioid dependence. Arch Gen Psychiatry. 2001;58(8):755-761.