User login
A 52-year-old man becomes intoxicated with alcohol so he can lie in his backyard and get a tan. Convinced that his skin is too pale and that he looks “like a ghost,” he is so self-conscious about how he looks that he can’t go outside without drinking excessively.
An attractive 23-year-old woman dropped out of the 10th grade because of her “hideous” appearance and has hidden in her bedroom in her parents’ house ever since. She leaves her room no more than once a month, only after covering her face with a veil, not letting even her family see her face.
A middle-aged man cuts his nose open with a razor blade, trying to remove his nasal cartilage and replace it with chicken cartilage, in the desired shape.
These patients have body dysmorphic disorder (BDD), a somatoform disorder that the Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition (DSM-IV) defines as a preoccupation with an imagined defect in appearance; if a slight physical anomaly is present, the person's concern is markedly excessive. The preoccupation causes clinically significant distress or impairment in social, occupational, or other important areas of functioning that are not attributed to another mental disorder.
Most of us are dissatisfied with some aspect of how we look. In fact, more than half of all women and nearly half of all men in the United States are dissatisfied with their overall appearance.1 As the preceding cases illustrate, however, BDD does not consist simply of normal appearance concerns.
BDD is a relatively common disorder2 (Box 1) that occurs in children as well as adults. It usually begins during the early teenage years.2 BDD has been described around the world for more than a century.3 It causes notable distress and impaired functioning, and can lead to suicide.4 This disorder typically goes undiagnosed in clinical settings, however, in part because many patients are too embarrassed and ashamed to discuss their symptoms with their physicians unless specifically asked.2,5 BDD often masquerades as other psychiatric disorders, and misdiagnosis appears common6 (Table 1). Diagnosing BDD is usually straightforward, however, and can be achieved using the questions in Box 2.4 Clues to the presence of BDD are presented in Box 3; patients who present with any of them should be carefully evaluated for BDD.
- 1 in 8 psychiatric inpatients (13%)
- 1 in 7 to nearly half of outpatients with atypical major depression (14%-42%)
- 1 in 8 to 9 outpatients with social phobia (11%-13%)
- 1 in 3 to 12 outpatients with obsessive-compulsive disorder (8%-37%)
- 1 in 8 patients seeking dermatologic treatment (12%)
- 1 in 7 to 15 patients seeking cosmetic surgery (6%-15%)
- Nearly 1 in 100 to more than 1 in 50 people in the general population (0.7%-2.3%)
Perceptions of patients with BDD
Individuals with BDD obsess that there is something wrong with their appearance when in fact they look fine; the perceived flaw is actually minimal or nonexistent.7 Prior to treatment, insight is usually poor or absent, however, so that most patients are convinced or fairly certain that they look abnormal.2,8 They may describe the perceived flaw as unattractive or deformed, or they may even say that they look like a freak, a monster, or the “elephant man” (Box 4). Individuals with this disorder think about the perceived appearance flaws, on average, for 3 to 8 hours a day, and they usually find the thoughts difficult to resist or control.9 Diagnostic errors that cause BDD to be missed
Table 1
Diagnostic errors that cause BDD to be missed
| Misdiagnosis | Diagnostic error | How to avoid the error |
|---|---|---|
| Depression | The depressive symptoms that often coexist with BDD are diagnosed and BDD is missed; or BDD symptoms are considered a symptom of depression. In the author’s clinical experience, this is the most common diagnostic error. | Look for BDD in all depressed patients; appearance concerns may not be simply a symptom of depression. |
| Social phobia | Social anxiety is a common consequence of BDD, which may be misdiagnosed as social phobia or avoidant personality disorder. | Explore the cause of social anxiety or avoidance and determine whether it is secondary to BDD. |
| Agoraphobia | Many BDD patients are housebound at some point, which may be misdiagnosed as agoraphobia. | Explore the cause of avoidance and determine whether it is due to BDD. |
| OCD | BDD’s prominent obsessions and compulsive behaviors may be misdiagnosed as OCD. | If the obsessions and behaviors focus on physical appearance, BDD is the more accurate diagnosis. |
| Panic disorder | Panic attacks that occur when looking in the mirror or experiencing referential thinking can be misdiagnosed as panic disorder. | Determine whether panic attacks have BDD-related triggers; if so, BDD should be diagnosed. |
| Trichotillomania | Some BDD patients remove their body, head, or facial hair in an effort to improve their appearance, which may be misdiagnosed as trichotillomania. | Determine whether hair removal reflects thoughts that the hair does not look right and is intended to improve appearance; if so, the patient may have BDD. |
| Schizophrenia. | Because BDD beliefs are often delusional, and many patients have referential thinking, occasionally patients are misdiagnosed with Schizophrenia | If psychotic symptoms are largely limited to a nonbizarre delusional belief about one’s physical appearance and/or related delusions of reference, BDD is the more accurate diagnosis. |
Although repetitive behaviors are not part of BDD’s diagnostic criteria, virtually all patients perform such behaviors, usually in an attempt to improve, hide, examine, or be reassured about the perceived flaw.7,9 (See Box 3 for a partial listing.) These behaviors are usually time-consuming, occurring for many hours a day, and, like the preoccupations, are typically difficult to resist or control. With the exception of camouflaging, however, they often do not diminish appearance concerns. In fact, some of them (e.g., mirror checking) may actually increase anxiety about the perceived flaw.
Comorbidity is common in patients seen in clinical settings.2,8 Major depression is the most frequent comorbid disorder, which often appears secondary to BDD.10 Other common comorbidities include substance-use disorders, obsessive-compulsive disorder (OCD), social phobia, and personality disorders (most often, avoidant personality disorder).
Individuals with BDD are distressed over their appearance, many to the point of contemplating, attempting, or completing suicide.4,5 Nearly one quarter of patients seen in a clinical setting have attempted suicide.9 Although some patients appear to function reasonably well, they usually function below their capacity—for example, by avoiding social situations or meetings at work where others will see them. Others are completely incapacitated by their BDD symptoms, unable to work or socialize, and may be housebound for years.2,8,9 In a study that used the SF-36 to measure health-related quality of life, outpatients with BDD scored notably worse in all mental health domains than did the general U.S. population and patients with depression, type II diabetes, or a recent myocardial infarction.2
- Are you worried about your appearance in any way? If yes: What is your concern? OR Are you unhappy with how you look? If yes: What is your concern?
- Does this concern preoccupy you? That is, do you think about it a lot and wish you could worry about it less? OR If you add up all the time you spend each day thinking about your appearance, how much time would you estimate you spend?
- What effect has this preoccupation with your appearance had on your life? Has it:
BDD is diagnosed in patients who 1) are concerned about a minimal or nonexistent appearance flaw, 2) are preoccupied with the “flaw” (e.g., think about it for at least an hour a day), and 3) experience clinically significant distress or impairment in functioning as a result of their concern.

- Mirror checking or avoidance, or checking other reflective surfaces, such as windows, car bumpers, or the backs of spoons
- Reassurance seeking, that is, asking other people how they look or insisting that they look bad
- Skin picking, which may be manifested by skin lesions or scarring
- Excessive grooming, for example hair styling, applying makeup, shaving, tweezing hair, or cutting hair or wigs
- Camouflaging with a hat, toupee, makeup, sunglasses, clothes, or body position
- Excessive tanning, to darken “pale” skin
- Ideas or delusions of reference, thinking others take special notice of the “flaw” in a negative way (e.g., mock it or stare at it)
- Treatment-resistant anxiety, especially social anxiety, or depression
- Social avoidance or being housebound
- Unnecessary surgery, dermatologic treatment, or other nonpsychiatric treatment (e.g., electrolysis)
Guidelines for treating BDD
- Establish trust. It is important to convey that you take the patient’s appearance concerns seriously. Many patients with BDD fear being considered silly or vain and do not divulge their symptoms. It is usually best to avoid reassuring patients that they look fine, since they usually do not believe the reassurance and can interpret it as trivializing their concerns.
- Provide psychoeducation. Explain to patients that they have a relatively common and treatable body image disorder. To decrease the patient’s reluctance to accept the diagnosis and treatment, it can be helpful to emphasize the excessive preoccupation, distress, and other problems their symptoms are causing. Discussions about whether the defect is “real” are usually fruitless, unless the patient already has good insight, which is rare. Several educational books and Web sites for patients are available. See Related Resources.
- Target BDD symptoms in treatment. Ignoring BDD symptoms and focusing treatment on other symptoms only may be unsuccessful because effective treatment for BDD differs in some important ways from that of most other psychiatric disorders, such as depression.10 It appears, for example, that non-selective serotonin reuptake inhibitor (SSRI) antidepressants are generally ineffective for BDD, unless used at higher SSRI doses than are often needed for depression. BDD symptoms also do not necessarily improve in concert with symptoms of other disorders, such as depression or OCD.10
- Avoid nonpsychiatric medical treatment. Although no one can predict how an individual patient will respond to nonpsychiatric treatment, (e.g., surgery or dermatologic treatment), explain that as best we know, such treatment usually appears to be ineffective for BDD and even can make the symptoms worse.11
Which psychopharmaceuticals should you consider?
Although BDD’s response to pharmacotherapy has received far less investigation than that of many other psychiatric disorders, research on this treatment approach has dramatically increased in recent years. The following strategies are suggested on the basis of evidence from controlled studies, open-label trials, and the author’s clinical experience (Figure 1):2,6,8,12-17
‘I’m as ugly as the elephant man’

Chris is a shy, anxious-appearing, 31-year-old man who was hospitalized after attempting suicide. He wears a baseball cap pulled down over his forehead and partially covering his eyes. It is difficult for him to reveal the reason for his suicide attempt: “It’s really hard to talk about this. I don’t know if I can. It’s too embarrassing.” Then he adds, “Well I guess I should tell you—after all, I’m in the hospital because of it. It’s my nose—these huge pock marks on my nose. They’re grotesque! I look like a monster. I’m as ugly as the elephant man!
“These marks on my nose are all I can think about. I’ve thought about them for hours a day every day for the past 15 years. I even have nightmares about them. And I think that everyone can see them and that they laugh at me because of them. That’s why I wear this hat all the time. And that’s why I couldn’t talk to you in a bright room. You’d notice the marks and see how ugly I am.” Chris actually appeared entirely normal, but no one could convince him of this.
“This has affected me in a lot of ways,” Chris adds. “This may be hard for you to believe, but this problem has ruined my life. All I can think about is my face, and I spend hours a day looking at the marks in the mirror. I just can’t resist. I thought I looked so ugly that I started missing more and more work, and I stopped going out with my friends and my girlfriend. I got so anxious when people looked at me that I started staying in the house most of the time. Sometimes when I did go out, I went through red lights so I wouldn’t have to sit at the light, where people might be staring at me. The hat helped a little, but it didn’t cover all the marks. I tried covering them with makeup for a while, but I thought people could see the makeup so that didn’t really help. The only time I really felt comfortable is when I wore my nephew’s Batman mask on Halloween—then no one could see the marks.
I finally missed so much work that I was fired. My girlfriend stuck it out with me for a long time, but finally she couldn’t take it any more. One thing that was really hard for her was that I started asking her about 50 times a day whether I looked OK and whether she could see the marks—I think that was the final straw. If I had a choice, I’d rather have cancer. It must be less painful. This is like an arrow through my heart.”
Chris had a notable, although only partial, response to fluoxetine 100 mg/d and buspirone 60 mg/d (higher doses of fluoxetine and buspirone were tried but were not more effective). Adding clonazepam was helpful for severe anxiety. Clomipramine, venlafaxine, lithium, mirtazapine, and various antipsychotics were sequentially added to this regimen, with minimal success, although a second trial of olanzapine, at a higher dose (15 mg/d) than he had been willing to try previously, further decreased Chris’ BDD and depressive symptoms. The addition of bupropion was somewhat helpful for depression but not for BDD.
Figure 1 Proposed pharmacotherapy for treating BDD
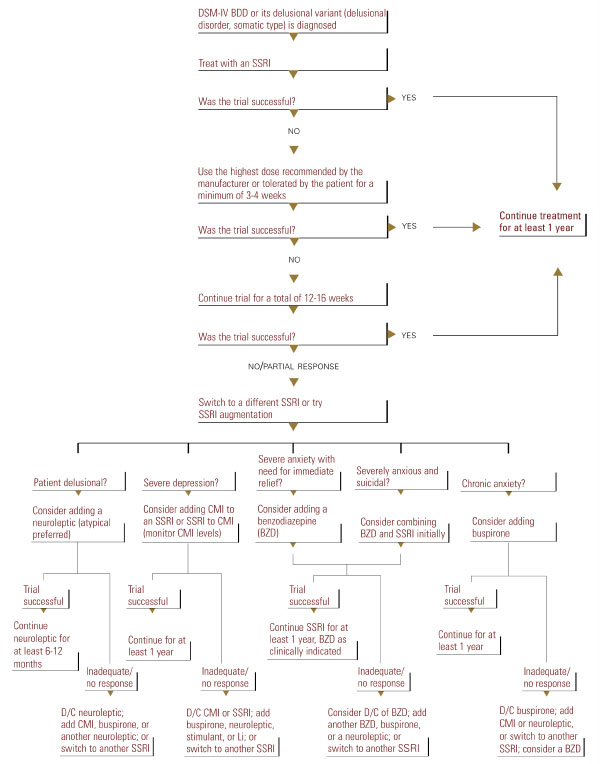
- Use an SSRI as a first-line approach. Other medications, including other antidepressants, appear less effective than SSRIs or clomipramine.2,8,9,13,15 An SSRI or clomipramine is also recommended for patients with delusional BDD (those who are completely convinced that they look abnormal and cannot be convinced otherwise), as Proposed pharmacotherapy for treating BDD these patients appear to respond to SSRIs as well as nondelusional patients do.12-17
- Use the maximum recommended or tolerated SSRI dose if lower doses are ineffective. Although no studies have compared different SSRI dosages, BDD appears to often require higher doses than those that are typically used for depression.
In a chart-review study of 90 patients with BDD treated in the author’s clinical practice, the mean SSRI doses used were fluoxetine 66.7 ±23.5 mg/d, fluvoxamine 308.3 ±49.2 mg/d, paroxetine 55.0 ± 12.9 mg/d, sertraline 202.1 ± 45.8 mg/d, and clomipramine 203.3 ±52.5 mg/d.17 Some patients respond only to doses higher than the maximum recommended dose (for example, 80-100 mg/d of citalopram or paroxetine).
- Treat for 12 to 16 weeks with an SSRI before concluding that the medication is ineffective. The average time to response is between 6 to 9 weeks.12,14,16 Clinical experience suggests that with continued treatment, relapse is rare and many patients further improve.
- Try sequential SSRIs if the first or second one does not work. A substantial percentage of patients who fail an initial SSRI trial will respond to a subsequent SSRI.17
- Continue an effective SSRI for at least 1 year before discontinuing it, as relapse appears likely with discontinuation.17 Severely ill patients may require treatment for life.
- Several SSRI augmentation and combination strategies might be helpful (Figure 1).16,17 If clomipramine is used in combination with an SSRI, the clomipramine level should be monitored.
What is the role of psychotherapy?
Although research on psychotherapy for BDD is limited, findings from clinical series and studies using waiting-list controls indicate that cognitive-behavioral therapy (CBT) is often effective.18-20 In contrast, supportive psychotherapy and insight-oriented and psychodynamic psychotherapy alone appear to be ineffective.9 CBT usually consists of a cognitive element (e.g., changing distorted views of the appearance “flaw”), exposure to feared and avoided situations (often social), and response prevention, avoiding repetitive behaviors such as excessive grooming.
- Consider using CBT as a first-line approach for milder BDD without significant comorbidity requiring pharmacotherapy.
- Use more intensive CBT treatment including frequent sessions and use of homework rather than less intensive treatment, although the optimal number and frequency of sessions is unknown.
- Consider maintenance and booster sessions for patients with more severe BDD following treatment to prevent relapse.
- Consider combining CBT and an SSRI. Although it is not known whether a combination of these treatments is more effective than either one alone, they are compatible and their combination may benefit certain patients. For patients with severe BDD, especially very depressed or suicidal patients, it is probably best to use CBT in combination with medication only, as sicker patients may not be able to tolerate or participate in CBT without first experiencing some improvement with medication.
- Phillips KA. The Broken Mirror: Understanding and Treating Body Dysmorphic Disorder. New York, NY: Oxford University Press, 1996.
- Pope HG, Phillips KA, Olivardia R. The Adonis Complex: The Secret Crisis of Male Body Obsession. New York, NY: The Free Press, 2000.
- Phillips KA, Van Noppen B, Shapiro L. Learning to Live with Body Dysmorphic Disorder. Milford, Conn: Obsessive-Compulsive Foundation, 1997.
- Body Dysmorphic Disorder (BDD)and Body Image Program Homepage at Butler Hospital (Providence, RI). http://www.bodyimageprogram.com
Drug brand names
- Bupropion • Wellbutrin, Zyban
- Buspirone • Buspar
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clonazepam • Ativan, Diastat, Halcion
- Fluoxetine • Prozac, Sarafem
- Fluvoxamine • Luvox
- Mirtazapine • Remeron, Remeron Solitab
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The author reports that she receives grant support and occasional speaking honoraria from Eli Lilly and Co.; receives grant support from Forest Pharmaceuticals and Gate Pharmaceuticals; is on the speakers' bureau of Solvay Pharmaceuticals; and serves as a consultant for Wyeth-Ayerst Pharmaceuticals.
1. Pope HG, Phillips KA, Olivardia R. The Adonis Complex: The Secret Crisis of Male Body Obsession. New York, NY: The Free Press, 2000.
2. Phillips KA. Body dysmorphic disorder. In: Phillips KA, ed. Somatoform and Factitious Disorders. Washington DC: American Psychiatric Publishing, 2001.
3. Phillips KA. Body dysmorphic disorder: the distress of imagined ugliness. Am J Psychiatry. 1991;148:1138-1149.
4. Phillips KA. The Broken Mirror: Understanding and Treating Body Dysmorphic Disorder. New York, NY: Oxford University Press, 1996.
5. Grant JE, et al. Prevalence and clinical features of body dysmorphic disorder in adolescent and adult psychiatric inpatients. J Clin Psychiatry. 2001;62:517-522.
6. Phillips KA. Body dysmorphic disorder: diagnostic controversies and treatment challenges. Bull Menninger Clin. 2000;64:18-35.
7. Hollander E, Cohen LJ, Simeon D. Body dysmorphic disorder. Psychiatric Annals. 1993;23:359-364.
8. Phillips KA, Castle DJ. Body dysmorphic disorder. In: Castle DJ, Phillips KA, eds. Disorders of Body Image. Hampshire, England: Wrightson Biomedical, in press.
9. Phillips KA, McElroy SL, Keck PE, Jr, Pope HG, Jr, Hudson JI. Body dysmorphic disorder: 30 cases of imagined ugliness. Am J Psychiatry. 1993;150:302-308.
10. Phillips KA: Body dysmorphic disorder and depression: theoretical considerations and treatment strategies. Psychiatry Quart. 1999;70:313-331.
11. Phillips KA, Grant JD, Siniscalchi J, Albertini RS. Surgical and nonpsychiatric medical treatment of patients with body dysmorphic disorder. Psychosomatics, in press.
12. Phillips KA, Dwight MM, McElroy SL. Efficacy and safety of fluvoxamine in body dysmorphic disorder. J Clin Psychiatry. 1998;59:165-171.
13. Hollander E, Allen A, Kwon J, Aronowitz B, Schmeidler J, Wong C, Simeon D. Clomipramine vs desipramine crossover trial in body dysmorphic disorder: selective efficacy of a serotonin reuptake inhibitor in imagined ugliness. Arch Gen Psychiatry. 1999;56:1033-1039.
14. Phillips KA, Albertini RS, Rasmussen SA. A randomized placebo-controlled trial of fluoxetine in body dysmorphic disorder. Arch Gen Psychiatry, in press.
15. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: review of the evidence and a recommended treatment approach. CNS Spectrums, in press.
16. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: a review of empirical data and a proposed treatment algorithm. Psychiatric Clin North Am. 2000;7:59-82.
17. Phillips KA, Albertini RS, Siniscalchi J, Khan A, Robinson M. Effectiveness of pharmacotherapy for body dysmorphic disorder: a chart-review study. J Clin Psychiatry. 2001;721-727.
18. Neziroglu FA, Yaryura-Tobias JA. Exposure, response prevention, and cognitive therapy in the treatment of body dysmorphic disorder. Behav Ther. 1993;24:431-438.
19. Veale D, Gournay K, Dryden W, Boocock A, Shah F, Willson R, Walburn J. Body dysmorphic disorder: a cognitive behavioural model and pilot randomized controlled trial. Behav Res Therapeut. 1996;34:717-729.
20. Wilhelm S, Otto MW, Lohr B, Deckersback T. Cognitive behavior group therapy for body dysmorphic disorder: a case series. Behav Res Ther. 1999;37:71-75.
A 52-year-old man becomes intoxicated with alcohol so he can lie in his backyard and get a tan. Convinced that his skin is too pale and that he looks “like a ghost,” he is so self-conscious about how he looks that he can’t go outside without drinking excessively.
An attractive 23-year-old woman dropped out of the 10th grade because of her “hideous” appearance and has hidden in her bedroom in her parents’ house ever since. She leaves her room no more than once a month, only after covering her face with a veil, not letting even her family see her face.
A middle-aged man cuts his nose open with a razor blade, trying to remove his nasal cartilage and replace it with chicken cartilage, in the desired shape.
These patients have body dysmorphic disorder (BDD), a somatoform disorder that the Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition (DSM-IV) defines as a preoccupation with an imagined defect in appearance; if a slight physical anomaly is present, the person's concern is markedly excessive. The preoccupation causes clinically significant distress or impairment in social, occupational, or other important areas of functioning that are not attributed to another mental disorder.
Most of us are dissatisfied with some aspect of how we look. In fact, more than half of all women and nearly half of all men in the United States are dissatisfied with their overall appearance.1 As the preceding cases illustrate, however, BDD does not consist simply of normal appearance concerns.
BDD is a relatively common disorder2 (Box 1) that occurs in children as well as adults. It usually begins during the early teenage years.2 BDD has been described around the world for more than a century.3 It causes notable distress and impaired functioning, and can lead to suicide.4 This disorder typically goes undiagnosed in clinical settings, however, in part because many patients are too embarrassed and ashamed to discuss their symptoms with their physicians unless specifically asked.2,5 BDD often masquerades as other psychiatric disorders, and misdiagnosis appears common6 (Table 1). Diagnosing BDD is usually straightforward, however, and can be achieved using the questions in Box 2.4 Clues to the presence of BDD are presented in Box 3; patients who present with any of them should be carefully evaluated for BDD.
- 1 in 8 psychiatric inpatients (13%)
- 1 in 7 to nearly half of outpatients with atypical major depression (14%-42%)
- 1 in 8 to 9 outpatients with social phobia (11%-13%)
- 1 in 3 to 12 outpatients with obsessive-compulsive disorder (8%-37%)
- 1 in 8 patients seeking dermatologic treatment (12%)
- 1 in 7 to 15 patients seeking cosmetic surgery (6%-15%)
- Nearly 1 in 100 to more than 1 in 50 people in the general population (0.7%-2.3%)
Perceptions of patients with BDD
Individuals with BDD obsess that there is something wrong with their appearance when in fact they look fine; the perceived flaw is actually minimal or nonexistent.7 Prior to treatment, insight is usually poor or absent, however, so that most patients are convinced or fairly certain that they look abnormal.2,8 They may describe the perceived flaw as unattractive or deformed, or they may even say that they look like a freak, a monster, or the “elephant man” (Box 4). Individuals with this disorder think about the perceived appearance flaws, on average, for 3 to 8 hours a day, and they usually find the thoughts difficult to resist or control.9 Diagnostic errors that cause BDD to be missed
Table 1
Diagnostic errors that cause BDD to be missed
| Misdiagnosis | Diagnostic error | How to avoid the error |
|---|---|---|
| Depression | The depressive symptoms that often coexist with BDD are diagnosed and BDD is missed; or BDD symptoms are considered a symptom of depression. In the author’s clinical experience, this is the most common diagnostic error. | Look for BDD in all depressed patients; appearance concerns may not be simply a symptom of depression. |
| Social phobia | Social anxiety is a common consequence of BDD, which may be misdiagnosed as social phobia or avoidant personality disorder. | Explore the cause of social anxiety or avoidance and determine whether it is secondary to BDD. |
| Agoraphobia | Many BDD patients are housebound at some point, which may be misdiagnosed as agoraphobia. | Explore the cause of avoidance and determine whether it is due to BDD. |
| OCD | BDD’s prominent obsessions and compulsive behaviors may be misdiagnosed as OCD. | If the obsessions and behaviors focus on physical appearance, BDD is the more accurate diagnosis. |
| Panic disorder | Panic attacks that occur when looking in the mirror or experiencing referential thinking can be misdiagnosed as panic disorder. | Determine whether panic attacks have BDD-related triggers; if so, BDD should be diagnosed. |
| Trichotillomania | Some BDD patients remove their body, head, or facial hair in an effort to improve their appearance, which may be misdiagnosed as trichotillomania. | Determine whether hair removal reflects thoughts that the hair does not look right and is intended to improve appearance; if so, the patient may have BDD. |
| Schizophrenia. | Because BDD beliefs are often delusional, and many patients have referential thinking, occasionally patients are misdiagnosed with Schizophrenia | If psychotic symptoms are largely limited to a nonbizarre delusional belief about one’s physical appearance and/or related delusions of reference, BDD is the more accurate diagnosis. |
Although repetitive behaviors are not part of BDD’s diagnostic criteria, virtually all patients perform such behaviors, usually in an attempt to improve, hide, examine, or be reassured about the perceived flaw.7,9 (See Box 3 for a partial listing.) These behaviors are usually time-consuming, occurring for many hours a day, and, like the preoccupations, are typically difficult to resist or control. With the exception of camouflaging, however, they often do not diminish appearance concerns. In fact, some of them (e.g., mirror checking) may actually increase anxiety about the perceived flaw.
Comorbidity is common in patients seen in clinical settings.2,8 Major depression is the most frequent comorbid disorder, which often appears secondary to BDD.10 Other common comorbidities include substance-use disorders, obsessive-compulsive disorder (OCD), social phobia, and personality disorders (most often, avoidant personality disorder).
Individuals with BDD are distressed over their appearance, many to the point of contemplating, attempting, or completing suicide.4,5 Nearly one quarter of patients seen in a clinical setting have attempted suicide.9 Although some patients appear to function reasonably well, they usually function below their capacity—for example, by avoiding social situations or meetings at work where others will see them. Others are completely incapacitated by their BDD symptoms, unable to work or socialize, and may be housebound for years.2,8,9 In a study that used the SF-36 to measure health-related quality of life, outpatients with BDD scored notably worse in all mental health domains than did the general U.S. population and patients with depression, type II diabetes, or a recent myocardial infarction.2
- Are you worried about your appearance in any way? If yes: What is your concern? OR Are you unhappy with how you look? If yes: What is your concern?
- Does this concern preoccupy you? That is, do you think about it a lot and wish you could worry about it less? OR If you add up all the time you spend each day thinking about your appearance, how much time would you estimate you spend?
- What effect has this preoccupation with your appearance had on your life? Has it:
BDD is diagnosed in patients who 1) are concerned about a minimal or nonexistent appearance flaw, 2) are preoccupied with the “flaw” (e.g., think about it for at least an hour a day), and 3) experience clinically significant distress or impairment in functioning as a result of their concern.
- Mirror checking or avoidance, or checking other reflective surfaces, such as windows, car bumpers, or the backs of spoons
- Reassurance seeking, that is, asking other people how they look or insisting that they look bad
- Skin picking, which may be manifested by skin lesions or scarring
- Excessive grooming, for example hair styling, applying makeup, shaving, tweezing hair, or cutting hair or wigs
- Camouflaging with a hat, toupee, makeup, sunglasses, clothes, or body position
- Excessive tanning, to darken “pale” skin
- Ideas or delusions of reference, thinking others take special notice of the “flaw” in a negative way (e.g., mock it or stare at it)
- Treatment-resistant anxiety, especially social anxiety, or depression
- Social avoidance or being housebound
- Unnecessary surgery, dermatologic treatment, or other nonpsychiatric treatment (e.g., electrolysis)
Guidelines for treating BDD
- Establish trust. It is important to convey that you take the patient’s appearance concerns seriously. Many patients with BDD fear being considered silly or vain and do not divulge their symptoms. It is usually best to avoid reassuring patients that they look fine, since they usually do not believe the reassurance and can interpret it as trivializing their concerns.
- Provide psychoeducation. Explain to patients that they have a relatively common and treatable body image disorder. To decrease the patient’s reluctance to accept the diagnosis and treatment, it can be helpful to emphasize the excessive preoccupation, distress, and other problems their symptoms are causing. Discussions about whether the defect is “real” are usually fruitless, unless the patient already has good insight, which is rare. Several educational books and Web sites for patients are available. See Related Resources.
- Target BDD symptoms in treatment. Ignoring BDD symptoms and focusing treatment on other symptoms only may be unsuccessful because effective treatment for BDD differs in some important ways from that of most other psychiatric disorders, such as depression.10 It appears, for example, that non-selective serotonin reuptake inhibitor (SSRI) antidepressants are generally ineffective for BDD, unless used at higher SSRI doses than are often needed for depression. BDD symptoms also do not necessarily improve in concert with symptoms of other disorders, such as depression or OCD.10
- Avoid nonpsychiatric medical treatment. Although no one can predict how an individual patient will respond to nonpsychiatric treatment, (e.g., surgery or dermatologic treatment), explain that as best we know, such treatment usually appears to be ineffective for BDD and even can make the symptoms worse.11
Which psychopharmaceuticals should you consider?
Although BDD’s response to pharmacotherapy has received far less investigation than that of many other psychiatric disorders, research on this treatment approach has dramatically increased in recent years. The following strategies are suggested on the basis of evidence from controlled studies, open-label trials, and the author’s clinical experience (Figure 1):2,6,8,12-17
‘I’m as ugly as the elephant man’
Chris is a shy, anxious-appearing, 31-year-old man who was hospitalized after attempting suicide. He wears a baseball cap pulled down over his forehead and partially covering his eyes. It is difficult for him to reveal the reason for his suicide attempt: “It’s really hard to talk about this. I don’t know if I can. It’s too embarrassing.” Then he adds, “Well I guess I should tell you—after all, I’m in the hospital because of it. It’s my nose—these huge pock marks on my nose. They’re grotesque! I look like a monster. I’m as ugly as the elephant man!
“These marks on my nose are all I can think about. I’ve thought about them for hours a day every day for the past 15 years. I even have nightmares about them. And I think that everyone can see them and that they laugh at me because of them. That’s why I wear this hat all the time. And that’s why I couldn’t talk to you in a bright room. You’d notice the marks and see how ugly I am.” Chris actually appeared entirely normal, but no one could convince him of this.
“This has affected me in a lot of ways,” Chris adds. “This may be hard for you to believe, but this problem has ruined my life. All I can think about is my face, and I spend hours a day looking at the marks in the mirror. I just can’t resist. I thought I looked so ugly that I started missing more and more work, and I stopped going out with my friends and my girlfriend. I got so anxious when people looked at me that I started staying in the house most of the time. Sometimes when I did go out, I went through red lights so I wouldn’t have to sit at the light, where people might be staring at me. The hat helped a little, but it didn’t cover all the marks. I tried covering them with makeup for a while, but I thought people could see the makeup so that didn’t really help. The only time I really felt comfortable is when I wore my nephew’s Batman mask on Halloween—then no one could see the marks.
I finally missed so much work that I was fired. My girlfriend stuck it out with me for a long time, but finally she couldn’t take it any more. One thing that was really hard for her was that I started asking her about 50 times a day whether I looked OK and whether she could see the marks—I think that was the final straw. If I had a choice, I’d rather have cancer. It must be less painful. This is like an arrow through my heart.”
Chris had a notable, although only partial, response to fluoxetine 100 mg/d and buspirone 60 mg/d (higher doses of fluoxetine and buspirone were tried but were not more effective). Adding clonazepam was helpful for severe anxiety. Clomipramine, venlafaxine, lithium, mirtazapine, and various antipsychotics were sequentially added to this regimen, with minimal success, although a second trial of olanzapine, at a higher dose (15 mg/d) than he had been willing to try previously, further decreased Chris’ BDD and depressive symptoms. The addition of bupropion was somewhat helpful for depression but not for BDD.
Figure 1 Proposed pharmacotherapy for treating BDD
- Use an SSRI as a first-line approach. Other medications, including other antidepressants, appear less effective than SSRIs or clomipramine.2,8,9,13,15 An SSRI or clomipramine is also recommended for patients with delusional BDD (those who are completely convinced that they look abnormal and cannot be convinced otherwise), as Proposed pharmacotherapy for treating BDD these patients appear to respond to SSRIs as well as nondelusional patients do.12-17
- Use the maximum recommended or tolerated SSRI dose if lower doses are ineffective. Although no studies have compared different SSRI dosages, BDD appears to often require higher doses than those that are typically used for depression.
In a chart-review study of 90 patients with BDD treated in the author’s clinical practice, the mean SSRI doses used were fluoxetine 66.7 ±23.5 mg/d, fluvoxamine 308.3 ±49.2 mg/d, paroxetine 55.0 ± 12.9 mg/d, sertraline 202.1 ± 45.8 mg/d, and clomipramine 203.3 ±52.5 mg/d.17 Some patients respond only to doses higher than the maximum recommended dose (for example, 80-100 mg/d of citalopram or paroxetine).
- Treat for 12 to 16 weeks with an SSRI before concluding that the medication is ineffective. The average time to response is between 6 to 9 weeks.12,14,16 Clinical experience suggests that with continued treatment, relapse is rare and many patients further improve.
- Try sequential SSRIs if the first or second one does not work. A substantial percentage of patients who fail an initial SSRI trial will respond to a subsequent SSRI.17
- Continue an effective SSRI for at least 1 year before discontinuing it, as relapse appears likely with discontinuation.17 Severely ill patients may require treatment for life.
- Several SSRI augmentation and combination strategies might be helpful (Figure 1).16,17 If clomipramine is used in combination with an SSRI, the clomipramine level should be monitored.
What is the role of psychotherapy?
Although research on psychotherapy for BDD is limited, findings from clinical series and studies using waiting-list controls indicate that cognitive-behavioral therapy (CBT) is often effective.18-20 In contrast, supportive psychotherapy and insight-oriented and psychodynamic psychotherapy alone appear to be ineffective.9 CBT usually consists of a cognitive element (e.g., changing distorted views of the appearance “flaw”), exposure to feared and avoided situations (often social), and response prevention, avoiding repetitive behaviors such as excessive grooming.
- Consider using CBT as a first-line approach for milder BDD without significant comorbidity requiring pharmacotherapy.
- Use more intensive CBT treatment including frequent sessions and use of homework rather than less intensive treatment, although the optimal number and frequency of sessions is unknown.
- Consider maintenance and booster sessions for patients with more severe BDD following treatment to prevent relapse.
- Consider combining CBT and an SSRI. Although it is not known whether a combination of these treatments is more effective than either one alone, they are compatible and their combination may benefit certain patients. For patients with severe BDD, especially very depressed or suicidal patients, it is probably best to use CBT in combination with medication only, as sicker patients may not be able to tolerate or participate in CBT without first experiencing some improvement with medication.
- Phillips KA. The Broken Mirror: Understanding and Treating Body Dysmorphic Disorder. New York, NY: Oxford University Press, 1996.
- Pope HG, Phillips KA, Olivardia R. The Adonis Complex: The Secret Crisis of Male Body Obsession. New York, NY: The Free Press, 2000.
- Phillips KA, Van Noppen B, Shapiro L. Learning to Live with Body Dysmorphic Disorder. Milford, Conn: Obsessive-Compulsive Foundation, 1997.
- Body Dysmorphic Disorder (BDD)and Body Image Program Homepage at Butler Hospital (Providence, RI). http://www.bodyimageprogram.com
Drug brand names
- Bupropion • Wellbutrin, Zyban
- Buspirone • Buspar
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clonazepam • Ativan, Diastat, Halcion
- Fluoxetine • Prozac, Sarafem
- Fluvoxamine • Luvox
- Mirtazapine • Remeron, Remeron Solitab
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The author reports that she receives grant support and occasional speaking honoraria from Eli Lilly and Co.; receives grant support from Forest Pharmaceuticals and Gate Pharmaceuticals; is on the speakers' bureau of Solvay Pharmaceuticals; and serves as a consultant for Wyeth-Ayerst Pharmaceuticals.
A 52-year-old man becomes intoxicated with alcohol so he can lie in his backyard and get a tan. Convinced that his skin is too pale and that he looks “like a ghost,” he is so self-conscious about how he looks that he can’t go outside without drinking excessively.
An attractive 23-year-old woman dropped out of the 10th grade because of her “hideous” appearance and has hidden in her bedroom in her parents’ house ever since. She leaves her room no more than once a month, only after covering her face with a veil, not letting even her family see her face.
A middle-aged man cuts his nose open with a razor blade, trying to remove his nasal cartilage and replace it with chicken cartilage, in the desired shape.
These patients have body dysmorphic disorder (BDD), a somatoform disorder that the Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition (DSM-IV) defines as a preoccupation with an imagined defect in appearance; if a slight physical anomaly is present, the person's concern is markedly excessive. The preoccupation causes clinically significant distress or impairment in social, occupational, or other important areas of functioning that are not attributed to another mental disorder.
Most of us are dissatisfied with some aspect of how we look. In fact, more than half of all women and nearly half of all men in the United States are dissatisfied with their overall appearance.1 As the preceding cases illustrate, however, BDD does not consist simply of normal appearance concerns.
BDD is a relatively common disorder2 (Box 1) that occurs in children as well as adults. It usually begins during the early teenage years.2 BDD has been described around the world for more than a century.3 It causes notable distress and impaired functioning, and can lead to suicide.4 This disorder typically goes undiagnosed in clinical settings, however, in part because many patients are too embarrassed and ashamed to discuss their symptoms with their physicians unless specifically asked.2,5 BDD often masquerades as other psychiatric disorders, and misdiagnosis appears common6 (Table 1). Diagnosing BDD is usually straightforward, however, and can be achieved using the questions in Box 2.4 Clues to the presence of BDD are presented in Box 3; patients who present with any of them should be carefully evaluated for BDD.
- 1 in 8 psychiatric inpatients (13%)
- 1 in 7 to nearly half of outpatients with atypical major depression (14%-42%)
- 1 in 8 to 9 outpatients with social phobia (11%-13%)
- 1 in 3 to 12 outpatients with obsessive-compulsive disorder (8%-37%)
- 1 in 8 patients seeking dermatologic treatment (12%)
- 1 in 7 to 15 patients seeking cosmetic surgery (6%-15%)
- Nearly 1 in 100 to more than 1 in 50 people in the general population (0.7%-2.3%)
Perceptions of patients with BDD
Individuals with BDD obsess that there is something wrong with their appearance when in fact they look fine; the perceived flaw is actually minimal or nonexistent.7 Prior to treatment, insight is usually poor or absent, however, so that most patients are convinced or fairly certain that they look abnormal.2,8 They may describe the perceived flaw as unattractive or deformed, or they may even say that they look like a freak, a monster, or the “elephant man” (Box 4). Individuals with this disorder think about the perceived appearance flaws, on average, for 3 to 8 hours a day, and they usually find the thoughts difficult to resist or control.9 Diagnostic errors that cause BDD to be missed
Table 1
Diagnostic errors that cause BDD to be missed
| Misdiagnosis | Diagnostic error | How to avoid the error |
|---|---|---|
| Depression | The depressive symptoms that often coexist with BDD are diagnosed and BDD is missed; or BDD symptoms are considered a symptom of depression. In the author’s clinical experience, this is the most common diagnostic error. | Look for BDD in all depressed patients; appearance concerns may not be simply a symptom of depression. |
| Social phobia | Social anxiety is a common consequence of BDD, which may be misdiagnosed as social phobia or avoidant personality disorder. | Explore the cause of social anxiety or avoidance and determine whether it is secondary to BDD. |
| Agoraphobia | Many BDD patients are housebound at some point, which may be misdiagnosed as agoraphobia. | Explore the cause of avoidance and determine whether it is due to BDD. |
| OCD | BDD’s prominent obsessions and compulsive behaviors may be misdiagnosed as OCD. | If the obsessions and behaviors focus on physical appearance, BDD is the more accurate diagnosis. |
| Panic disorder | Panic attacks that occur when looking in the mirror or experiencing referential thinking can be misdiagnosed as panic disorder. | Determine whether panic attacks have BDD-related triggers; if so, BDD should be diagnosed. |
| Trichotillomania | Some BDD patients remove their body, head, or facial hair in an effort to improve their appearance, which may be misdiagnosed as trichotillomania. | Determine whether hair removal reflects thoughts that the hair does not look right and is intended to improve appearance; if so, the patient may have BDD. |
| Schizophrenia. | Because BDD beliefs are often delusional, and many patients have referential thinking, occasionally patients are misdiagnosed with Schizophrenia | If psychotic symptoms are largely limited to a nonbizarre delusional belief about one’s physical appearance and/or related delusions of reference, BDD is the more accurate diagnosis. |
Although repetitive behaviors are not part of BDD’s diagnostic criteria, virtually all patients perform such behaviors, usually in an attempt to improve, hide, examine, or be reassured about the perceived flaw.7,9 (See Box 3 for a partial listing.) These behaviors are usually time-consuming, occurring for many hours a day, and, like the preoccupations, are typically difficult to resist or control. With the exception of camouflaging, however, they often do not diminish appearance concerns. In fact, some of them (e.g., mirror checking) may actually increase anxiety about the perceived flaw.
Comorbidity is common in patients seen in clinical settings.2,8 Major depression is the most frequent comorbid disorder, which often appears secondary to BDD.10 Other common comorbidities include substance-use disorders, obsessive-compulsive disorder (OCD), social phobia, and personality disorders (most often, avoidant personality disorder).
Individuals with BDD are distressed over their appearance, many to the point of contemplating, attempting, or completing suicide.4,5 Nearly one quarter of patients seen in a clinical setting have attempted suicide.9 Although some patients appear to function reasonably well, they usually function below their capacity—for example, by avoiding social situations or meetings at work where others will see them. Others are completely incapacitated by their BDD symptoms, unable to work or socialize, and may be housebound for years.2,8,9 In a study that used the SF-36 to measure health-related quality of life, outpatients with BDD scored notably worse in all mental health domains than did the general U.S. population and patients with depression, type II diabetes, or a recent myocardial infarction.2
- Are you worried about your appearance in any way? If yes: What is your concern? OR Are you unhappy with how you look? If yes: What is your concern?
- Does this concern preoccupy you? That is, do you think about it a lot and wish you could worry about it less? OR If you add up all the time you spend each day thinking about your appearance, how much time would you estimate you spend?
- What effect has this preoccupation with your appearance had on your life? Has it:
BDD is diagnosed in patients who 1) are concerned about a minimal or nonexistent appearance flaw, 2) are preoccupied with the “flaw” (e.g., think about it for at least an hour a day), and 3) experience clinically significant distress or impairment in functioning as a result of their concern.
- Mirror checking or avoidance, or checking other reflective surfaces, such as windows, car bumpers, or the backs of spoons
- Reassurance seeking, that is, asking other people how they look or insisting that they look bad
- Skin picking, which may be manifested by skin lesions or scarring
- Excessive grooming, for example hair styling, applying makeup, shaving, tweezing hair, or cutting hair or wigs
- Camouflaging with a hat, toupee, makeup, sunglasses, clothes, or body position
- Excessive tanning, to darken “pale” skin
- Ideas or delusions of reference, thinking others take special notice of the “flaw” in a negative way (e.g., mock it or stare at it)
- Treatment-resistant anxiety, especially social anxiety, or depression
- Social avoidance or being housebound
- Unnecessary surgery, dermatologic treatment, or other nonpsychiatric treatment (e.g., electrolysis)
Guidelines for treating BDD
- Establish trust. It is important to convey that you take the patient’s appearance concerns seriously. Many patients with BDD fear being considered silly or vain and do not divulge their symptoms. It is usually best to avoid reassuring patients that they look fine, since they usually do not believe the reassurance and can interpret it as trivializing their concerns.
- Provide psychoeducation. Explain to patients that they have a relatively common and treatable body image disorder. To decrease the patient’s reluctance to accept the diagnosis and treatment, it can be helpful to emphasize the excessive preoccupation, distress, and other problems their symptoms are causing. Discussions about whether the defect is “real” are usually fruitless, unless the patient already has good insight, which is rare. Several educational books and Web sites for patients are available. See Related Resources.
- Target BDD symptoms in treatment. Ignoring BDD symptoms and focusing treatment on other symptoms only may be unsuccessful because effective treatment for BDD differs in some important ways from that of most other psychiatric disorders, such as depression.10 It appears, for example, that non-selective serotonin reuptake inhibitor (SSRI) antidepressants are generally ineffective for BDD, unless used at higher SSRI doses than are often needed for depression. BDD symptoms also do not necessarily improve in concert with symptoms of other disorders, such as depression or OCD.10
- Avoid nonpsychiatric medical treatment. Although no one can predict how an individual patient will respond to nonpsychiatric treatment, (e.g., surgery or dermatologic treatment), explain that as best we know, such treatment usually appears to be ineffective for BDD and even can make the symptoms worse.11
Which psychopharmaceuticals should you consider?
Although BDD’s response to pharmacotherapy has received far less investigation than that of many other psychiatric disorders, research on this treatment approach has dramatically increased in recent years. The following strategies are suggested on the basis of evidence from controlled studies, open-label trials, and the author’s clinical experience (Figure 1):2,6,8,12-17
‘I’m as ugly as the elephant man’
Chris is a shy, anxious-appearing, 31-year-old man who was hospitalized after attempting suicide. He wears a baseball cap pulled down over his forehead and partially covering his eyes. It is difficult for him to reveal the reason for his suicide attempt: “It’s really hard to talk about this. I don’t know if I can. It’s too embarrassing.” Then he adds, “Well I guess I should tell you—after all, I’m in the hospital because of it. It’s my nose—these huge pock marks on my nose. They’re grotesque! I look like a monster. I’m as ugly as the elephant man!
“These marks on my nose are all I can think about. I’ve thought about them for hours a day every day for the past 15 years. I even have nightmares about them. And I think that everyone can see them and that they laugh at me because of them. That’s why I wear this hat all the time. And that’s why I couldn’t talk to you in a bright room. You’d notice the marks and see how ugly I am.” Chris actually appeared entirely normal, but no one could convince him of this.
“This has affected me in a lot of ways,” Chris adds. “This may be hard for you to believe, but this problem has ruined my life. All I can think about is my face, and I spend hours a day looking at the marks in the mirror. I just can’t resist. I thought I looked so ugly that I started missing more and more work, and I stopped going out with my friends and my girlfriend. I got so anxious when people looked at me that I started staying in the house most of the time. Sometimes when I did go out, I went through red lights so I wouldn’t have to sit at the light, where people might be staring at me. The hat helped a little, but it didn’t cover all the marks. I tried covering them with makeup for a while, but I thought people could see the makeup so that didn’t really help. The only time I really felt comfortable is when I wore my nephew’s Batman mask on Halloween—then no one could see the marks.
I finally missed so much work that I was fired. My girlfriend stuck it out with me for a long time, but finally she couldn’t take it any more. One thing that was really hard for her was that I started asking her about 50 times a day whether I looked OK and whether she could see the marks—I think that was the final straw. If I had a choice, I’d rather have cancer. It must be less painful. This is like an arrow through my heart.”
Chris had a notable, although only partial, response to fluoxetine 100 mg/d and buspirone 60 mg/d (higher doses of fluoxetine and buspirone were tried but were not more effective). Adding clonazepam was helpful for severe anxiety. Clomipramine, venlafaxine, lithium, mirtazapine, and various antipsychotics were sequentially added to this regimen, with minimal success, although a second trial of olanzapine, at a higher dose (15 mg/d) than he had been willing to try previously, further decreased Chris’ BDD and depressive symptoms. The addition of bupropion was somewhat helpful for depression but not for BDD.
Figure 1 Proposed pharmacotherapy for treating BDD
- Use an SSRI as a first-line approach. Other medications, including other antidepressants, appear less effective than SSRIs or clomipramine.2,8,9,13,15 An SSRI or clomipramine is also recommended for patients with delusional BDD (those who are completely convinced that they look abnormal and cannot be convinced otherwise), as Proposed pharmacotherapy for treating BDD these patients appear to respond to SSRIs as well as nondelusional patients do.12-17
- Use the maximum recommended or tolerated SSRI dose if lower doses are ineffective. Although no studies have compared different SSRI dosages, BDD appears to often require higher doses than those that are typically used for depression.
In a chart-review study of 90 patients with BDD treated in the author’s clinical practice, the mean SSRI doses used were fluoxetine 66.7 ±23.5 mg/d, fluvoxamine 308.3 ±49.2 mg/d, paroxetine 55.0 ± 12.9 mg/d, sertraline 202.1 ± 45.8 mg/d, and clomipramine 203.3 ±52.5 mg/d.17 Some patients respond only to doses higher than the maximum recommended dose (for example, 80-100 mg/d of citalopram or paroxetine).
- Treat for 12 to 16 weeks with an SSRI before concluding that the medication is ineffective. The average time to response is between 6 to 9 weeks.12,14,16 Clinical experience suggests that with continued treatment, relapse is rare and many patients further improve.
- Try sequential SSRIs if the first or second one does not work. A substantial percentage of patients who fail an initial SSRI trial will respond to a subsequent SSRI.17
- Continue an effective SSRI for at least 1 year before discontinuing it, as relapse appears likely with discontinuation.17 Severely ill patients may require treatment for life.
- Several SSRI augmentation and combination strategies might be helpful (Figure 1).16,17 If clomipramine is used in combination with an SSRI, the clomipramine level should be monitored.
What is the role of psychotherapy?
Although research on psychotherapy for BDD is limited, findings from clinical series and studies using waiting-list controls indicate that cognitive-behavioral therapy (CBT) is often effective.18-20 In contrast, supportive psychotherapy and insight-oriented and psychodynamic psychotherapy alone appear to be ineffective.9 CBT usually consists of a cognitive element (e.g., changing distorted views of the appearance “flaw”), exposure to feared and avoided situations (often social), and response prevention, avoiding repetitive behaviors such as excessive grooming.
- Consider using CBT as a first-line approach for milder BDD without significant comorbidity requiring pharmacotherapy.
- Use more intensive CBT treatment including frequent sessions and use of homework rather than less intensive treatment, although the optimal number and frequency of sessions is unknown.
- Consider maintenance and booster sessions for patients with more severe BDD following treatment to prevent relapse.
- Consider combining CBT and an SSRI. Although it is not known whether a combination of these treatments is more effective than either one alone, they are compatible and their combination may benefit certain patients. For patients with severe BDD, especially very depressed or suicidal patients, it is probably best to use CBT in combination with medication only, as sicker patients may not be able to tolerate or participate in CBT without first experiencing some improvement with medication.
- Phillips KA. The Broken Mirror: Understanding and Treating Body Dysmorphic Disorder. New York, NY: Oxford University Press, 1996.
- Pope HG, Phillips KA, Olivardia R. The Adonis Complex: The Secret Crisis of Male Body Obsession. New York, NY: The Free Press, 2000.
- Phillips KA, Van Noppen B, Shapiro L. Learning to Live with Body Dysmorphic Disorder. Milford, Conn: Obsessive-Compulsive Foundation, 1997.
- Body Dysmorphic Disorder (BDD)and Body Image Program Homepage at Butler Hospital (Providence, RI). http://www.bodyimageprogram.com
Drug brand names
- Bupropion • Wellbutrin, Zyban
- Buspirone • Buspar
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clonazepam • Ativan, Diastat, Halcion
- Fluoxetine • Prozac, Sarafem
- Fluvoxamine • Luvox
- Mirtazapine • Remeron, Remeron Solitab
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The author reports that she receives grant support and occasional speaking honoraria from Eli Lilly and Co.; receives grant support from Forest Pharmaceuticals and Gate Pharmaceuticals; is on the speakers' bureau of Solvay Pharmaceuticals; and serves as a consultant for Wyeth-Ayerst Pharmaceuticals.
1. Pope HG, Phillips KA, Olivardia R. The Adonis Complex: The Secret Crisis of Male Body Obsession. New York, NY: The Free Press, 2000.
2. Phillips KA. Body dysmorphic disorder. In: Phillips KA, ed. Somatoform and Factitious Disorders. Washington DC: American Psychiatric Publishing, 2001.
3. Phillips KA. Body dysmorphic disorder: the distress of imagined ugliness. Am J Psychiatry. 1991;148:1138-1149.
4. Phillips KA. The Broken Mirror: Understanding and Treating Body Dysmorphic Disorder. New York, NY: Oxford University Press, 1996.
5. Grant JE, et al. Prevalence and clinical features of body dysmorphic disorder in adolescent and adult psychiatric inpatients. J Clin Psychiatry. 2001;62:517-522.
6. Phillips KA. Body dysmorphic disorder: diagnostic controversies and treatment challenges. Bull Menninger Clin. 2000;64:18-35.
7. Hollander E, Cohen LJ, Simeon D. Body dysmorphic disorder. Psychiatric Annals. 1993;23:359-364.
8. Phillips KA, Castle DJ. Body dysmorphic disorder. In: Castle DJ, Phillips KA, eds. Disorders of Body Image. Hampshire, England: Wrightson Biomedical, in press.
9. Phillips KA, McElroy SL, Keck PE, Jr, Pope HG, Jr, Hudson JI. Body dysmorphic disorder: 30 cases of imagined ugliness. Am J Psychiatry. 1993;150:302-308.
10. Phillips KA: Body dysmorphic disorder and depression: theoretical considerations and treatment strategies. Psychiatry Quart. 1999;70:313-331.
11. Phillips KA, Grant JD, Siniscalchi J, Albertini RS. Surgical and nonpsychiatric medical treatment of patients with body dysmorphic disorder. Psychosomatics, in press.
12. Phillips KA, Dwight MM, McElroy SL. Efficacy and safety of fluvoxamine in body dysmorphic disorder. J Clin Psychiatry. 1998;59:165-171.
13. Hollander E, Allen A, Kwon J, Aronowitz B, Schmeidler J, Wong C, Simeon D. Clomipramine vs desipramine crossover trial in body dysmorphic disorder: selective efficacy of a serotonin reuptake inhibitor in imagined ugliness. Arch Gen Psychiatry. 1999;56:1033-1039.
14. Phillips KA, Albertini RS, Rasmussen SA. A randomized placebo-controlled trial of fluoxetine in body dysmorphic disorder. Arch Gen Psychiatry, in press.
15. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: review of the evidence and a recommended treatment approach. CNS Spectrums, in press.
16. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: a review of empirical data and a proposed treatment algorithm. Psychiatric Clin North Am. 2000;7:59-82.
17. Phillips KA, Albertini RS, Siniscalchi J, Khan A, Robinson M. Effectiveness of pharmacotherapy for body dysmorphic disorder: a chart-review study. J Clin Psychiatry. 2001;721-727.
18. Neziroglu FA, Yaryura-Tobias JA. Exposure, response prevention, and cognitive therapy in the treatment of body dysmorphic disorder. Behav Ther. 1993;24:431-438.
19. Veale D, Gournay K, Dryden W, Boocock A, Shah F, Willson R, Walburn J. Body dysmorphic disorder: a cognitive behavioural model and pilot randomized controlled trial. Behav Res Therapeut. 1996;34:717-729.
20. Wilhelm S, Otto MW, Lohr B, Deckersback T. Cognitive behavior group therapy for body dysmorphic disorder: a case series. Behav Res Ther. 1999;37:71-75.
1. Pope HG, Phillips KA, Olivardia R. The Adonis Complex: The Secret Crisis of Male Body Obsession. New York, NY: The Free Press, 2000.
2. Phillips KA. Body dysmorphic disorder. In: Phillips KA, ed. Somatoform and Factitious Disorders. Washington DC: American Psychiatric Publishing, 2001.
3. Phillips KA. Body dysmorphic disorder: the distress of imagined ugliness. Am J Psychiatry. 1991;148:1138-1149.
4. Phillips KA. The Broken Mirror: Understanding and Treating Body Dysmorphic Disorder. New York, NY: Oxford University Press, 1996.
5. Grant JE, et al. Prevalence and clinical features of body dysmorphic disorder in adolescent and adult psychiatric inpatients. J Clin Psychiatry. 2001;62:517-522.
6. Phillips KA. Body dysmorphic disorder: diagnostic controversies and treatment challenges. Bull Menninger Clin. 2000;64:18-35.
7. Hollander E, Cohen LJ, Simeon D. Body dysmorphic disorder. Psychiatric Annals. 1993;23:359-364.
8. Phillips KA, Castle DJ. Body dysmorphic disorder. In: Castle DJ, Phillips KA, eds. Disorders of Body Image. Hampshire, England: Wrightson Biomedical, in press.
9. Phillips KA, McElroy SL, Keck PE, Jr, Pope HG, Jr, Hudson JI. Body dysmorphic disorder: 30 cases of imagined ugliness. Am J Psychiatry. 1993;150:302-308.
10. Phillips KA: Body dysmorphic disorder and depression: theoretical considerations and treatment strategies. Psychiatry Quart. 1999;70:313-331.
11. Phillips KA, Grant JD, Siniscalchi J, Albertini RS. Surgical and nonpsychiatric medical treatment of patients with body dysmorphic disorder. Psychosomatics, in press.
12. Phillips KA, Dwight MM, McElroy SL. Efficacy and safety of fluvoxamine in body dysmorphic disorder. J Clin Psychiatry. 1998;59:165-171.
13. Hollander E, Allen A, Kwon J, Aronowitz B, Schmeidler J, Wong C, Simeon D. Clomipramine vs desipramine crossover trial in body dysmorphic disorder: selective efficacy of a serotonin reuptake inhibitor in imagined ugliness. Arch Gen Psychiatry. 1999;56:1033-1039.
14. Phillips KA, Albertini RS, Rasmussen SA. A randomized placebo-controlled trial of fluoxetine in body dysmorphic disorder. Arch Gen Psychiatry, in press.
15. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: review of the evidence and a recommended treatment approach. CNS Spectrums, in press.
16. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: a review of empirical data and a proposed treatment algorithm. Psychiatric Clin North Am. 2000;7:59-82.
17. Phillips KA, Albertini RS, Siniscalchi J, Khan A, Robinson M. Effectiveness of pharmacotherapy for body dysmorphic disorder: a chart-review study. J Clin Psychiatry. 2001;721-727.
18. Neziroglu FA, Yaryura-Tobias JA. Exposure, response prevention, and cognitive therapy in the treatment of body dysmorphic disorder. Behav Ther. 1993;24:431-438.
19. Veale D, Gournay K, Dryden W, Boocock A, Shah F, Willson R, Walburn J. Body dysmorphic disorder: a cognitive behavioural model and pilot randomized controlled trial. Behav Res Therapeut. 1996;34:717-729.
20. Wilhelm S, Otto MW, Lohr B, Deckersback T. Cognitive behavior group therapy for body dysmorphic disorder: a case series. Behav Res Ther. 1999;37:71-75.