User login
NEW YORK – About one in four patients with abdominal aortic aneurysm may be at risk for thoracic aneurysm, judging by results of a single-center retrospective study of more than 1,000 patients.
Dr. Rabih Chaer, a vascular surgeon at the University of Pittsburgh, and his colleagues found that, among 1,082 patients diagnosed with abdominal aortic aneurysms (AAA) who had chest CT at follow-up, 23.4% had some sort of thoracic aneurysm afterward.
“Despite the clinical associations that have been observed between AAAs and peripheral aneurysms and thoracic aneurysms, screening for other common aneurysms continues to be controversial,” Dr. Chaer said at the annual meeting of the Eastern Vascular Society.
Therefore, they conducted the study to quantify the risk for thoracic aneurysm in these patients and to identify risk factors that could provide screening parameters, he said. The researchers defined an aneurysm as a greater than 50% increase in the adjacent aorta diameter or a 3 cm or larger increase in the setting of AAA, Dr. Chaer said. Thoracic aneurysms were categorized by two subgroups: synchronous (occurring within 2 years of initial AAA diagnosis) and metachronous (occurring 2 years or more after diagnosis). About 11% of patients had the former, and 12.6% the latter, Dr. Chaer said. The average time to diagnosis was 2.3 years, he said.
In all, the researchers considered 2,196 patients diagnosed with AAA between 2000 and 2008, but only 49% (1,082) had chest CT that qualified them for further analysis, Dr. Chaer noted. The chest studies were conducted for suspected pulmonary disease in 74% of patients, for chest screening in 15%, and for miscellaneous reasons in 11%.
One predisposing factor for thoracic aneurysm was the type of AAA, Dr. Chaer explained. “Those patients who had a thoracic aneurysm component were more likely to have a suprarenal or juxtarenal aortic aneurysm, and those patients who did not have any thoracic aneurysm were more likely to have had an infrarenal aneurysm,” he said.
The median age of patients who had a thoracic aneurysm vs. those who did not was 76 years vs. 74 years, he said.
Other predictors for thoracic aortic aneurysm included African American race, family history of thoracic aneurysm, personal history of obesity hypertension, and an AAA diameter more than 5 cm on presentation, he said. Factors that conferred a protective effect were a diagnosis of diabetes mellitus, infrarenal AAA location, and – “counterintuitively” – a history of smoking.
“We propose that routine or targeted screening with chest CT at the time of aortic aneurysm diagnosis may be indicated, not only to really define the natural history of disease, but more importantly to try to prevent late aortic events,” Dr. Chaer said.
But Dr. James Black, of Johns Hopkins University in Baltimore, questioned the cost effectiveness of routine screening. At his institution, chest CT would add about $3,000 per patient, he said. “If you took a chest CT at diagnosis of AAA for 100 patients, 90% of the scans would be negative for thoracic aneurysm, at a rough cost in our institution of about $300,000 a year,” he said.
Cost of routine chest CT is an issue, Dr. Chaer acknowledged, although the chest CT could be done in the same scan as the abdominal CT.
“It would be nice to have a surrogate marker for thoracic aneurysm,” Dr. Chaer said. “Although we found that a thoracic aneurysm was more common in patients who had a juxtarenal aneurysm, those numbers were not hard enough to confidently say that the juxtarenal component is always predictive of a surrogate marker of thoracic aneurysm development. It is something that could be the subject of future studies.”
In addition, there is a need to identify risk factors. “We are trying to identify a high-risk group of patients in whom it would be more cost effective to screen,” he said. “That would bring down the number significantly and therefore the cost.”
Dr. Chaer noted that the heterogeneous population and the retrospective nature were limitations of the study. He reported no disclosures relevant to the presentation.
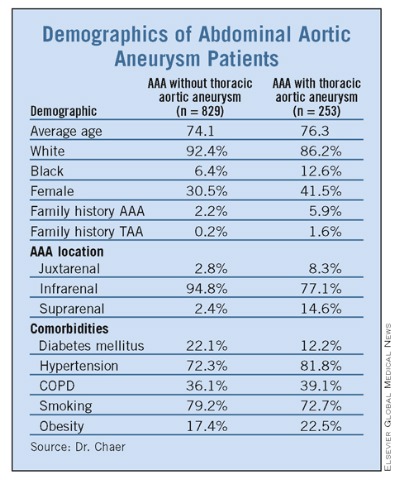
Demographics of Abdominal Aortic Aneurysm Patients
NEW YORK – About one in four patients with abdominal aortic aneurysm may be at risk for thoracic aneurysm, judging by results of a single-center retrospective study of more than 1,000 patients.
Dr. Rabih Chaer, a vascular surgeon at the University of Pittsburgh, and his colleagues found that, among 1,082 patients diagnosed with abdominal aortic aneurysms (AAA) who had chest CT at follow-up, 23.4% had some sort of thoracic aneurysm afterward.
“Despite the clinical associations that have been observed between AAAs and peripheral aneurysms and thoracic aneurysms, screening for other common aneurysms continues to be controversial,” Dr. Chaer said at the annual meeting of the Eastern Vascular Society.
Therefore, they conducted the study to quantify the risk for thoracic aneurysm in these patients and to identify risk factors that could provide screening parameters, he said. The researchers defined an aneurysm as a greater than 50% increase in the adjacent aorta diameter or a 3 cm or larger increase in the setting of AAA, Dr. Chaer said. Thoracic aneurysms were categorized by two subgroups: synchronous (occurring within 2 years of initial AAA diagnosis) and metachronous (occurring 2 years or more after diagnosis). About 11% of patients had the former, and 12.6% the latter, Dr. Chaer said. The average time to diagnosis was 2.3 years, he said.
In all, the researchers considered 2,196 patients diagnosed with AAA between 2000 and 2008, but only 49% (1,082) had chest CT that qualified them for further analysis, Dr. Chaer noted. The chest studies were conducted for suspected pulmonary disease in 74% of patients, for chest screening in 15%, and for miscellaneous reasons in 11%.
One predisposing factor for thoracic aneurysm was the type of AAA, Dr. Chaer explained. “Those patients who had a thoracic aneurysm component were more likely to have a suprarenal or juxtarenal aortic aneurysm, and those patients who did not have any thoracic aneurysm were more likely to have had an infrarenal aneurysm,” he said.
The median age of patients who had a thoracic aneurysm vs. those who did not was 76 years vs. 74 years, he said.
Other predictors for thoracic aortic aneurysm included African American race, family history of thoracic aneurysm, personal history of obesity hypertension, and an AAA diameter more than 5 cm on presentation, he said. Factors that conferred a protective effect were a diagnosis of diabetes mellitus, infrarenal AAA location, and – “counterintuitively” – a history of smoking.
“We propose that routine or targeted screening with chest CT at the time of aortic aneurysm diagnosis may be indicated, not only to really define the natural history of disease, but more importantly to try to prevent late aortic events,” Dr. Chaer said.
But Dr. James Black, of Johns Hopkins University in Baltimore, questioned the cost effectiveness of routine screening. At his institution, chest CT would add about $3,000 per patient, he said. “If you took a chest CT at diagnosis of AAA for 100 patients, 90% of the scans would be negative for thoracic aneurysm, at a rough cost in our institution of about $300,000 a year,” he said.
Cost of routine chest CT is an issue, Dr. Chaer acknowledged, although the chest CT could be done in the same scan as the abdominal CT.
“It would be nice to have a surrogate marker for thoracic aneurysm,” Dr. Chaer said. “Although we found that a thoracic aneurysm was more common in patients who had a juxtarenal aneurysm, those numbers were not hard enough to confidently say that the juxtarenal component is always predictive of a surrogate marker of thoracic aneurysm development. It is something that could be the subject of future studies.”
In addition, there is a need to identify risk factors. “We are trying to identify a high-risk group of patients in whom it would be more cost effective to screen,” he said. “That would bring down the number significantly and therefore the cost.”
Dr. Chaer noted that the heterogeneous population and the retrospective nature were limitations of the study. He reported no disclosures relevant to the presentation.
Demographics of Abdominal Aortic Aneurysm Patients
NEW YORK – About one in four patients with abdominal aortic aneurysm may be at risk for thoracic aneurysm, judging by results of a single-center retrospective study of more than 1,000 patients.
Dr. Rabih Chaer, a vascular surgeon at the University of Pittsburgh, and his colleagues found that, among 1,082 patients diagnosed with abdominal aortic aneurysms (AAA) who had chest CT at follow-up, 23.4% had some sort of thoracic aneurysm afterward.
“Despite the clinical associations that have been observed between AAAs and peripheral aneurysms and thoracic aneurysms, screening for other common aneurysms continues to be controversial,” Dr. Chaer said at the annual meeting of the Eastern Vascular Society.
Therefore, they conducted the study to quantify the risk for thoracic aneurysm in these patients and to identify risk factors that could provide screening parameters, he said. The researchers defined an aneurysm as a greater than 50% increase in the adjacent aorta diameter or a 3 cm or larger increase in the setting of AAA, Dr. Chaer said. Thoracic aneurysms were categorized by two subgroups: synchronous (occurring within 2 years of initial AAA diagnosis) and metachronous (occurring 2 years or more after diagnosis). About 11% of patients had the former, and 12.6% the latter, Dr. Chaer said. The average time to diagnosis was 2.3 years, he said.
In all, the researchers considered 2,196 patients diagnosed with AAA between 2000 and 2008, but only 49% (1,082) had chest CT that qualified them for further analysis, Dr. Chaer noted. The chest studies were conducted for suspected pulmonary disease in 74% of patients, for chest screening in 15%, and for miscellaneous reasons in 11%.
One predisposing factor for thoracic aneurysm was the type of AAA, Dr. Chaer explained. “Those patients who had a thoracic aneurysm component were more likely to have a suprarenal or juxtarenal aortic aneurysm, and those patients who did not have any thoracic aneurysm were more likely to have had an infrarenal aneurysm,” he said.
The median age of patients who had a thoracic aneurysm vs. those who did not was 76 years vs. 74 years, he said.
Other predictors for thoracic aortic aneurysm included African American race, family history of thoracic aneurysm, personal history of obesity hypertension, and an AAA diameter more than 5 cm on presentation, he said. Factors that conferred a protective effect were a diagnosis of diabetes mellitus, infrarenal AAA location, and – “counterintuitively” – a history of smoking.
“We propose that routine or targeted screening with chest CT at the time of aortic aneurysm diagnosis may be indicated, not only to really define the natural history of disease, but more importantly to try to prevent late aortic events,” Dr. Chaer said.
But Dr. James Black, of Johns Hopkins University in Baltimore, questioned the cost effectiveness of routine screening. At his institution, chest CT would add about $3,000 per patient, he said. “If you took a chest CT at diagnosis of AAA for 100 patients, 90% of the scans would be negative for thoracic aneurysm, at a rough cost in our institution of about $300,000 a year,” he said.
Cost of routine chest CT is an issue, Dr. Chaer acknowledged, although the chest CT could be done in the same scan as the abdominal CT.
“It would be nice to have a surrogate marker for thoracic aneurysm,” Dr. Chaer said. “Although we found that a thoracic aneurysm was more common in patients who had a juxtarenal aneurysm, those numbers were not hard enough to confidently say that the juxtarenal component is always predictive of a surrogate marker of thoracic aneurysm development. It is something that could be the subject of future studies.”
In addition, there is a need to identify risk factors. “We are trying to identify a high-risk group of patients in whom it would be more cost effective to screen,” he said. “That would bring down the number significantly and therefore the cost.”
Dr. Chaer noted that the heterogeneous population and the retrospective nature were limitations of the study. He reported no disclosures relevant to the presentation.
Demographics of Abdominal Aortic Aneurysm Patients
FROM THE ANNUAL MEETING OF THE EASTERN VASCULAR SOCIETY