User login
Disclaimer: This article is not intended to promote a specific company or product. Rather its purpose is to give hospitalists an overview of technological solutions available to them today.
Electronic medical records (EMR). Healthcare information technology legislation. With all the focus on ramping up technology in hospitals, are there any IT solutions specific to hospitalists? It turns out that, yes, there are several technology systems on the market today designed especially for hospital medicine groups and the physicians who work for them.
IT and the Bottom Line
David Delaney, MD, vice president and chief medical officer of technology vendor MedAptus, Inc., Boston, says his company’s most popular solution suite is “charge capture—without a doubt. If you look at it from the perspective of driving meaningful revenue, you can increase collections from $20,000-$30,000 per hospitalist. There’s very little that’s more compelling than saying you’ll get paid more for doing the same amount of work. You can use the increased revenue to pay for other applications or to help fund EMR.”
Other major players in hospital medicine applications agree: Charge capture is the biggest draw for hospital medicine groups interested in purchasing their applications. Delaney says that in hospital medicine, “Market penetration [for electronic charge capture] is small but accelerating rapidly. I’d say only about 20% of the market is using true charge capture applications.”
One of the groups within that 20% is Inpatient Management Medical Group (IMMG), Novato, Calif. Arieh Rosenbaum, MD, director of hospitalists for IMMG’s Davies Campus, convinced the group to purchase a solution suite from one of the major vendors covered in this article, arguing that the technology would improve revenues and help the group collect their own data.
“Our first purchase was the billing program,” says Dr. Rosenbaum. “This was a huge change for us; we went from physicians basically carrying pieces of paper around in our pockets to a fully electronic billing system. It definitely helped our revenue; we’ve vastly improved our ability to capture charges.”
Jeffrey D. Kin, MD, of the Fredericksburg (Va.) Hospitalist Group, agrees. His practice purchased a different charge capture product than IMMG but experienced the same results: “There are fewer errors, and our collections are going up,” he says. “There are a lot of upsides to having a computerized system. Last year we copied 80,000 pieces of paper. Not all of that was billing slips, but a lot was.”
Both groups are relatively new customers, and both plan to begin mining the data in their new systems. “We don’t want to rely on the data provided by the hospital,” says Dr. Rosenbaum. “With the information in the system, we can look at diagnoses, length of stay, all sorts of things. This can provide a way for us to prove our value to the hospital.”
Eventually, Dr. Rosenbaum would like to merge core measures into the charge capture process so hospitalists can ensure they are following best practices as they work. “It’s a way to improve ourselves,” he says.
Help for the Working Hospitalist
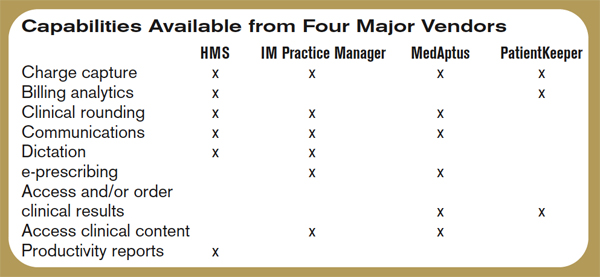
But there is much more out there besides financial tools. The four leading technology product suites examined for this article offer time-saving and efficiency-boosting utilities geared toward the working hospitalist, including the ability to call up lab results for patients, e-prescribing, integrated communication with colleagues and primary care physicians (PCPs), and much more.
“Our rounding program is helping patient care,” says Dr. Rosenbaum. “It’s the only way we round on my campus now. It’s pretty useful; the simplicity is what sold me on it, and it works concurrently with the billing [software].”
The Fredericksburg Hospitalist Group relies on communications software to alert primary care physicians when their patients are admitted and discharged. “Most [community] physicians have access to the hospital’s computer system,” explains Dr. Kin. “By our alerting them that their patient has been admitted, they can access labs, our dictations—pretty much everything. The idea is that with automatic notification, we give them a heads-up; this is a real help to us.”
Here is an overview of IT solutions that include hospitalist-specific features to spark your imagination on how technology might change your day-to-day job—and probably will.
David J. Brailer, MD, Ph, national coordinator for health information technology at the Department of Health and Human Services, will be a keynote speaker at this year’s Annual Meeting in Dallas at the Gaylord Texan Resort. Dr. Brailer is a recognized leader in the strategy and financing of quality and efficiency in healthcare. He focuses on health information technology and health systems management.
For more information on his address at the Annual Meeting, visit www.hospitalmedicine.org and click the “Events” tab on the left-hand menu.
Hospital Management System (HMS) (BMA Enterprises, Inc.)
A Web-based charge capture and primacy care physician communication system designed specifically for hospitalists, “HMS is a single product with various configuration options,” explains Dennis C. Wiltshire, president.
The charge capture software includes warning messages that alert the user to duplicate charges or missed charges. “An obvious problem with hospitalists is the way their shifts work; one rolls off the shift and another takes over the patient load,” says Wiltshire. “Each physician who sees a patient will see the patient roster with warnings, etc. For example, if, on Tuesday, Dr. Johnson admits the patient and enters the charges, and Dr. Wilson sees the same patient on Thursday and enters his charges, the missed day of service shows up. You then have to check and see what happened on Wednesday.”
As with their competitors’ charge capture programs, billing logic is used to minimize lost charges, and billing files can be created electronically.
Part of HMS’ charge capture package is a feature that allows the customer to create a “favorite list” of ICD9s and CPT codes. “The group administrator informs us of their most frequently used codes,” explains Wiltshire. Those codes are added to the favorites list. “The favorites are group-wide.”
HMS also offers a solution for built-in communication with PCPs upon their patients’ admission and discharge, along with a unique follow-up system for discharged patients.
“As soon as an admission or discharge code is entered, you’ll see a screen for additional comments,” explains Wiltshire. “The PCP information is already in the system—it’s entered upon admission—and the program generates a fax at our site. The fax is sent with customized, pertinent information.”
Why fax? “There’s an issue with e-mail: It’s not secure,” says Wiltshire. “And most PCPs are familiar and comfortable with getting faxes.”
As for follow-up after discharge, says Wiltshire, “It’s a tickler system. Upon discharge, the physician can elect whether to create a follow-up system. It might be a reminder to check the patient’s X-rays or lab results or that an appointment was made with their PCP. You can select these options to create a to-do list, and the patient won’t leave the patient roster until the list is completed.”
Whatever follow-up steps are taken can then be permanently documented and, if appropriate, faxed to the PCP to show completion.
IM Practice Manager 1.0 (Ingenious Med, Inc.)
This overall system includes clinical rounding, charge capture, communication, and business intelligence suites. Ingenious Med can aggregate data across multiple facilities, integrating with hospital EMR, information, and billing systems, enabling real-time management reports, allowing physicians to enter and access data via the Internet or mobile devices, and promoting rapid dissemination of critical information across hospital and national physician networks.
“Customers typically start off with our basic product, which is comprehensive. As the practice matures, that’s where we get customers asking for other modules,” says Steven Liu, MD, founder, CEO, chief architect, and a practicing hospitalist at Emory Eastside Medical Center, Snellville, Ga. “Our suite of products is within Practice Manager. It’s designed primarily for physician practices, which is a little different than those designed for a hospital.”
As the name implies IM Practice Manager includes tools for the practice. “As the hospitalist movement has become a bigger player, hospitalists need to prove their value,” says Dr. Liu. “We provide tools for data-mining performance. These are modeled a lot on SHM and what they state as best requirements, as well as what the individual [hospital medicine practice] requires.”
Dr. Liu stresses that they only include the features that hospitalists really need to do their jobs: “This software is designed by physicians; we don’t do technology for technology’s sake.”
IM Practice Manager offers tools for both the administrators and the hospitalists in a given group. “On the business end, business intelligence is a very important part of any practice,” says Dr. Liu. “We’ve put a lot of resources into creating a comprehensive system. Other utilities are more geared to individual physicians.”
Those utilities include communications: “You can send e-mails as long as they’re within the practice,” says Dr. Liu. “This is secure and controllable. But the system is built to help hospital medicine groups to communicate with everyone they encounter—staff, the back office, patients, and other providers.”
MedAptus Point-of-Care Solution Suite (MedAptus, Inc.)
As with its competitors, MedAptus points to the improved coding compliance, decreased administrative burden, and greatly enhanced reimbursement that result from their electronic charge capture suite.
“We send out compliance or maintenance releases annually, and a real-time call goes out over the Web when new rules are issued,” explains Dr. Delaney. The result is an automatic update for users. “It all happens behind the scenes.”
Other software features target physicians’ daily activities. “The crucial thing is to get it right from the hospitalist’s perspective,” says Dr. Delaney. “Hospital medicine differs a lot [from other physician specialties]. It tends to practices sharing groups of patients, so we have rounding lists of patients built in. Your colleague can pull up a team of patients to see changes and updates to care.”
On dictation, a feature that not all systems offer, Dr. Delaney explains, “If they’re dictating today, this is a tremendous help. It’s seamlessly integrated into the system. However, if they’re currently writing notes, this is a convenient feature, but it’s also a new expense and can add to turnaround time.”
Another feature of MedAptus—one that is unique to its product—is the Clinical Content application, which connects the user to current medical knowledge in books and publications—pre-selected by the customer group—at any point in patient interaction. “We’re very excited about this,” says Dr. Delaney. “It allows just-in-time information on specific clinical questions. It takes you to the exact information you need at any point in the process.”
The overall solution from MedAptus also includes the ability to receive lab and radiology results, as well as clinical notes, electronically at any time, anywhere. “We help leverage and extend existing IT assets in a mobile form factor,” summarizes Dr. Delaney. “We’re on version seven; we’ve had the opportunity to figure out how to fit in with a physician’s work flow.”
PatientKeeper (PatientKeeper, Inc.)
The most established software for hospitalists, PatientKeeper is a single integrated system designed to support a physician throughout the entire day. At any time, from any location, physicians can access their patients’ electronic records, write prescriptions, enter charges, dictate notes, document encounters, place orders, or send secure messages to other caregivers.
Stephen S. Hau, founder and vice president, marketing and business development, agrees that charge capture is the most requested utility. “This is a huge financial advantage for an institution, plus it increases physician satisfaction,” he says. “In three taps, you can capture a charge, and there are 900 rules [in the software] that help ensure the charge is correct and a clean bill is entered.”
But getting back to the daily tasks of hospitalists, “Our whole take is trying to fill the void where institutions have purchased information systems but there’s nothing to support the physician,” says Hau.
For example, Hau says, “One of the tasks that eats up a lot of time is finding information—the ‘chart chase,’ along with communicating with other providers. We help make it easier to send information to each other. You can send a patient-specific instant message, saying, ‘waiting on lab results for patient Molly Doe.’ Now more providers are in play per patient, so communication is more important.”
This improves patient care and even quality of life for working hospitalists. “One physician said he used to get calls at home about discharges,” recalls Hau. “Now he can access the information and discharge a patient over the phone if it’s appropriate. That shortens length of stay.”
PatientKeeper also allows individual users to customize the utility. “The exciting, challenging thing about [designing software for] physicians is that one size does not fit all,” says Hau. “One thing we provide is the ability to easily manage your own patient list; you can organize it by your schedule or by location or rounding path. We call features like that ‘physician delighters.’ These are what has made us so successful.”
Perhaps because of the physician delighters, or perhaps because they’ve been around the longest, PatientKeeper is currently the most widely used technology solution in hospital medicine. “We’re in 350 hospitals across the country, so I guess we’re the market leader,” says Hau. “We just announced two new patents, so we believe we’re also the technology leaders.”
Conclusion
Programs like the ones outlined here are definitely the future of healthcare, but the first step might be the most painful. “The investment is sizeable,” warns Dr. Rosenbaum. “The main problem is that it’s expensive. You need an upfront investment with no real guarantee of the returns.” TH
Jane Jerrard has written for The Hospitalist since 2005.
Disclaimer: This article is not intended to promote a specific company or product. Rather its purpose is to give hospitalists an overview of technological solutions available to them today.
Electronic medical records (EMR). Healthcare information technology legislation. With all the focus on ramping up technology in hospitals, are there any IT solutions specific to hospitalists? It turns out that, yes, there are several technology systems on the market today designed especially for hospital medicine groups and the physicians who work for them.
IT and the Bottom Line
David Delaney, MD, vice president and chief medical officer of technology vendor MedAptus, Inc., Boston, says his company’s most popular solution suite is “charge capture—without a doubt. If you look at it from the perspective of driving meaningful revenue, you can increase collections from $20,000-$30,000 per hospitalist. There’s very little that’s more compelling than saying you’ll get paid more for doing the same amount of work. You can use the increased revenue to pay for other applications or to help fund EMR.”
Other major players in hospital medicine applications agree: Charge capture is the biggest draw for hospital medicine groups interested in purchasing their applications. Delaney says that in hospital medicine, “Market penetration [for electronic charge capture] is small but accelerating rapidly. I’d say only about 20% of the market is using true charge capture applications.”
One of the groups within that 20% is Inpatient Management Medical Group (IMMG), Novato, Calif. Arieh Rosenbaum, MD, director of hospitalists for IMMG’s Davies Campus, convinced the group to purchase a solution suite from one of the major vendors covered in this article, arguing that the technology would improve revenues and help the group collect their own data.
“Our first purchase was the billing program,” says Dr. Rosenbaum. “This was a huge change for us; we went from physicians basically carrying pieces of paper around in our pockets to a fully electronic billing system. It definitely helped our revenue; we’ve vastly improved our ability to capture charges.”
Jeffrey D. Kin, MD, of the Fredericksburg (Va.) Hospitalist Group, agrees. His practice purchased a different charge capture product than IMMG but experienced the same results: “There are fewer errors, and our collections are going up,” he says. “There are a lot of upsides to having a computerized system. Last year we copied 80,000 pieces of paper. Not all of that was billing slips, but a lot was.”
Both groups are relatively new customers, and both plan to begin mining the data in their new systems. “We don’t want to rely on the data provided by the hospital,” says Dr. Rosenbaum. “With the information in the system, we can look at diagnoses, length of stay, all sorts of things. This can provide a way for us to prove our value to the hospital.”
Eventually, Dr. Rosenbaum would like to merge core measures into the charge capture process so hospitalists can ensure they are following best practices as they work. “It’s a way to improve ourselves,” he says.
Help for the Working Hospitalist
But there is much more out there besides financial tools. The four leading technology product suites examined for this article offer time-saving and efficiency-boosting utilities geared toward the working hospitalist, including the ability to call up lab results for patients, e-prescribing, integrated communication with colleagues and primary care physicians (PCPs), and much more.
“Our rounding program is helping patient care,” says Dr. Rosenbaum. “It’s the only way we round on my campus now. It’s pretty useful; the simplicity is what sold me on it, and it works concurrently with the billing [software].”
The Fredericksburg Hospitalist Group relies on communications software to alert primary care physicians when their patients are admitted and discharged. “Most [community] physicians have access to the hospital’s computer system,” explains Dr. Kin. “By our alerting them that their patient has been admitted, they can access labs, our dictations—pretty much everything. The idea is that with automatic notification, we give them a heads-up; this is a real help to us.”
Here is an overview of IT solutions that include hospitalist-specific features to spark your imagination on how technology might change your day-to-day job—and probably will.
David J. Brailer, MD, Ph, national coordinator for health information technology at the Department of Health and Human Services, will be a keynote speaker at this year’s Annual Meeting in Dallas at the Gaylord Texan Resort. Dr. Brailer is a recognized leader in the strategy and financing of quality and efficiency in healthcare. He focuses on health information technology and health systems management.
For more information on his address at the Annual Meeting, visit www.hospitalmedicine.org and click the “Events” tab on the left-hand menu.
Hospital Management System (HMS) (BMA Enterprises, Inc.)
A Web-based charge capture and primacy care physician communication system designed specifically for hospitalists, “HMS is a single product with various configuration options,” explains Dennis C. Wiltshire, president.
The charge capture software includes warning messages that alert the user to duplicate charges or missed charges. “An obvious problem with hospitalists is the way their shifts work; one rolls off the shift and another takes over the patient load,” says Wiltshire. “Each physician who sees a patient will see the patient roster with warnings, etc. For example, if, on Tuesday, Dr. Johnson admits the patient and enters the charges, and Dr. Wilson sees the same patient on Thursday and enters his charges, the missed day of service shows up. You then have to check and see what happened on Wednesday.”
As with their competitors’ charge capture programs, billing logic is used to minimize lost charges, and billing files can be created electronically.
Part of HMS’ charge capture package is a feature that allows the customer to create a “favorite list” of ICD9s and CPT codes. “The group administrator informs us of their most frequently used codes,” explains Wiltshire. Those codes are added to the favorites list. “The favorites are group-wide.”
HMS also offers a solution for built-in communication with PCPs upon their patients’ admission and discharge, along with a unique follow-up system for discharged patients.
“As soon as an admission or discharge code is entered, you’ll see a screen for additional comments,” explains Wiltshire. “The PCP information is already in the system—it’s entered upon admission—and the program generates a fax at our site. The fax is sent with customized, pertinent information.”
Why fax? “There’s an issue with e-mail: It’s not secure,” says Wiltshire. “And most PCPs are familiar and comfortable with getting faxes.”
As for follow-up after discharge, says Wiltshire, “It’s a tickler system. Upon discharge, the physician can elect whether to create a follow-up system. It might be a reminder to check the patient’s X-rays or lab results or that an appointment was made with their PCP. You can select these options to create a to-do list, and the patient won’t leave the patient roster until the list is completed.”
Whatever follow-up steps are taken can then be permanently documented and, if appropriate, faxed to the PCP to show completion.
IM Practice Manager 1.0 (Ingenious Med, Inc.)
This overall system includes clinical rounding, charge capture, communication, and business intelligence suites. Ingenious Med can aggregate data across multiple facilities, integrating with hospital EMR, information, and billing systems, enabling real-time management reports, allowing physicians to enter and access data via the Internet or mobile devices, and promoting rapid dissemination of critical information across hospital and national physician networks.
“Customers typically start off with our basic product, which is comprehensive. As the practice matures, that’s where we get customers asking for other modules,” says Steven Liu, MD, founder, CEO, chief architect, and a practicing hospitalist at Emory Eastside Medical Center, Snellville, Ga. “Our suite of products is within Practice Manager. It’s designed primarily for physician practices, which is a little different than those designed for a hospital.”
As the name implies IM Practice Manager includes tools for the practice. “As the hospitalist movement has become a bigger player, hospitalists need to prove their value,” says Dr. Liu. “We provide tools for data-mining performance. These are modeled a lot on SHM and what they state as best requirements, as well as what the individual [hospital medicine practice] requires.”
Dr. Liu stresses that they only include the features that hospitalists really need to do their jobs: “This software is designed by physicians; we don’t do technology for technology’s sake.”
IM Practice Manager offers tools for both the administrators and the hospitalists in a given group. “On the business end, business intelligence is a very important part of any practice,” says Dr. Liu. “We’ve put a lot of resources into creating a comprehensive system. Other utilities are more geared to individual physicians.”
Those utilities include communications: “You can send e-mails as long as they’re within the practice,” says Dr. Liu. “This is secure and controllable. But the system is built to help hospital medicine groups to communicate with everyone they encounter—staff, the back office, patients, and other providers.”
MedAptus Point-of-Care Solution Suite (MedAptus, Inc.)
As with its competitors, MedAptus points to the improved coding compliance, decreased administrative burden, and greatly enhanced reimbursement that result from their electronic charge capture suite.
“We send out compliance or maintenance releases annually, and a real-time call goes out over the Web when new rules are issued,” explains Dr. Delaney. The result is an automatic update for users. “It all happens behind the scenes.”
Other software features target physicians’ daily activities. “The crucial thing is to get it right from the hospitalist’s perspective,” says Dr. Delaney. “Hospital medicine differs a lot [from other physician specialties]. It tends to practices sharing groups of patients, so we have rounding lists of patients built in. Your colleague can pull up a team of patients to see changes and updates to care.”
On dictation, a feature that not all systems offer, Dr. Delaney explains, “If they’re dictating today, this is a tremendous help. It’s seamlessly integrated into the system. However, if they’re currently writing notes, this is a convenient feature, but it’s also a new expense and can add to turnaround time.”
Another feature of MedAptus—one that is unique to its product—is the Clinical Content application, which connects the user to current medical knowledge in books and publications—pre-selected by the customer group—at any point in patient interaction. “We’re very excited about this,” says Dr. Delaney. “It allows just-in-time information on specific clinical questions. It takes you to the exact information you need at any point in the process.”
The overall solution from MedAptus also includes the ability to receive lab and radiology results, as well as clinical notes, electronically at any time, anywhere. “We help leverage and extend existing IT assets in a mobile form factor,” summarizes Dr. Delaney. “We’re on version seven; we’ve had the opportunity to figure out how to fit in with a physician’s work flow.”
PatientKeeper (PatientKeeper, Inc.)
The most established software for hospitalists, PatientKeeper is a single integrated system designed to support a physician throughout the entire day. At any time, from any location, physicians can access their patients’ electronic records, write prescriptions, enter charges, dictate notes, document encounters, place orders, or send secure messages to other caregivers.
Stephen S. Hau, founder and vice president, marketing and business development, agrees that charge capture is the most requested utility. “This is a huge financial advantage for an institution, plus it increases physician satisfaction,” he says. “In three taps, you can capture a charge, and there are 900 rules [in the software] that help ensure the charge is correct and a clean bill is entered.”
But getting back to the daily tasks of hospitalists, “Our whole take is trying to fill the void where institutions have purchased information systems but there’s nothing to support the physician,” says Hau.
For example, Hau says, “One of the tasks that eats up a lot of time is finding information—the ‘chart chase,’ along with communicating with other providers. We help make it easier to send information to each other. You can send a patient-specific instant message, saying, ‘waiting on lab results for patient Molly Doe.’ Now more providers are in play per patient, so communication is more important.”
This improves patient care and even quality of life for working hospitalists. “One physician said he used to get calls at home about discharges,” recalls Hau. “Now he can access the information and discharge a patient over the phone if it’s appropriate. That shortens length of stay.”
PatientKeeper also allows individual users to customize the utility. “The exciting, challenging thing about [designing software for] physicians is that one size does not fit all,” says Hau. “One thing we provide is the ability to easily manage your own patient list; you can organize it by your schedule or by location or rounding path. We call features like that ‘physician delighters.’ These are what has made us so successful.”
Perhaps because of the physician delighters, or perhaps because they’ve been around the longest, PatientKeeper is currently the most widely used technology solution in hospital medicine. “We’re in 350 hospitals across the country, so I guess we’re the market leader,” says Hau. “We just announced two new patents, so we believe we’re also the technology leaders.”
Conclusion
Programs like the ones outlined here are definitely the future of healthcare, but the first step might be the most painful. “The investment is sizeable,” warns Dr. Rosenbaum. “The main problem is that it’s expensive. You need an upfront investment with no real guarantee of the returns.” TH
Jane Jerrard has written for The Hospitalist since 2005.
Disclaimer: This article is not intended to promote a specific company or product. Rather its purpose is to give hospitalists an overview of technological solutions available to them today.
Electronic medical records (EMR). Healthcare information technology legislation. With all the focus on ramping up technology in hospitals, are there any IT solutions specific to hospitalists? It turns out that, yes, there are several technology systems on the market today designed especially for hospital medicine groups and the physicians who work for them.
IT and the Bottom Line
David Delaney, MD, vice president and chief medical officer of technology vendor MedAptus, Inc., Boston, says his company’s most popular solution suite is “charge capture—without a doubt. If you look at it from the perspective of driving meaningful revenue, you can increase collections from $20,000-$30,000 per hospitalist. There’s very little that’s more compelling than saying you’ll get paid more for doing the same amount of work. You can use the increased revenue to pay for other applications or to help fund EMR.”
Other major players in hospital medicine applications agree: Charge capture is the biggest draw for hospital medicine groups interested in purchasing their applications. Delaney says that in hospital medicine, “Market penetration [for electronic charge capture] is small but accelerating rapidly. I’d say only about 20% of the market is using true charge capture applications.”
One of the groups within that 20% is Inpatient Management Medical Group (IMMG), Novato, Calif. Arieh Rosenbaum, MD, director of hospitalists for IMMG’s Davies Campus, convinced the group to purchase a solution suite from one of the major vendors covered in this article, arguing that the technology would improve revenues and help the group collect their own data.
“Our first purchase was the billing program,” says Dr. Rosenbaum. “This was a huge change for us; we went from physicians basically carrying pieces of paper around in our pockets to a fully electronic billing system. It definitely helped our revenue; we’ve vastly improved our ability to capture charges.”
Jeffrey D. Kin, MD, of the Fredericksburg (Va.) Hospitalist Group, agrees. His practice purchased a different charge capture product than IMMG but experienced the same results: “There are fewer errors, and our collections are going up,” he says. “There are a lot of upsides to having a computerized system. Last year we copied 80,000 pieces of paper. Not all of that was billing slips, but a lot was.”
Both groups are relatively new customers, and both plan to begin mining the data in their new systems. “We don’t want to rely on the data provided by the hospital,” says Dr. Rosenbaum. “With the information in the system, we can look at diagnoses, length of stay, all sorts of things. This can provide a way for us to prove our value to the hospital.”
Eventually, Dr. Rosenbaum would like to merge core measures into the charge capture process so hospitalists can ensure they are following best practices as they work. “It’s a way to improve ourselves,” he says.
Help for the Working Hospitalist
But there is much more out there besides financial tools. The four leading technology product suites examined for this article offer time-saving and efficiency-boosting utilities geared toward the working hospitalist, including the ability to call up lab results for patients, e-prescribing, integrated communication with colleagues and primary care physicians (PCPs), and much more.
“Our rounding program is helping patient care,” says Dr. Rosenbaum. “It’s the only way we round on my campus now. It’s pretty useful; the simplicity is what sold me on it, and it works concurrently with the billing [software].”
The Fredericksburg Hospitalist Group relies on communications software to alert primary care physicians when their patients are admitted and discharged. “Most [community] physicians have access to the hospital’s computer system,” explains Dr. Kin. “By our alerting them that their patient has been admitted, they can access labs, our dictations—pretty much everything. The idea is that with automatic notification, we give them a heads-up; this is a real help to us.”
Here is an overview of IT solutions that include hospitalist-specific features to spark your imagination on how technology might change your day-to-day job—and probably will.
David J. Brailer, MD, Ph, national coordinator for health information technology at the Department of Health and Human Services, will be a keynote speaker at this year’s Annual Meeting in Dallas at the Gaylord Texan Resort. Dr. Brailer is a recognized leader in the strategy and financing of quality and efficiency in healthcare. He focuses on health information technology and health systems management.
For more information on his address at the Annual Meeting, visit www.hospitalmedicine.org and click the “Events” tab on the left-hand menu.
Hospital Management System (HMS) (BMA Enterprises, Inc.)
A Web-based charge capture and primacy care physician communication system designed specifically for hospitalists, “HMS is a single product with various configuration options,” explains Dennis C. Wiltshire, president.
The charge capture software includes warning messages that alert the user to duplicate charges or missed charges. “An obvious problem with hospitalists is the way their shifts work; one rolls off the shift and another takes over the patient load,” says Wiltshire. “Each physician who sees a patient will see the patient roster with warnings, etc. For example, if, on Tuesday, Dr. Johnson admits the patient and enters the charges, and Dr. Wilson sees the same patient on Thursday and enters his charges, the missed day of service shows up. You then have to check and see what happened on Wednesday.”
As with their competitors’ charge capture programs, billing logic is used to minimize lost charges, and billing files can be created electronically.
Part of HMS’ charge capture package is a feature that allows the customer to create a “favorite list” of ICD9s and CPT codes. “The group administrator informs us of their most frequently used codes,” explains Wiltshire. Those codes are added to the favorites list. “The favorites are group-wide.”
HMS also offers a solution for built-in communication with PCPs upon their patients’ admission and discharge, along with a unique follow-up system for discharged patients.
“As soon as an admission or discharge code is entered, you’ll see a screen for additional comments,” explains Wiltshire. “The PCP information is already in the system—it’s entered upon admission—and the program generates a fax at our site. The fax is sent with customized, pertinent information.”
Why fax? “There’s an issue with e-mail: It’s not secure,” says Wiltshire. “And most PCPs are familiar and comfortable with getting faxes.”
As for follow-up after discharge, says Wiltshire, “It’s a tickler system. Upon discharge, the physician can elect whether to create a follow-up system. It might be a reminder to check the patient’s X-rays or lab results or that an appointment was made with their PCP. You can select these options to create a to-do list, and the patient won’t leave the patient roster until the list is completed.”
Whatever follow-up steps are taken can then be permanently documented and, if appropriate, faxed to the PCP to show completion.
IM Practice Manager 1.0 (Ingenious Med, Inc.)
This overall system includes clinical rounding, charge capture, communication, and business intelligence suites. Ingenious Med can aggregate data across multiple facilities, integrating with hospital EMR, information, and billing systems, enabling real-time management reports, allowing physicians to enter and access data via the Internet or mobile devices, and promoting rapid dissemination of critical information across hospital and national physician networks.
“Customers typically start off with our basic product, which is comprehensive. As the practice matures, that’s where we get customers asking for other modules,” says Steven Liu, MD, founder, CEO, chief architect, and a practicing hospitalist at Emory Eastside Medical Center, Snellville, Ga. “Our suite of products is within Practice Manager. It’s designed primarily for physician practices, which is a little different than those designed for a hospital.”
As the name implies IM Practice Manager includes tools for the practice. “As the hospitalist movement has become a bigger player, hospitalists need to prove their value,” says Dr. Liu. “We provide tools for data-mining performance. These are modeled a lot on SHM and what they state as best requirements, as well as what the individual [hospital medicine practice] requires.”
Dr. Liu stresses that they only include the features that hospitalists really need to do their jobs: “This software is designed by physicians; we don’t do technology for technology’s sake.”
IM Practice Manager offers tools for both the administrators and the hospitalists in a given group. “On the business end, business intelligence is a very important part of any practice,” says Dr. Liu. “We’ve put a lot of resources into creating a comprehensive system. Other utilities are more geared to individual physicians.”
Those utilities include communications: “You can send e-mails as long as they’re within the practice,” says Dr. Liu. “This is secure and controllable. But the system is built to help hospital medicine groups to communicate with everyone they encounter—staff, the back office, patients, and other providers.”
MedAptus Point-of-Care Solution Suite (MedAptus, Inc.)
As with its competitors, MedAptus points to the improved coding compliance, decreased administrative burden, and greatly enhanced reimbursement that result from their electronic charge capture suite.
“We send out compliance or maintenance releases annually, and a real-time call goes out over the Web when new rules are issued,” explains Dr. Delaney. The result is an automatic update for users. “It all happens behind the scenes.”
Other software features target physicians’ daily activities. “The crucial thing is to get it right from the hospitalist’s perspective,” says Dr. Delaney. “Hospital medicine differs a lot [from other physician specialties]. It tends to practices sharing groups of patients, so we have rounding lists of patients built in. Your colleague can pull up a team of patients to see changes and updates to care.”
On dictation, a feature that not all systems offer, Dr. Delaney explains, “If they’re dictating today, this is a tremendous help. It’s seamlessly integrated into the system. However, if they’re currently writing notes, this is a convenient feature, but it’s also a new expense and can add to turnaround time.”
Another feature of MedAptus—one that is unique to its product—is the Clinical Content application, which connects the user to current medical knowledge in books and publications—pre-selected by the customer group—at any point in patient interaction. “We’re very excited about this,” says Dr. Delaney. “It allows just-in-time information on specific clinical questions. It takes you to the exact information you need at any point in the process.”
The overall solution from MedAptus also includes the ability to receive lab and radiology results, as well as clinical notes, electronically at any time, anywhere. “We help leverage and extend existing IT assets in a mobile form factor,” summarizes Dr. Delaney. “We’re on version seven; we’ve had the opportunity to figure out how to fit in with a physician’s work flow.”
PatientKeeper (PatientKeeper, Inc.)
The most established software for hospitalists, PatientKeeper is a single integrated system designed to support a physician throughout the entire day. At any time, from any location, physicians can access their patients’ electronic records, write prescriptions, enter charges, dictate notes, document encounters, place orders, or send secure messages to other caregivers.
Stephen S. Hau, founder and vice president, marketing and business development, agrees that charge capture is the most requested utility. “This is a huge financial advantage for an institution, plus it increases physician satisfaction,” he says. “In three taps, you can capture a charge, and there are 900 rules [in the software] that help ensure the charge is correct and a clean bill is entered.”
But getting back to the daily tasks of hospitalists, “Our whole take is trying to fill the void where institutions have purchased information systems but there’s nothing to support the physician,” says Hau.
For example, Hau says, “One of the tasks that eats up a lot of time is finding information—the ‘chart chase,’ along with communicating with other providers. We help make it easier to send information to each other. You can send a patient-specific instant message, saying, ‘waiting on lab results for patient Molly Doe.’ Now more providers are in play per patient, so communication is more important.”
This improves patient care and even quality of life for working hospitalists. “One physician said he used to get calls at home about discharges,” recalls Hau. “Now he can access the information and discharge a patient over the phone if it’s appropriate. That shortens length of stay.”
PatientKeeper also allows individual users to customize the utility. “The exciting, challenging thing about [designing software for] physicians is that one size does not fit all,” says Hau. “One thing we provide is the ability to easily manage your own patient list; you can organize it by your schedule or by location or rounding path. We call features like that ‘physician delighters.’ These are what has made us so successful.”
Perhaps because of the physician delighters, or perhaps because they’ve been around the longest, PatientKeeper is currently the most widely used technology solution in hospital medicine. “We’re in 350 hospitals across the country, so I guess we’re the market leader,” says Hau. “We just announced two new patents, so we believe we’re also the technology leaders.”
Conclusion
Programs like the ones outlined here are definitely the future of healthcare, but the first step might be the most painful. “The investment is sizeable,” warns Dr. Rosenbaum. “The main problem is that it’s expensive. You need an upfront investment with no real guarantee of the returns.” TH
Jane Jerrard has written for The Hospitalist since 2005.