User login
ANSWER
The correct answer is Poikiloderma of Civatte (POC; choice “a”), a consequence of extensive and poorly tolerated sun exposure. Although it is the result of multiple sunburns, POC is permanently fixed to affected skin, not merely a temporary phenomenon like sunburn—so choice “b” is incorrect.
Some forms of lupus (choice “c”) present with redness, but it tends to be of acute onset (in the beginning at least) and will usually involve epidermal disturbance (eg, scaling or erosions). The condition often manifests as discrete and confluent lesions with clearing centers.
Rosacea (choice “d”) can affect the neck and face. However, it will typically wax and wane, and will often involve papules and pustules as well. By contrast, POC is basically unchanging and has no palpable component.
DISCUSSION
POC is one of many indices of dermatoheliosis (chronic sun damage) and is reportedly more common in women, although it is not at all unusual in men with a history of overexposure to ultraviolet light sources. As this case demonstrates, POC often develops so gradually that even patients with pronounced involvement of several years’ duration may not be aware of their condition until it is pointed out to them.
The history of overexposure to the sun, the photodistribution of the erythema, and the distinct sparing provided by the chin all serve to confirm the nature of the problem. So too does the presence of multiple other indices of dermatoheliosis, such as actinic keratoses, solar lentigines, weathering, and the stellate scars on the dorsal arms of older patients.
Affected patients need a thorough skin check for possible malignancies at the time of the initial visit, with arrangements made for ongoing periodic checks. Patient education on the need for better sun protection can be reinforced by providing samples of sunscreen products. The diagnosis of POC is often a shock to patients, but the occasion provides the perfect opportunity to educate them about the effects of chronic overexposure to the sun.
For pronounced cases such as this one, ablation with the appropriate laser is, by far, the most effective option. But since POC is not truly a disease, most patients are content to learn the nature of their diagnosis and their role in limiting its worsening.
ANSWER
The correct answer is Poikiloderma of Civatte (POC; choice “a”), a consequence of extensive and poorly tolerated sun exposure. Although it is the result of multiple sunburns, POC is permanently fixed to affected skin, not merely a temporary phenomenon like sunburn—so choice “b” is incorrect.
Some forms of lupus (choice “c”) present with redness, but it tends to be of acute onset (in the beginning at least) and will usually involve epidermal disturbance (eg, scaling or erosions). The condition often manifests as discrete and confluent lesions with clearing centers.
Rosacea (choice “d”) can affect the neck and face. However, it will typically wax and wane, and will often involve papules and pustules as well. By contrast, POC is basically unchanging and has no palpable component.
DISCUSSION
POC is one of many indices of dermatoheliosis (chronic sun damage) and is reportedly more common in women, although it is not at all unusual in men with a history of overexposure to ultraviolet light sources. As this case demonstrates, POC often develops so gradually that even patients with pronounced involvement of several years’ duration may not be aware of their condition until it is pointed out to them.
The history of overexposure to the sun, the photodistribution of the erythema, and the distinct sparing provided by the chin all serve to confirm the nature of the problem. So too does the presence of multiple other indices of dermatoheliosis, such as actinic keratoses, solar lentigines, weathering, and the stellate scars on the dorsal arms of older patients.
Affected patients need a thorough skin check for possible malignancies at the time of the initial visit, with arrangements made for ongoing periodic checks. Patient education on the need for better sun protection can be reinforced by providing samples of sunscreen products. The diagnosis of POC is often a shock to patients, but the occasion provides the perfect opportunity to educate them about the effects of chronic overexposure to the sun.
For pronounced cases such as this one, ablation with the appropriate laser is, by far, the most effective option. But since POC is not truly a disease, most patients are content to learn the nature of their diagnosis and their role in limiting its worsening.
ANSWER
The correct answer is Poikiloderma of Civatte (POC; choice “a”), a consequence of extensive and poorly tolerated sun exposure. Although it is the result of multiple sunburns, POC is permanently fixed to affected skin, not merely a temporary phenomenon like sunburn—so choice “b” is incorrect.
Some forms of lupus (choice “c”) present with redness, but it tends to be of acute onset (in the beginning at least) and will usually involve epidermal disturbance (eg, scaling or erosions). The condition often manifests as discrete and confluent lesions with clearing centers.
Rosacea (choice “d”) can affect the neck and face. However, it will typically wax and wane, and will often involve papules and pustules as well. By contrast, POC is basically unchanging and has no palpable component.
DISCUSSION
POC is one of many indices of dermatoheliosis (chronic sun damage) and is reportedly more common in women, although it is not at all unusual in men with a history of overexposure to ultraviolet light sources. As this case demonstrates, POC often develops so gradually that even patients with pronounced involvement of several years’ duration may not be aware of their condition until it is pointed out to them.
The history of overexposure to the sun, the photodistribution of the erythema, and the distinct sparing provided by the chin all serve to confirm the nature of the problem. So too does the presence of multiple other indices of dermatoheliosis, such as actinic keratoses, solar lentigines, weathering, and the stellate scars on the dorsal arms of older patients.
Affected patients need a thorough skin check for possible malignancies at the time of the initial visit, with arrangements made for ongoing periodic checks. Patient education on the need for better sun protection can be reinforced by providing samples of sunscreen products. The diagnosis of POC is often a shock to patients, but the occasion provides the perfect opportunity to educate them about the effects of chronic overexposure to the sun.
For pronounced cases such as this one, ablation with the appropriate laser is, by far, the most effective option. But since POC is not truly a disease, most patients are content to learn the nature of their diagnosis and their role in limiting its worsening.
A 36-year-old man urgently self-refers to dermatology for evaluation of skin changes that a friend recently noticed and promptly insisted he seek care for. The patient denies symptoms and has never had any previous medical provider comment on his skin.
He has a long history of overexposure to the sun, as an oil field worker and as a professional bass fisherman on weekends. “If the sun is up, chances are I’m out in it, seven days a week,” is how the patient puts it, adding that he knows he needs sunscreen but has just never bothered with it. At work, he is required to wear a hardhat; in his leisure time, he wears short sleeves and a ball cap, if anything, on his head.
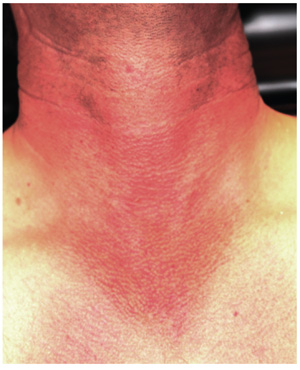
Overall, the patient looks easily 10 years older than his stated age, with splotchy, weathered skin and a very red face on which multiple actinic keratoses are readily noted. With the patient’s shirt off, the primary reason for his visit is apparent: an intensely red, sharply demarcated, blanchable macular V-shaped patch of skin that roughly coincides with the area not usually covered by his shirt. This same process extends onto his anterior neck and cheeks, becoming slightly less intense on posterior neck skin. The U-shaped area of his anterior neck (directly under his chin) is spared, with sharply defined margins between red and white skin.
Examination with 10x magnification reveals a dense mat of fine telangiectatic, blanchable blood vessels comprising the bulk of the erythema. On both sides of the anterolateral neck, rows of sharply defined, 1- to 1.5-mm whitish yellow papules can be seen, virtually covering the area. These gradually thin out, then end, as normal skin is encountered on the upper chest.
