User login
Joel Barker describes leadership as “…the ability to take people where they otherwise would not go.” In other words, leadership is about creating change in something that exists today. Management, on the other hand, may be considered a series of steps to ensure that things happen the desired and consistent way. Although this article is not of scope sufficient to explore the differences between management and leadership, it will address a domain in which the 2 intimately intersect. Managing others relies upon many foundations of leadership, such as establishing the group’s vision and setting key strategic goals. In like manner, successful leadership in stimulating change is dependent on the effective management of personnel to ensure that the culture, work habits, outcomes, and behaviors are consistent with the change efforts. This article will focus on the management of physicians in hospital medicine groups. The 8 steps outlined are applicable regardless of employer type, group size, or mission. Almost all of the skills necessary to effectively implement a performance management system can be learned and are best practiced on a regular basis. Furthermore, there are many existing resources for further education and development in these areas based on one’s current level of competency.
The author wishes to acknowledge the faculty of the American College of Physician Executives for their work in assembling many of the concepts found in this article. The course “Managing Physician Performance in Organizations” serves to underscore an integrated model of performance management and explores some of the theoretical bases of human behavior not included here.
Defining Your Group
Before you can manage performance, you must know the parameters by which the group is defined. The prerequisites for performance management include salient statements of mission, vision, and values. The mission defines the purpose for the group being in place and usually reflects the interests of the hospital(s) or medical group affiliated with or actually employing the hospital medicine group. The mission statement should be able to answer the questions “Why does our hospital medicine group exist? What purpose does it serve? In very broad terms, what scope of services do we provide?” The vision is a concise summary of what the group would like to be or achieve in the future, and it may relate to growth, range of services, outcomes, or other dimensions. Most often the vision is the leader’s platform for change in order to articulate the rationale for creating a better future. Values are those characteristics that guide decision making and provide guidance for everyone’s expected behavior and conduct in the group. Values can be thought of as the “lens” through which the vision is carried out and the mission upheld.
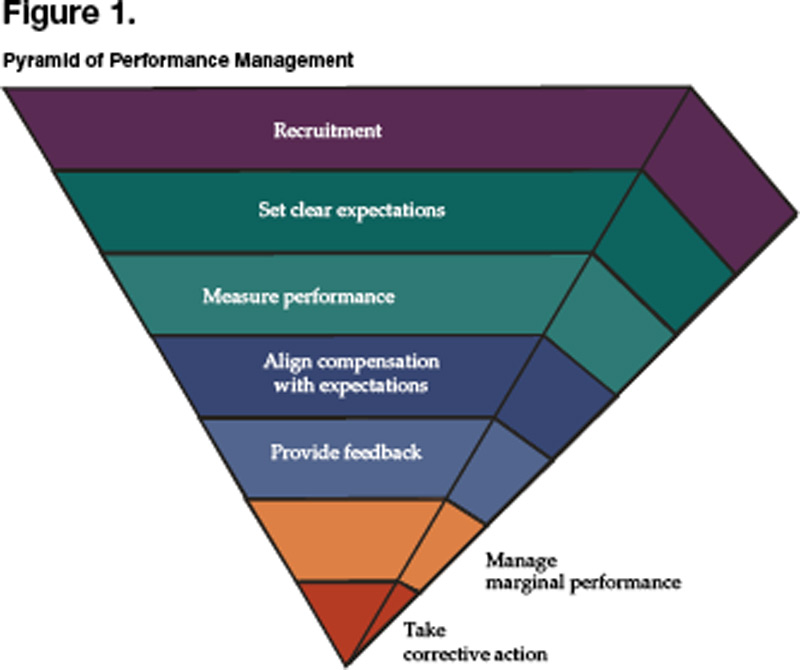
From the mission, vision, and values come strategies for achieving successful change and the more specific goals that the group is to attain. In some cases the group may have undertaken a formal strategic planning process that rendered a series of goals, objectives, and/or programs to be carried out in the immediate to intermediate term. We now reach the vital area in which a well structured and supported performance management system can play a pivotal role in ensuring the successful implementation of strategic thinking. Until now, the thought and planning process had focused on the right thing to do. From here, the focus becomes doing things right. Once you have completely answered the questions above and have a confident sense of where your group is heading and why, then the steps that follow will enable you to stack the deck in favor of achieving the level of performance you desire. Note that each step is embedded in action. Figure 1 represents the pyramid of performance management, a prioritized approach to managing others.
Recruiting the Right People
Not everyone has the luxury of personally hiring each physician in their group, much less having a surplus of candidates that are outstanding in every dimension. The reality in 2005 is that there continues to be demand for hospitalists far exceeding the available supply. This “seller’s market” (i.e., a hospitalist “sells” his or her services to an employer) represents a challenging dynamic for new or growing hospital medicine groups attempting to recruit the top candidates. It gets even worse when you consider hospital medicine as a new specialty, often finding itself in hospitals where the medical staff are skeptical or apprehensive in accepting the new group, and one bad hire can undermine the group’s chances of success. Furthermore, there may not be adequate experience or expertise in recruiting new physicians or correctly identifying those who would be a proper fit for the group. So how does one go about recruiting the right people?
Planning begins with having defined the group in terms of the mission and values. Knowing the vision and specific strategies to be employed lends insight into what type of individual would best fit with the needs and culture of the group. It is important to list the desired qualities on paper and plan for assessing each one, knowing that there is no perfect candidate and these characteristics must therefore be prioritized. Remember, what makes a good hospitalist in your group does not mean they will be good somewhere else; be sure you define very clearly what exactly “good” means. At the same time, it is also critical to outline the selling points of potentially joining your group in terms of 3 areas: the practice itself, compensation, and location.
The next step consists of preparing a slate of candidates for interviews. There are many methods of finding (i.e., sourcing) strong candidates, one of the best of which is to ask members of your current group or other trusted colleagues for referrals. If you are interested in filling a position with a more specific skill set such as information technology, palliative care, or clinical teaching, then a “make or buy” decision needs to be made to either recruit for the individual already in possession of such credentials or to hire more generically and then train accordingly. Once candidates are identified, a deliberate process of reviewing their written materials and interviewing them by telephone will determine the appropriateness of an in person interview. Speaking with references can occur at any time, and some advocate for this to occur prior to bringing a candidate for formal interview, as another mechanism of screening and to focus interview questions on site. The formal interview itself should be well structured and enable your key stakeholders to meet with the candidate and submit an immediate assessment. The shorter the turnaround time to extend an offer, the more decisive and committed to the candidate you will appear. Likewise, if you have a diverse composition of interviewers who weigh in with their perspectives, then there should be little to delay a hiring decision.
There are 3 additional points to remember when looking to hire an additional hospitalist into your group. First, it is estimated that 70% of physicians who leave a job do so because of spousal discontent. To mitigate this possibility, invite the spouse to accompany the candidate to the interview location, and assemble a parallel agenda for him or her.. Do not consider yourself on a “best behavior” basis during courtship alone; you need to continue nurturing the candidate and family well into the first year of employment to ensure a good transition. Second, be realistic about your expectations. There is no perfect candidate, so you must prioritize those qualities you want most from them. If you wait for perfection, the delay will cause you to overlook many very good physicians. Finally, take another look at the performance management pyramid. The reason the area for recruitment is so large is because of the disproportionate amount of time that one should invest in recruitment processes. Hiring the right people up front will make the rest of the steps far easier and minimize the likelihood of your being drawn into the nadir of the pyramid.
Setting Clear Expectations
Do you have a job description? When you read it, does it adequately describe what is expected of your hospitalists? Do you have an orientation for new members to your group? How long does it last? Is additional training offered? Are there outcomes that you expect from this training? And once you have oriented, trained, and offered a job description, does the actual work environment support or negate your efforts―i.e., does culture trump your formal process?
The cycle of setting clear expectations about work performance begins during the recruitment phase. Being absolutely forthcoming about what it is like to work in your group and what you expect from each and every member is paramount to allow both you and the candidate to determine a good fit. Once the physician has joined your group, orientation and training should hardly be a 1-, 2- or 3-day exercise. These are continuous and ongoing processes, given our rapidly changing practice environment. In fact, change is one of the only reliable characteristics of what we do, and extending the welcome “The job you take today is unlikely to be the job you will have next year” is hardly inappropriate. Be mindful that setting clear expectations with all of your hospitalists is the bedrock of a functional performance management system. Defining expectations alone will often improve performance, vis-à-vis the Hawthorne effect.
Expectations should always be depersonalized and focus on behavior. Behavior itself may be regarded in 2 distinct domains: those behaviors that are observed, and those outcomes that are measurable. Examples of observable behaviors include interpersonal interactions with nurses and consultants, pager response times, and attendance at monthly team meetings. Measurable outcomes include work RVU productivity, patient satisfaction, readmission rates, and compliance with coding and documentation guidelines. There are many ways to organize dimensions of performance that you may expect from your physicians―the 6 aims of quality (safe, timely, effective, efficient, equitable, and patient centered, as outlined in the IOM report Crossing the Quality Chasm), maintenance of a healthy workplace, citizenship, relationships with others, etc.―yet the key is to define and communicate them, then check often for understanding.
Measuring Actual Performance
Be the first to admit “the numbers are wrong,” and you will save hearing it from many others. There are many inherent problems in measuring actual performance, and the data may never be perfect. As an exercise, try assigning individual readmission rates within your group, and you will find that because of handoffs within the group and lack of precision in identifying who actually discharged the patient, there will be many arguments over whether the data is valid. However, in most circumstances, if the data is flawed, it still may serve a strong purpose to highlight the relative variation within the group. Searching for quantifiable systemic data and being transparent about the limitations of the data will be an exercise worth undertaking. In like manner, behavioral observation data are potentially fraught with conflict if the data are focused on judgment of character traits (I believe this hospitalist has a good bedside manner) rather than on observable behaviors (This hospitalist always/sometimes/never comes to meetings on time). Measures are best when they are objective, relevant to the position, and interpretable. Remember: All measures are flawed; some are useful.
Aligning Compensation With Expectations
Conventional wisdom states that people will do more of what they are incentivized to do. The corollary to this is to be sure what you incentivize is actually what you want. For the group that is trying to improve individual productivity and reduce length of stay, providing financial rewards for work RVU’s alone may result in less assertiveness in managing timely discharges and bickering over who picks up the 11 p.m. vs. 2 a.m. overnight admission the following morning. Ultimately, compensation must be intimately linked with the mission of the group, and tremendous care must be taken in determining the construct of any system. Although it is well beyond the scope of this article to detail the many considerations of designing a compensation system, one must understand that it is only one component―and not the most important component―of a performance management program.
Here are a few points to consider as you integrate your compensation system into the rest of the steps in the pyramid:
- A straight salary with or without a “guaranteed” bonus is unlikely to reward or motivate any new behaviors.
- For a performance-based compensation plan to have sufficient impact, at least 20%–30% of compensation must be tied to performance.
- Consider having both group and individual measures as part of your plan to engender a sense of teamwork and collective effort in performing well.
- Limit the number of variables in the plan to 3–5; otherwise, measures are too diluted to carry meaningful weight.
- Perform a local market comparison for benchmarking your goal median compensation; often administrative staff are more willing to share this information with other administrative staff if the understanding is that all market results will be shared.
- The process of constructing or evolving your plan, being inclusive of members of your group as well as any group sponsors, ends up being far more valuable than the final plan itself.
Providing Regular Feedback
Have you ever had a complaint that sounded like “I get way too much feedback around here?” Probably not. More likely is the case that your hospitalists wonder how they stand in terms of being compared to others and to themselves over time. The creed “no news must be good news” is hardly supportive of promoting top performance. Feedback itself can be highly influential and reflects the expectations explained by the group leader. Expectations not measured or fed back to the individual hospitalists will be expectations soon forgotten or ignored, because they may be felt not to matter.
Effective feedback is both formal and informal. The annual performance review is a common example of the former, but it is in no way meant to be the only feedback a hospitalist should receive, nor is it the most powerful. The annual review should be well structured, can outline longer term goals and ideas for self-improvement, and may serve in some key administrative functions like compensation and promotion. Informal, regular feedback, however, may serve you much better in driving performance, because it is timelier, more relevant to daily work, and more specific to the individual. Individuals also respond much more constructively to positive feedback, and some experts believe the ratio of positive to negative feedback should be on the order of 9 to 1. Be sure that feedback is done in a coaching manner and focuses on the behavior (You may try sitting down when you talk with patients as a way of making them feel more at ease) rather than on the person themselves (You’re really not a good communicator).
Managing Marginal Performance
Marginal performance can be defined as a physician whose observed behaviors or measured outcomes are at significant variance from what is expected. This pattern takes place over time and happens in spite of having in place all the other elements of a performance management system. Consider the “clock puncher” who rarely helps out the rest of the team on busy days and never shows up to group meetings or committees. Or the “tortoise” that has wonderful staff relations but chronically arrives at work late and repeatedly forgets to submit inpatient charges. Then there’s the “hothead” who is clinically adept and has high patient satisfaction but loses his or her temper with nursing and is pervasively confrontational with consultants. The steps to be taken in these and other cases like them include ensuring adequate documentation, reaching an agreement with the individual in recognizing that there is a problem, generating options for causality, negotiating a contract for improvement, and then letting future behavior determine the consequences.
Taking Corrective Action
Sometimes you simply cannot fix everything, and you need to be easy on yourself for having reached the point where the situation is no longer remediable in spite of your best efforts. In the end, everyone will be better off. When physician conduct becomes detrimental to patient safety, staff safety or quality patient care; is disruptive to the organization; or is otherwise chronically aberrant, then it is time to take adverse action. Since there are many pitfalls that have HR and legal implications, it is advisable to consult with relevant personnel to avoid problems with inadequate documentation and the potential need to report actions to state agencies and the National Practitioner Data Bank (per the Healthcare Quality Improvement Act of 1986).
Resources
- Ury W, Fisher R. Getting to Yes: Negotiating Agreement Without Giving In. 2nd ed. New York: Penguin Books; 1991.
- Reinertsen J. Physicians as leaders in the improvement of health care systems. Ann Intern Med. 1998;128:833-8.
- Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
- American College of Physician Executives. Managing Physician Performance in Organizations. Ongoing courses available at www.acpe.org.
Joel Barker describes leadership as “…the ability to take people where they otherwise would not go.” In other words, leadership is about creating change in something that exists today. Management, on the other hand, may be considered a series of steps to ensure that things happen the desired and consistent way. Although this article is not of scope sufficient to explore the differences between management and leadership, it will address a domain in which the 2 intimately intersect. Managing others relies upon many foundations of leadership, such as establishing the group’s vision and setting key strategic goals. In like manner, successful leadership in stimulating change is dependent on the effective management of personnel to ensure that the culture, work habits, outcomes, and behaviors are consistent with the change efforts. This article will focus on the management of physicians in hospital medicine groups. The 8 steps outlined are applicable regardless of employer type, group size, or mission. Almost all of the skills necessary to effectively implement a performance management system can be learned and are best practiced on a regular basis. Furthermore, there are many existing resources for further education and development in these areas based on one’s current level of competency.
The author wishes to acknowledge the faculty of the American College of Physician Executives for their work in assembling many of the concepts found in this article. The course “Managing Physician Performance in Organizations” serves to underscore an integrated model of performance management and explores some of the theoretical bases of human behavior not included here.
Defining Your Group
Before you can manage performance, you must know the parameters by which the group is defined. The prerequisites for performance management include salient statements of mission, vision, and values. The mission defines the purpose for the group being in place and usually reflects the interests of the hospital(s) or medical group affiliated with or actually employing the hospital medicine group. The mission statement should be able to answer the questions “Why does our hospital medicine group exist? What purpose does it serve? In very broad terms, what scope of services do we provide?” The vision is a concise summary of what the group would like to be or achieve in the future, and it may relate to growth, range of services, outcomes, or other dimensions. Most often the vision is the leader’s platform for change in order to articulate the rationale for creating a better future. Values are those characteristics that guide decision making and provide guidance for everyone’s expected behavior and conduct in the group. Values can be thought of as the “lens” through which the vision is carried out and the mission upheld.
From the mission, vision, and values come strategies for achieving successful change and the more specific goals that the group is to attain. In some cases the group may have undertaken a formal strategic planning process that rendered a series of goals, objectives, and/or programs to be carried out in the immediate to intermediate term. We now reach the vital area in which a well structured and supported performance management system can play a pivotal role in ensuring the successful implementation of strategic thinking. Until now, the thought and planning process had focused on the right thing to do. From here, the focus becomes doing things right. Once you have completely answered the questions above and have a confident sense of where your group is heading and why, then the steps that follow will enable you to stack the deck in favor of achieving the level of performance you desire. Note that each step is embedded in action. Figure 1 represents the pyramid of performance management, a prioritized approach to managing others.
Recruiting the Right People
Not everyone has the luxury of personally hiring each physician in their group, much less having a surplus of candidates that are outstanding in every dimension. The reality in 2005 is that there continues to be demand for hospitalists far exceeding the available supply. This “seller’s market” (i.e., a hospitalist “sells” his or her services to an employer) represents a challenging dynamic for new or growing hospital medicine groups attempting to recruit the top candidates. It gets even worse when you consider hospital medicine as a new specialty, often finding itself in hospitals where the medical staff are skeptical or apprehensive in accepting the new group, and one bad hire can undermine the group’s chances of success. Furthermore, there may not be adequate experience or expertise in recruiting new physicians or correctly identifying those who would be a proper fit for the group. So how does one go about recruiting the right people?
Planning begins with having defined the group in terms of the mission and values. Knowing the vision and specific strategies to be employed lends insight into what type of individual would best fit with the needs and culture of the group. It is important to list the desired qualities on paper and plan for assessing each one, knowing that there is no perfect candidate and these characteristics must therefore be prioritized. Remember, what makes a good hospitalist in your group does not mean they will be good somewhere else; be sure you define very clearly what exactly “good” means. At the same time, it is also critical to outline the selling points of potentially joining your group in terms of 3 areas: the practice itself, compensation, and location.
The next step consists of preparing a slate of candidates for interviews. There are many methods of finding (i.e., sourcing) strong candidates, one of the best of which is to ask members of your current group or other trusted colleagues for referrals. If you are interested in filling a position with a more specific skill set such as information technology, palliative care, or clinical teaching, then a “make or buy” decision needs to be made to either recruit for the individual already in possession of such credentials or to hire more generically and then train accordingly. Once candidates are identified, a deliberate process of reviewing their written materials and interviewing them by telephone will determine the appropriateness of an in person interview. Speaking with references can occur at any time, and some advocate for this to occur prior to bringing a candidate for formal interview, as another mechanism of screening and to focus interview questions on site. The formal interview itself should be well structured and enable your key stakeholders to meet with the candidate and submit an immediate assessment. The shorter the turnaround time to extend an offer, the more decisive and committed to the candidate you will appear. Likewise, if you have a diverse composition of interviewers who weigh in with their perspectives, then there should be little to delay a hiring decision.
There are 3 additional points to remember when looking to hire an additional hospitalist into your group. First, it is estimated that 70% of physicians who leave a job do so because of spousal discontent. To mitigate this possibility, invite the spouse to accompany the candidate to the interview location, and assemble a parallel agenda for him or her.. Do not consider yourself on a “best behavior” basis during courtship alone; you need to continue nurturing the candidate and family well into the first year of employment to ensure a good transition. Second, be realistic about your expectations. There is no perfect candidate, so you must prioritize those qualities you want most from them. If you wait for perfection, the delay will cause you to overlook many very good physicians. Finally, take another look at the performance management pyramid. The reason the area for recruitment is so large is because of the disproportionate amount of time that one should invest in recruitment processes. Hiring the right people up front will make the rest of the steps far easier and minimize the likelihood of your being drawn into the nadir of the pyramid.
Setting Clear Expectations
Do you have a job description? When you read it, does it adequately describe what is expected of your hospitalists? Do you have an orientation for new members to your group? How long does it last? Is additional training offered? Are there outcomes that you expect from this training? And once you have oriented, trained, and offered a job description, does the actual work environment support or negate your efforts―i.e., does culture trump your formal process?
The cycle of setting clear expectations about work performance begins during the recruitment phase. Being absolutely forthcoming about what it is like to work in your group and what you expect from each and every member is paramount to allow both you and the candidate to determine a good fit. Once the physician has joined your group, orientation and training should hardly be a 1-, 2- or 3-day exercise. These are continuous and ongoing processes, given our rapidly changing practice environment. In fact, change is one of the only reliable characteristics of what we do, and extending the welcome “The job you take today is unlikely to be the job you will have next year” is hardly inappropriate. Be mindful that setting clear expectations with all of your hospitalists is the bedrock of a functional performance management system. Defining expectations alone will often improve performance, vis-à-vis the Hawthorne effect.
Expectations should always be depersonalized and focus on behavior. Behavior itself may be regarded in 2 distinct domains: those behaviors that are observed, and those outcomes that are measurable. Examples of observable behaviors include interpersonal interactions with nurses and consultants, pager response times, and attendance at monthly team meetings. Measurable outcomes include work RVU productivity, patient satisfaction, readmission rates, and compliance with coding and documentation guidelines. There are many ways to organize dimensions of performance that you may expect from your physicians―the 6 aims of quality (safe, timely, effective, efficient, equitable, and patient centered, as outlined in the IOM report Crossing the Quality Chasm), maintenance of a healthy workplace, citizenship, relationships with others, etc.―yet the key is to define and communicate them, then check often for understanding.
Measuring Actual Performance
Be the first to admit “the numbers are wrong,” and you will save hearing it from many others. There are many inherent problems in measuring actual performance, and the data may never be perfect. As an exercise, try assigning individual readmission rates within your group, and you will find that because of handoffs within the group and lack of precision in identifying who actually discharged the patient, there will be many arguments over whether the data is valid. However, in most circumstances, if the data is flawed, it still may serve a strong purpose to highlight the relative variation within the group. Searching for quantifiable systemic data and being transparent about the limitations of the data will be an exercise worth undertaking. In like manner, behavioral observation data are potentially fraught with conflict if the data are focused on judgment of character traits (I believe this hospitalist has a good bedside manner) rather than on observable behaviors (This hospitalist always/sometimes/never comes to meetings on time). Measures are best when they are objective, relevant to the position, and interpretable. Remember: All measures are flawed; some are useful.
Aligning Compensation With Expectations
Conventional wisdom states that people will do more of what they are incentivized to do. The corollary to this is to be sure what you incentivize is actually what you want. For the group that is trying to improve individual productivity and reduce length of stay, providing financial rewards for work RVU’s alone may result in less assertiveness in managing timely discharges and bickering over who picks up the 11 p.m. vs. 2 a.m. overnight admission the following morning. Ultimately, compensation must be intimately linked with the mission of the group, and tremendous care must be taken in determining the construct of any system. Although it is well beyond the scope of this article to detail the many considerations of designing a compensation system, one must understand that it is only one component―and not the most important component―of a performance management program.
Here are a few points to consider as you integrate your compensation system into the rest of the steps in the pyramid:
- A straight salary with or without a “guaranteed” bonus is unlikely to reward or motivate any new behaviors.
- For a performance-based compensation plan to have sufficient impact, at least 20%–30% of compensation must be tied to performance.
- Consider having both group and individual measures as part of your plan to engender a sense of teamwork and collective effort in performing well.
- Limit the number of variables in the plan to 3–5; otherwise, measures are too diluted to carry meaningful weight.
- Perform a local market comparison for benchmarking your goal median compensation; often administrative staff are more willing to share this information with other administrative staff if the understanding is that all market results will be shared.
- The process of constructing or evolving your plan, being inclusive of members of your group as well as any group sponsors, ends up being far more valuable than the final plan itself.
Providing Regular Feedback
Have you ever had a complaint that sounded like “I get way too much feedback around here?” Probably not. More likely is the case that your hospitalists wonder how they stand in terms of being compared to others and to themselves over time. The creed “no news must be good news” is hardly supportive of promoting top performance. Feedback itself can be highly influential and reflects the expectations explained by the group leader. Expectations not measured or fed back to the individual hospitalists will be expectations soon forgotten or ignored, because they may be felt not to matter.
Effective feedback is both formal and informal. The annual performance review is a common example of the former, but it is in no way meant to be the only feedback a hospitalist should receive, nor is it the most powerful. The annual review should be well structured, can outline longer term goals and ideas for self-improvement, and may serve in some key administrative functions like compensation and promotion. Informal, regular feedback, however, may serve you much better in driving performance, because it is timelier, more relevant to daily work, and more specific to the individual. Individuals also respond much more constructively to positive feedback, and some experts believe the ratio of positive to negative feedback should be on the order of 9 to 1. Be sure that feedback is done in a coaching manner and focuses on the behavior (You may try sitting down when you talk with patients as a way of making them feel more at ease) rather than on the person themselves (You’re really not a good communicator).
Managing Marginal Performance
Marginal performance can be defined as a physician whose observed behaviors or measured outcomes are at significant variance from what is expected. This pattern takes place over time and happens in spite of having in place all the other elements of a performance management system. Consider the “clock puncher” who rarely helps out the rest of the team on busy days and never shows up to group meetings or committees. Or the “tortoise” that has wonderful staff relations but chronically arrives at work late and repeatedly forgets to submit inpatient charges. Then there’s the “hothead” who is clinically adept and has high patient satisfaction but loses his or her temper with nursing and is pervasively confrontational with consultants. The steps to be taken in these and other cases like them include ensuring adequate documentation, reaching an agreement with the individual in recognizing that there is a problem, generating options for causality, negotiating a contract for improvement, and then letting future behavior determine the consequences.
Taking Corrective Action
Sometimes you simply cannot fix everything, and you need to be easy on yourself for having reached the point where the situation is no longer remediable in spite of your best efforts. In the end, everyone will be better off. When physician conduct becomes detrimental to patient safety, staff safety or quality patient care; is disruptive to the organization; or is otherwise chronically aberrant, then it is time to take adverse action. Since there are many pitfalls that have HR and legal implications, it is advisable to consult with relevant personnel to avoid problems with inadequate documentation and the potential need to report actions to state agencies and the National Practitioner Data Bank (per the Healthcare Quality Improvement Act of 1986).
Resources
- Ury W, Fisher R. Getting to Yes: Negotiating Agreement Without Giving In. 2nd ed. New York: Penguin Books; 1991.
- Reinertsen J. Physicians as leaders in the improvement of health care systems. Ann Intern Med. 1998;128:833-8.
- Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
- American College of Physician Executives. Managing Physician Performance in Organizations. Ongoing courses available at www.acpe.org.
Joel Barker describes leadership as “…the ability to take people where they otherwise would not go.” In other words, leadership is about creating change in something that exists today. Management, on the other hand, may be considered a series of steps to ensure that things happen the desired and consistent way. Although this article is not of scope sufficient to explore the differences between management and leadership, it will address a domain in which the 2 intimately intersect. Managing others relies upon many foundations of leadership, such as establishing the group’s vision and setting key strategic goals. In like manner, successful leadership in stimulating change is dependent on the effective management of personnel to ensure that the culture, work habits, outcomes, and behaviors are consistent with the change efforts. This article will focus on the management of physicians in hospital medicine groups. The 8 steps outlined are applicable regardless of employer type, group size, or mission. Almost all of the skills necessary to effectively implement a performance management system can be learned and are best practiced on a regular basis. Furthermore, there are many existing resources for further education and development in these areas based on one’s current level of competency.
The author wishes to acknowledge the faculty of the American College of Physician Executives for their work in assembling many of the concepts found in this article. The course “Managing Physician Performance in Organizations” serves to underscore an integrated model of performance management and explores some of the theoretical bases of human behavior not included here.
Defining Your Group
Before you can manage performance, you must know the parameters by which the group is defined. The prerequisites for performance management include salient statements of mission, vision, and values. The mission defines the purpose for the group being in place and usually reflects the interests of the hospital(s) or medical group affiliated with or actually employing the hospital medicine group. The mission statement should be able to answer the questions “Why does our hospital medicine group exist? What purpose does it serve? In very broad terms, what scope of services do we provide?” The vision is a concise summary of what the group would like to be or achieve in the future, and it may relate to growth, range of services, outcomes, or other dimensions. Most often the vision is the leader’s platform for change in order to articulate the rationale for creating a better future. Values are those characteristics that guide decision making and provide guidance for everyone’s expected behavior and conduct in the group. Values can be thought of as the “lens” through which the vision is carried out and the mission upheld.
From the mission, vision, and values come strategies for achieving successful change and the more specific goals that the group is to attain. In some cases the group may have undertaken a formal strategic planning process that rendered a series of goals, objectives, and/or programs to be carried out in the immediate to intermediate term. We now reach the vital area in which a well structured and supported performance management system can play a pivotal role in ensuring the successful implementation of strategic thinking. Until now, the thought and planning process had focused on the right thing to do. From here, the focus becomes doing things right. Once you have completely answered the questions above and have a confident sense of where your group is heading and why, then the steps that follow will enable you to stack the deck in favor of achieving the level of performance you desire. Note that each step is embedded in action. Figure 1 represents the pyramid of performance management, a prioritized approach to managing others.
Recruiting the Right People
Not everyone has the luxury of personally hiring each physician in their group, much less having a surplus of candidates that are outstanding in every dimension. The reality in 2005 is that there continues to be demand for hospitalists far exceeding the available supply. This “seller’s market” (i.e., a hospitalist “sells” his or her services to an employer) represents a challenging dynamic for new or growing hospital medicine groups attempting to recruit the top candidates. It gets even worse when you consider hospital medicine as a new specialty, often finding itself in hospitals where the medical staff are skeptical or apprehensive in accepting the new group, and one bad hire can undermine the group’s chances of success. Furthermore, there may not be adequate experience or expertise in recruiting new physicians or correctly identifying those who would be a proper fit for the group. So how does one go about recruiting the right people?
Planning begins with having defined the group in terms of the mission and values. Knowing the vision and specific strategies to be employed lends insight into what type of individual would best fit with the needs and culture of the group. It is important to list the desired qualities on paper and plan for assessing each one, knowing that there is no perfect candidate and these characteristics must therefore be prioritized. Remember, what makes a good hospitalist in your group does not mean they will be good somewhere else; be sure you define very clearly what exactly “good” means. At the same time, it is also critical to outline the selling points of potentially joining your group in terms of 3 areas: the practice itself, compensation, and location.
The next step consists of preparing a slate of candidates for interviews. There are many methods of finding (i.e., sourcing) strong candidates, one of the best of which is to ask members of your current group or other trusted colleagues for referrals. If you are interested in filling a position with a more specific skill set such as information technology, palliative care, or clinical teaching, then a “make or buy” decision needs to be made to either recruit for the individual already in possession of such credentials or to hire more generically and then train accordingly. Once candidates are identified, a deliberate process of reviewing their written materials and interviewing them by telephone will determine the appropriateness of an in person interview. Speaking with references can occur at any time, and some advocate for this to occur prior to bringing a candidate for formal interview, as another mechanism of screening and to focus interview questions on site. The formal interview itself should be well structured and enable your key stakeholders to meet with the candidate and submit an immediate assessment. The shorter the turnaround time to extend an offer, the more decisive and committed to the candidate you will appear. Likewise, if you have a diverse composition of interviewers who weigh in with their perspectives, then there should be little to delay a hiring decision.
There are 3 additional points to remember when looking to hire an additional hospitalist into your group. First, it is estimated that 70% of physicians who leave a job do so because of spousal discontent. To mitigate this possibility, invite the spouse to accompany the candidate to the interview location, and assemble a parallel agenda for him or her.. Do not consider yourself on a “best behavior” basis during courtship alone; you need to continue nurturing the candidate and family well into the first year of employment to ensure a good transition. Second, be realistic about your expectations. There is no perfect candidate, so you must prioritize those qualities you want most from them. If you wait for perfection, the delay will cause you to overlook many very good physicians. Finally, take another look at the performance management pyramid. The reason the area for recruitment is so large is because of the disproportionate amount of time that one should invest in recruitment processes. Hiring the right people up front will make the rest of the steps far easier and minimize the likelihood of your being drawn into the nadir of the pyramid.
Setting Clear Expectations
Do you have a job description? When you read it, does it adequately describe what is expected of your hospitalists? Do you have an orientation for new members to your group? How long does it last? Is additional training offered? Are there outcomes that you expect from this training? And once you have oriented, trained, and offered a job description, does the actual work environment support or negate your efforts―i.e., does culture trump your formal process?
The cycle of setting clear expectations about work performance begins during the recruitment phase. Being absolutely forthcoming about what it is like to work in your group and what you expect from each and every member is paramount to allow both you and the candidate to determine a good fit. Once the physician has joined your group, orientation and training should hardly be a 1-, 2- or 3-day exercise. These are continuous and ongoing processes, given our rapidly changing practice environment. In fact, change is one of the only reliable characteristics of what we do, and extending the welcome “The job you take today is unlikely to be the job you will have next year” is hardly inappropriate. Be mindful that setting clear expectations with all of your hospitalists is the bedrock of a functional performance management system. Defining expectations alone will often improve performance, vis-à-vis the Hawthorne effect.
Expectations should always be depersonalized and focus on behavior. Behavior itself may be regarded in 2 distinct domains: those behaviors that are observed, and those outcomes that are measurable. Examples of observable behaviors include interpersonal interactions with nurses and consultants, pager response times, and attendance at monthly team meetings. Measurable outcomes include work RVU productivity, patient satisfaction, readmission rates, and compliance with coding and documentation guidelines. There are many ways to organize dimensions of performance that you may expect from your physicians―the 6 aims of quality (safe, timely, effective, efficient, equitable, and patient centered, as outlined in the IOM report Crossing the Quality Chasm), maintenance of a healthy workplace, citizenship, relationships with others, etc.―yet the key is to define and communicate them, then check often for understanding.
Measuring Actual Performance
Be the first to admit “the numbers are wrong,” and you will save hearing it from many others. There are many inherent problems in measuring actual performance, and the data may never be perfect. As an exercise, try assigning individual readmission rates within your group, and you will find that because of handoffs within the group and lack of precision in identifying who actually discharged the patient, there will be many arguments over whether the data is valid. However, in most circumstances, if the data is flawed, it still may serve a strong purpose to highlight the relative variation within the group. Searching for quantifiable systemic data and being transparent about the limitations of the data will be an exercise worth undertaking. In like manner, behavioral observation data are potentially fraught with conflict if the data are focused on judgment of character traits (I believe this hospitalist has a good bedside manner) rather than on observable behaviors (This hospitalist always/sometimes/never comes to meetings on time). Measures are best when they are objective, relevant to the position, and interpretable. Remember: All measures are flawed; some are useful.
Aligning Compensation With Expectations
Conventional wisdom states that people will do more of what they are incentivized to do. The corollary to this is to be sure what you incentivize is actually what you want. For the group that is trying to improve individual productivity and reduce length of stay, providing financial rewards for work RVU’s alone may result in less assertiveness in managing timely discharges and bickering over who picks up the 11 p.m. vs. 2 a.m. overnight admission the following morning. Ultimately, compensation must be intimately linked with the mission of the group, and tremendous care must be taken in determining the construct of any system. Although it is well beyond the scope of this article to detail the many considerations of designing a compensation system, one must understand that it is only one component―and not the most important component―of a performance management program.
Here are a few points to consider as you integrate your compensation system into the rest of the steps in the pyramid:
- A straight salary with or without a “guaranteed” bonus is unlikely to reward or motivate any new behaviors.
- For a performance-based compensation plan to have sufficient impact, at least 20%–30% of compensation must be tied to performance.
- Consider having both group and individual measures as part of your plan to engender a sense of teamwork and collective effort in performing well.
- Limit the number of variables in the plan to 3–5; otherwise, measures are too diluted to carry meaningful weight.
- Perform a local market comparison for benchmarking your goal median compensation; often administrative staff are more willing to share this information with other administrative staff if the understanding is that all market results will be shared.
- The process of constructing or evolving your plan, being inclusive of members of your group as well as any group sponsors, ends up being far more valuable than the final plan itself.
Providing Regular Feedback
Have you ever had a complaint that sounded like “I get way too much feedback around here?” Probably not. More likely is the case that your hospitalists wonder how they stand in terms of being compared to others and to themselves over time. The creed “no news must be good news” is hardly supportive of promoting top performance. Feedback itself can be highly influential and reflects the expectations explained by the group leader. Expectations not measured or fed back to the individual hospitalists will be expectations soon forgotten or ignored, because they may be felt not to matter.
Effective feedback is both formal and informal. The annual performance review is a common example of the former, but it is in no way meant to be the only feedback a hospitalist should receive, nor is it the most powerful. The annual review should be well structured, can outline longer term goals and ideas for self-improvement, and may serve in some key administrative functions like compensation and promotion. Informal, regular feedback, however, may serve you much better in driving performance, because it is timelier, more relevant to daily work, and more specific to the individual. Individuals also respond much more constructively to positive feedback, and some experts believe the ratio of positive to negative feedback should be on the order of 9 to 1. Be sure that feedback is done in a coaching manner and focuses on the behavior (You may try sitting down when you talk with patients as a way of making them feel more at ease) rather than on the person themselves (You’re really not a good communicator).
Managing Marginal Performance
Marginal performance can be defined as a physician whose observed behaviors or measured outcomes are at significant variance from what is expected. This pattern takes place over time and happens in spite of having in place all the other elements of a performance management system. Consider the “clock puncher” who rarely helps out the rest of the team on busy days and never shows up to group meetings or committees. Or the “tortoise” that has wonderful staff relations but chronically arrives at work late and repeatedly forgets to submit inpatient charges. Then there’s the “hothead” who is clinically adept and has high patient satisfaction but loses his or her temper with nursing and is pervasively confrontational with consultants. The steps to be taken in these and other cases like them include ensuring adequate documentation, reaching an agreement with the individual in recognizing that there is a problem, generating options for causality, negotiating a contract for improvement, and then letting future behavior determine the consequences.
Taking Corrective Action
Sometimes you simply cannot fix everything, and you need to be easy on yourself for having reached the point where the situation is no longer remediable in spite of your best efforts. In the end, everyone will be better off. When physician conduct becomes detrimental to patient safety, staff safety or quality patient care; is disruptive to the organization; or is otherwise chronically aberrant, then it is time to take adverse action. Since there are many pitfalls that have HR and legal implications, it is advisable to consult with relevant personnel to avoid problems with inadequate documentation and the potential need to report actions to state agencies and the National Practitioner Data Bank (per the Healthcare Quality Improvement Act of 1986).
Resources
- Ury W, Fisher R. Getting to Yes: Negotiating Agreement Without Giving In. 2nd ed. New York: Penguin Books; 1991.
- Reinertsen J. Physicians as leaders in the improvement of health care systems. Ann Intern Med. 1998;128:833-8.
- Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
- American College of Physician Executives. Managing Physician Performance in Organizations. Ongoing courses available at www.acpe.org.