User login
CASE: First-episode mania
Mrs. P, age 47, is brought to the emergency department (ED) because her family is concerned about her behavioral changes over the last week. Her husband reports that Mrs. P has become hyper-religious and talkative. She has been perseverating on numbers and dates and incessantly calling people. Mrs. P reports increased energy and decreased need for sleep. On examination, she has pressured speech. She has no psychiatric history; however, for the past year, she has been taking sertraline, 100 mg/d, and desipramine, 25 mg/d, which her primary care physician prescribed for unknown reasons.
Mrs. P has struggled with chronic back pain for years, but an MRI of her spine is negative. Her family strongly believes that for the past 3 years Mrs. P has been receiving too many medications from her pain management specialist. Six weeks before her current presentation, she was receiving methadone, 40 mg/d, hydrocodone, at least 20 mg/d, and tramadol, 400 mg/d in divided doses. She also was taking an unknown dose of at least 1 benzodiazepine.
Mrs. P’s husband notes she stopped taking methadone abruptly approximately 5 weeks ago. However, about 3 weeks ago, Mrs. P accidentally overdosed on opioids and was hospitalized for several days. Urine drug screen at the time was positive for acetaminophen, salicylate, propoxyphene, opiate, benzodiazepine, and tricyclic antidepressant.
Mrs. P’s medical history includes auditory nerve loss from birth; her mother had German measles (rubella). Mrs. P never learned American Sign Language. She underwent cochlear implant surgery 1 year ago and now has only mild difficulties speaking.
The authors’ observations
Manic symptoms are common in patients with comorbid medical disorders and present a diagnostic challenge. Obtaining an accurate history from the patient may be difficult. Such evaluations often require extensive investigation and collection of data from multiple sources, including:
- medical records
- family members
- patient observation.
Mrs. P’s history is marked by contradicting data from these sources. For example, her family says she stopped taking “pain medications” 5 weeks ago, but 2 weeks later her urine drug screen showed opioids.
Both illicit drugs and prescribed medications can precipitate manic symptoms. From medical records and drug testing, it was evident that Mrs. P had a history of medication abuse/overdose/misuse.
Mania also has been associated with substance withdrawal. Mrs. P allegedly stopped taking methadone 4 weeks before the onset of manic symptoms. Methadone is a synthetic opioid with a pharmacokinetic and pharmacodynamic profile that presents clinical challenges, including:
- large interindividual variability in methadone pharmacokinetics
- lack of reliable equianalgesic conversion ratio to and from other opioids
- potential for multiple drug interactions and complex pharmacodynamics.
An opioid’s half-life determines the onset and duration of withdrawal syndrome symptoms.1 Methadone metabolism is predominantly mediated by CYP3A4, CYP2B6, CYP2D6, and to some extent by CYP2C19.1 We performed genetic testing to help evaluate how Mrs. P metabolized medications. Mrs. P had a normal genotype for CYP2D6, which meant that she should process opioids at a normal rate; however, she was heterozygous for CYP2C19*2 polymorphism, so it is possible that methadone stayed in her system longer than average.
Evidence documenting methadone drug interactions is limited (Table 1).1 Mrs. P was taking sertraline and desipramine; both have potent effects via 2D6 inhibition that could increase plasma methadone concentration. Other evidence indicates that benzodiazepines and methadone may have synergistic interactions that could increase opioid sedation or respiratory depression.1
Table 1
Is a drug interaction with methadone causing Mrs. P’s mania?
| Medication class/agent | Effect on methadone level | Effect on methadone metabolism | Additional effects of interaction |
|---|---|---|---|
| Selective serotonin reuptake inhibitors | |||
| Fluvoxamine | Increase | Inhibition | Opioid toxicity |
| Fluoxetine | Increase | Inhibition | Torsades de pointes |
| Paroxetine | Increase | Inhibition | Decreased hepatic metabolism |
| Sertraline* | Increase | Autoinduction | Torsades de pointes |
| Citalopram | — | — | Torsades de pointes |
| Tricyclic antidepressants | |||
| Desipramine* | — | Inhibition | Increased desipramine levels/inhibition of desipramine metabolism |
| Amitriptyline | Increase methadone clearance | — | Torsades de pointes/prolonged QT interval |
| Anti-inflammatory drugs | |||
| NSAIDs* | — | — | Enhanced analgesia/opioid-sparing effect |
| Aspirin* | — | — | Paradoxical activation of platelet receptors |
| Benzodiazepines | |||
| Alprazolam | — | — | CNS depression/sedation/overdose |
| Diazepam* | — | Inhibition | Additive depressant effects |
| Opioid agonists | |||
| Dextromethorphan | — | Inhibition (not significant) | Increased side effects, especially sleepiness and drowsiness |
| Tramadol* | — | — | Well tolerated |
| Nicotine | Decrease | Can increase smoking rate | |
| *Medications taken by Mrs. P | |||
| NSAIDs: nonsteroidal anti-inflammatory drugs | |||
| Source: Reference 1 | |||
EVALUATION: Few clues
In our ED, Mrs. P’s urine drug abuse screen is positive for salicylate and benzodiazepine only. Findings from physical examination, vital signs, ECG, and chest radiography are within normal limits. Internal medicine consultation is unremarkable. Mrs. P’s laboratory investigation is notable for an elevated white blood cell count, but this normalizes over a week.
Mrs. P shows no evidence of infection and is normoglycemic. B12 and folate are within normal limits. Serum electrolytes, liver function testing, sensitive thyroid stimulating hormone, and C-reactive protein are within normal limits. Urinalysis is negative except for a small amount of hemoglobin. Her creatine kinase (CK) is in the upper normal range. Human immunodeficiency virus (HIV) and syphilis testing is negative. Ceruloplasmin level also is normal. Heavy metal screen is negative. Head MRI and CT from previous hospitalizations were unremarkable.
The authors’ observations
Our first step was to clarify Mrs. P’s diagnosis. In reviewing differential diagnoses, we considered:
- serotonin syndrome
- benzodiazepine withdrawal syndrome
- antidepressant-induced mania
- adrenergic toxicity
- malignant hyperthermia
- heat stroke
- infectious causes.
Our index of suspicion for serotonin syndrome was low because Mrs. P didn’t meet criteria required for diagnosis. Relevant signs and symptoms included confusion, elevated mood (major) and agitation, nervousness, insomnia, and low blood pressure (minor).
Based on concerns about medication interactions, we discontinued sertraline and desipramine. According to the patient’s sister, Mrs. P’s manic symptoms markedly responded to PRN doses of lorazepam. We prescribed lorazepam, 1 mg every 6 hours, and observed Mrs. P for signs and symptoms of benzodiazepine withdrawal.
HISTORY: OTC drug use
According to Mrs. P’s mother, after her daughter abruptly discontinued methadone, she began to have very strong headaches, which she treated with Excedrin or Excedrin Sinus. The mother said that 4 days before Mrs. P came to the ED, she found her daughter holding 4 tablets of Excedrin and an empty bottle. Unfortunately her mother was unable to say what type of Excedrin it was. When the treatment team asks Mrs. P how many pills she usually takes, she says she doesn’t know but usually until the pain stops.
The authors’ observations
Management of secondary mania should focus on treating the underlying condition (Algorithm). Neurology categorizes mania into 3 categories:2
- confusional-delirious states
- manic symptoms associated with focal or multifocal cerebral lesions
- affective disorders (manic-depressive and depressive psychoses).
Medical workup ruled out common secondary causes of psychosis. Collaborative information from relatives revealed no family history of mental illness.
Patients with hearing loss and deafness have been shown to be at increased risk for psychotic disorders compared with the general population. Severe sensory deficits early in Mrs. P’s life may have influenced the orderly development of neural connections in her sensory cortex and association areas.3 Mrs. P was deaf for the first 45 years of life. It could be hypothesized that her sensory deficits significantly influenced her ability to reality test. After receiving a cochlear implant, Mrs. P rapidly went from no auditory stimulation to marked improvement. This stressor might precipitate psychotic symptoms. However, her presentation seemed to be characterized more by manic symptoms or an agitated delirium. It also did not fit temporally with her presentation.
We begin to suspect that Mrs. P’s mania is substance-induced. Excedrin, an over-the-counter medication, contains aspirin and caffeine. Excedrin Sinus also contains phenylephrine. Amphetamines, caffeine, ephedrine, pseudoephedrine, and phenylpropanolamine have all been linked to manic-like psychotic episodes.
Concerns about the illicit conversion of pseudoephedrine into methamphetamine obliged pharmaceutical companies in the United States to switch product formulations to phenylephrine in 2005,4 although some “behind-the-counter” medications may contain pseudoephedrine. Phenylephrine is a relatively selective α1 agonist with weak α2 adrenoceptor agonist activity and low β agonist activity. It is very similar to pseudo-ephedrine, which is known to be implicated in the development of manic symptoms.5,6
Pseudoephedrine can raise CK levels and cause rhabdomyolysis.7,8 Mrs. P’s CK level was 176 (normal range 36 to 176 U/L) 4 days after her initial presentation, and she had a moderate amount of myoglobin in her urine. Her creatinine was normal. The patient was taking excessive amounts of caffeine and—if she was using Excedrin Sinus—pseudoephedrine or phenylephrine. We were unable to determine whether her Excedrin contained pseudoephedrine or phenylephrine. In addition, she was going through opioid withdrawal and reported problems with her sleep. There was also a question of Mrs. P’s unknown methadone use combined with its decreased clearance secondary to medication interactions.
While previously hospitalized for overdose, Mrs. P tested positive for propoxyphene. Excessive use of propoxyphene also can cause numerous adverse reactions. Some of that could have explained why Mrs. P’s presentation includes nervousness, CNS stimulation, excitement, insomnia, and restlessness.5
Based on multiple factors, we believe Mrs. P meets DSM-IV-TR criteria for substance-induced mood disorder (Table 2).9 This diagnosis is supported by Mrs. P’s history of complex polypharmacy, excessive caffeine use, sleep deprivation, and possible opioid withdrawal.
Algorithm: Managing substance-induced manic disorder
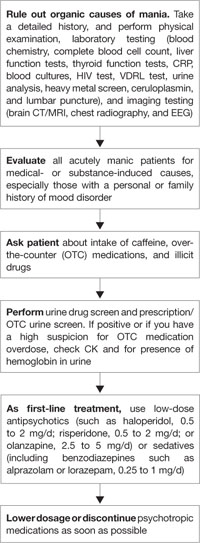
CK: creatine kinase; CRP: C-reactive protein; CT: computed tomography; EEG: electroencephalogram; HIV: human immunodeficiency virus; MRI: magnetic resonance imaging; VDRL: venereal disease research laboratoryTable 2
DSM-IV-TR criteria for substance-induced mood disorder*
| A. A prominent and persistent disturbance in mood predominates in the clinical picture and is characterized by either (or both) of the following: 1. depressed mood or markedly diminished interest or pleasure in all, or almost all, activities 2. elevated, expansive, or irritable mood |
| B. There is evidence from the history, physical examination, or laboratory findings of: 1. the symptoms in Criterion A developed during, or within 1 month of, substance intoxication or withdrawal, or 2. medication use is etiologically related to the disturbance |
| C. The disturbance is not better accounted for by a mood disorder that is not substance-induced |
| D. The disturbance does not occur exclusively during the course of a delirium |
| E. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| Minimal criteria are A plus B plus E |
| *Make this diagnosis only when mood symptoms are in excess of those usually associated with substance intoxication or substance withdrawal syndrome and when symptoms are sufficiently severe to warrant independent clinical attention |
| Source: Reference 9 |
TREATMENT: Escalating symptoms
While hospitalized, Mrs. P focuses solely on receiving pain medication. She does not know why she is in the hospital. She is easily distractible, intermittently intrusive, and disorganized and tangential in her thought process.
Two days after admission, her uncontrolled behavior escalates and she has marked psychomotor agitation. She is confused but remains oriented to time, place, and person. We start treatment with risperidone, 0.5 mg each morning and 1 mg at bedtime, because this agent is well tolerated, efficacious, and easily titrated to symptom response. Mrs. P’s symptoms improve, but she does not return to her reported baseline. Two days later, we increase risperidone to 1 mg every morning and 2 mg at bedtime. On the 6th day of hospitalization, Mrs. P is more organized and able to follow simple commands. She denies auditory or visual hallucinations. On the 10th day, she improves markedly and is back to her baseline level of functioning.
We perform psychological testing, including the Wechsler Adult Intelligence Scale (WAIS III) and the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS, Form A). The results show global neurocognitive deficits. Mrs. P’s intellectual skill is significantly below average, with verbal abilities reflecting functioning in the mildly retarded range. Nonverbal skills were stronger but still below average. Mrs. P’s capacity to learn and retain new information and to understand even modestly complex concepts is quite limited.
Because of Mrs. P’s long history of poly-substance abuse, inability to process information, and chronic back pain, we judge her to be at high risk for relapse. However, Mrs. P and her family are not interested in chemical dependence treatment.
This left us facing a difficult clinical situation. Mrs. P had a pattern of presenting to multiple physicians and eventually receiving narcotics. Her family provided transportation for her to these appointments but also was concerned about her drug use. With the patient and her family, we carefully outline Mrs. P’s treatment needs, including:
- medication monitoring by a psychiatrist after discharge
- a single, consistent primary care physician to manage her care
- a treatment plan shared by all clinicians involved in her care.
We review with Mrs. P and her family the benefits of behavioral approaches to chronic pain management. They agree to our recommendation that the family control Mrs. P’s medication supply. We discharge her on risperidone, 0.5 mg each morning and 1 mg at bedtime, and she is scheduled for follow-up with a local psychiatrist.
Related resource
- Krauthammer C, Klerman GL. Manic syndromes associated with antecedent physical illness or drugs. Arch Gen Psychiatry. 1978;35(11):1333-1339.
Drug brand names
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Citalopram • Celexa
- Desipramine • Norpramin
- Diazepam • Valium
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Hydrocodone • Vicodin, Lortab, others
- Lorazepam • Ativan
- Methadone • Dolophine, Methadose
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Propoxyphene • Darvon, Darvocet, others
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. De Fazio S, Gallelli L, De Siena A, et al. Role of CYP3A5 in abnormal clearance methadone. Ann Pharmacother. 2008;42(6):893-897.
2. Ropper AH, Brown RH. Adams and Victor’s principles of neurology. 8th ed. New York, NY: McGraw-Hill Professional; 2005.
3. Thewissen V, Myin-Germeys I, Bentall R, et al. Hearing impairment and psychosis revisited. Schizophr Res. 2005;76(1):99-103.
4. Eccles R. Substitution of phenylephrine for pseudoephedrine as a nasal decongeststant. An illogical way to control methamphetamine abuse. Br J Clin Pharmacol. 2007;63(1):10-14.
5. Wilson H, Woods D. Pseudoephedrine causing mania-like symptoms. N Z Med J. 2002;115(1148):86.-
6. Dalton R. Mixed bipolar disorder precipitated by pseudoephedrine hydrochloride. South Med J. 1990;83(1):64-65.
7. Mansi IA, Huang J. Rhabdomyolysis in response to weight-loss herbal medicine. Am J Med Sci. 2004;327:356-357.
8. Sandhu RS, Como JJ, Scalea TS. Renal failure and exercise-induced rhabdomyolysis in patients taking performance-enhancing compounds. J Trauma. 2002;53:761-764.
9. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
CASE: First-episode mania
Mrs. P, age 47, is brought to the emergency department (ED) because her family is concerned about her behavioral changes over the last week. Her husband reports that Mrs. P has become hyper-religious and talkative. She has been perseverating on numbers and dates and incessantly calling people. Mrs. P reports increased energy and decreased need for sleep. On examination, she has pressured speech. She has no psychiatric history; however, for the past year, she has been taking sertraline, 100 mg/d, and desipramine, 25 mg/d, which her primary care physician prescribed for unknown reasons.
Mrs. P has struggled with chronic back pain for years, but an MRI of her spine is negative. Her family strongly believes that for the past 3 years Mrs. P has been receiving too many medications from her pain management specialist. Six weeks before her current presentation, she was receiving methadone, 40 mg/d, hydrocodone, at least 20 mg/d, and tramadol, 400 mg/d in divided doses. She also was taking an unknown dose of at least 1 benzodiazepine.
Mrs. P’s husband notes she stopped taking methadone abruptly approximately 5 weeks ago. However, about 3 weeks ago, Mrs. P accidentally overdosed on opioids and was hospitalized for several days. Urine drug screen at the time was positive for acetaminophen, salicylate, propoxyphene, opiate, benzodiazepine, and tricyclic antidepressant.
Mrs. P’s medical history includes auditory nerve loss from birth; her mother had German measles (rubella). Mrs. P never learned American Sign Language. She underwent cochlear implant surgery 1 year ago and now has only mild difficulties speaking.
The authors’ observations
Manic symptoms are common in patients with comorbid medical disorders and present a diagnostic challenge. Obtaining an accurate history from the patient may be difficult. Such evaluations often require extensive investigation and collection of data from multiple sources, including:
- medical records
- family members
- patient observation.
Mrs. P’s history is marked by contradicting data from these sources. For example, her family says she stopped taking “pain medications” 5 weeks ago, but 2 weeks later her urine drug screen showed opioids.
Both illicit drugs and prescribed medications can precipitate manic symptoms. From medical records and drug testing, it was evident that Mrs. P had a history of medication abuse/overdose/misuse.
Mania also has been associated with substance withdrawal. Mrs. P allegedly stopped taking methadone 4 weeks before the onset of manic symptoms. Methadone is a synthetic opioid with a pharmacokinetic and pharmacodynamic profile that presents clinical challenges, including:
- large interindividual variability in methadone pharmacokinetics
- lack of reliable equianalgesic conversion ratio to and from other opioids
- potential for multiple drug interactions and complex pharmacodynamics.
An opioid’s half-life determines the onset and duration of withdrawal syndrome symptoms.1 Methadone metabolism is predominantly mediated by CYP3A4, CYP2B6, CYP2D6, and to some extent by CYP2C19.1 We performed genetic testing to help evaluate how Mrs. P metabolized medications. Mrs. P had a normal genotype for CYP2D6, which meant that she should process opioids at a normal rate; however, she was heterozygous for CYP2C19*2 polymorphism, so it is possible that methadone stayed in her system longer than average.
Evidence documenting methadone drug interactions is limited (Table 1).1 Mrs. P was taking sertraline and desipramine; both have potent effects via 2D6 inhibition that could increase plasma methadone concentration. Other evidence indicates that benzodiazepines and methadone may have synergistic interactions that could increase opioid sedation or respiratory depression.1
Table 1
Is a drug interaction with methadone causing Mrs. P’s mania?
| Medication class/agent | Effect on methadone level | Effect on methadone metabolism | Additional effects of interaction |
|---|---|---|---|
| Selective serotonin reuptake inhibitors | |||
| Fluvoxamine | Increase | Inhibition | Opioid toxicity |
| Fluoxetine | Increase | Inhibition | Torsades de pointes |
| Paroxetine | Increase | Inhibition | Decreased hepatic metabolism |
| Sertraline* | Increase | Autoinduction | Torsades de pointes |
| Citalopram | — | — | Torsades de pointes |
| Tricyclic antidepressants | |||
| Desipramine* | — | Inhibition | Increased desipramine levels/inhibition of desipramine metabolism |
| Amitriptyline | Increase methadone clearance | — | Torsades de pointes/prolonged QT interval |
| Anti-inflammatory drugs | |||
| NSAIDs* | — | — | Enhanced analgesia/opioid-sparing effect |
| Aspirin* | — | — | Paradoxical activation of platelet receptors |
| Benzodiazepines | |||
| Alprazolam | — | — | CNS depression/sedation/overdose |
| Diazepam* | — | Inhibition | Additive depressant effects |
| Opioid agonists | |||
| Dextromethorphan | — | Inhibition (not significant) | Increased side effects, especially sleepiness and drowsiness |
| Tramadol* | — | — | Well tolerated |
| Nicotine | Decrease | Can increase smoking rate | |
| *Medications taken by Mrs. P | |||
| NSAIDs: nonsteroidal anti-inflammatory drugs | |||
| Source: Reference 1 | |||
EVALUATION: Few clues
In our ED, Mrs. P’s urine drug abuse screen is positive for salicylate and benzodiazepine only. Findings from physical examination, vital signs, ECG, and chest radiography are within normal limits. Internal medicine consultation is unremarkable. Mrs. P’s laboratory investigation is notable for an elevated white blood cell count, but this normalizes over a week.
Mrs. P shows no evidence of infection and is normoglycemic. B12 and folate are within normal limits. Serum electrolytes, liver function testing, sensitive thyroid stimulating hormone, and C-reactive protein are within normal limits. Urinalysis is negative except for a small amount of hemoglobin. Her creatine kinase (CK) is in the upper normal range. Human immunodeficiency virus (HIV) and syphilis testing is negative. Ceruloplasmin level also is normal. Heavy metal screen is negative. Head MRI and CT from previous hospitalizations were unremarkable.
The authors’ observations
Our first step was to clarify Mrs. P’s diagnosis. In reviewing differential diagnoses, we considered:
- serotonin syndrome
- benzodiazepine withdrawal syndrome
- antidepressant-induced mania
- adrenergic toxicity
- malignant hyperthermia
- heat stroke
- infectious causes.
Our index of suspicion for serotonin syndrome was low because Mrs. P didn’t meet criteria required for diagnosis. Relevant signs and symptoms included confusion, elevated mood (major) and agitation, nervousness, insomnia, and low blood pressure (minor).
Based on concerns about medication interactions, we discontinued sertraline and desipramine. According to the patient’s sister, Mrs. P’s manic symptoms markedly responded to PRN doses of lorazepam. We prescribed lorazepam, 1 mg every 6 hours, and observed Mrs. P for signs and symptoms of benzodiazepine withdrawal.
HISTORY: OTC drug use
According to Mrs. P’s mother, after her daughter abruptly discontinued methadone, she began to have very strong headaches, which she treated with Excedrin or Excedrin Sinus. The mother said that 4 days before Mrs. P came to the ED, she found her daughter holding 4 tablets of Excedrin and an empty bottle. Unfortunately her mother was unable to say what type of Excedrin it was. When the treatment team asks Mrs. P how many pills she usually takes, she says she doesn’t know but usually until the pain stops.
The authors’ observations
Management of secondary mania should focus on treating the underlying condition (Algorithm). Neurology categorizes mania into 3 categories:2
- confusional-delirious states
- manic symptoms associated with focal or multifocal cerebral lesions
- affective disorders (manic-depressive and depressive psychoses).
Medical workup ruled out common secondary causes of psychosis. Collaborative information from relatives revealed no family history of mental illness.
Patients with hearing loss and deafness have been shown to be at increased risk for psychotic disorders compared with the general population. Severe sensory deficits early in Mrs. P’s life may have influenced the orderly development of neural connections in her sensory cortex and association areas.3 Mrs. P was deaf for the first 45 years of life. It could be hypothesized that her sensory deficits significantly influenced her ability to reality test. After receiving a cochlear implant, Mrs. P rapidly went from no auditory stimulation to marked improvement. This stressor might precipitate psychotic symptoms. However, her presentation seemed to be characterized more by manic symptoms or an agitated delirium. It also did not fit temporally with her presentation.
We begin to suspect that Mrs. P’s mania is substance-induced. Excedrin, an over-the-counter medication, contains aspirin and caffeine. Excedrin Sinus also contains phenylephrine. Amphetamines, caffeine, ephedrine, pseudoephedrine, and phenylpropanolamine have all been linked to manic-like psychotic episodes.
Concerns about the illicit conversion of pseudoephedrine into methamphetamine obliged pharmaceutical companies in the United States to switch product formulations to phenylephrine in 2005,4 although some “behind-the-counter” medications may contain pseudoephedrine. Phenylephrine is a relatively selective α1 agonist with weak α2 adrenoceptor agonist activity and low β agonist activity. It is very similar to pseudo-ephedrine, which is known to be implicated in the development of manic symptoms.5,6
Pseudoephedrine can raise CK levels and cause rhabdomyolysis.7,8 Mrs. P’s CK level was 176 (normal range 36 to 176 U/L) 4 days after her initial presentation, and she had a moderate amount of myoglobin in her urine. Her creatinine was normal. The patient was taking excessive amounts of caffeine and—if she was using Excedrin Sinus—pseudoephedrine or phenylephrine. We were unable to determine whether her Excedrin contained pseudoephedrine or phenylephrine. In addition, she was going through opioid withdrawal and reported problems with her sleep. There was also a question of Mrs. P’s unknown methadone use combined with its decreased clearance secondary to medication interactions.
While previously hospitalized for overdose, Mrs. P tested positive for propoxyphene. Excessive use of propoxyphene also can cause numerous adverse reactions. Some of that could have explained why Mrs. P’s presentation includes nervousness, CNS stimulation, excitement, insomnia, and restlessness.5
Based on multiple factors, we believe Mrs. P meets DSM-IV-TR criteria for substance-induced mood disorder (Table 2).9 This diagnosis is supported by Mrs. P’s history of complex polypharmacy, excessive caffeine use, sleep deprivation, and possible opioid withdrawal.
Algorithm: Managing substance-induced manic disorder
CK: creatine kinase; CRP: C-reactive protein; CT: computed tomography; EEG: electroencephalogram; HIV: human immunodeficiency virus; MRI: magnetic resonance imaging; VDRL: venereal disease research laboratoryTable 2
DSM-IV-TR criteria for substance-induced mood disorder*
| A. A prominent and persistent disturbance in mood predominates in the clinical picture and is characterized by either (or both) of the following: 1. depressed mood or markedly diminished interest or pleasure in all, or almost all, activities 2. elevated, expansive, or irritable mood |
| B. There is evidence from the history, physical examination, or laboratory findings of: 1. the symptoms in Criterion A developed during, or within 1 month of, substance intoxication or withdrawal, or 2. medication use is etiologically related to the disturbance |
| C. The disturbance is not better accounted for by a mood disorder that is not substance-induced |
| D. The disturbance does not occur exclusively during the course of a delirium |
| E. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| Minimal criteria are A plus B plus E |
| *Make this diagnosis only when mood symptoms are in excess of those usually associated with substance intoxication or substance withdrawal syndrome and when symptoms are sufficiently severe to warrant independent clinical attention |
| Source: Reference 9 |
TREATMENT: Escalating symptoms
While hospitalized, Mrs. P focuses solely on receiving pain medication. She does not know why she is in the hospital. She is easily distractible, intermittently intrusive, and disorganized and tangential in her thought process.
Two days after admission, her uncontrolled behavior escalates and she has marked psychomotor agitation. She is confused but remains oriented to time, place, and person. We start treatment with risperidone, 0.5 mg each morning and 1 mg at bedtime, because this agent is well tolerated, efficacious, and easily titrated to symptom response. Mrs. P’s symptoms improve, but she does not return to her reported baseline. Two days later, we increase risperidone to 1 mg every morning and 2 mg at bedtime. On the 6th day of hospitalization, Mrs. P is more organized and able to follow simple commands. She denies auditory or visual hallucinations. On the 10th day, she improves markedly and is back to her baseline level of functioning.
We perform psychological testing, including the Wechsler Adult Intelligence Scale (WAIS III) and the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS, Form A). The results show global neurocognitive deficits. Mrs. P’s intellectual skill is significantly below average, with verbal abilities reflecting functioning in the mildly retarded range. Nonverbal skills were stronger but still below average. Mrs. P’s capacity to learn and retain new information and to understand even modestly complex concepts is quite limited.
Because of Mrs. P’s long history of poly-substance abuse, inability to process information, and chronic back pain, we judge her to be at high risk for relapse. However, Mrs. P and her family are not interested in chemical dependence treatment.
This left us facing a difficult clinical situation. Mrs. P had a pattern of presenting to multiple physicians and eventually receiving narcotics. Her family provided transportation for her to these appointments but also was concerned about her drug use. With the patient and her family, we carefully outline Mrs. P’s treatment needs, including:
- medication monitoring by a psychiatrist after discharge
- a single, consistent primary care physician to manage her care
- a treatment plan shared by all clinicians involved in her care.
We review with Mrs. P and her family the benefits of behavioral approaches to chronic pain management. They agree to our recommendation that the family control Mrs. P’s medication supply. We discharge her on risperidone, 0.5 mg each morning and 1 mg at bedtime, and she is scheduled for follow-up with a local psychiatrist.
Related resource
- Krauthammer C, Klerman GL. Manic syndromes associated with antecedent physical illness or drugs. Arch Gen Psychiatry. 1978;35(11):1333-1339.
Drug brand names
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Citalopram • Celexa
- Desipramine • Norpramin
- Diazepam • Valium
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Hydrocodone • Vicodin, Lortab, others
- Lorazepam • Ativan
- Methadone • Dolophine, Methadose
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Propoxyphene • Darvon, Darvocet, others
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: First-episode mania
Mrs. P, age 47, is brought to the emergency department (ED) because her family is concerned about her behavioral changes over the last week. Her husband reports that Mrs. P has become hyper-religious and talkative. She has been perseverating on numbers and dates and incessantly calling people. Mrs. P reports increased energy and decreased need for sleep. On examination, she has pressured speech. She has no psychiatric history; however, for the past year, she has been taking sertraline, 100 mg/d, and desipramine, 25 mg/d, which her primary care physician prescribed for unknown reasons.
Mrs. P has struggled with chronic back pain for years, but an MRI of her spine is negative. Her family strongly believes that for the past 3 years Mrs. P has been receiving too many medications from her pain management specialist. Six weeks before her current presentation, she was receiving methadone, 40 mg/d, hydrocodone, at least 20 mg/d, and tramadol, 400 mg/d in divided doses. She also was taking an unknown dose of at least 1 benzodiazepine.
Mrs. P’s husband notes she stopped taking methadone abruptly approximately 5 weeks ago. However, about 3 weeks ago, Mrs. P accidentally overdosed on opioids and was hospitalized for several days. Urine drug screen at the time was positive for acetaminophen, salicylate, propoxyphene, opiate, benzodiazepine, and tricyclic antidepressant.
Mrs. P’s medical history includes auditory nerve loss from birth; her mother had German measles (rubella). Mrs. P never learned American Sign Language. She underwent cochlear implant surgery 1 year ago and now has only mild difficulties speaking.
The authors’ observations
Manic symptoms are common in patients with comorbid medical disorders and present a diagnostic challenge. Obtaining an accurate history from the patient may be difficult. Such evaluations often require extensive investigation and collection of data from multiple sources, including:
- medical records
- family members
- patient observation.
Mrs. P’s history is marked by contradicting data from these sources. For example, her family says she stopped taking “pain medications” 5 weeks ago, but 2 weeks later her urine drug screen showed opioids.
Both illicit drugs and prescribed medications can precipitate manic symptoms. From medical records and drug testing, it was evident that Mrs. P had a history of medication abuse/overdose/misuse.
Mania also has been associated with substance withdrawal. Mrs. P allegedly stopped taking methadone 4 weeks before the onset of manic symptoms. Methadone is a synthetic opioid with a pharmacokinetic and pharmacodynamic profile that presents clinical challenges, including:
- large interindividual variability in methadone pharmacokinetics
- lack of reliable equianalgesic conversion ratio to and from other opioids
- potential for multiple drug interactions and complex pharmacodynamics.
An opioid’s half-life determines the onset and duration of withdrawal syndrome symptoms.1 Methadone metabolism is predominantly mediated by CYP3A4, CYP2B6, CYP2D6, and to some extent by CYP2C19.1 We performed genetic testing to help evaluate how Mrs. P metabolized medications. Mrs. P had a normal genotype for CYP2D6, which meant that she should process opioids at a normal rate; however, she was heterozygous for CYP2C19*2 polymorphism, so it is possible that methadone stayed in her system longer than average.
Evidence documenting methadone drug interactions is limited (Table 1).1 Mrs. P was taking sertraline and desipramine; both have potent effects via 2D6 inhibition that could increase plasma methadone concentration. Other evidence indicates that benzodiazepines and methadone may have synergistic interactions that could increase opioid sedation or respiratory depression.1
Table 1
Is a drug interaction with methadone causing Mrs. P’s mania?
| Medication class/agent | Effect on methadone level | Effect on methadone metabolism | Additional effects of interaction |
|---|---|---|---|
| Selective serotonin reuptake inhibitors | |||
| Fluvoxamine | Increase | Inhibition | Opioid toxicity |
| Fluoxetine | Increase | Inhibition | Torsades de pointes |
| Paroxetine | Increase | Inhibition | Decreased hepatic metabolism |
| Sertraline* | Increase | Autoinduction | Torsades de pointes |
| Citalopram | — | — | Torsades de pointes |
| Tricyclic antidepressants | |||
| Desipramine* | — | Inhibition | Increased desipramine levels/inhibition of desipramine metabolism |
| Amitriptyline | Increase methadone clearance | — | Torsades de pointes/prolonged QT interval |
| Anti-inflammatory drugs | |||
| NSAIDs* | — | — | Enhanced analgesia/opioid-sparing effect |
| Aspirin* | — | — | Paradoxical activation of platelet receptors |
| Benzodiazepines | |||
| Alprazolam | — | — | CNS depression/sedation/overdose |
| Diazepam* | — | Inhibition | Additive depressant effects |
| Opioid agonists | |||
| Dextromethorphan | — | Inhibition (not significant) | Increased side effects, especially sleepiness and drowsiness |
| Tramadol* | — | — | Well tolerated |
| Nicotine | Decrease | Can increase smoking rate | |
| *Medications taken by Mrs. P | |||
| NSAIDs: nonsteroidal anti-inflammatory drugs | |||
| Source: Reference 1 | |||
EVALUATION: Few clues
In our ED, Mrs. P’s urine drug abuse screen is positive for salicylate and benzodiazepine only. Findings from physical examination, vital signs, ECG, and chest radiography are within normal limits. Internal medicine consultation is unremarkable. Mrs. P’s laboratory investigation is notable for an elevated white blood cell count, but this normalizes over a week.
Mrs. P shows no evidence of infection and is normoglycemic. B12 and folate are within normal limits. Serum electrolytes, liver function testing, sensitive thyroid stimulating hormone, and C-reactive protein are within normal limits. Urinalysis is negative except for a small amount of hemoglobin. Her creatine kinase (CK) is in the upper normal range. Human immunodeficiency virus (HIV) and syphilis testing is negative. Ceruloplasmin level also is normal. Heavy metal screen is negative. Head MRI and CT from previous hospitalizations were unremarkable.
The authors’ observations
Our first step was to clarify Mrs. P’s diagnosis. In reviewing differential diagnoses, we considered:
- serotonin syndrome
- benzodiazepine withdrawal syndrome
- antidepressant-induced mania
- adrenergic toxicity
- malignant hyperthermia
- heat stroke
- infectious causes.
Our index of suspicion for serotonin syndrome was low because Mrs. P didn’t meet criteria required for diagnosis. Relevant signs and symptoms included confusion, elevated mood (major) and agitation, nervousness, insomnia, and low blood pressure (minor).
Based on concerns about medication interactions, we discontinued sertraline and desipramine. According to the patient’s sister, Mrs. P’s manic symptoms markedly responded to PRN doses of lorazepam. We prescribed lorazepam, 1 mg every 6 hours, and observed Mrs. P for signs and symptoms of benzodiazepine withdrawal.
HISTORY: OTC drug use
According to Mrs. P’s mother, after her daughter abruptly discontinued methadone, she began to have very strong headaches, which she treated with Excedrin or Excedrin Sinus. The mother said that 4 days before Mrs. P came to the ED, she found her daughter holding 4 tablets of Excedrin and an empty bottle. Unfortunately her mother was unable to say what type of Excedrin it was. When the treatment team asks Mrs. P how many pills she usually takes, she says she doesn’t know but usually until the pain stops.
The authors’ observations
Management of secondary mania should focus on treating the underlying condition (Algorithm). Neurology categorizes mania into 3 categories:2
- confusional-delirious states
- manic symptoms associated with focal or multifocal cerebral lesions
- affective disorders (manic-depressive and depressive psychoses).
Medical workup ruled out common secondary causes of psychosis. Collaborative information from relatives revealed no family history of mental illness.
Patients with hearing loss and deafness have been shown to be at increased risk for psychotic disorders compared with the general population. Severe sensory deficits early in Mrs. P’s life may have influenced the orderly development of neural connections in her sensory cortex and association areas.3 Mrs. P was deaf for the first 45 years of life. It could be hypothesized that her sensory deficits significantly influenced her ability to reality test. After receiving a cochlear implant, Mrs. P rapidly went from no auditory stimulation to marked improvement. This stressor might precipitate psychotic symptoms. However, her presentation seemed to be characterized more by manic symptoms or an agitated delirium. It also did not fit temporally with her presentation.
We begin to suspect that Mrs. P’s mania is substance-induced. Excedrin, an over-the-counter medication, contains aspirin and caffeine. Excedrin Sinus also contains phenylephrine. Amphetamines, caffeine, ephedrine, pseudoephedrine, and phenylpropanolamine have all been linked to manic-like psychotic episodes.
Concerns about the illicit conversion of pseudoephedrine into methamphetamine obliged pharmaceutical companies in the United States to switch product formulations to phenylephrine in 2005,4 although some “behind-the-counter” medications may contain pseudoephedrine. Phenylephrine is a relatively selective α1 agonist with weak α2 adrenoceptor agonist activity and low β agonist activity. It is very similar to pseudo-ephedrine, which is known to be implicated in the development of manic symptoms.5,6
Pseudoephedrine can raise CK levels and cause rhabdomyolysis.7,8 Mrs. P’s CK level was 176 (normal range 36 to 176 U/L) 4 days after her initial presentation, and she had a moderate amount of myoglobin in her urine. Her creatinine was normal. The patient was taking excessive amounts of caffeine and—if she was using Excedrin Sinus—pseudoephedrine or phenylephrine. We were unable to determine whether her Excedrin contained pseudoephedrine or phenylephrine. In addition, she was going through opioid withdrawal and reported problems with her sleep. There was also a question of Mrs. P’s unknown methadone use combined with its decreased clearance secondary to medication interactions.
While previously hospitalized for overdose, Mrs. P tested positive for propoxyphene. Excessive use of propoxyphene also can cause numerous adverse reactions. Some of that could have explained why Mrs. P’s presentation includes nervousness, CNS stimulation, excitement, insomnia, and restlessness.5
Based on multiple factors, we believe Mrs. P meets DSM-IV-TR criteria for substance-induced mood disorder (Table 2).9 This diagnosis is supported by Mrs. P’s history of complex polypharmacy, excessive caffeine use, sleep deprivation, and possible opioid withdrawal.
Algorithm: Managing substance-induced manic disorder
CK: creatine kinase; CRP: C-reactive protein; CT: computed tomography; EEG: electroencephalogram; HIV: human immunodeficiency virus; MRI: magnetic resonance imaging; VDRL: venereal disease research laboratoryTable 2
DSM-IV-TR criteria for substance-induced mood disorder*
| A. A prominent and persistent disturbance in mood predominates in the clinical picture and is characterized by either (or both) of the following: 1. depressed mood or markedly diminished interest or pleasure in all, or almost all, activities 2. elevated, expansive, or irritable mood |
| B. There is evidence from the history, physical examination, or laboratory findings of: 1. the symptoms in Criterion A developed during, or within 1 month of, substance intoxication or withdrawal, or 2. medication use is etiologically related to the disturbance |
| C. The disturbance is not better accounted for by a mood disorder that is not substance-induced |
| D. The disturbance does not occur exclusively during the course of a delirium |
| E. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| Minimal criteria are A plus B plus E |
| *Make this diagnosis only when mood symptoms are in excess of those usually associated with substance intoxication or substance withdrawal syndrome and when symptoms are sufficiently severe to warrant independent clinical attention |
| Source: Reference 9 |
TREATMENT: Escalating symptoms
While hospitalized, Mrs. P focuses solely on receiving pain medication. She does not know why she is in the hospital. She is easily distractible, intermittently intrusive, and disorganized and tangential in her thought process.
Two days after admission, her uncontrolled behavior escalates and she has marked psychomotor agitation. She is confused but remains oriented to time, place, and person. We start treatment with risperidone, 0.5 mg each morning and 1 mg at bedtime, because this agent is well tolerated, efficacious, and easily titrated to symptom response. Mrs. P’s symptoms improve, but she does not return to her reported baseline. Two days later, we increase risperidone to 1 mg every morning and 2 mg at bedtime. On the 6th day of hospitalization, Mrs. P is more organized and able to follow simple commands. She denies auditory or visual hallucinations. On the 10th day, she improves markedly and is back to her baseline level of functioning.
We perform psychological testing, including the Wechsler Adult Intelligence Scale (WAIS III) and the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS, Form A). The results show global neurocognitive deficits. Mrs. P’s intellectual skill is significantly below average, with verbal abilities reflecting functioning in the mildly retarded range. Nonverbal skills were stronger but still below average. Mrs. P’s capacity to learn and retain new information and to understand even modestly complex concepts is quite limited.
Because of Mrs. P’s long history of poly-substance abuse, inability to process information, and chronic back pain, we judge her to be at high risk for relapse. However, Mrs. P and her family are not interested in chemical dependence treatment.
This left us facing a difficult clinical situation. Mrs. P had a pattern of presenting to multiple physicians and eventually receiving narcotics. Her family provided transportation for her to these appointments but also was concerned about her drug use. With the patient and her family, we carefully outline Mrs. P’s treatment needs, including:
- medication monitoring by a psychiatrist after discharge
- a single, consistent primary care physician to manage her care
- a treatment plan shared by all clinicians involved in her care.
We review with Mrs. P and her family the benefits of behavioral approaches to chronic pain management. They agree to our recommendation that the family control Mrs. P’s medication supply. We discharge her on risperidone, 0.5 mg each morning and 1 mg at bedtime, and she is scheduled for follow-up with a local psychiatrist.
Related resource
- Krauthammer C, Klerman GL. Manic syndromes associated with antecedent physical illness or drugs. Arch Gen Psychiatry. 1978;35(11):1333-1339.
Drug brand names
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Citalopram • Celexa
- Desipramine • Norpramin
- Diazepam • Valium
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Hydrocodone • Vicodin, Lortab, others
- Lorazepam • Ativan
- Methadone • Dolophine, Methadose
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Propoxyphene • Darvon, Darvocet, others
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. De Fazio S, Gallelli L, De Siena A, et al. Role of CYP3A5 in abnormal clearance methadone. Ann Pharmacother. 2008;42(6):893-897.
2. Ropper AH, Brown RH. Adams and Victor’s principles of neurology. 8th ed. New York, NY: McGraw-Hill Professional; 2005.
3. Thewissen V, Myin-Germeys I, Bentall R, et al. Hearing impairment and psychosis revisited. Schizophr Res. 2005;76(1):99-103.
4. Eccles R. Substitution of phenylephrine for pseudoephedrine as a nasal decongeststant. An illogical way to control methamphetamine abuse. Br J Clin Pharmacol. 2007;63(1):10-14.
5. Wilson H, Woods D. Pseudoephedrine causing mania-like symptoms. N Z Med J. 2002;115(1148):86.-
6. Dalton R. Mixed bipolar disorder precipitated by pseudoephedrine hydrochloride. South Med J. 1990;83(1):64-65.
7. Mansi IA, Huang J. Rhabdomyolysis in response to weight-loss herbal medicine. Am J Med Sci. 2004;327:356-357.
8. Sandhu RS, Como JJ, Scalea TS. Renal failure and exercise-induced rhabdomyolysis in patients taking performance-enhancing compounds. J Trauma. 2002;53:761-764.
9. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
1. De Fazio S, Gallelli L, De Siena A, et al. Role of CYP3A5 in abnormal clearance methadone. Ann Pharmacother. 2008;42(6):893-897.
2. Ropper AH, Brown RH. Adams and Victor’s principles of neurology. 8th ed. New York, NY: McGraw-Hill Professional; 2005.
3. Thewissen V, Myin-Germeys I, Bentall R, et al. Hearing impairment and psychosis revisited. Schizophr Res. 2005;76(1):99-103.
4. Eccles R. Substitution of phenylephrine for pseudoephedrine as a nasal decongeststant. An illogical way to control methamphetamine abuse. Br J Clin Pharmacol. 2007;63(1):10-14.
5. Wilson H, Woods D. Pseudoephedrine causing mania-like symptoms. N Z Med J. 2002;115(1148):86.-
6. Dalton R. Mixed bipolar disorder precipitated by pseudoephedrine hydrochloride. South Med J. 1990;83(1):64-65.
7. Mansi IA, Huang J. Rhabdomyolysis in response to weight-loss herbal medicine. Am J Med Sci. 2004;327:356-357.
8. Sandhu RS, Como JJ, Scalea TS. Renal failure and exercise-induced rhabdomyolysis in patients taking performance-enhancing compounds. J Trauma. 2002;53:761-764.
9. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.