User login
Delivery of the shoulders often gets overlooked in discussions
of episiotomy
(Comment & Controversy, November 2012)
Difficult fetal extraction at cesarean delivery:
What should you do?
Robert L. Barbieri, MD (Editorial, January 2012)
What is the significance of the head-to-body delivery interval
in shoulder dystocia?
William A. Grobman, MD, MBA (Examining the Evidence, December 2011)
Does the use of multiple maneuvers in the management of shoulder dystocia increase the risk of neonatal injury?
Robert B. Gherman, MD (Examining the Evidence, August 2011)
CASE: Shoulder dystocia resulting in persistent injury to C5 and C6
A 30-year-old, G2P1 woman presented in labor at 39 weeks and reported a strong desire to have a natural childbirth. She was taking insulin for gestational diabetes mellitus diagnosed in the second trimester. Her body mass index was 43 kg/m2, and her height was 4 ft 11 in. The estimated fetal weight was 9 lb. She had a prior vaginal delivery. During her antepartum care the patient was extensively counseled about the risk of shoulder dystocia and obstetric brachial plexus (OBP) injury.
The patient progressed normally through labor without anesthesia. At birth, the baby delivered occiput posterior and restituted to right occiput transverse. There was a turtle sign, and the obstetrician diagnosed a shoulder dystocia, called for help, and told the mother to stop pushing. An attempt to deliver the fetal head with gentle downward guidance was unsuccessful. The McRoberts maneuver and suprapubic pressure combined with gentle downward guidance on the fetal head did not result in delivery. A mediolateral episiotomy was made and the Rubin and Wood maneuvers were attempted without success. The obstetrician then successfully delivered the posterior arm and the body of the baby was easily delivered.
The shoulder dystocia lasted 2 minutes before successful delivery. The Apgar scores were 3 and 6 at one and five minutes, respectively. The umbilical cord artery pH was 7.18. The birthweight was 9 lb 2 oz. A diagnosis of OBP injury involving C5 and C6 was made. At discharge the OBP injury persisted.
What is OBP injury?
Shoulder dystocia, which affected this mother and fetus, is a problem involving the impaction of the fetal shoulder behind the maternal symphysis pubis. Shoulder dystocia is a “bony problem.” Although shoulder dystocia cannot be predicted reliably, risk factors include:
- fetal macrosomia
- maternal diabetes
- maternal weight gain
- prepregnancy obesity
- multiparity
- operative vaginal delivery.1-3
The injury can be serious and permanent. The feared consequence of shoulder dystocia is permanent obstetric brachial plexus injury and/or fetal neurologic damage caused by reduced cord blood flow and fetal asphyxia. Occasionally, shoulder dystocia results in fetal death.
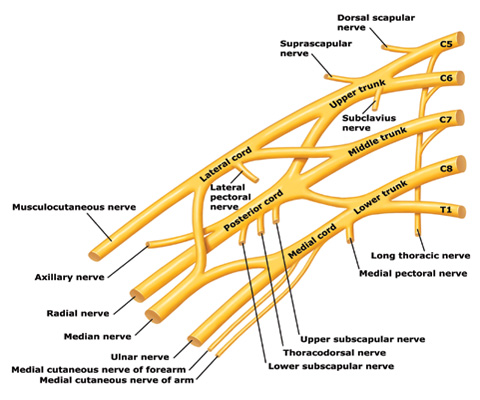
Trunks and cords of the brachial plexus
C5 and C6 roots merge to form the upper trunk, C7 root forms the middle trunk, and C8 and T1 roots merge to form the lower trunk.
How can an OBP injury occur?
Most cases are unilateral and arise when one or more of the brachial plexus nerves ( Figure ) are compromised. The forces of labor, fetal position, maternal pushing, and force applied to the fetal head and neck by a clinician all may contribute to an OBP injury.4 It is important to note that up to one-third of all OBP injuries occur in births not associated with a recognized shoulder dystocia.5
Erb’s palsy. Injuries to the C5 and C6 nerves account for about 50% of cases. The muscle groups impacted by this injury include the deltoid and infraspinatus muscles (mainly C5) and the biceps muscle (mainly C6). This pattern results in an adducted and internally rotated upper arm, an extended forearm, with preservation of hand and wrist movement.
Erb’s palsy plus. Injury to C5, C6, and C7 nerves accounts for about 35% of cases and manifests as adduction and internal rotation of the arm, extension and pronation of the forearm, plus flexion of the wrist and fingers—the so-called waiter’s tip posture.
Klumpke’s palsy. Isolated injury to the C8 nerve and T1 root occurs infrequently and manifests as isolated hand paralysis and Horner’s syndrome.
Approximately one in five OBP injuries persist for years following birth. The incidence of OBP injury ranges from 1.0 to 3.0 cases per 1,000 births.6-8 In a review of studies with at least 3 years of follow-up and less than 10% loss to follow-up, the authors reported that the three best studies observed a risk of persistent OBP of 10%, 19%, and 27%.9
Long-term management of OBP injury
The optimal approach to management of OBP injury is unknown because few high-quality studies are available to guide therapy. Typically, 3 to 9 months of observation and physical therapy are recommended following birth, with the hope that the majority of newborns will recover some or almost all function. Physical therapy is focused on reducing the occurrence of joint contractures and maintaining range of motion in the shoulder, elbow, wrist, and fingers.
Surgical exploration of the plexus is often advised when biceps muscle function is absent at 3 months of age. Some surgeons recommend waiting until 9 months before pursuing surgical exploration.10 No randomized trials have been performed demonstrating the value of surgical intervention, but case series report that surgical intervention with nerve grafting or nerve transfer is superior to management without neurosurgery.
The consequences of permanent OBP injury
A lifetime of corrective therapy for the child. OBP injury may result in a permanent brachial plexus injury—permanent arm weakness requiring decades of physical therapy and multiple surgeries to try to reduce functional disabilities. Problems that frequently occur in children with OBP injury include:
- shoulder contractures
- limb length differences
- winged scapula
- behavioral and developmental problems.
A patient’s care may be coordinated at a brachial plexus injury specialty center, where coordinated access to pediatric neurologists, neurosurgeons, orthopedic surgeons, and neurophysiologists is available and physical and occupational therapy are provided.
Years of emotional response for the parents. Following a birth complicated by shoulder dystocia, the parents may experience grief and anger. During the decades following the birth, the parents of the child will wonder if the injury could have been avoided. They may be asked by friends and relatives, “Would a cesarean delivery have prevented the injury?” Physical therapists, pediatric neurologists, orthopedic and neurosurgeons may reinforce the idea that the injury was caused when the obstetrician applied excessive lateral force to the head and neck, resulting in an injury to the brachial plexus.
Decades-long exposure to these ideas, unresolved anger, financial stress, and lingering doubts may result in the parents and child pursuing civil litigation against the delivering clinician.
Can we reduce the incidence of OBP injury and our risk of litigation?
There are no interventions proven to reduce the incidence of OBP injury. However, many experts advise that a multifaceted approach to this obstetric emergency may reduce the incidence of severe OBP injury at the same time that we reduce our risk of litigation.
When counseling patients about the risk for OBP injury, use teach-back. Patients tend to misunderstand or forget much of what their clinicians teach them.11 Teach-back is an iterative communication process in which the clinician teaches the patient a concept or technique, then asks the patient to repeat the concept in their own words or demonstrate the technique. The clinician then amplifies the concept or technique and corrects misunderstandings. The patient is then asked to repeat the concept or demonstrate the technique. When using teach-back, the clinician never asks, “Do you understand?” The clinician encourages the patient to teach the concept to the clinician using the patient’s own words.12
In the case above, the patient has multiple risk factors for shoulder dystocia, including obesity, short stature, insulin-treated gestational diabetes, and a large fetus. Given the high risk for shoulder dystocia, teach-back might help the patient better understand the situation. After explaining the concepts to the patient, the teach-back questions to the patient might include:
- “Can you tell me what is a shoulder dystocia?”
- “Can you list the health conditions that you have that increase your baby’s risk of shoulder dystocia?”
- “When a shoulder dystocia occurs, what actions will we take at birth to try to fix the shoulder dystocia?”
- “When a baby has experienced a shoulder dystocia, what can happen to the baby’s arm?”
Regularly perform multidisciplinary shoulder dystocia drills. The Joint Commission recommends that clinical drills be performed to help staff prepare for high-risk labor and delivery events, including shoulder dystocia, emergency cesarean delivery, and maternal hemorrhage.13
When shoulder dystocia occurs, extensively chart the event and interventions used. The American College of Obstetricians and Gynecologists has developed a patient safety checklist focused on key clinical elements in the antepartum, intrapartum, and postpartum periods and overall timing of the delivery to document when a shoulder dystocia occurs.14
Stop using the term “traction” in the medical record and obstetric literature. Words are meaningful and open to multiple interpretations. Often, words have unintended consequences. Plaintiff attorneys often highlight the obstetrician’s use of “traction” or “excessive traction” as the cause of an OBP injury. Orthopedic surgeons and pediatricians often state in their records that the OBP injury was a “traction injury,” further supporting the plaintiff attorney’s contention that excessive traction applied by the obstetrician caused the traction injury. Obstetricians do not use traction to deliver a baby. Motorized tractors generate traction, not obstetricians. We use gentle downward guidance to deliver the fetal shoulders and body.
In a high-risk situation, proceed quickly to delivery of the posterior arm. When you recognize a shoulder dystocia in a high-risk situation (maternal diabetes and large fetus), it may be wise to move quickly to delivery of the posterior arm.15,16 In high-risk situations, delivery of the posterior arm is the maneuver with the greatest likelihood of resolving a severe shoulder dystocia, with the least force applied to the brachial plexus that is trapped under the mother’s symphysis pubis.
SHOULDER DYSTOCIA?
Most of our monthly Medical Verdicts columns include cases about shoulder dystocia, brachial plexus injury, or Erb’s palsy. CLICK HERE to read those from 2012 and 2013.
Practice, and then practice some more
A difficult-to-resolve shoulder dystocia is one of the most dramatic and frightening obstetric events. We know that we will all experience such cases. If we prepare well and frequently practice shoulder dystocia maneuvers, the dread of being responsible for resolving a shoulder dystocia will diminish. In most cases we will be able to report, “Mother and newborn safely birthed.”
INSTANT POLL: In your experience, what can clinicians do to reduce their exposure to brachial plexus injury litigation? Click here to respond.
1. Acker DB, Sachs BP, Friedman EA. Risk factors for shoulder dystocia. Obstet Gynecol. 1985;66(6):762-768.
2. Benedetti TJ, Gabbe SG. Shoulder dystocia: a complication of fetal macrosomia and prolonged second stage of labor with midpelvic delivery. Obstet Gynecol. 1978;52(5):526-529.
3. Gilbert WM, Nesbitt TS, Danielsen B. Associated factors in 1611 cases of brachial plexus injury. Obstet Gynecol. 1999;93(4):536-540.
4. Gonik B, Walker A, Grimm M. Mathematic modeling of forces associated with shoulder dystocia: a comparison of endogenous and exogenous sources. Am J Obstet Gynecol. 2000;182(3):689-691.
5. Rouse DJ, Owen J, Goldenberg RL, Cliver SP. The effectiveness and costs of elective cesarean delivery for fetal macrosomia diagnosed by ultrasound. JAMA. 1996;276(18):1480-1486.
6. Ecker JL, Greenberg JA, Norwitz ER, Nadel AS, Repke JT. Birth weight as a predictor of brachial plexus injury. Obstet Gynecol 1997;89(5 pt 1):643-647.
7. Bager B. Perinatally acquired brachial plexus palsy—a persisting challenge. Acta Paediatr. 1997;86(11):1216-1219.
8. Dawodu A, Sankaran-Kutty M, Rajan TV. Risk factors and prognosis for brachial plexus injury and clavicular fracture in neonates: a prospective analysis from the United Arab Emirates. Ann Trop Paediatr. 1997;17(3):195-200.
9. Pondaag W, Malessy MJA, van Dijk JG, Thomeer RT. Natural history of obstetric brachial plexus palsy: a systematic review. Dev Med Child Neurol. 2004;46(2):138-144.
10. Grossman JA. Early operative intervention for birth injuries to the brachial plexus. Semin Pediatr Neurol. 2000;7(1):36-43.
11. Institute of Medicine. Nielsen-Bohlman L Panzer AM, Kindig DA, eds. Health Literacy: A Prescription to End Confusion. Washington, DC: National Academies Press; 2004. http://www.nap.edu/openbook.php?isbn=0309091179. Accessed January 15, 2013.
12. Wu H, Nishimi RY, Page-Lopez CM, Kizer KW. Improving patient safety through informed consent for patients with limited health literacy. Washington DC; National Quality Forum; 2005. http://www.qualityforum.org/Publications/2005/09/Improving_Patient_Safety_Through_Informed_Consent_for_Patients_with_Limited_Health_Literacy.aspx. Accessed January 15, 2013.
13. The Joint Commission. Sentinel Event Alert Issue 30: Preventing infant death and injury during delivery. http://www.jointcommission.org/assets/1/18/SEA_30.PDF. Published July 21, 2004. Accessed January 15, 2013.
14. Patient safety checklist No. 6: documenting shoulder dystocia. Obstet Gynecol. 2012;120(2 pt 1):430-431.http://www.acog.org/Resources_And_Publications/Patient_Safety_Checklists_List. Accessed January 15 2013.
15. Poggi SH, Spong CY, Allen RH. Prioritizing posterior arm delivery during severe shoulder dystocia. Obstet Gynecol. 2003;101(5 pt 2):1068-1072.
16. Hoffman MK, Bailit JL, Branch DW, et al. Consortium on Safe Labor. A comparison of obstetric maneuvers for the acute management of shoulder dystocia. Obstet Gynecol. 2011;117(6):1272-1278.

Robert L. Barbieri, MD
Editor in Chief
rbarbieri@frontlinemedcom.com
Robert L. Barbieri, MD
Editor in Chief
rbarbieri@frontlinemedcom.com
Robert L. Barbieri, MD
Editor in Chief
rbarbieri@frontlinemedcom.com
Delivery of the shoulders often gets overlooked in discussions
of episiotomy
(Comment & Controversy, November 2012)
Difficult fetal extraction at cesarean delivery:
What should you do?
Robert L. Barbieri, MD (Editorial, January 2012)
What is the significance of the head-to-body delivery interval
in shoulder dystocia?
William A. Grobman, MD, MBA (Examining the Evidence, December 2011)
Does the use of multiple maneuvers in the management of shoulder dystocia increase the risk of neonatal injury?
Robert B. Gherman, MD (Examining the Evidence, August 2011)
CASE: Shoulder dystocia resulting in persistent injury to C5 and C6
A 30-year-old, G2P1 woman presented in labor at 39 weeks and reported a strong desire to have a natural childbirth. She was taking insulin for gestational diabetes mellitus diagnosed in the second trimester. Her body mass index was 43 kg/m2, and her height was 4 ft 11 in. The estimated fetal weight was 9 lb. She had a prior vaginal delivery. During her antepartum care the patient was extensively counseled about the risk of shoulder dystocia and obstetric brachial plexus (OBP) injury.
The patient progressed normally through labor without anesthesia. At birth, the baby delivered occiput posterior and restituted to right occiput transverse. There was a turtle sign, and the obstetrician diagnosed a shoulder dystocia, called for help, and told the mother to stop pushing. An attempt to deliver the fetal head with gentle downward guidance was unsuccessful. The McRoberts maneuver and suprapubic pressure combined with gentle downward guidance on the fetal head did not result in delivery. A mediolateral episiotomy was made and the Rubin and Wood maneuvers were attempted without success. The obstetrician then successfully delivered the posterior arm and the body of the baby was easily delivered.
The shoulder dystocia lasted 2 minutes before successful delivery. The Apgar scores were 3 and 6 at one and five minutes, respectively. The umbilical cord artery pH was 7.18. The birthweight was 9 lb 2 oz. A diagnosis of OBP injury involving C5 and C6 was made. At discharge the OBP injury persisted.
What is OBP injury?
Shoulder dystocia, which affected this mother and fetus, is a problem involving the impaction of the fetal shoulder behind the maternal symphysis pubis. Shoulder dystocia is a “bony problem.” Although shoulder dystocia cannot be predicted reliably, risk factors include:
- fetal macrosomia
- maternal diabetes
- maternal weight gain
- prepregnancy obesity
- multiparity
- operative vaginal delivery.1-3
The injury can be serious and permanent. The feared consequence of shoulder dystocia is permanent obstetric brachial plexus injury and/or fetal neurologic damage caused by reduced cord blood flow and fetal asphyxia. Occasionally, shoulder dystocia results in fetal death.
Trunks and cords of the brachial plexus
C5 and C6 roots merge to form the upper trunk, C7 root forms the middle trunk, and C8 and T1 roots merge to form the lower trunk.
How can an OBP injury occur?
Most cases are unilateral and arise when one or more of the brachial plexus nerves ( Figure ) are compromised. The forces of labor, fetal position, maternal pushing, and force applied to the fetal head and neck by a clinician all may contribute to an OBP injury.4 It is important to note that up to one-third of all OBP injuries occur in births not associated with a recognized shoulder dystocia.5
Erb’s palsy. Injuries to the C5 and C6 nerves account for about 50% of cases. The muscle groups impacted by this injury include the deltoid and infraspinatus muscles (mainly C5) and the biceps muscle (mainly C6). This pattern results in an adducted and internally rotated upper arm, an extended forearm, with preservation of hand and wrist movement.
Erb’s palsy plus. Injury to C5, C6, and C7 nerves accounts for about 35% of cases and manifests as adduction and internal rotation of the arm, extension and pronation of the forearm, plus flexion of the wrist and fingers—the so-called waiter’s tip posture.
Klumpke’s palsy. Isolated injury to the C8 nerve and T1 root occurs infrequently and manifests as isolated hand paralysis and Horner’s syndrome.
Approximately one in five OBP injuries persist for years following birth. The incidence of OBP injury ranges from 1.0 to 3.0 cases per 1,000 births.6-8 In a review of studies with at least 3 years of follow-up and less than 10% loss to follow-up, the authors reported that the three best studies observed a risk of persistent OBP of 10%, 19%, and 27%.9
Long-term management of OBP injury
The optimal approach to management of OBP injury is unknown because few high-quality studies are available to guide therapy. Typically, 3 to 9 months of observation and physical therapy are recommended following birth, with the hope that the majority of newborns will recover some or almost all function. Physical therapy is focused on reducing the occurrence of joint contractures and maintaining range of motion in the shoulder, elbow, wrist, and fingers.
Surgical exploration of the plexus is often advised when biceps muscle function is absent at 3 months of age. Some surgeons recommend waiting until 9 months before pursuing surgical exploration.10 No randomized trials have been performed demonstrating the value of surgical intervention, but case series report that surgical intervention with nerve grafting or nerve transfer is superior to management without neurosurgery.
The consequences of permanent OBP injury
A lifetime of corrective therapy for the child. OBP injury may result in a permanent brachial plexus injury—permanent arm weakness requiring decades of physical therapy and multiple surgeries to try to reduce functional disabilities. Problems that frequently occur in children with OBP injury include:
- shoulder contractures
- limb length differences
- winged scapula
- behavioral and developmental problems.
A patient’s care may be coordinated at a brachial plexus injury specialty center, where coordinated access to pediatric neurologists, neurosurgeons, orthopedic surgeons, and neurophysiologists is available and physical and occupational therapy are provided.
Years of emotional response for the parents. Following a birth complicated by shoulder dystocia, the parents may experience grief and anger. During the decades following the birth, the parents of the child will wonder if the injury could have been avoided. They may be asked by friends and relatives, “Would a cesarean delivery have prevented the injury?” Physical therapists, pediatric neurologists, orthopedic and neurosurgeons may reinforce the idea that the injury was caused when the obstetrician applied excessive lateral force to the head and neck, resulting in an injury to the brachial plexus.
Decades-long exposure to these ideas, unresolved anger, financial stress, and lingering doubts may result in the parents and child pursuing civil litigation against the delivering clinician.
Can we reduce the incidence of OBP injury and our risk of litigation?
There are no interventions proven to reduce the incidence of OBP injury. However, many experts advise that a multifaceted approach to this obstetric emergency may reduce the incidence of severe OBP injury at the same time that we reduce our risk of litigation.
When counseling patients about the risk for OBP injury, use teach-back. Patients tend to misunderstand or forget much of what their clinicians teach them.11 Teach-back is an iterative communication process in which the clinician teaches the patient a concept or technique, then asks the patient to repeat the concept in their own words or demonstrate the technique. The clinician then amplifies the concept or technique and corrects misunderstandings. The patient is then asked to repeat the concept or demonstrate the technique. When using teach-back, the clinician never asks, “Do you understand?” The clinician encourages the patient to teach the concept to the clinician using the patient’s own words.12
In the case above, the patient has multiple risk factors for shoulder dystocia, including obesity, short stature, insulin-treated gestational diabetes, and a large fetus. Given the high risk for shoulder dystocia, teach-back might help the patient better understand the situation. After explaining the concepts to the patient, the teach-back questions to the patient might include:
- “Can you tell me what is a shoulder dystocia?”
- “Can you list the health conditions that you have that increase your baby’s risk of shoulder dystocia?”
- “When a shoulder dystocia occurs, what actions will we take at birth to try to fix the shoulder dystocia?”
- “When a baby has experienced a shoulder dystocia, what can happen to the baby’s arm?”
Regularly perform multidisciplinary shoulder dystocia drills. The Joint Commission recommends that clinical drills be performed to help staff prepare for high-risk labor and delivery events, including shoulder dystocia, emergency cesarean delivery, and maternal hemorrhage.13
When shoulder dystocia occurs, extensively chart the event and interventions used. The American College of Obstetricians and Gynecologists has developed a patient safety checklist focused on key clinical elements in the antepartum, intrapartum, and postpartum periods and overall timing of the delivery to document when a shoulder dystocia occurs.14
Stop using the term “traction” in the medical record and obstetric literature. Words are meaningful and open to multiple interpretations. Often, words have unintended consequences. Plaintiff attorneys often highlight the obstetrician’s use of “traction” or “excessive traction” as the cause of an OBP injury. Orthopedic surgeons and pediatricians often state in their records that the OBP injury was a “traction injury,” further supporting the plaintiff attorney’s contention that excessive traction applied by the obstetrician caused the traction injury. Obstetricians do not use traction to deliver a baby. Motorized tractors generate traction, not obstetricians. We use gentle downward guidance to deliver the fetal shoulders and body.
In a high-risk situation, proceed quickly to delivery of the posterior arm. When you recognize a shoulder dystocia in a high-risk situation (maternal diabetes and large fetus), it may be wise to move quickly to delivery of the posterior arm.15,16 In high-risk situations, delivery of the posterior arm is the maneuver with the greatest likelihood of resolving a severe shoulder dystocia, with the least force applied to the brachial plexus that is trapped under the mother’s symphysis pubis.
SHOULDER DYSTOCIA?
Most of our monthly Medical Verdicts columns include cases about shoulder dystocia, brachial plexus injury, or Erb’s palsy. CLICK HERE to read those from 2012 and 2013.
Practice, and then practice some more
A difficult-to-resolve shoulder dystocia is one of the most dramatic and frightening obstetric events. We know that we will all experience such cases. If we prepare well and frequently practice shoulder dystocia maneuvers, the dread of being responsible for resolving a shoulder dystocia will diminish. In most cases we will be able to report, “Mother and newborn safely birthed.”
INSTANT POLL: In your experience, what can clinicians do to reduce their exposure to brachial plexus injury litigation? Click here to respond.
Delivery of the shoulders often gets overlooked in discussions
of episiotomy
(Comment & Controversy, November 2012)
Difficult fetal extraction at cesarean delivery:
What should you do?
Robert L. Barbieri, MD (Editorial, January 2012)
What is the significance of the head-to-body delivery interval
in shoulder dystocia?
William A. Grobman, MD, MBA (Examining the Evidence, December 2011)
Does the use of multiple maneuvers in the management of shoulder dystocia increase the risk of neonatal injury?
Robert B. Gherman, MD (Examining the Evidence, August 2011)
CASE: Shoulder dystocia resulting in persistent injury to C5 and C6
A 30-year-old, G2P1 woman presented in labor at 39 weeks and reported a strong desire to have a natural childbirth. She was taking insulin for gestational diabetes mellitus diagnosed in the second trimester. Her body mass index was 43 kg/m2, and her height was 4 ft 11 in. The estimated fetal weight was 9 lb. She had a prior vaginal delivery. During her antepartum care the patient was extensively counseled about the risk of shoulder dystocia and obstetric brachial plexus (OBP) injury.
The patient progressed normally through labor without anesthesia. At birth, the baby delivered occiput posterior and restituted to right occiput transverse. There was a turtle sign, and the obstetrician diagnosed a shoulder dystocia, called for help, and told the mother to stop pushing. An attempt to deliver the fetal head with gentle downward guidance was unsuccessful. The McRoberts maneuver and suprapubic pressure combined with gentle downward guidance on the fetal head did not result in delivery. A mediolateral episiotomy was made and the Rubin and Wood maneuvers were attempted without success. The obstetrician then successfully delivered the posterior arm and the body of the baby was easily delivered.
The shoulder dystocia lasted 2 minutes before successful delivery. The Apgar scores were 3 and 6 at one and five minutes, respectively. The umbilical cord artery pH was 7.18. The birthweight was 9 lb 2 oz. A diagnosis of OBP injury involving C5 and C6 was made. At discharge the OBP injury persisted.
What is OBP injury?
Shoulder dystocia, which affected this mother and fetus, is a problem involving the impaction of the fetal shoulder behind the maternal symphysis pubis. Shoulder dystocia is a “bony problem.” Although shoulder dystocia cannot be predicted reliably, risk factors include:
- fetal macrosomia
- maternal diabetes
- maternal weight gain
- prepregnancy obesity
- multiparity
- operative vaginal delivery.1-3
The injury can be serious and permanent. The feared consequence of shoulder dystocia is permanent obstetric brachial plexus injury and/or fetal neurologic damage caused by reduced cord blood flow and fetal asphyxia. Occasionally, shoulder dystocia results in fetal death.
Trunks and cords of the brachial plexus
C5 and C6 roots merge to form the upper trunk, C7 root forms the middle trunk, and C8 and T1 roots merge to form the lower trunk.
How can an OBP injury occur?
Most cases are unilateral and arise when one or more of the brachial plexus nerves ( Figure ) are compromised. The forces of labor, fetal position, maternal pushing, and force applied to the fetal head and neck by a clinician all may contribute to an OBP injury.4 It is important to note that up to one-third of all OBP injuries occur in births not associated with a recognized shoulder dystocia.5
Erb’s palsy. Injuries to the C5 and C6 nerves account for about 50% of cases. The muscle groups impacted by this injury include the deltoid and infraspinatus muscles (mainly C5) and the biceps muscle (mainly C6). This pattern results in an adducted and internally rotated upper arm, an extended forearm, with preservation of hand and wrist movement.
Erb’s palsy plus. Injury to C5, C6, and C7 nerves accounts for about 35% of cases and manifests as adduction and internal rotation of the arm, extension and pronation of the forearm, plus flexion of the wrist and fingers—the so-called waiter’s tip posture.
Klumpke’s palsy. Isolated injury to the C8 nerve and T1 root occurs infrequently and manifests as isolated hand paralysis and Horner’s syndrome.
Approximately one in five OBP injuries persist for years following birth. The incidence of OBP injury ranges from 1.0 to 3.0 cases per 1,000 births.6-8 In a review of studies with at least 3 years of follow-up and less than 10% loss to follow-up, the authors reported that the three best studies observed a risk of persistent OBP of 10%, 19%, and 27%.9
Long-term management of OBP injury
The optimal approach to management of OBP injury is unknown because few high-quality studies are available to guide therapy. Typically, 3 to 9 months of observation and physical therapy are recommended following birth, with the hope that the majority of newborns will recover some or almost all function. Physical therapy is focused on reducing the occurrence of joint contractures and maintaining range of motion in the shoulder, elbow, wrist, and fingers.
Surgical exploration of the plexus is often advised when biceps muscle function is absent at 3 months of age. Some surgeons recommend waiting until 9 months before pursuing surgical exploration.10 No randomized trials have been performed demonstrating the value of surgical intervention, but case series report that surgical intervention with nerve grafting or nerve transfer is superior to management without neurosurgery.
The consequences of permanent OBP injury
A lifetime of corrective therapy for the child. OBP injury may result in a permanent brachial plexus injury—permanent arm weakness requiring decades of physical therapy and multiple surgeries to try to reduce functional disabilities. Problems that frequently occur in children with OBP injury include:
- shoulder contractures
- limb length differences
- winged scapula
- behavioral and developmental problems.
A patient’s care may be coordinated at a brachial plexus injury specialty center, where coordinated access to pediatric neurologists, neurosurgeons, orthopedic surgeons, and neurophysiologists is available and physical and occupational therapy are provided.
Years of emotional response for the parents. Following a birth complicated by shoulder dystocia, the parents may experience grief and anger. During the decades following the birth, the parents of the child will wonder if the injury could have been avoided. They may be asked by friends and relatives, “Would a cesarean delivery have prevented the injury?” Physical therapists, pediatric neurologists, orthopedic and neurosurgeons may reinforce the idea that the injury was caused when the obstetrician applied excessive lateral force to the head and neck, resulting in an injury to the brachial plexus.
Decades-long exposure to these ideas, unresolved anger, financial stress, and lingering doubts may result in the parents and child pursuing civil litigation against the delivering clinician.
Can we reduce the incidence of OBP injury and our risk of litigation?
There are no interventions proven to reduce the incidence of OBP injury. However, many experts advise that a multifaceted approach to this obstetric emergency may reduce the incidence of severe OBP injury at the same time that we reduce our risk of litigation.
When counseling patients about the risk for OBP injury, use teach-back. Patients tend to misunderstand or forget much of what their clinicians teach them.11 Teach-back is an iterative communication process in which the clinician teaches the patient a concept or technique, then asks the patient to repeat the concept in their own words or demonstrate the technique. The clinician then amplifies the concept or technique and corrects misunderstandings. The patient is then asked to repeat the concept or demonstrate the technique. When using teach-back, the clinician never asks, “Do you understand?” The clinician encourages the patient to teach the concept to the clinician using the patient’s own words.12
In the case above, the patient has multiple risk factors for shoulder dystocia, including obesity, short stature, insulin-treated gestational diabetes, and a large fetus. Given the high risk for shoulder dystocia, teach-back might help the patient better understand the situation. After explaining the concepts to the patient, the teach-back questions to the patient might include:
- “Can you tell me what is a shoulder dystocia?”
- “Can you list the health conditions that you have that increase your baby’s risk of shoulder dystocia?”
- “When a shoulder dystocia occurs, what actions will we take at birth to try to fix the shoulder dystocia?”
- “When a baby has experienced a shoulder dystocia, what can happen to the baby’s arm?”
Regularly perform multidisciplinary shoulder dystocia drills. The Joint Commission recommends that clinical drills be performed to help staff prepare for high-risk labor and delivery events, including shoulder dystocia, emergency cesarean delivery, and maternal hemorrhage.13
When shoulder dystocia occurs, extensively chart the event and interventions used. The American College of Obstetricians and Gynecologists has developed a patient safety checklist focused on key clinical elements in the antepartum, intrapartum, and postpartum periods and overall timing of the delivery to document when a shoulder dystocia occurs.14
Stop using the term “traction” in the medical record and obstetric literature. Words are meaningful and open to multiple interpretations. Often, words have unintended consequences. Plaintiff attorneys often highlight the obstetrician’s use of “traction” or “excessive traction” as the cause of an OBP injury. Orthopedic surgeons and pediatricians often state in their records that the OBP injury was a “traction injury,” further supporting the plaintiff attorney’s contention that excessive traction applied by the obstetrician caused the traction injury. Obstetricians do not use traction to deliver a baby. Motorized tractors generate traction, not obstetricians. We use gentle downward guidance to deliver the fetal shoulders and body.
In a high-risk situation, proceed quickly to delivery of the posterior arm. When you recognize a shoulder dystocia in a high-risk situation (maternal diabetes and large fetus), it may be wise to move quickly to delivery of the posterior arm.15,16 In high-risk situations, delivery of the posterior arm is the maneuver with the greatest likelihood of resolving a severe shoulder dystocia, with the least force applied to the brachial plexus that is trapped under the mother’s symphysis pubis.
SHOULDER DYSTOCIA?
Most of our monthly Medical Verdicts columns include cases about shoulder dystocia, brachial plexus injury, or Erb’s palsy. CLICK HERE to read those from 2012 and 2013.
Practice, and then practice some more
A difficult-to-resolve shoulder dystocia is one of the most dramatic and frightening obstetric events. We know that we will all experience such cases. If we prepare well and frequently practice shoulder dystocia maneuvers, the dread of being responsible for resolving a shoulder dystocia will diminish. In most cases we will be able to report, “Mother and newborn safely birthed.”
INSTANT POLL: In your experience, what can clinicians do to reduce their exposure to brachial plexus injury litigation? Click here to respond.
1. Acker DB, Sachs BP, Friedman EA. Risk factors for shoulder dystocia. Obstet Gynecol. 1985;66(6):762-768.
2. Benedetti TJ, Gabbe SG. Shoulder dystocia: a complication of fetal macrosomia and prolonged second stage of labor with midpelvic delivery. Obstet Gynecol. 1978;52(5):526-529.
3. Gilbert WM, Nesbitt TS, Danielsen B. Associated factors in 1611 cases of brachial plexus injury. Obstet Gynecol. 1999;93(4):536-540.
4. Gonik B, Walker A, Grimm M. Mathematic modeling of forces associated with shoulder dystocia: a comparison of endogenous and exogenous sources. Am J Obstet Gynecol. 2000;182(3):689-691.
5. Rouse DJ, Owen J, Goldenberg RL, Cliver SP. The effectiveness and costs of elective cesarean delivery for fetal macrosomia diagnosed by ultrasound. JAMA. 1996;276(18):1480-1486.
6. Ecker JL, Greenberg JA, Norwitz ER, Nadel AS, Repke JT. Birth weight as a predictor of brachial plexus injury. Obstet Gynecol 1997;89(5 pt 1):643-647.
7. Bager B. Perinatally acquired brachial plexus palsy—a persisting challenge. Acta Paediatr. 1997;86(11):1216-1219.
8. Dawodu A, Sankaran-Kutty M, Rajan TV. Risk factors and prognosis for brachial plexus injury and clavicular fracture in neonates: a prospective analysis from the United Arab Emirates. Ann Trop Paediatr. 1997;17(3):195-200.
9. Pondaag W, Malessy MJA, van Dijk JG, Thomeer RT. Natural history of obstetric brachial plexus palsy: a systematic review. Dev Med Child Neurol. 2004;46(2):138-144.
10. Grossman JA. Early operative intervention for birth injuries to the brachial plexus. Semin Pediatr Neurol. 2000;7(1):36-43.
11. Institute of Medicine. Nielsen-Bohlman L Panzer AM, Kindig DA, eds. Health Literacy: A Prescription to End Confusion. Washington, DC: National Academies Press; 2004. http://www.nap.edu/openbook.php?isbn=0309091179. Accessed January 15, 2013.
12. Wu H, Nishimi RY, Page-Lopez CM, Kizer KW. Improving patient safety through informed consent for patients with limited health literacy. Washington DC; National Quality Forum; 2005. http://www.qualityforum.org/Publications/2005/09/Improving_Patient_Safety_Through_Informed_Consent_for_Patients_with_Limited_Health_Literacy.aspx. Accessed January 15, 2013.
13. The Joint Commission. Sentinel Event Alert Issue 30: Preventing infant death and injury during delivery. http://www.jointcommission.org/assets/1/18/SEA_30.PDF. Published July 21, 2004. Accessed January 15, 2013.
14. Patient safety checklist No. 6: documenting shoulder dystocia. Obstet Gynecol. 2012;120(2 pt 1):430-431.http://www.acog.org/Resources_And_Publications/Patient_Safety_Checklists_List. Accessed January 15 2013.
15. Poggi SH, Spong CY, Allen RH. Prioritizing posterior arm delivery during severe shoulder dystocia. Obstet Gynecol. 2003;101(5 pt 2):1068-1072.
16. Hoffman MK, Bailit JL, Branch DW, et al. Consortium on Safe Labor. A comparison of obstetric maneuvers for the acute management of shoulder dystocia. Obstet Gynecol. 2011;117(6):1272-1278.
1. Acker DB, Sachs BP, Friedman EA. Risk factors for shoulder dystocia. Obstet Gynecol. 1985;66(6):762-768.
2. Benedetti TJ, Gabbe SG. Shoulder dystocia: a complication of fetal macrosomia and prolonged second stage of labor with midpelvic delivery. Obstet Gynecol. 1978;52(5):526-529.
3. Gilbert WM, Nesbitt TS, Danielsen B. Associated factors in 1611 cases of brachial plexus injury. Obstet Gynecol. 1999;93(4):536-540.
4. Gonik B, Walker A, Grimm M. Mathematic modeling of forces associated with shoulder dystocia: a comparison of endogenous and exogenous sources. Am J Obstet Gynecol. 2000;182(3):689-691.
5. Rouse DJ, Owen J, Goldenberg RL, Cliver SP. The effectiveness and costs of elective cesarean delivery for fetal macrosomia diagnosed by ultrasound. JAMA. 1996;276(18):1480-1486.
6. Ecker JL, Greenberg JA, Norwitz ER, Nadel AS, Repke JT. Birth weight as a predictor of brachial plexus injury. Obstet Gynecol 1997;89(5 pt 1):643-647.
7. Bager B. Perinatally acquired brachial plexus palsy—a persisting challenge. Acta Paediatr. 1997;86(11):1216-1219.
8. Dawodu A, Sankaran-Kutty M, Rajan TV. Risk factors and prognosis for brachial plexus injury and clavicular fracture in neonates: a prospective analysis from the United Arab Emirates. Ann Trop Paediatr. 1997;17(3):195-200.
9. Pondaag W, Malessy MJA, van Dijk JG, Thomeer RT. Natural history of obstetric brachial plexus palsy: a systematic review. Dev Med Child Neurol. 2004;46(2):138-144.
10. Grossman JA. Early operative intervention for birth injuries to the brachial plexus. Semin Pediatr Neurol. 2000;7(1):36-43.
11. Institute of Medicine. Nielsen-Bohlman L Panzer AM, Kindig DA, eds. Health Literacy: A Prescription to End Confusion. Washington, DC: National Academies Press; 2004. http://www.nap.edu/openbook.php?isbn=0309091179. Accessed January 15, 2013.
12. Wu H, Nishimi RY, Page-Lopez CM, Kizer KW. Improving patient safety through informed consent for patients with limited health literacy. Washington DC; National Quality Forum; 2005. http://www.qualityforum.org/Publications/2005/09/Improving_Patient_Safety_Through_Informed_Consent_for_Patients_with_Limited_Health_Literacy.aspx. Accessed January 15, 2013.
13. The Joint Commission. Sentinel Event Alert Issue 30: Preventing infant death and injury during delivery. http://www.jointcommission.org/assets/1/18/SEA_30.PDF. Published July 21, 2004. Accessed January 15, 2013.
14. Patient safety checklist No. 6: documenting shoulder dystocia. Obstet Gynecol. 2012;120(2 pt 1):430-431.http://www.acog.org/Resources_And_Publications/Patient_Safety_Checklists_List. Accessed January 15 2013.
15. Poggi SH, Spong CY, Allen RH. Prioritizing posterior arm delivery during severe shoulder dystocia. Obstet Gynecol. 2003;101(5 pt 2):1068-1072.
16. Hoffman MK, Bailit JL, Branch DW, et al. Consortium on Safe Labor. A comparison of obstetric maneuvers for the acute management of shoulder dystocia. Obstet Gynecol. 2011;117(6):1272-1278.