User login
Susan Connelly of Fruitland Park, Fla., is a volunteer at her local community hospital who until recently had never heard of a hospitalist. One day, she entered a hospital room and, as she regularly did with patients she visited, asked if there was anything the man in the bed needed.
“I want to know where my doctor is,” the patient said.
“You mean your doctor hasn’t seen you?” Connelly asked.
“No,” he said. “I’m not even sure he knows I’m here.”
Somewhat incredulous, Connelly retrieved the hospital’s physician handbook and helped the patient look up his physician’s phone number. “I didn’t think too much about it,” she says. But the following week, when she appeared at the hospital to volunteer, a supervisor called her into the office. The supervisor asked Connelly about the incident and gently admonished her for encouraging the patient to call his primary-care physician (PCP), as “a hospitalist is working with him now.”
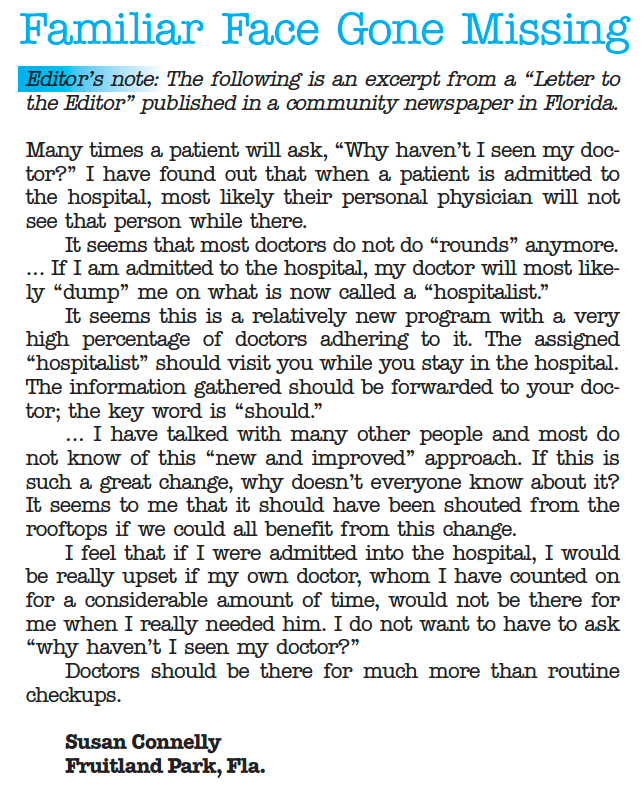
“A what? I had never even heard the term,” Connelly says. She asked her fellow volunteers, known as patient representatives at her hospital, if they had ever heard of a hospitalist. One had, but only because her husband had been admitted for a hospital stay. Concerned, Connelly wrote letters to the editors of two local newspapers. Both were published (see Figure 2, “Familiar Face Gone Missing,” p. 30).
—Robert Centor, MD, associate dean of medicine, University of Alabama at Birmingham
“If I am admitted to the hospital, my doctor will most likely ‘dump’ me on what is now called a ‘hospitalist,’ ” she wrote. “Information gathered [by the hospitalist] should be forwarded to your doctor; the key word is ‘should.’ Why develop this long-term relationship with a doctor, if when you really need him, he is not there for you and you are dealing with a stranger?”
Why indeed?
It might not happen with every new admission, but patient fears are a reality. The uncertainty of a hospital stay, a new physician, and new medications can take their toll on the human psyche. Patients are upset with their PCP, the hospital, the system; many times it’s the hospitalist who feels the brunt of their anger. Not only do hospitalists have to calm a patient worried about PCP disconnect, but they also have to reassure the patient that they will be attentive to their needs, provide a high quality of care during the hospital stay, and communicate with their PCP about diagnoses, medications, and follow-up care. Hospitalists should weave in some of the documented plusses a hospitalist brings to the table: shorter length of stays, greater patient access and availability, and improved quality of care.
Although some patients might view hospitalists as “strangers,” HM physicians can learn methods to ease patient anxiety and answer tough questions from patients about the role they play in hospital care.
Restore Confidence
Simple conversations can help hospitalists defuse patient dissatisfaction. When a patient asks why their PCP won’t be seeing them in the hospital, it’s best to begin with a reassuring approach. For example, introduce yourself and say you have reviewed the case with their PCP. You can include key information from their medical history and recent hospitalizations, if appropriate.
Robert Centor, MD, a hospitalist and associate dean of medicine at the University of Alabama at Birmingham, suggests a few other key behaviors for initial patient visits. He finds a way to make appropriate physical contact by taking a pulse, checking the heart and lungs, or patting a shoulder to clearly embody the role of the physician in charge.
“And pull up a chair,” he says. “If there is no chair, bring in a chair. But sit down—always.”
Dr. Centor also recommends a transparent approach, “especially in hospital medicine,” he explains. “Be explicit about what you’re thinking, what you’re doing, and why you’re doing it.”1
Transparency can protect you as it informs and comforts patients and their families. For instance, “hospitalized patients are probably hearing from every relative they have and half the friends they have,” Dr. Centor says. “If one of those people is a physician, they may be second-guessing you. You can overcome their wariness by remembering that this is all about bedside manner and the explanations you give them, including discharge instructions.”
Dr. Centor says your bedside manner needs to fit your personality. When you talk to a patient, use language that matches your personality. You can adopt someone else’s introductory script; just make sure to modify it to fit your work environment (see “Strategies to Ease Patient Concerns,” p. 29).
“What Is This?”
Earlier this year, CJ Clarke of Leesburg, Fla., underwent a colonoscopy screening at a local doctor’s office. She had been kept on warfarin (Coumadin) to prevent complications, but after she bled for four days from a puncture sustained during the procedure, she went to the ED. She was admitted, but it wasn’t until the following afternoon that she learned that hospitalists—not her PCP— would be taking care of her.
“This totally unknown guy came in and said he would be filling in for my doctor and communicating with [my PCP],” Clarke says. “It was a weekend, and it turns out the first hospitalist was a substitute hospitalist, so then I got another hospitalist. The first one was subbing for the first hospitalist. I wasn’t exactly mad, but I thought, what is this?”
Clarke thought the first hospitalist was knowledgeable; she took comfort in that. “But the second one was extremely knowledgeable and explained the differences between Coumadin and heparin. He really knew his stuff. He talked to my cardiologist when she came in,” Clarke says. “The only thing that I was sorry about was that my primary didn’t seem to get the information very rapidly.”
Care coordination is a vital step in the discharge process, especially when patients think the flow of information between a hospital and a PCP is immediate and seamless. When Clarke was discharged and she returned home, she scheduled an appointment with her PCP. “When I first called, my [PCP] had not even heard I had been admitted,” Clarke says. But by the time she visited the PCP, “she knew everything. … I think it would have been good if sometime during that five-day hospitalization, she had been told—not afterward. Not that she would have come in, because that is not her policy, but just to know she knew.”
HM’s Role: Extended Education
Many HM groups have designated policies for educating patients and assuaging their fears. Because some PCPs might feel left out of the loop when hospitalists care for their patients, these strategies go beyond patient education.
One of the first steps is to involve PCPs in meaningful ways in their patients’ hospital care. When a patient is particularly angered by his PCP’s absence, invite the PCP to visit, or call the PCP more often and let the patient know you’re doing so. As proposed by Bob Wachter, MD, professor and chief of the division of hospital medicine at the University of California at San Francisco, a former SHM president, and author of the blog “Wachter’s World,” and Steven Pantilat, MD, FHM, professor of clinical medicine in the division of hospital medicine at UCSF, and a former SHM president, “the PCP can endorse the hospitalist model and the individual hospitalist, notice subtle findings that differ from the patient’s baseline, and help clarify patient preferences regarding difficult situations by drawing on their previous relationship with the patient. This visit may also benefit the PCP by providing insights into the patient’s illness, personality, or social support that he or she was unaware of previously.”2,3
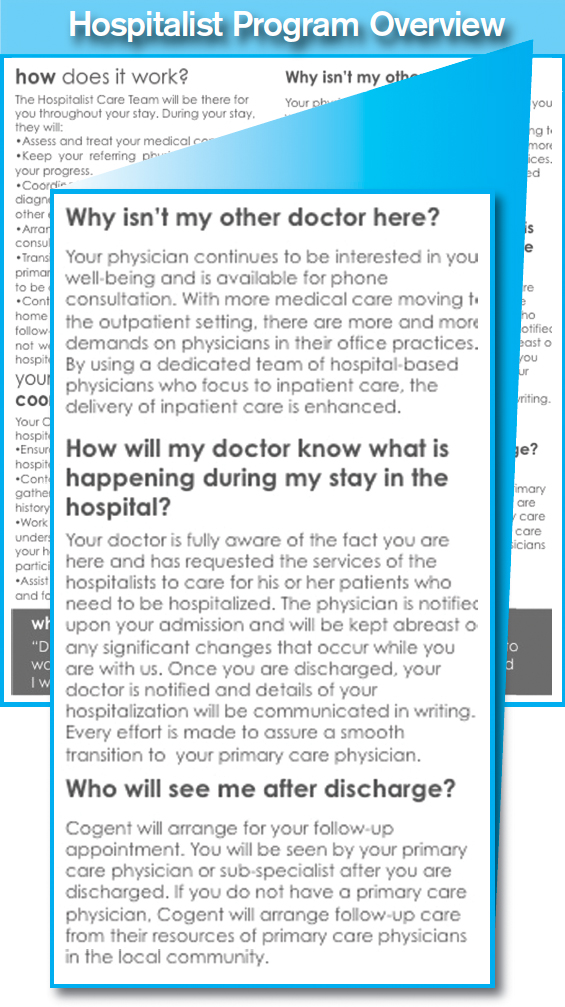
Cogent Healthcare uses an outreach program to calm patient fears and connect with PCPs. The Brentwood, Tenn.-based hospitalist company distributes patient education pamphlets to the PCPs with whom they work, and distributes a flier on admission to show patients the photographs and names of their HM team (see “Make Patient Education A Priority,” p. 29).
Hospitalist training in this arena helps prepare physicians for a potentially uncomfortable work environment. “We need to stress in residency training the specific issue of helping make the patient feel comfortable when their own doctor is not seeing them in the hospital,” Dr. Centor says. “Most young hospitalists right out of their residencies have not experienced primary-care practice, and, so far, we don’t know how to get around that.”
Hospitalist groups also should consider broad initiatives to bring hospitalists together with patient representatives and other volunteers who work with patients. If volunteers are ignored in the educational outreach process, it could exacerbate patients’ negative reactions. Teach volunteers what hospitalists are, their benefit to care delivery, and their value in upholding the mission of quality HM. TH
Andrea Sattinger is a freelance writer based in North Carolina.
References
- Centor RM. A hospitalist inpatient system does not improve patient care outcomes. Arch Intern Med. 2008;168(12):1257-1258.
- Lo B. Ethical and policy implications of hospitalist systems. Dis Mon. 2002;48(4):281-290.
- Wachter RM, Pantilat SZ. The “continuity visit” and the hospitalist model of care. Dis Mon. 2002;48(4): 267-272.
Image Source: PETRI ARTTURI ASIKAINEN / GETTY IMAGES
Susan Connelly of Fruitland Park, Fla., is a volunteer at her local community hospital who until recently had never heard of a hospitalist. One day, she entered a hospital room and, as she regularly did with patients she visited, asked if there was anything the man in the bed needed.
“I want to know where my doctor is,” the patient said.
“You mean your doctor hasn’t seen you?” Connelly asked.
“No,” he said. “I’m not even sure he knows I’m here.”
Somewhat incredulous, Connelly retrieved the hospital’s physician handbook and helped the patient look up his physician’s phone number. “I didn’t think too much about it,” she says. But the following week, when she appeared at the hospital to volunteer, a supervisor called her into the office. The supervisor asked Connelly about the incident and gently admonished her for encouraging the patient to call his primary-care physician (PCP), as “a hospitalist is working with him now.”
“A what? I had never even heard the term,” Connelly says. She asked her fellow volunteers, known as patient representatives at her hospital, if they had ever heard of a hospitalist. One had, but only because her husband had been admitted for a hospital stay. Concerned, Connelly wrote letters to the editors of two local newspapers. Both were published (see Figure 2, “Familiar Face Gone Missing,” p. 30).
—Robert Centor, MD, associate dean of medicine, University of Alabama at Birmingham
“If I am admitted to the hospital, my doctor will most likely ‘dump’ me on what is now called a ‘hospitalist,’ ” she wrote. “Information gathered [by the hospitalist] should be forwarded to your doctor; the key word is ‘should.’ Why develop this long-term relationship with a doctor, if when you really need him, he is not there for you and you are dealing with a stranger?”
Why indeed?
It might not happen with every new admission, but patient fears are a reality. The uncertainty of a hospital stay, a new physician, and new medications can take their toll on the human psyche. Patients are upset with their PCP, the hospital, the system; many times it’s the hospitalist who feels the brunt of their anger. Not only do hospitalists have to calm a patient worried about PCP disconnect, but they also have to reassure the patient that they will be attentive to their needs, provide a high quality of care during the hospital stay, and communicate with their PCP about diagnoses, medications, and follow-up care. Hospitalists should weave in some of the documented plusses a hospitalist brings to the table: shorter length of stays, greater patient access and availability, and improved quality of care.
Although some patients might view hospitalists as “strangers,” HM physicians can learn methods to ease patient anxiety and answer tough questions from patients about the role they play in hospital care.
Restore Confidence
Simple conversations can help hospitalists defuse patient dissatisfaction. When a patient asks why their PCP won’t be seeing them in the hospital, it’s best to begin with a reassuring approach. For example, introduce yourself and say you have reviewed the case with their PCP. You can include key information from their medical history and recent hospitalizations, if appropriate.
Robert Centor, MD, a hospitalist and associate dean of medicine at the University of Alabama at Birmingham, suggests a few other key behaviors for initial patient visits. He finds a way to make appropriate physical contact by taking a pulse, checking the heart and lungs, or patting a shoulder to clearly embody the role of the physician in charge.
“And pull up a chair,” he says. “If there is no chair, bring in a chair. But sit down—always.”
Dr. Centor also recommends a transparent approach, “especially in hospital medicine,” he explains. “Be explicit about what you’re thinking, what you’re doing, and why you’re doing it.”1
Transparency can protect you as it informs and comforts patients and their families. For instance, “hospitalized patients are probably hearing from every relative they have and half the friends they have,” Dr. Centor says. “If one of those people is a physician, they may be second-guessing you. You can overcome their wariness by remembering that this is all about bedside manner and the explanations you give them, including discharge instructions.”
Dr. Centor says your bedside manner needs to fit your personality. When you talk to a patient, use language that matches your personality. You can adopt someone else’s introductory script; just make sure to modify it to fit your work environment (see “Strategies to Ease Patient Concerns,” p. 29).
“What Is This?”
Earlier this year, CJ Clarke of Leesburg, Fla., underwent a colonoscopy screening at a local doctor’s office. She had been kept on warfarin (Coumadin) to prevent complications, but after she bled for four days from a puncture sustained during the procedure, she went to the ED. She was admitted, but it wasn’t until the following afternoon that she learned that hospitalists—not her PCP— would be taking care of her.
“This totally unknown guy came in and said he would be filling in for my doctor and communicating with [my PCP],” Clarke says. “It was a weekend, and it turns out the first hospitalist was a substitute hospitalist, so then I got another hospitalist. The first one was subbing for the first hospitalist. I wasn’t exactly mad, but I thought, what is this?”
Clarke thought the first hospitalist was knowledgeable; she took comfort in that. “But the second one was extremely knowledgeable and explained the differences between Coumadin and heparin. He really knew his stuff. He talked to my cardiologist when she came in,” Clarke says. “The only thing that I was sorry about was that my primary didn’t seem to get the information very rapidly.”
Care coordination is a vital step in the discharge process, especially when patients think the flow of information between a hospital and a PCP is immediate and seamless. When Clarke was discharged and she returned home, she scheduled an appointment with her PCP. “When I first called, my [PCP] had not even heard I had been admitted,” Clarke says. But by the time she visited the PCP, “she knew everything. … I think it would have been good if sometime during that five-day hospitalization, she had been told—not afterward. Not that she would have come in, because that is not her policy, but just to know she knew.”
HM’s Role: Extended Education
Many HM groups have designated policies for educating patients and assuaging their fears. Because some PCPs might feel left out of the loop when hospitalists care for their patients, these strategies go beyond patient education.
One of the first steps is to involve PCPs in meaningful ways in their patients’ hospital care. When a patient is particularly angered by his PCP’s absence, invite the PCP to visit, or call the PCP more often and let the patient know you’re doing so. As proposed by Bob Wachter, MD, professor and chief of the division of hospital medicine at the University of California at San Francisco, a former SHM president, and author of the blog “Wachter’s World,” and Steven Pantilat, MD, FHM, professor of clinical medicine in the division of hospital medicine at UCSF, and a former SHM president, “the PCP can endorse the hospitalist model and the individual hospitalist, notice subtle findings that differ from the patient’s baseline, and help clarify patient preferences regarding difficult situations by drawing on their previous relationship with the patient. This visit may also benefit the PCP by providing insights into the patient’s illness, personality, or social support that he or she was unaware of previously.”2,3
Cogent Healthcare uses an outreach program to calm patient fears and connect with PCPs. The Brentwood, Tenn.-based hospitalist company distributes patient education pamphlets to the PCPs with whom they work, and distributes a flier on admission to show patients the photographs and names of their HM team (see “Make Patient Education A Priority,” p. 29).
Hospitalist training in this arena helps prepare physicians for a potentially uncomfortable work environment. “We need to stress in residency training the specific issue of helping make the patient feel comfortable when their own doctor is not seeing them in the hospital,” Dr. Centor says. “Most young hospitalists right out of their residencies have not experienced primary-care practice, and, so far, we don’t know how to get around that.”
Hospitalist groups also should consider broad initiatives to bring hospitalists together with patient representatives and other volunteers who work with patients. If volunteers are ignored in the educational outreach process, it could exacerbate patients’ negative reactions. Teach volunteers what hospitalists are, their benefit to care delivery, and their value in upholding the mission of quality HM. TH
Andrea Sattinger is a freelance writer based in North Carolina.
References
- Centor RM. A hospitalist inpatient system does not improve patient care outcomes. Arch Intern Med. 2008;168(12):1257-1258.
- Lo B. Ethical and policy implications of hospitalist systems. Dis Mon. 2002;48(4):281-290.
- Wachter RM, Pantilat SZ. The “continuity visit” and the hospitalist model of care. Dis Mon. 2002;48(4): 267-272.
Image Source: PETRI ARTTURI ASIKAINEN / GETTY IMAGES
Susan Connelly of Fruitland Park, Fla., is a volunteer at her local community hospital who until recently had never heard of a hospitalist. One day, she entered a hospital room and, as she regularly did with patients she visited, asked if there was anything the man in the bed needed.
“I want to know where my doctor is,” the patient said.
“You mean your doctor hasn’t seen you?” Connelly asked.
“No,” he said. “I’m not even sure he knows I’m here.”
Somewhat incredulous, Connelly retrieved the hospital’s physician handbook and helped the patient look up his physician’s phone number. “I didn’t think too much about it,” she says. But the following week, when she appeared at the hospital to volunteer, a supervisor called her into the office. The supervisor asked Connelly about the incident and gently admonished her for encouraging the patient to call his primary-care physician (PCP), as “a hospitalist is working with him now.”
“A what? I had never even heard the term,” Connelly says. She asked her fellow volunteers, known as patient representatives at her hospital, if they had ever heard of a hospitalist. One had, but only because her husband had been admitted for a hospital stay. Concerned, Connelly wrote letters to the editors of two local newspapers. Both were published (see Figure 2, “Familiar Face Gone Missing,” p. 30).
—Robert Centor, MD, associate dean of medicine, University of Alabama at Birmingham
“If I am admitted to the hospital, my doctor will most likely ‘dump’ me on what is now called a ‘hospitalist,’ ” she wrote. “Information gathered [by the hospitalist] should be forwarded to your doctor; the key word is ‘should.’ Why develop this long-term relationship with a doctor, if when you really need him, he is not there for you and you are dealing with a stranger?”
Why indeed?
It might not happen with every new admission, but patient fears are a reality. The uncertainty of a hospital stay, a new physician, and new medications can take their toll on the human psyche. Patients are upset with their PCP, the hospital, the system; many times it’s the hospitalist who feels the brunt of their anger. Not only do hospitalists have to calm a patient worried about PCP disconnect, but they also have to reassure the patient that they will be attentive to their needs, provide a high quality of care during the hospital stay, and communicate with their PCP about diagnoses, medications, and follow-up care. Hospitalists should weave in some of the documented plusses a hospitalist brings to the table: shorter length of stays, greater patient access and availability, and improved quality of care.
Although some patients might view hospitalists as “strangers,” HM physicians can learn methods to ease patient anxiety and answer tough questions from patients about the role they play in hospital care.
Restore Confidence
Simple conversations can help hospitalists defuse patient dissatisfaction. When a patient asks why their PCP won’t be seeing them in the hospital, it’s best to begin with a reassuring approach. For example, introduce yourself and say you have reviewed the case with their PCP. You can include key information from their medical history and recent hospitalizations, if appropriate.
Robert Centor, MD, a hospitalist and associate dean of medicine at the University of Alabama at Birmingham, suggests a few other key behaviors for initial patient visits. He finds a way to make appropriate physical contact by taking a pulse, checking the heart and lungs, or patting a shoulder to clearly embody the role of the physician in charge.
“And pull up a chair,” he says. “If there is no chair, bring in a chair. But sit down—always.”
Dr. Centor also recommends a transparent approach, “especially in hospital medicine,” he explains. “Be explicit about what you’re thinking, what you’re doing, and why you’re doing it.”1
Transparency can protect you as it informs and comforts patients and their families. For instance, “hospitalized patients are probably hearing from every relative they have and half the friends they have,” Dr. Centor says. “If one of those people is a physician, they may be second-guessing you. You can overcome their wariness by remembering that this is all about bedside manner and the explanations you give them, including discharge instructions.”
Dr. Centor says your bedside manner needs to fit your personality. When you talk to a patient, use language that matches your personality. You can adopt someone else’s introductory script; just make sure to modify it to fit your work environment (see “Strategies to Ease Patient Concerns,” p. 29).
“What Is This?”
Earlier this year, CJ Clarke of Leesburg, Fla., underwent a colonoscopy screening at a local doctor’s office. She had been kept on warfarin (Coumadin) to prevent complications, but after she bled for four days from a puncture sustained during the procedure, she went to the ED. She was admitted, but it wasn’t until the following afternoon that she learned that hospitalists—not her PCP— would be taking care of her.
“This totally unknown guy came in and said he would be filling in for my doctor and communicating with [my PCP],” Clarke says. “It was a weekend, and it turns out the first hospitalist was a substitute hospitalist, so then I got another hospitalist. The first one was subbing for the first hospitalist. I wasn’t exactly mad, but I thought, what is this?”
Clarke thought the first hospitalist was knowledgeable; she took comfort in that. “But the second one was extremely knowledgeable and explained the differences between Coumadin and heparin. He really knew his stuff. He talked to my cardiologist when she came in,” Clarke says. “The only thing that I was sorry about was that my primary didn’t seem to get the information very rapidly.”
Care coordination is a vital step in the discharge process, especially when patients think the flow of information between a hospital and a PCP is immediate and seamless. When Clarke was discharged and she returned home, she scheduled an appointment with her PCP. “When I first called, my [PCP] had not even heard I had been admitted,” Clarke says. But by the time she visited the PCP, “she knew everything. … I think it would have been good if sometime during that five-day hospitalization, she had been told—not afterward. Not that she would have come in, because that is not her policy, but just to know she knew.”
HM’s Role: Extended Education
Many HM groups have designated policies for educating patients and assuaging their fears. Because some PCPs might feel left out of the loop when hospitalists care for their patients, these strategies go beyond patient education.
One of the first steps is to involve PCPs in meaningful ways in their patients’ hospital care. When a patient is particularly angered by his PCP’s absence, invite the PCP to visit, or call the PCP more often and let the patient know you’re doing so. As proposed by Bob Wachter, MD, professor and chief of the division of hospital medicine at the University of California at San Francisco, a former SHM president, and author of the blog “Wachter’s World,” and Steven Pantilat, MD, FHM, professor of clinical medicine in the division of hospital medicine at UCSF, and a former SHM president, “the PCP can endorse the hospitalist model and the individual hospitalist, notice subtle findings that differ from the patient’s baseline, and help clarify patient preferences regarding difficult situations by drawing on their previous relationship with the patient. This visit may also benefit the PCP by providing insights into the patient’s illness, personality, or social support that he or she was unaware of previously.”2,3
Cogent Healthcare uses an outreach program to calm patient fears and connect with PCPs. The Brentwood, Tenn.-based hospitalist company distributes patient education pamphlets to the PCPs with whom they work, and distributes a flier on admission to show patients the photographs and names of their HM team (see “Make Patient Education A Priority,” p. 29).
Hospitalist training in this arena helps prepare physicians for a potentially uncomfortable work environment. “We need to stress in residency training the specific issue of helping make the patient feel comfortable when their own doctor is not seeing them in the hospital,” Dr. Centor says. “Most young hospitalists right out of their residencies have not experienced primary-care practice, and, so far, we don’t know how to get around that.”
Hospitalist groups also should consider broad initiatives to bring hospitalists together with patient representatives and other volunteers who work with patients. If volunteers are ignored in the educational outreach process, it could exacerbate patients’ negative reactions. Teach volunteers what hospitalists are, their benefit to care delivery, and their value in upholding the mission of quality HM. TH
Andrea Sattinger is a freelance writer based in North Carolina.
References
- Centor RM. A hospitalist inpatient system does not improve patient care outcomes. Arch Intern Med. 2008;168(12):1257-1258.
- Lo B. Ethical and policy implications of hospitalist systems. Dis Mon. 2002;48(4):281-290.
- Wachter RM, Pantilat SZ. The “continuity visit” and the hospitalist model of care. Dis Mon. 2002;48(4): 267-272.
Image Source: PETRI ARTTURI ASIKAINEN / GETTY IMAGES