User login
Skillful use of intravenous pain medications can be a powerful tool in the clinician’s pain management armamentarium. Yet many physicians are uncomfortable prescribing IV pain medications, especially opioids, even when their patients are experiencing severe pain—7-10 on the verbal analogue scale (VAS). This reticence, say the palliative care specialists interviewed for this article, may be due to a lack of training and knowledge, as well as misperceptions about proper use of IV opioids. The end result for patients can be inadequate pain control, which, according to researchers, continues to be a problem in U.S. hospitals.1
Even hospitalists not affiliated with a surgical service who do not treat perioperative patients are likely to encounter many different scenarios in which IV pain medications could appropriately address patients’ discomfort. David Ling, MD, a member of SHM’s Palliative Care Task Force, a hospitalist at Baystate Medical Center in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine (Boston), says patients who need IV pain medicines range from those with acute abdominal pain, pancreatitis, or small bowel obstructions to patients with end-stage cancer, renal disease, or congestive heart failure.
“It’s probably a bigger number on the medical service than most people realize,” he says.
The Short List
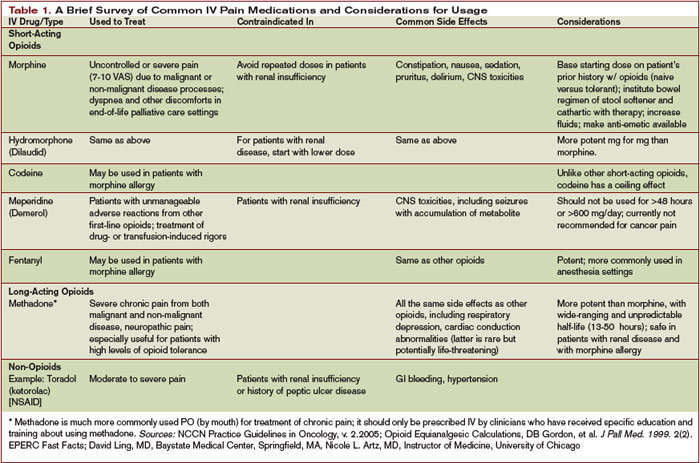
When it comes to effective IV pain medications very few choices exist, according to recommendations from the National Comprehensive Cancer Network and other pain advocacy organizations. An informal poll of interview sources corroborates this revelation.
“Morphine is the gold standard in pain control,” says Thomas Bookwalter, PharmD, clinical pharmacist on the General Medicine Service at the University of California at San Francisco (UCSF) Medical Center, a Health Sciences associate clinical professor at the UCSF School of Pharmacy, and a member of SHM’s Palliative Care Task Force.
Preferences for morphine or other opioids vary by practitioner and institution. For instance, says Dr. Bookwalter, the pain service at UCSF has been using hydromorphone more frequently of late.
Nicole L. Artz, MD, director of the Adult Sickle Cell Disease Care Team at the University of Chicago Hospitals and instructor of medicine at the University of Chicago Medical School, also occasionally uses IV infusions of ketorolac—a powerful NSAID designed for short-term management of moderately severe pain in adults. But, like morphine, it is contraindicated in patients with renal insufficiency and can have GI side effects.
Common Missteps
That opioids remain the drugs of choice for controlling severe pain puts some physicians outside their comfort zone. Dr. Ling, who has extensive experience with IV opioids, has observed two common tendencies among physicians inexperienced with prescribing opioids. “There is a tendency, based on the traditional teaching, to prescribe a lower-than-necessary first dose and for those doses to not be frequent enough,” he says.
Dr. Artz, who has a special interest in pain management, lectures on effectively using opioids to house staff at the University of Chicago. She has observed a deficit in physician training in pain management and has seen physicians make many errors when writing orders for opioids, including mixing IV and short-acting oral opioids or two long-acting opioids, not distinguishing between patients who are opioid-naïve and opioid-tolerant in choosing a starting dose, failing to titrate short-acting opioids rapidly despite inadequate pain control, and giving orders for repeated doses of morphine in patients with renal insufficiency.
Dr. Bookwalter says the World Health Organization’s stepladder approach to treating pain (starting with oral NSAIDs and moving up to opioids) does not align with current scientific thinking on prescribing pain medication. For severe pain, a clinician should consider immediately starting an IV opioid, reassessing the patient every 15-30 minutes to see whether the dose is effectively decreasing the pain. National Comprehensive Cancer Network (NCCN) Guidelines for Adult Cancer Pain recommend rapid dose escalation to address the level of the patient’s pain.2
Skill Sets to Acquire
In addition to postgraduate and conference courses on pain control, another good first step in educating oneself about pain is to become familiar with equianalgesic doses of opioids. It is also mandatory to know not only how to convert between different opioids but between different routes of administration, Dr. Artz emphasizes. This step is crucial when patients have been stabilized and are ready for discharge. When conversions from IV opioids to equianalgesic doses of oral opioids are performed incorrectly, patients get the idea that the oral medication doesn’t work as well and that they need the IV pain medicine, “when, in reality, we didn’t give them an equivalent dose of oral pain medicine.”
Equianalgesic tables for use in converting 24-hour standing doses of an IV opioid to an oral formulation are readily available. Dr. Bookwalter offers a cautionary note about the use of conversion charts: “These charts are based on single-dose studies. The thing to remember is that these are ballpark numbers. Every place and every practitioner will use them in a slightly different way. The key thing is close monitoring to make sure the pain is relieved and that side effects are kept at a minimum.”
Familiarity with various pain intensity scales is also necessary. The Wong numerical rating scale—either written or verbal (0 = no pain and 10 = worst pain imaginable)—is the most commonly used. The Wong-Baker FACES Pain Rating Scale is helpful when assessing patients who are not English speakers or who have other impairments.3 Dr. Artz reminds hospitalists never to guess by just looking at their patients what their levels of pain are. Many patients have developed coping strategies to mask their pain.
Finally, Dr. Ling advises hospitalists to examine their own beliefs about using opioids for pain control. “Narcotics, in general, have a social stigma attached to them,” he points out. “I think most doctors, without additional experience and training [in prescribing IV opioids], will have a natural built-in response of, ‘Do I really want to give them that much?’ ”
Dr. Ling admits even he sometimes becomes a little uncomfortable with titrating to larger doses. “But some patients—especially those with a new diagnosis of metastatic cancer—or cancer that is invading an organ system, have appropriately high requirements for pain medication,” he stresses. Dr. Ling recalls one educational video made by the colleague of a patient who required a 400-mg dose of IV morphine daily. While the patient’s surgeon, anesthesiologist, and internist did not believe that the patient required that much morphine, her hospitalist finally convinced the treatment team by achieving adequate pain control using her own pain management skill.
“It’s not the dose so much as looking at the patient and talking with the patient” that should guide dosing decisions, says Eva Chittenden, MD, assistant director of the UCSF Palliative Care Service and chair of SHM’s Palliative Care Task Force. “You will know within 10 to 15 minutes if a dose is working.”
Adds Howard R. Epstein, MD, medical director of Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and also a member of SHM’s Palliative Care Task Force, “You have to assess your intervention: Was it effective? Did it relieve the patient’s pain? How long did it last?”
Dr. Bookwalter says hospitalists have an edge with pain patients. “The advantage that hospitalists have is that they can do more frequent monitoring,” he says. “The choice of drug is key, but frequent monitoring is even more key: You have to know if the patient is getting nauseated, or is still in pain, or how much the pain decreased with a certain dose.”
Special Considerations
Multiple variables influence a clinician’s decision to prescribe IV opioids for a patient—and at what dose and frequency. Basic principles of pain management dictate administering an initial IV bolus by a provider or by using patient-controlled analgesia (PCA) at lower doses if the patient is opioid-naïve, and at higher doses if a patient has already been taking oral narcotics. The NCCN recommends starting doses of 1-5 mg of IV morphine or equivalent for opioid-naïve patients, or a dose 10%-20% of a daily IV morphine equivalent for those already on opioids.2
The clinician should reassess the patient at 15 minutes to determine whether the pain score is unchanged, increased, or decreased. “If, after 15 minutes, that patient is still in severe pain, you want to be giving another dose,” emphasizes Dr. Chittenden. “You want to get the pain under control and then figure out what the standing dose should be.” The NCCN advises increasing the dose by 50%-100% if the pain score is unchanged or has increased after the initial dose.
IV opioids can also be indicated in elderly patients, unless they suffer from renal insufficiency. Palliative care specialists usually follow the maxim “start low and go slow” for elderly patients, and a 0.5 to 1-mg initial dose would be a reasonable place to begin treating an elderly patient in pain, says Dr. Chittenden. In addition to reassessing every 15 minutes for changes in the pain score, the hospitalist should also closely monitor the patient for sedation, respiratory rate, and other untoward side effects.
Hospitalists as Advocates
Hospitalists can play a vital role in advocating for better pain control for hospitalized patients. “Unfortunately,” notes Dr. Epstein, “pain management is not very well taught in most residency programs. But it’s an essential skill—not to mention a core competency—for hospitalists. If they don’t feel comfortable with their current fund of knowledge, there are plenty of resources out there to gain the skills or develop a higher comfort level and provide more competent pain management—to palliative as well as non-palliative patients.”
In actively dying patients, adequate pain control frees them from suffering. “If people have severe pain, they can’t talk with their families, and they can’t do the other things that might be important to them, whether they’re dying or not dying,” says Dr. Chittenden. “We should be trying to address pain in all patients in the hospital, not just those who are dying. Those in the ICU, those who have just had operations, those who have chronic pain—it’s not OK for them to come to the hospital and be having terrible pain.”
Dr. Artz agrees: “I cannot imagine that it is good for healing if a patient’s sympathetic nervous system is revved up because they’re in severe pain. I believe that adequate pain control is a really important piece of helping people get better.”
Dr. Ling urges colleagues to put themselves in the patient’s shoes, asking themselves, “If I were the patient, what would I need to control my pain?” Everyone’s pain threshold is different, he asserts, and physicians should listen to their patients’ reports. “Rather than asking why would we need to prescribe a large dose of narcotics, ask, ‘Why wouldn’t you want to control the pain?’ ” TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Gordon DB, Stevenson KK, Griffie J, et al. Opioid equianalgesic calculations. J Palliat Med. 1999 summer;2(2):209-218.
- National Comprehensive Cancer Network Practice Guidelines in Oncology. Adult cancer pain. Available at: www.nccn.org/professionals/physician_gls/PDF/pain.pdf. Last accessed January 28, 2007.
- Wong DL, Hockenberry-Eaton M, Wilson D, et al. Wong’s Essentials of Pediatric Nursing. 6th ed. St. Louis: Mosby;2001:1301.
Skillful use of intravenous pain medications can be a powerful tool in the clinician’s pain management armamentarium. Yet many physicians are uncomfortable prescribing IV pain medications, especially opioids, even when their patients are experiencing severe pain—7-10 on the verbal analogue scale (VAS). This reticence, say the palliative care specialists interviewed for this article, may be due to a lack of training and knowledge, as well as misperceptions about proper use of IV opioids. The end result for patients can be inadequate pain control, which, according to researchers, continues to be a problem in U.S. hospitals.1
Even hospitalists not affiliated with a surgical service who do not treat perioperative patients are likely to encounter many different scenarios in which IV pain medications could appropriately address patients’ discomfort. David Ling, MD, a member of SHM’s Palliative Care Task Force, a hospitalist at Baystate Medical Center in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine (Boston), says patients who need IV pain medicines range from those with acute abdominal pain, pancreatitis, or small bowel obstructions to patients with end-stage cancer, renal disease, or congestive heart failure.
“It’s probably a bigger number on the medical service than most people realize,” he says.
The Short List
When it comes to effective IV pain medications very few choices exist, according to recommendations from the National Comprehensive Cancer Network and other pain advocacy organizations. An informal poll of interview sources corroborates this revelation.
“Morphine is the gold standard in pain control,” says Thomas Bookwalter, PharmD, clinical pharmacist on the General Medicine Service at the University of California at San Francisco (UCSF) Medical Center, a Health Sciences associate clinical professor at the UCSF School of Pharmacy, and a member of SHM’s Palliative Care Task Force.
Preferences for morphine or other opioids vary by practitioner and institution. For instance, says Dr. Bookwalter, the pain service at UCSF has been using hydromorphone more frequently of late.
Nicole L. Artz, MD, director of the Adult Sickle Cell Disease Care Team at the University of Chicago Hospitals and instructor of medicine at the University of Chicago Medical School, also occasionally uses IV infusions of ketorolac—a powerful NSAID designed for short-term management of moderately severe pain in adults. But, like morphine, it is contraindicated in patients with renal insufficiency and can have GI side effects.
Common Missteps
That opioids remain the drugs of choice for controlling severe pain puts some physicians outside their comfort zone. Dr. Ling, who has extensive experience with IV opioids, has observed two common tendencies among physicians inexperienced with prescribing opioids. “There is a tendency, based on the traditional teaching, to prescribe a lower-than-necessary first dose and for those doses to not be frequent enough,” he says.
Dr. Artz, who has a special interest in pain management, lectures on effectively using opioids to house staff at the University of Chicago. She has observed a deficit in physician training in pain management and has seen physicians make many errors when writing orders for opioids, including mixing IV and short-acting oral opioids or two long-acting opioids, not distinguishing between patients who are opioid-naïve and opioid-tolerant in choosing a starting dose, failing to titrate short-acting opioids rapidly despite inadequate pain control, and giving orders for repeated doses of morphine in patients with renal insufficiency.
Dr. Bookwalter says the World Health Organization’s stepladder approach to treating pain (starting with oral NSAIDs and moving up to opioids) does not align with current scientific thinking on prescribing pain medication. For severe pain, a clinician should consider immediately starting an IV opioid, reassessing the patient every 15-30 minutes to see whether the dose is effectively decreasing the pain. National Comprehensive Cancer Network (NCCN) Guidelines for Adult Cancer Pain recommend rapid dose escalation to address the level of the patient’s pain.2
Skill Sets to Acquire
In addition to postgraduate and conference courses on pain control, another good first step in educating oneself about pain is to become familiar with equianalgesic doses of opioids. It is also mandatory to know not only how to convert between different opioids but between different routes of administration, Dr. Artz emphasizes. This step is crucial when patients have been stabilized and are ready for discharge. When conversions from IV opioids to equianalgesic doses of oral opioids are performed incorrectly, patients get the idea that the oral medication doesn’t work as well and that they need the IV pain medicine, “when, in reality, we didn’t give them an equivalent dose of oral pain medicine.”
Equianalgesic tables for use in converting 24-hour standing doses of an IV opioid to an oral formulation are readily available. Dr. Bookwalter offers a cautionary note about the use of conversion charts: “These charts are based on single-dose studies. The thing to remember is that these are ballpark numbers. Every place and every practitioner will use them in a slightly different way. The key thing is close monitoring to make sure the pain is relieved and that side effects are kept at a minimum.”
Familiarity with various pain intensity scales is also necessary. The Wong numerical rating scale—either written or verbal (0 = no pain and 10 = worst pain imaginable)—is the most commonly used. The Wong-Baker FACES Pain Rating Scale is helpful when assessing patients who are not English speakers or who have other impairments.3 Dr. Artz reminds hospitalists never to guess by just looking at their patients what their levels of pain are. Many patients have developed coping strategies to mask their pain.
Finally, Dr. Ling advises hospitalists to examine their own beliefs about using opioids for pain control. “Narcotics, in general, have a social stigma attached to them,” he points out. “I think most doctors, without additional experience and training [in prescribing IV opioids], will have a natural built-in response of, ‘Do I really want to give them that much?’ ”
Dr. Ling admits even he sometimes becomes a little uncomfortable with titrating to larger doses. “But some patients—especially those with a new diagnosis of metastatic cancer—or cancer that is invading an organ system, have appropriately high requirements for pain medication,” he stresses. Dr. Ling recalls one educational video made by the colleague of a patient who required a 400-mg dose of IV morphine daily. While the patient’s surgeon, anesthesiologist, and internist did not believe that the patient required that much morphine, her hospitalist finally convinced the treatment team by achieving adequate pain control using her own pain management skill.
“It’s not the dose so much as looking at the patient and talking with the patient” that should guide dosing decisions, says Eva Chittenden, MD, assistant director of the UCSF Palliative Care Service and chair of SHM’s Palliative Care Task Force. “You will know within 10 to 15 minutes if a dose is working.”
Adds Howard R. Epstein, MD, medical director of Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and also a member of SHM’s Palliative Care Task Force, “You have to assess your intervention: Was it effective? Did it relieve the patient’s pain? How long did it last?”
Dr. Bookwalter says hospitalists have an edge with pain patients. “The advantage that hospitalists have is that they can do more frequent monitoring,” he says. “The choice of drug is key, but frequent monitoring is even more key: You have to know if the patient is getting nauseated, or is still in pain, or how much the pain decreased with a certain dose.”
Special Considerations
Multiple variables influence a clinician’s decision to prescribe IV opioids for a patient—and at what dose and frequency. Basic principles of pain management dictate administering an initial IV bolus by a provider or by using patient-controlled analgesia (PCA) at lower doses if the patient is opioid-naïve, and at higher doses if a patient has already been taking oral narcotics. The NCCN recommends starting doses of 1-5 mg of IV morphine or equivalent for opioid-naïve patients, or a dose 10%-20% of a daily IV morphine equivalent for those already on opioids.2
The clinician should reassess the patient at 15 minutes to determine whether the pain score is unchanged, increased, or decreased. “If, after 15 minutes, that patient is still in severe pain, you want to be giving another dose,” emphasizes Dr. Chittenden. “You want to get the pain under control and then figure out what the standing dose should be.” The NCCN advises increasing the dose by 50%-100% if the pain score is unchanged or has increased after the initial dose.
IV opioids can also be indicated in elderly patients, unless they suffer from renal insufficiency. Palliative care specialists usually follow the maxim “start low and go slow” for elderly patients, and a 0.5 to 1-mg initial dose would be a reasonable place to begin treating an elderly patient in pain, says Dr. Chittenden. In addition to reassessing every 15 minutes for changes in the pain score, the hospitalist should also closely monitor the patient for sedation, respiratory rate, and other untoward side effects.
Hospitalists as Advocates
Hospitalists can play a vital role in advocating for better pain control for hospitalized patients. “Unfortunately,” notes Dr. Epstein, “pain management is not very well taught in most residency programs. But it’s an essential skill—not to mention a core competency—for hospitalists. If they don’t feel comfortable with their current fund of knowledge, there are plenty of resources out there to gain the skills or develop a higher comfort level and provide more competent pain management—to palliative as well as non-palliative patients.”
In actively dying patients, adequate pain control frees them from suffering. “If people have severe pain, they can’t talk with their families, and they can’t do the other things that might be important to them, whether they’re dying or not dying,” says Dr. Chittenden. “We should be trying to address pain in all patients in the hospital, not just those who are dying. Those in the ICU, those who have just had operations, those who have chronic pain—it’s not OK for them to come to the hospital and be having terrible pain.”
Dr. Artz agrees: “I cannot imagine that it is good for healing if a patient’s sympathetic nervous system is revved up because they’re in severe pain. I believe that adequate pain control is a really important piece of helping people get better.”
Dr. Ling urges colleagues to put themselves in the patient’s shoes, asking themselves, “If I were the patient, what would I need to control my pain?” Everyone’s pain threshold is different, he asserts, and physicians should listen to their patients’ reports. “Rather than asking why would we need to prescribe a large dose of narcotics, ask, ‘Why wouldn’t you want to control the pain?’ ” TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Gordon DB, Stevenson KK, Griffie J, et al. Opioid equianalgesic calculations. J Palliat Med. 1999 summer;2(2):209-218.
- National Comprehensive Cancer Network Practice Guidelines in Oncology. Adult cancer pain. Available at: www.nccn.org/professionals/physician_gls/PDF/pain.pdf. Last accessed January 28, 2007.
- Wong DL, Hockenberry-Eaton M, Wilson D, et al. Wong’s Essentials of Pediatric Nursing. 6th ed. St. Louis: Mosby;2001:1301.
Skillful use of intravenous pain medications can be a powerful tool in the clinician’s pain management armamentarium. Yet many physicians are uncomfortable prescribing IV pain medications, especially opioids, even when their patients are experiencing severe pain—7-10 on the verbal analogue scale (VAS). This reticence, say the palliative care specialists interviewed for this article, may be due to a lack of training and knowledge, as well as misperceptions about proper use of IV opioids. The end result for patients can be inadequate pain control, which, according to researchers, continues to be a problem in U.S. hospitals.1
Even hospitalists not affiliated with a surgical service who do not treat perioperative patients are likely to encounter many different scenarios in which IV pain medications could appropriately address patients’ discomfort. David Ling, MD, a member of SHM’s Palliative Care Task Force, a hospitalist at Baystate Medical Center in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine (Boston), says patients who need IV pain medicines range from those with acute abdominal pain, pancreatitis, or small bowel obstructions to patients with end-stage cancer, renal disease, or congestive heart failure.
“It’s probably a bigger number on the medical service than most people realize,” he says.
The Short List
When it comes to effective IV pain medications very few choices exist, according to recommendations from the National Comprehensive Cancer Network and other pain advocacy organizations. An informal poll of interview sources corroborates this revelation.
“Morphine is the gold standard in pain control,” says Thomas Bookwalter, PharmD, clinical pharmacist on the General Medicine Service at the University of California at San Francisco (UCSF) Medical Center, a Health Sciences associate clinical professor at the UCSF School of Pharmacy, and a member of SHM’s Palliative Care Task Force.
Preferences for morphine or other opioids vary by practitioner and institution. For instance, says Dr. Bookwalter, the pain service at UCSF has been using hydromorphone more frequently of late.
Nicole L. Artz, MD, director of the Adult Sickle Cell Disease Care Team at the University of Chicago Hospitals and instructor of medicine at the University of Chicago Medical School, also occasionally uses IV infusions of ketorolac—a powerful NSAID designed for short-term management of moderately severe pain in adults. But, like morphine, it is contraindicated in patients with renal insufficiency and can have GI side effects.
Common Missteps
That opioids remain the drugs of choice for controlling severe pain puts some physicians outside their comfort zone. Dr. Ling, who has extensive experience with IV opioids, has observed two common tendencies among physicians inexperienced with prescribing opioids. “There is a tendency, based on the traditional teaching, to prescribe a lower-than-necessary first dose and for those doses to not be frequent enough,” he says.
Dr. Artz, who has a special interest in pain management, lectures on effectively using opioids to house staff at the University of Chicago. She has observed a deficit in physician training in pain management and has seen physicians make many errors when writing orders for opioids, including mixing IV and short-acting oral opioids or two long-acting opioids, not distinguishing between patients who are opioid-naïve and opioid-tolerant in choosing a starting dose, failing to titrate short-acting opioids rapidly despite inadequate pain control, and giving orders for repeated doses of morphine in patients with renal insufficiency.
Dr. Bookwalter says the World Health Organization’s stepladder approach to treating pain (starting with oral NSAIDs and moving up to opioids) does not align with current scientific thinking on prescribing pain medication. For severe pain, a clinician should consider immediately starting an IV opioid, reassessing the patient every 15-30 minutes to see whether the dose is effectively decreasing the pain. National Comprehensive Cancer Network (NCCN) Guidelines for Adult Cancer Pain recommend rapid dose escalation to address the level of the patient’s pain.2
Skill Sets to Acquire
In addition to postgraduate and conference courses on pain control, another good first step in educating oneself about pain is to become familiar with equianalgesic doses of opioids. It is also mandatory to know not only how to convert between different opioids but between different routes of administration, Dr. Artz emphasizes. This step is crucial when patients have been stabilized and are ready for discharge. When conversions from IV opioids to equianalgesic doses of oral opioids are performed incorrectly, patients get the idea that the oral medication doesn’t work as well and that they need the IV pain medicine, “when, in reality, we didn’t give them an equivalent dose of oral pain medicine.”
Equianalgesic tables for use in converting 24-hour standing doses of an IV opioid to an oral formulation are readily available. Dr. Bookwalter offers a cautionary note about the use of conversion charts: “These charts are based on single-dose studies. The thing to remember is that these are ballpark numbers. Every place and every practitioner will use them in a slightly different way. The key thing is close monitoring to make sure the pain is relieved and that side effects are kept at a minimum.”
Familiarity with various pain intensity scales is also necessary. The Wong numerical rating scale—either written or verbal (0 = no pain and 10 = worst pain imaginable)—is the most commonly used. The Wong-Baker FACES Pain Rating Scale is helpful when assessing patients who are not English speakers or who have other impairments.3 Dr. Artz reminds hospitalists never to guess by just looking at their patients what their levels of pain are. Many patients have developed coping strategies to mask their pain.
Finally, Dr. Ling advises hospitalists to examine their own beliefs about using opioids for pain control. “Narcotics, in general, have a social stigma attached to them,” he points out. “I think most doctors, without additional experience and training [in prescribing IV opioids], will have a natural built-in response of, ‘Do I really want to give them that much?’ ”
Dr. Ling admits even he sometimes becomes a little uncomfortable with titrating to larger doses. “But some patients—especially those with a new diagnosis of metastatic cancer—or cancer that is invading an organ system, have appropriately high requirements for pain medication,” he stresses. Dr. Ling recalls one educational video made by the colleague of a patient who required a 400-mg dose of IV morphine daily. While the patient’s surgeon, anesthesiologist, and internist did not believe that the patient required that much morphine, her hospitalist finally convinced the treatment team by achieving adequate pain control using her own pain management skill.
“It’s not the dose so much as looking at the patient and talking with the patient” that should guide dosing decisions, says Eva Chittenden, MD, assistant director of the UCSF Palliative Care Service and chair of SHM’s Palliative Care Task Force. “You will know within 10 to 15 minutes if a dose is working.”
Adds Howard R. Epstein, MD, medical director of Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and also a member of SHM’s Palliative Care Task Force, “You have to assess your intervention: Was it effective? Did it relieve the patient’s pain? How long did it last?”
Dr. Bookwalter says hospitalists have an edge with pain patients. “The advantage that hospitalists have is that they can do more frequent monitoring,” he says. “The choice of drug is key, but frequent monitoring is even more key: You have to know if the patient is getting nauseated, or is still in pain, or how much the pain decreased with a certain dose.”
Special Considerations
Multiple variables influence a clinician’s decision to prescribe IV opioids for a patient—and at what dose and frequency. Basic principles of pain management dictate administering an initial IV bolus by a provider or by using patient-controlled analgesia (PCA) at lower doses if the patient is opioid-naïve, and at higher doses if a patient has already been taking oral narcotics. The NCCN recommends starting doses of 1-5 mg of IV morphine or equivalent for opioid-naïve patients, or a dose 10%-20% of a daily IV morphine equivalent for those already on opioids.2
The clinician should reassess the patient at 15 minutes to determine whether the pain score is unchanged, increased, or decreased. “If, after 15 minutes, that patient is still in severe pain, you want to be giving another dose,” emphasizes Dr. Chittenden. “You want to get the pain under control and then figure out what the standing dose should be.” The NCCN advises increasing the dose by 50%-100% if the pain score is unchanged or has increased after the initial dose.
IV opioids can also be indicated in elderly patients, unless they suffer from renal insufficiency. Palliative care specialists usually follow the maxim “start low and go slow” for elderly patients, and a 0.5 to 1-mg initial dose would be a reasonable place to begin treating an elderly patient in pain, says Dr. Chittenden. In addition to reassessing every 15 minutes for changes in the pain score, the hospitalist should also closely monitor the patient for sedation, respiratory rate, and other untoward side effects.
Hospitalists as Advocates
Hospitalists can play a vital role in advocating for better pain control for hospitalized patients. “Unfortunately,” notes Dr. Epstein, “pain management is not very well taught in most residency programs. But it’s an essential skill—not to mention a core competency—for hospitalists. If they don’t feel comfortable with their current fund of knowledge, there are plenty of resources out there to gain the skills or develop a higher comfort level and provide more competent pain management—to palliative as well as non-palliative patients.”
In actively dying patients, adequate pain control frees them from suffering. “If people have severe pain, they can’t talk with their families, and they can’t do the other things that might be important to them, whether they’re dying or not dying,” says Dr. Chittenden. “We should be trying to address pain in all patients in the hospital, not just those who are dying. Those in the ICU, those who have just had operations, those who have chronic pain—it’s not OK for them to come to the hospital and be having terrible pain.”
Dr. Artz agrees: “I cannot imagine that it is good for healing if a patient’s sympathetic nervous system is revved up because they’re in severe pain. I believe that adequate pain control is a really important piece of helping people get better.”
Dr. Ling urges colleagues to put themselves in the patient’s shoes, asking themselves, “If I were the patient, what would I need to control my pain?” Everyone’s pain threshold is different, he asserts, and physicians should listen to their patients’ reports. “Rather than asking why would we need to prescribe a large dose of narcotics, ask, ‘Why wouldn’t you want to control the pain?’ ” TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Gordon DB, Stevenson KK, Griffie J, et al. Opioid equianalgesic calculations. J Palliat Med. 1999 summer;2(2):209-218.
- National Comprehensive Cancer Network Practice Guidelines in Oncology. Adult cancer pain. Available at: www.nccn.org/professionals/physician_gls/PDF/pain.pdf. Last accessed January 28, 2007.
- Wong DL, Hockenberry-Eaton M, Wilson D, et al. Wong’s Essentials of Pediatric Nursing. 6th ed. St. Louis: Mosby;2001:1301.