Predicting 1-Year Postoperative Visual Analog Scale Pain Scores and American Shoulder and Elbow Surgeons Function Scores in Total and Reverse Total Shoulder Arthroplasty
Shared decision-making tools, such as predictive models, can help empower the patient to make decisions for or against surgery equipped with more information about the expected outcome.
There is a role for preoperative collection of PROMs in the clinical decision-making process.
Mental health state, as reported by the VR-12 MCS, is a significant predictor of postoperative pain and function as reported by the VAS pain and ASES function scores.
A significant portion of the predictive ability of this model comes from the fact that at 1-year postoperatively, patients receiving a rTSA will on average have a 3.8 point lower on ASES function score than those receiving a TSA (P < .001, ω2=.083).
Future studies to discern the role of different modalities to improve a patient’s emotional health preoperatively will be beneficial as the healthcare industry trends toward value based medicine collecting PROMs as part of reimbursement schemes.
Over the past few decades, decisions regarding patients’ care have gradually transitioned from a paternalistic model to a more cooperative exchange between patient and physician. Shared decision-making provides patients a measure of autonomy in making choices for their health and their future. Patient participation may mitigate uncertainty and discomfort during selection of a course of treatment, which may lead to increased satisfaction levels after surgery.1 Moreover, shared decision-making may help patients better manage postoperative expectations through evidenced-based discussions of preoperative health levels and their corresponding outcomes. Patient-reported outcome measures (PROMs) use clinically sensitive and specific metrics to evaluate a patient’s self-reported pain, functional ability, and mental state.2 These metrics are useful in setting patient expectations for potential outcomes of treatment options. Use of evidence-based clinical decision-making tools, such as PROM-based predictive models, can facilitate a collaborative decision-making environment for patient and physician. Given the present cost-containment era, and the need for preoperative metrics that can assist in predictive analysis of postoperative improvement, models are clearly valuable.
In attempts to help patients set well-informed and reasonable expectations, physicians have turned to PROMs to facilitate preoperative evidence-based discussions. Although PROMs have been in use for almost 30 years, only recently have they been used to create tools that can aid quantitatively in the surgical decision-making process.2-6 Combining physical examination findings, imaging studies, comorbidities, and quantitative tools, such as this model, may enhance patients’ understanding of their preoperative condition and expected prognosis and thereby guide their surgical decisions.
We conducted a study to determine whether certain preoperative PROMs can predict 1-year postoperative visual analog scale (VAS) pain scores and American Shoulder and Elbow Surgeons (ASES) Function scores in total shoulder arthroplasty (TSA) and reverse TSA (rTSA). We hypothesized that preoperative mental health status as captured by Veterans RAND 12-Item Health Survey (VR-12) mental health component summary (MCS) score and preoperative VAS pain score would predict both VAS pain score and ASES Function score 1 year after surgery. Specifically, we hypothesized that a higher preoperative VR-12 MCS score would predict less pain and better function 1 year after surgery and that a higher preoperative VAS pain score would predict more pain and worse function 1 year after surgery.
Methods
This study was approved by the Institutional Review Board of Partners Healthcare. The study used the Surgical Outcome System (Arthrex), a comprehensive prospective database that stores preoperative and 1-year postoperative patient demographics and TSA-PROM data. Surveys are emailed to all enrolled patients before surgery and 1 year after surgery. As indicated by the Institutional Review Boards of all participating institutions, patients in the Surgical Outcome System have to sign a consent form to permit use of their responses in research.
The database includes patient data from 42 orthopedic surgeons across the United States. All primary TSAs and primary rTSAs in the database were included in this study, regardless of arthroplasty indication. Revisions were excluded. Also excluded were cases in which the 1-year postoperative questionnaire was not completed. Of the 1681 patients eligible for 1-year follow-up, 1225 (73%) completed the 1-year postoperative questionnaire. PROMs used in the study were VAS pain score, ASES Function score, VR-12 MCS score, and Single Assessment Numerical Evaluation (SANE). Unfortunately, not all surgeons use every measure in the 1-year postoperative questionnaire set. Thus, in our complete models, total number of observations was 1004 for modeling 1-year postoperative VAS pain scores and 986 for modeling 1-year postoperative ASES Function scores.
Metrics
On VAS, pain is rated from 0 (no pain) to 10 (pain as bad as it can be). Tashjian and colleagues7 estimated that the minimal clinically important difference (MCID) for postoperative VAS pain scores was 1.4 in a cohort of 326 patients who had TSA, rTSA, or shoulder hemiarthroplasty. ASES Function score is scaled from 0 to 30, with 30 representing best function.8 Wong and colleagues9 identified an MCID of 6.5 for ASES Function scores in a cohort of 107 patients who had TSA or rTSA. SANE ratings range from 0% to 100%, with 100% indicating the patient’s shoulder was totally “normal.”10 VR-12 MCS scores appear on a logarithmic scale, with higher numbers representing better mental health. The population mean estimate for VR-12 MCS scores is 50.1 (SD, 11.49; overall possible range, –2.47 to 76.1).11 Our patient population’s scores ranged from 12.5 to 73.8.
Statistical Analysis
Simple bivariate and multivariate linear regressions were performed to evaluate the predictive value of each of the outlined PROMs. Our complete model controls for patient sex, age, and type of arthroplasty. Categorical variables were dummy-coded. Both 1-year postoperative VAS pain score and 1-year postoperative ASES Function score were investigated as dependent variables. Regression coefficients and P and ω2 values are reported. Omega square represents how much of the variance in an outcome variable a model explains, like R2, and ω2 values can also be calculated for individual factors to see how much variance a given factor accounts for. For a simple relative risk calculation, we divided our cohort into 3 equal-sized groups based on preoperative VR-12 MCS scores and compared the risk that patients with scores in the top third (better mental health) would end up below certain ASES Total scores with the risk of patients with scores in the bottom third (worse mental health). All statistical analyses were performed with Stata (StataCorp).
Results
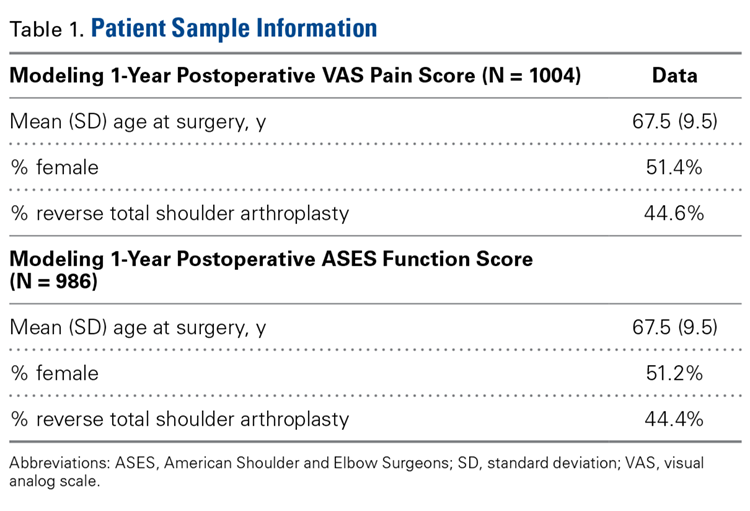
Table 1 lists summary statistics for the population used in these models.
Table 1.Our complete model for predicting VAS pain score 1 year after surgery accounted for 8% of the variability in this pain score (ω2 = .076), whereas our complete model for predicting ASES Function score 1 year after surgery accounted for 22% of the variability (ω2 = .219). These models include preoperative scores for VAS pain, ASES Function, VR-12 MCS, SANE, age at time of surgery, sex, and type of arthroplasty as possible explanatory variables.
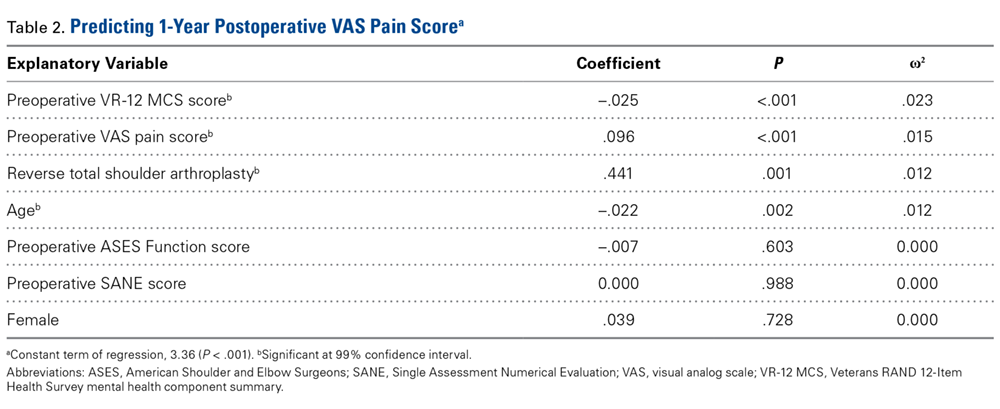
Table 2.Predicting VAS Pain Score (Table 2)
Preoperative VAS pain score and VR-12 MCS score both predicted 1-year postoperative VAS pain score (P < .001). Preoperative ASES Function score did not predict pain 1 year after surgery. By contrast, higher preoperative VAS pain scores were associated with higher VAS pain scores 1 year after surgery. Higher preoperative VR-12 MCS scores were significantly associated with lower VAS pain scores 1 year after surgery, indicating that better preoperative mental health is significantly associated with better self-reported outcomes in terms of pain 1 year after surgery. These associations remained statistically significant when controlling for age at time of surgery, sex, and type of arthroplasty.
Preoperative VR-12 MCS score was more predictive of 1-year postoperative VAS pain score than preoperative VAS pain score was. In other words, preoperative VR-12 MCS score accounted for more variability in outcome for 1-year postoperative VAS pain score (2.4%; ω2 = .023) than preoperative VAS pain score did (1.6%; ω2 = .015).
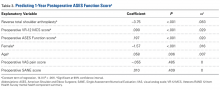
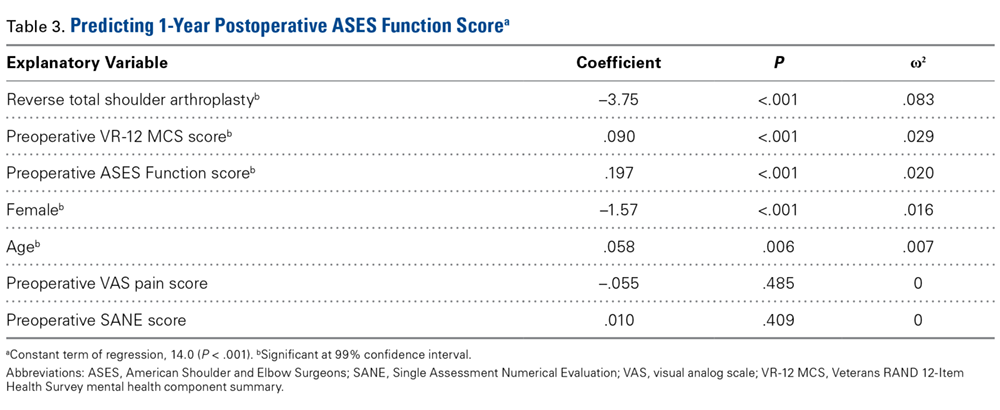
Table 3.Predicting ASES Function Score (Table 3)
By contrast, preoperative VAS pain score did not predict 1-year postoperative ASES Function score. Preoperative ASES Function and VR-12 MCS scores both predicted 1-year postoperative ASES Function score (P < .001). Higher preoperative ASES Function scores were associated with higher 1-year postoperative ASES Function scores. In other words, reporting better shoulder function before surgery was associated with reporting better shoulder function after surgery.
An example gives a sense of the effect size associated with the coefficient for preoperative ASES Function score. Our model predicts that, compared with a patient who reports 5 points lower on preoperative ASES Function (which ranges from 0-30), a patient who reports 5 points higher will report on average about 1 point higher on 1-year postoperative ASES Function. As in the model for postoperative pain, these associations with preoperative function and mental health scores held when controlling for age, sex, and type of arthroplasty.
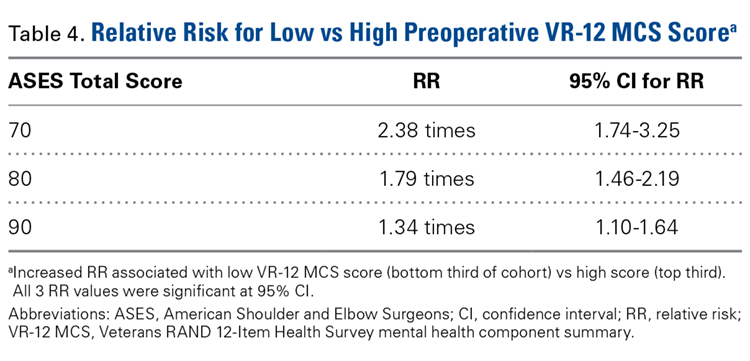
As in the postoperative pain model, preoperative VR-12 MCS score was more predictive of 1-year postoperative ASES Function score than preoperative ASES Function score was. Preoperative VR-12 MCS score accounted for more of the variation that our model predicts (ω2 = .029) than preoperative ASES Function score did (ω2 = .020). We compared the risk that patients with high preoperative VR-12 MCS scores (top third of cohort) would end up with ASES Total scores below 70, below 80, or below 90 with the risk of patients with low preoperative VR-12 MCS scores (bottom third). Results appear in Table 4.
Table 4.
A significant part of the predictive ability of our model for postoperative ASES Function scores stems from the fact that a patient who undergoes rTSA (vs TSA) is predicted to have an ASES Function score 3.8 points lower 1 year after surgery (P < .001, ω2 = .083). With type of arthroplasty controlled for, female sex is associated with an ASES Function score 1.6 points lower 1 year after surgery (P < .001, ω2 = .016).
Preoperative SANE score did not predict 1-year postoperative VAS pain score or ASES Function score. In addition, when our complete model was run with 1-year postoperative SANE score as the dependent variable, preoperative SANE score did not predict 1-year postoperative SANE score. Our data provide no supporting evidence for the use of SANE scores for predictive modeling for shoulder arthroplasty.
Discussion
We prospectively gathered data to determine which factors would predict patient subjective outcomes of primary TSA and primary rTSA. We hypothesized that preoperative VR-12 MCS scores and preoperative VAS pain scores would predict postoperative pain and function as measured with those PROMs. Second, we hypothesized that better preoperative mental health (as measured with VR-12 MCS scores) would predict lower postoperative pain (VAS pain scores) and better postoperative function (ASES Function scores). Third, we hypothesized that higher preoperative pain (VAS pain scores) would correlate with higher postoperative pain (VAS pain scores) and worse postoperative function (ASES Function scores).
Our main goal is to provide patients and surgeons with a predictive model that generates insights into what patients can expect after surgery. This model is not intended to be a screening tool for operative indications, but a clinical tool for helping set expectations.
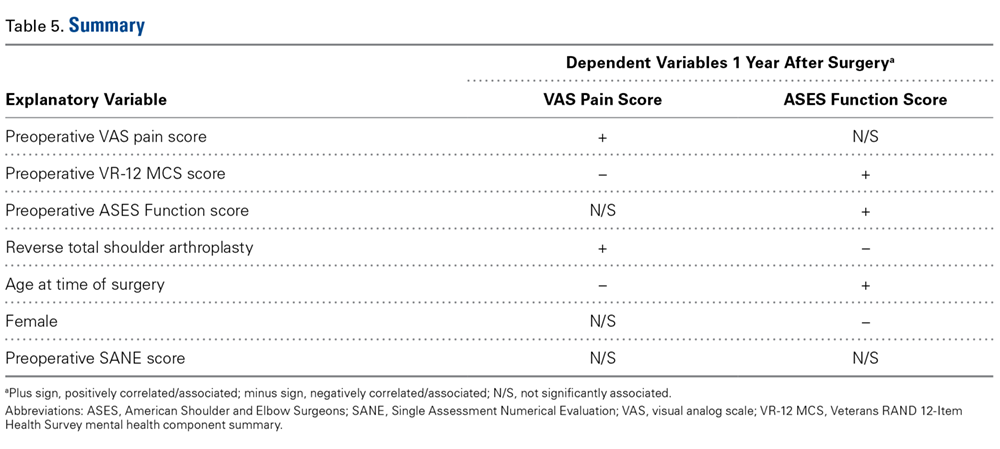
Our results showed that patients with more pain before surgery were more likely to have more pain 1 year after surgery—confirming the hypothesized relationship between pain before and after surgery. Contrary to the hypothesis, however, degree of pain before surgery was not associated with function 1 year after surgery. Our mental health hypothesis was confirmed: Patients with better preoperative mental health scores had on average less pain and better function 1 year after surgery. Not surprisingly, our model demonstrated that patients with better self-reported function before surgery had better self-reported function after surgery. Patient-reported function before surgery did not significantly affect how much pain the patient had 1 year after surgery. Although we did not hypothesize about the role of function in predicting 1-year outcomes, function is a significant factor to be considered when setting patient expectations regarding shoulder arthroplasty outcomes (Table 5).
Table 5.
Although the effect sizes of each analyzed factor are small, together our models for 1-year postoperative pain and function provide significant insight into patients’ likely outcomes 1 year after TSA and rTSA.
Table 6.
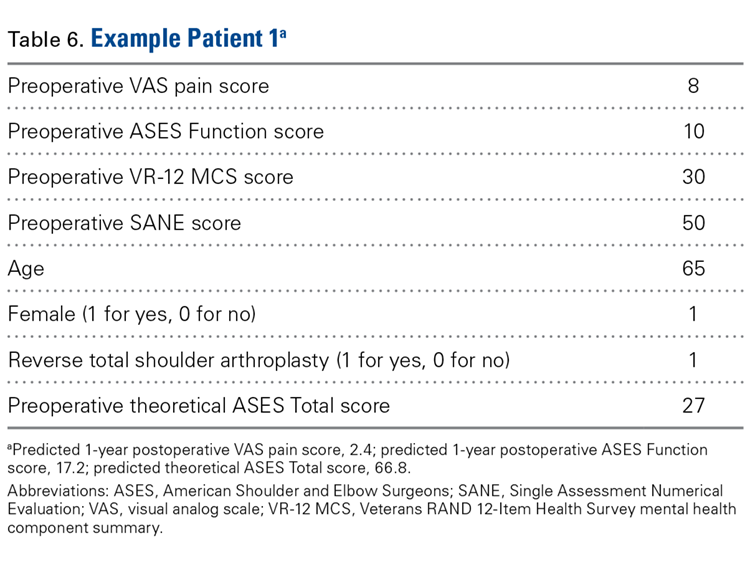
Table 7.Table 6 and Table 7 listpreoperative PROMs and baseline characteristics for 2 sample patients and the corresponding 1-year postoperative results they should expect according to our model. Patient 1 (Table 6) achieves a theoretical ASES Total score of 67, and patient 2 (Table 7) achieves a theoretical ASES Total score of 90. During discussion of surgical options, these patients should be counseled differently. If patient 1 expects a “normal” shoulder after surgery, he or she likely will be disappointed with the outcome. Tools such as those provided here can contribute to evidence-based discussions and well-informed decision making.
Many studies have found that mental health correlated with pain and function during recovery from orthopedic trauma.12-18 For example, Wylie and colleagues19 found that preoperative mental health, as measured with the 36-Item Short Form Health Survey (SF-36) MCS score, predicted patient-reported pain and function in the setting of rotator cuff injury, regardless of treatment type (operative, nonoperative). Others have found that mental health may play a role in how patients report their pain and function on various PROMs.20,21 Modalities for improving patients’ emotional health baseline may even become a preoperative requirement as the healthcare industry moves toward value-based medicine and collection of patient-related outcomes as part of reimbursement schemes.
By contrast, some studies have found that preoperative mental health did not predict postoperative outcomes. For example, Kennedy and colleagues22 found that preoperative mental health (as measured with SF-36 MCS scores) did not predict functional outcome in patients with ankle arthritis treated with ankle arthroplasty or arthrodesis. Likewise, Styron and colleagues23 found no correlation between preoperative mental health (SF-12 MCS scores) and postoperative mental health and function in TSA. Their findings contradict those of the present study and many other studies.12-18 The contradiction in findings demonstrates the need for well-designed, sufficiently powered studies of the link between preoperative mental health and postoperative outcome. Our study, with its large sample and heterogeneous population, is a start.
Two other groups (Simmen and colleagues,18 Matsen and colleagues24) have attempted to develop a model predicting outcomes of shoulder arthroplasty. Simmen and colleagues18 estimated the probability of “treatment success” 1 year after TSA. Their model had 4 factors predictive of patient outcomes. Previous shoulder surgery and age over 75 years were significantly associated with lower probability of success, whereas higher preoperative SF-36 MCS scores and higher preoperative DASH (Disabilities of the Arm, Shoulder, and Hand) Function scores were associated with higher probability of success. The authors deemed TSA successful if the patient achieved a Constant score of ≥80 out of 100. Their model predicts probability of TSA “success,” whereas our models predict particular outcome scores. Both their results and ours support the hypothesis that preoperative mental health and function scores can predict how well a patient fares after surgery. Simmen and colleagues18 based their model on a cohort of only 140 patients and reported a 33.6% success rate (47/140 surgeries).
Matsen and colleagues24 used a 1-practice cohort of 337 patients who underwent different types of arthroplasties, including TSA, rTSA, hemiarthroplasty, and ream-and-run arthroplasty. Although their focus was not preoperative PROMs predicting postoperative PROMs, they used the Simple Shoulder Test (SST) baseline score as a predictive variable. They found that 6 baseline characteristics—American Society of Anesthesiologists class I, shoulder problem unrelated to work, no prior shoulder surgery, glenoid type other than A1, humeral head not superiorly displaced on anteroposterior radiograph, and lower baseline SST score—were statistically associated with better outcomes, and they developed a model driven by these characteristics. They urged other investigators to perform the same kind of analysis with larger patient populations from multiple practices. One of the strengths of our study is its large patient population. We collected data on 1004 patients for modeling 1-year postoperative VAS pain scores and 986 patients for modeling 1-year postoperative ASES Function scores.
Our study had several limitations. First, its data came from a 42-surgeon database, and there may be variations in how these surgeons enroll patients in the registry. If some surgeons did not enroll all their surgical patients, our sample could have been subject to selection bias. Second, in developing our model, we used only patient characteristics that were available in the database. On the other hand, the heterogeneity of the surgeon sample lended external validity to the model. A third limitation was that the model always predicts better pain and function outcomes after TSA than after rTSA. In other words, it does not consider whether TSA is appropriate for a particular patient. Instead, it predicts 1-year shoulder arthroplasty outcomes.
Our goal here is not to provide outcomes information or a surgical screening tool, but to report on our use of a simple data-driven tool for setting expectations. When appropriate data become available, tools like this should be expanded to predict longer-term shoulder arthroplasty outcomes. We need more studies that combine preoperative PROMs, more baseline clinical and patient characteristics (following the Matsen and colleagues24 model), and large sample sizes.
Conclusion
The educational models presented here can help patients and surgeons learn what to expect after surgery. These models reveal the value in collecting preoperative subjective PROMs and show how a quantitative tool can help facilitate shared decision-making and set patient expectations. Separately, the effect size of each factor is small, but together a patient’s preoperative VAS pain score, ASES Function score, VR-12 MCS score, age, sex, and type of arthroplasty can provide information predictive of the patient’s self-reported pain and function 1 year after surgery.
References
1. Stacey D, Légaré F, Col NF, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2014;(1):CD001431.
2. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. Can preoperative patient-reported outcome measures be used to predict meaningful improvement in function after TKA? Clin Orthop Relat Res. 2017;475(1):149-157.
3. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. John Charnley award: preoperative patient-reported outcome measures predict clinically meaningful improvement in function after THA. Clin Orthop Relat Res. 2016;474(2):321-329.
4. Wong SE, Zhang AL, Berliner JL, Ma CB, Feeley BT. Preoperative patient-reported scores can predict postoperative outcomes after shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(6):913-919.
5. Werner BC, Chang B, Nguyen JT, Dines DM, Gulotta LV. What change in American Shoulder and Elbow Surgeons score represents a clinically important change after shoulder arthroplasty? Clin Orthop Relat Res. 2016;474(12):2672-2681.
7. Tashjian RZ, Hung M, Keener JD, et al. Determining the minimal clinically important difference for the American Shoulder and Elbow Surgeons score, Simple Shoulder Test, and visual analog scale (VAS) measuring pain after shoulder arthroplasty. J Shoulder Elbow Surg. 2017;26(1):144-148.
8. Michener LA, McClure PW, Sennett BJ. American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, patient self-report section: reliability, validity, and responsiveness. J Shoulder Elbow Surg. 2002;11(6):587-594.
9. Wong SE, Zhang AL, Berliner JL, Ma CB, Feeley BT. Preoperative patient-reported scores can predict postoperative outcomes after shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(6):913-919.
10. Williams GN, Gangel TJ, Arciero RA, Uhorchak JM, Taylor DC. Comparison of the Single Assessment Numeric Evaluation method and two shoulder rating scales. Outcomes measures after shoulder surgery. Am J Sports Med. 1999;27(2):214-221.
11. Selim AJ, Rogers W, Fleishman JA, et al. Updated U.S. population standard for the Veterans RAND 12-Item Health Survey (VR-12). Qual Life Res. 2009;18(1):43-52.
12. Ayers DC, Franklin PD, Ploutz-Snyder R, Boisvert CB. Total knee replacement outcome and coexisting physical and emotional illness. Clin Orthop Relat Res. 2005;(440):157-161.
13. Ayers DC, Franklin PD, Trief PM, Ploutz-Snyder R, Freund D. Psychological attributes of preoperative total joint replacement patients: implications for optimal physical outcome. J Arthroplasty. 2004;19(7 suppl 2):125-130.
14. Barlow JD, Bishop JY, Dunn WR, Kuhn JE; MOON Shoulder Group. What factors are predictors of emotional health in patients with full-thickness rotator cuff tears? J Shoulder Elbow Surg. 2016;25(11):1769-1773.
15. Gandhi R, Davey JR, Mahomed NN. Predicting patient dissatisfaction following joint replacement surgery. J Rheumatol. 2008;35(12):2415-2418.
16. Parr J, Borsa P, Fillingim R, et al. Psychological influences predict recovery following exercise induced shoulder pain. Int J Sports Med. 2014;35(3):232-237.
18. Simmen BR, Bachmann LM, Drerup S, Schwyzer HK, Burkhart A, Goldhahn J. Development of a predictive model for estimating the probability of treatment success one year after total shoulder replacement—cohort study. Osteoarthritis Cartilage. 2008;16(5):631-634.
19. Wylie JD, Suter T, Potter MQ, Granger EK, Tashjian RZ. Mental health has a stronger association with patient-reported shoulder pain and function than tear size in patients with full-thickness rotator cuff tears. J Bone Joint Surg Am. 2016;98(4):251-256.
20. Potter MQ, Wylie JD, Greis PE, Burks RT, Tashjian RZ. Psychological distress negatively affects self-assessment of shoulder function in patients with rotator cuff tears. Clin Orthop Relat Res. 2014;472(12):3926-3932.
21. Roh YH, Noh JH, Oh JH, Baek GH, Gong HS. To what degree do shoulder outcome instruments reflect patients’ psychologic distress? Clin Orthop Relat Res. 2012;470(12):3470-3477.
22. Kennedy S, Barske H, Wing K, et al. SF-36 mental component summary (MCS) score does not predict functional outcome after surgery for end-stage ankle arthritis. J Bone Joint Surg Am. 2015;97(20):1702-1707.
23. Styron JF, Higuera CA, Strnad G, Iannotti JP. Greater patient confidence yields greater functional outcomes after primary total shoulder arthroplasty. J Shoulder Elbow Surg. 2015;24(8):1263-1267.
24. Matsen FA, Russ SM, Vu PT, Hsu JE, Lucas RM, Comstock BA. What factors are predictive of patient-reported outcomes? A prospective study of 337 shoulder arthroplasties. Clin Orthop Relat Res. 2016;474(11):2496-2510.
Shared decision-making tools, such as predictive models, can help empower the patient to make decisions for or against surgery equipped with more information about the expected outcome.
There is a role for preoperative collection of PROMs in the clinical decision-making process.
Mental health state, as reported by the VR-12 MCS, is a significant predictor of postoperative pain and function as reported by the VAS pain and ASES function scores.
A significant portion of the predictive ability of this model comes from the fact that at 1-year postoperatively, patients receiving a rTSA will on average have a 3.8 point lower on ASES function score than those receiving a TSA (P < .001, ω2=.083).
Future studies to discern the role of different modalities to improve a patient’s emotional health preoperatively will be beneficial as the healthcare industry trends toward value based medicine collecting PROMs as part of reimbursement schemes.
Over the past few decades, decisions regarding patients’ care have gradually transitioned from a paternalistic model to a more cooperative exchange between patient and physician. Shared decision-making provides patients a measure of autonomy in making choices for their health and their future. Patient participation may mitigate uncertainty and discomfort during selection of a course of treatment, which may lead to increased satisfaction levels after surgery.1 Moreover, shared decision-making may help patients better manage postoperative expectations through evidenced-based discussions of preoperative health levels and their corresponding outcomes. Patient-reported outcome measures (PROMs) use clinically sensitive and specific metrics to evaluate a patient’s self-reported pain, functional ability, and mental state.2 These metrics are useful in setting patient expectations for potential outcomes of treatment options. Use of evidence-based clinical decision-making tools, such as PROM-based predictive models, can facilitate a collaborative decision-making environment for patient and physician. Given the present cost-containment era, and the need for preoperative metrics that can assist in predictive analysis of postoperative improvement, models are clearly valuable.
In attempts to help patients set well-informed and reasonable expectations, physicians have turned to PROMs to facilitate preoperative evidence-based discussions. Although PROMs have been in use for almost 30 years, only recently have they been used to create tools that can aid quantitatively in the surgical decision-making process.2-6 Combining physical examination findings, imaging studies, comorbidities, and quantitative tools, such as this model, may enhance patients’ understanding of their preoperative condition and expected prognosis and thereby guide their surgical decisions.
We conducted a study to determine whether certain preoperative PROMs can predict 1-year postoperative visual analog scale (VAS) pain scores and American Shoulder and Elbow Surgeons (ASES) Function scores in total shoulder arthroplasty (TSA) and reverse TSA (rTSA). We hypothesized that preoperative mental health status as captured by Veterans RAND 12-Item Health Survey (VR-12) mental health component summary (MCS) score and preoperative VAS pain score would predict both VAS pain score and ASES Function score 1 year after surgery. Specifically, we hypothesized that a higher preoperative VR-12 MCS score would predict less pain and better function 1 year after surgery and that a higher preoperative VAS pain score would predict more pain and worse function 1 year after surgery.
Methods
This study was approved by the Institutional Review Board of Partners Healthcare. The study used the Surgical Outcome System (Arthrex), a comprehensive prospective database that stores preoperative and 1-year postoperative patient demographics and TSA-PROM data. Surveys are emailed to all enrolled patients before surgery and 1 year after surgery. As indicated by the Institutional Review Boards of all participating institutions, patients in the Surgical Outcome System have to sign a consent form to permit use of their responses in research.
The database includes patient data from 42 orthopedic surgeons across the United States. All primary TSAs and primary rTSAs in the database were included in this study, regardless of arthroplasty indication. Revisions were excluded. Also excluded were cases in which the 1-year postoperative questionnaire was not completed. Of the 1681 patients eligible for 1-year follow-up, 1225 (73%) completed the 1-year postoperative questionnaire. PROMs used in the study were VAS pain score, ASES Function score, VR-12 MCS score, and Single Assessment Numerical Evaluation (SANE). Unfortunately, not all surgeons use every measure in the 1-year postoperative questionnaire set. Thus, in our complete models, total number of observations was 1004 for modeling 1-year postoperative VAS pain scores and 986 for modeling 1-year postoperative ASES Function scores.
Metrics
On VAS, pain is rated from 0 (no pain) to 10 (pain as bad as it can be). Tashjian and colleagues7 estimated that the minimal clinically important difference (MCID) for postoperative VAS pain scores was 1.4 in a cohort of 326 patients who had TSA, rTSA, or shoulder hemiarthroplasty. ASES Function score is scaled from 0 to 30, with 30 representing best function.8 Wong and colleagues9 identified an MCID of 6.5 for ASES Function scores in a cohort of 107 patients who had TSA or rTSA. SANE ratings range from 0% to 100%, with 100% indicating the patient’s shoulder was totally “normal.”10 VR-12 MCS scores appear on a logarithmic scale, with higher numbers representing better mental health. The population mean estimate for VR-12 MCS scores is 50.1 (SD, 11.49; overall possible range, –2.47 to 76.1).11 Our patient population’s scores ranged from 12.5 to 73.8.
Statistical Analysis
Simple bivariate and multivariate linear regressions were performed to evaluate the predictive value of each of the outlined PROMs. Our complete model controls for patient sex, age, and type of arthroplasty. Categorical variables were dummy-coded. Both 1-year postoperative VAS pain score and 1-year postoperative ASES Function score were investigated as dependent variables. Regression coefficients and P and ω2 values are reported. Omega square represents how much of the variance in an outcome variable a model explains, like R2, and ω2 values can also be calculated for individual factors to see how much variance a given factor accounts for. For a simple relative risk calculation, we divided our cohort into 3 equal-sized groups based on preoperative VR-12 MCS scores and compared the risk that patients with scores in the top third (better mental health) would end up below certain ASES Total scores with the risk of patients with scores in the bottom third (worse mental health). All statistical analyses were performed with Stata (StataCorp).
Results
Table 1 lists summary statistics for the population used in these models.
Table 1.Our complete model for predicting VAS pain score 1 year after surgery accounted for 8% of the variability in this pain score (ω2 = .076), whereas our complete model for predicting ASES Function score 1 year after surgery accounted for 22% of the variability (ω2 = .219). These models include preoperative scores for VAS pain, ASES Function, VR-12 MCS, SANE, age at time of surgery, sex, and type of arthroplasty as possible explanatory variables.
Table 2.Predicting VAS Pain Score (Table 2)
Preoperative VAS pain score and VR-12 MCS score both predicted 1-year postoperative VAS pain score (P < .001). Preoperative ASES Function score did not predict pain 1 year after surgery. By contrast, higher preoperative VAS pain scores were associated with higher VAS pain scores 1 year after surgery. Higher preoperative VR-12 MCS scores were significantly associated with lower VAS pain scores 1 year after surgery, indicating that better preoperative mental health is significantly associated with better self-reported outcomes in terms of pain 1 year after surgery. These associations remained statistically significant when controlling for age at time of surgery, sex, and type of arthroplasty.
Preoperative VR-12 MCS score was more predictive of 1-year postoperative VAS pain score than preoperative VAS pain score was. In other words, preoperative VR-12 MCS score accounted for more variability in outcome for 1-year postoperative VAS pain score (2.4%; ω2 = .023) than preoperative VAS pain score did (1.6%; ω2 = .015).
Table 3.Predicting ASES Function Score (Table 3)
By contrast, preoperative VAS pain score did not predict 1-year postoperative ASES Function score. Preoperative ASES Function and VR-12 MCS scores both predicted 1-year postoperative ASES Function score (P < .001). Higher preoperative ASES Function scores were associated with higher 1-year postoperative ASES Function scores. In other words, reporting better shoulder function before surgery was associated with reporting better shoulder function after surgery.
An example gives a sense of the effect size associated with the coefficient for preoperative ASES Function score. Our model predicts that, compared with a patient who reports 5 points lower on preoperative ASES Function (which ranges from 0-30), a patient who reports 5 points higher will report on average about 1 point higher on 1-year postoperative ASES Function. As in the model for postoperative pain, these associations with preoperative function and mental health scores held when controlling for age, sex, and type of arthroplasty.
As in the postoperative pain model, preoperative VR-12 MCS score was more predictive of 1-year postoperative ASES Function score than preoperative ASES Function score was. Preoperative VR-12 MCS score accounted for more of the variation that our model predicts (ω2 = .029) than preoperative ASES Function score did (ω2 = .020). We compared the risk that patients with high preoperative VR-12 MCS scores (top third of cohort) would end up with ASES Total scores below 70, below 80, or below 90 with the risk of patients with low preoperative VR-12 MCS scores (bottom third). Results appear in Table 4.
Table 4.
A significant part of the predictive ability of our model for postoperative ASES Function scores stems from the fact that a patient who undergoes rTSA (vs TSA) is predicted to have an ASES Function score 3.8 points lower 1 year after surgery (P < .001, ω2 = .083). With type of arthroplasty controlled for, female sex is associated with an ASES Function score 1.6 points lower 1 year after surgery (P < .001, ω2 = .016).
Preoperative SANE score did not predict 1-year postoperative VAS pain score or ASES Function score. In addition, when our complete model was run with 1-year postoperative SANE score as the dependent variable, preoperative SANE score did not predict 1-year postoperative SANE score. Our data provide no supporting evidence for the use of SANE scores for predictive modeling for shoulder arthroplasty.
Discussion
We prospectively gathered data to determine which factors would predict patient subjective outcomes of primary TSA and primary rTSA. We hypothesized that preoperative VR-12 MCS scores and preoperative VAS pain scores would predict postoperative pain and function as measured with those PROMs. Second, we hypothesized that better preoperative mental health (as measured with VR-12 MCS scores) would predict lower postoperative pain (VAS pain scores) and better postoperative function (ASES Function scores). Third, we hypothesized that higher preoperative pain (VAS pain scores) would correlate with higher postoperative pain (VAS pain scores) and worse postoperative function (ASES Function scores).
Our main goal is to provide patients and surgeons with a predictive model that generates insights into what patients can expect after surgery. This model is not intended to be a screening tool for operative indications, but a clinical tool for helping set expectations.
Our results showed that patients with more pain before surgery were more likely to have more pain 1 year after surgery—confirming the hypothesized relationship between pain before and after surgery. Contrary to the hypothesis, however, degree of pain before surgery was not associated with function 1 year after surgery. Our mental health hypothesis was confirmed: Patients with better preoperative mental health scores had on average less pain and better function 1 year after surgery. Not surprisingly, our model demonstrated that patients with better self-reported function before surgery had better self-reported function after surgery. Patient-reported function before surgery did not significantly affect how much pain the patient had 1 year after surgery. Although we did not hypothesize about the role of function in predicting 1-year outcomes, function is a significant factor to be considered when setting patient expectations regarding shoulder arthroplasty outcomes (Table 5).
Table 5.
Although the effect sizes of each analyzed factor are small, together our models for 1-year postoperative pain and function provide significant insight into patients’ likely outcomes 1 year after TSA and rTSA.
Table 6.
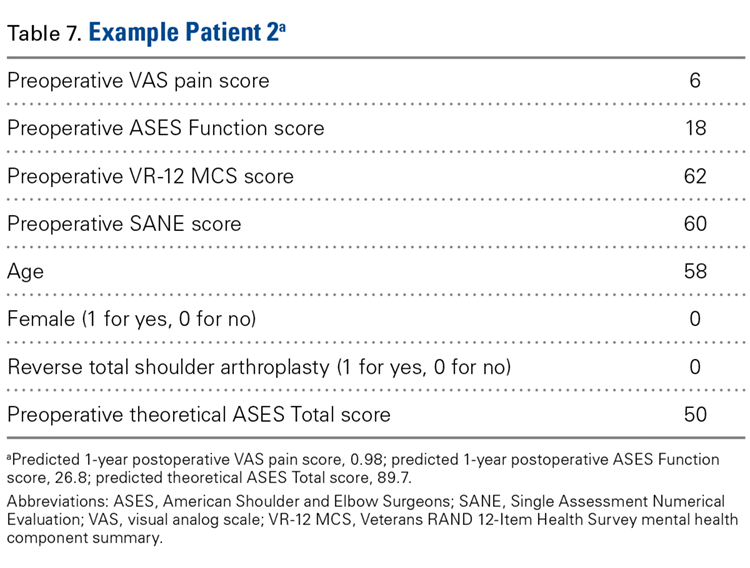
Table 7.Table 6 and Table 7 listpreoperative PROMs and baseline characteristics for 2 sample patients and the corresponding 1-year postoperative results they should expect according to our model. Patient 1 (Table 6) achieves a theoretical ASES Total score of 67, and patient 2 (Table 7) achieves a theoretical ASES Total score of 90. During discussion of surgical options, these patients should be counseled differently. If patient 1 expects a “normal” shoulder after surgery, he or she likely will be disappointed with the outcome. Tools such as those provided here can contribute to evidence-based discussions and well-informed decision making.
Many studies have found that mental health correlated with pain and function during recovery from orthopedic trauma.12-18 For example, Wylie and colleagues19 found that preoperative mental health, as measured with the 36-Item Short Form Health Survey (SF-36) MCS score, predicted patient-reported pain and function in the setting of rotator cuff injury, regardless of treatment type (operative, nonoperative). Others have found that mental health may play a role in how patients report their pain and function on various PROMs.20,21 Modalities for improving patients’ emotional health baseline may even become a preoperative requirement as the healthcare industry moves toward value-based medicine and collection of patient-related outcomes as part of reimbursement schemes.
By contrast, some studies have found that preoperative mental health did not predict postoperative outcomes. For example, Kennedy and colleagues22 found that preoperative mental health (as measured with SF-36 MCS scores) did not predict functional outcome in patients with ankle arthritis treated with ankle arthroplasty or arthrodesis. Likewise, Styron and colleagues23 found no correlation between preoperative mental health (SF-12 MCS scores) and postoperative mental health and function in TSA. Their findings contradict those of the present study and many other studies.12-18 The contradiction in findings demonstrates the need for well-designed, sufficiently powered studies of the link between preoperative mental health and postoperative outcome. Our study, with its large sample and heterogeneous population, is a start.
Two other groups (Simmen and colleagues,18 Matsen and colleagues24) have attempted to develop a model predicting outcomes of shoulder arthroplasty. Simmen and colleagues18 estimated the probability of “treatment success” 1 year after TSA. Their model had 4 factors predictive of patient outcomes. Previous shoulder surgery and age over 75 years were significantly associated with lower probability of success, whereas higher preoperative SF-36 MCS scores and higher preoperative DASH (Disabilities of the Arm, Shoulder, and Hand) Function scores were associated with higher probability of success. The authors deemed TSA successful if the patient achieved a Constant score of ≥80 out of 100. Their model predicts probability of TSA “success,” whereas our models predict particular outcome scores. Both their results and ours support the hypothesis that preoperative mental health and function scores can predict how well a patient fares after surgery. Simmen and colleagues18 based their model on a cohort of only 140 patients and reported a 33.6% success rate (47/140 surgeries).
Matsen and colleagues24 used a 1-practice cohort of 337 patients who underwent different types of arthroplasties, including TSA, rTSA, hemiarthroplasty, and ream-and-run arthroplasty. Although their focus was not preoperative PROMs predicting postoperative PROMs, they used the Simple Shoulder Test (SST) baseline score as a predictive variable. They found that 6 baseline characteristics—American Society of Anesthesiologists class I, shoulder problem unrelated to work, no prior shoulder surgery, glenoid type other than A1, humeral head not superiorly displaced on anteroposterior radiograph, and lower baseline SST score—were statistically associated with better outcomes, and they developed a model driven by these characteristics. They urged other investigators to perform the same kind of analysis with larger patient populations from multiple practices. One of the strengths of our study is its large patient population. We collected data on 1004 patients for modeling 1-year postoperative VAS pain scores and 986 patients for modeling 1-year postoperative ASES Function scores.
Our study had several limitations. First, its data came from a 42-surgeon database, and there may be variations in how these surgeons enroll patients in the registry. If some surgeons did not enroll all their surgical patients, our sample could have been subject to selection bias. Second, in developing our model, we used only patient characteristics that were available in the database. On the other hand, the heterogeneity of the surgeon sample lended external validity to the model. A third limitation was that the model always predicts better pain and function outcomes after TSA than after rTSA. In other words, it does not consider whether TSA is appropriate for a particular patient. Instead, it predicts 1-year shoulder arthroplasty outcomes.
Our goal here is not to provide outcomes information or a surgical screening tool, but to report on our use of a simple data-driven tool for setting expectations. When appropriate data become available, tools like this should be expanded to predict longer-term shoulder arthroplasty outcomes. We need more studies that combine preoperative PROMs, more baseline clinical and patient characteristics (following the Matsen and colleagues24 model), and large sample sizes.
Conclusion
The educational models presented here can help patients and surgeons learn what to expect after surgery. These models reveal the value in collecting preoperative subjective PROMs and show how a quantitative tool can help facilitate shared decision-making and set patient expectations. Separately, the effect size of each factor is small, but together a patient’s preoperative VAS pain score, ASES Function score, VR-12 MCS score, age, sex, and type of arthroplasty can provide information predictive of the patient’s self-reported pain and function 1 year after surgery.
Take-Home Points
Shared decision-making tools, such as predictive models, can help empower the patient to make decisions for or against surgery equipped with more information about the expected outcome.
There is a role for preoperative collection of PROMs in the clinical decision-making process.
Mental health state, as reported by the VR-12 MCS, is a significant predictor of postoperative pain and function as reported by the VAS pain and ASES function scores.
A significant portion of the predictive ability of this model comes from the fact that at 1-year postoperatively, patients receiving a rTSA will on average have a 3.8 point lower on ASES function score than those receiving a TSA (P < .001, ω2=.083).
Future studies to discern the role of different modalities to improve a patient’s emotional health preoperatively will be beneficial as the healthcare industry trends toward value based medicine collecting PROMs as part of reimbursement schemes.
Over the past few decades, decisions regarding patients’ care have gradually transitioned from a paternalistic model to a more cooperative exchange between patient and physician. Shared decision-making provides patients a measure of autonomy in making choices for their health and their future. Patient participation may mitigate uncertainty and discomfort during selection of a course of treatment, which may lead to increased satisfaction levels after surgery.1 Moreover, shared decision-making may help patients better manage postoperative expectations through evidenced-based discussions of preoperative health levels and their corresponding outcomes. Patient-reported outcome measures (PROMs) use clinically sensitive and specific metrics to evaluate a patient’s self-reported pain, functional ability, and mental state.2 These metrics are useful in setting patient expectations for potential outcomes of treatment options. Use of evidence-based clinical decision-making tools, such as PROM-based predictive models, can facilitate a collaborative decision-making environment for patient and physician. Given the present cost-containment era, and the need for preoperative metrics that can assist in predictive analysis of postoperative improvement, models are clearly valuable.
In attempts to help patients set well-informed and reasonable expectations, physicians have turned to PROMs to facilitate preoperative evidence-based discussions. Although PROMs have been in use for almost 30 years, only recently have they been used to create tools that can aid quantitatively in the surgical decision-making process.2-6 Combining physical examination findings, imaging studies, comorbidities, and quantitative tools, such as this model, may enhance patients’ understanding of their preoperative condition and expected prognosis and thereby guide their surgical decisions.
We conducted a study to determine whether certain preoperative PROMs can predict 1-year postoperative visual analog scale (VAS) pain scores and American Shoulder and Elbow Surgeons (ASES) Function scores in total shoulder arthroplasty (TSA) and reverse TSA (rTSA). We hypothesized that preoperative mental health status as captured by Veterans RAND 12-Item Health Survey (VR-12) mental health component summary (MCS) score and preoperative VAS pain score would predict both VAS pain score and ASES Function score 1 year after surgery. Specifically, we hypothesized that a higher preoperative VR-12 MCS score would predict less pain and better function 1 year after surgery and that a higher preoperative VAS pain score would predict more pain and worse function 1 year after surgery.
Methods
This study was approved by the Institutional Review Board of Partners Healthcare. The study used the Surgical Outcome System (Arthrex), a comprehensive prospective database that stores preoperative and 1-year postoperative patient demographics and TSA-PROM data. Surveys are emailed to all enrolled patients before surgery and 1 year after surgery. As indicated by the Institutional Review Boards of all participating institutions, patients in the Surgical Outcome System have to sign a consent form to permit use of their responses in research.
The database includes patient data from 42 orthopedic surgeons across the United States. All primary TSAs and primary rTSAs in the database were included in this study, regardless of arthroplasty indication. Revisions were excluded. Also excluded were cases in which the 1-year postoperative questionnaire was not completed. Of the 1681 patients eligible for 1-year follow-up, 1225 (73%) completed the 1-year postoperative questionnaire. PROMs used in the study were VAS pain score, ASES Function score, VR-12 MCS score, and Single Assessment Numerical Evaluation (SANE). Unfortunately, not all surgeons use every measure in the 1-year postoperative questionnaire set. Thus, in our complete models, total number of observations was 1004 for modeling 1-year postoperative VAS pain scores and 986 for modeling 1-year postoperative ASES Function scores.
Metrics
On VAS, pain is rated from 0 (no pain) to 10 (pain as bad as it can be). Tashjian and colleagues7 estimated that the minimal clinically important difference (MCID) for postoperative VAS pain scores was 1.4 in a cohort of 326 patients who had TSA, rTSA, or shoulder hemiarthroplasty. ASES Function score is scaled from 0 to 30, with 30 representing best function.8 Wong and colleagues9 identified an MCID of 6.5 for ASES Function scores in a cohort of 107 patients who had TSA or rTSA. SANE ratings range from 0% to 100%, with 100% indicating the patient’s shoulder was totally “normal.”10 VR-12 MCS scores appear on a logarithmic scale, with higher numbers representing better mental health. The population mean estimate for VR-12 MCS scores is 50.1 (SD, 11.49; overall possible range, –2.47 to 76.1).11 Our patient population’s scores ranged from 12.5 to 73.8.
Statistical Analysis
Simple bivariate and multivariate linear regressions were performed to evaluate the predictive value of each of the outlined PROMs. Our complete model controls for patient sex, age, and type of arthroplasty. Categorical variables were dummy-coded. Both 1-year postoperative VAS pain score and 1-year postoperative ASES Function score were investigated as dependent variables. Regression coefficients and P and ω2 values are reported. Omega square represents how much of the variance in an outcome variable a model explains, like R2, and ω2 values can also be calculated for individual factors to see how much variance a given factor accounts for. For a simple relative risk calculation, we divided our cohort into 3 equal-sized groups based on preoperative VR-12 MCS scores and compared the risk that patients with scores in the top third (better mental health) would end up below certain ASES Total scores with the risk of patients with scores in the bottom third (worse mental health). All statistical analyses were performed with Stata (StataCorp).
Results
Table 1 lists summary statistics for the population used in these models.
Table 1.Our complete model for predicting VAS pain score 1 year after surgery accounted for 8% of the variability in this pain score (ω2 = .076), whereas our complete model for predicting ASES Function score 1 year after surgery accounted for 22% of the variability (ω2 = .219). These models include preoperative scores for VAS pain, ASES Function, VR-12 MCS, SANE, age at time of surgery, sex, and type of arthroplasty as possible explanatory variables.
Table 2.Predicting VAS Pain Score (Table 2)
Preoperative VAS pain score and VR-12 MCS score both predicted 1-year postoperative VAS pain score (P < .001). Preoperative ASES Function score did not predict pain 1 year after surgery. By contrast, higher preoperative VAS pain scores were associated with higher VAS pain scores 1 year after surgery. Higher preoperative VR-12 MCS scores were significantly associated with lower VAS pain scores 1 year after surgery, indicating that better preoperative mental health is significantly associated with better self-reported outcomes in terms of pain 1 year after surgery. These associations remained statistically significant when controlling for age at time of surgery, sex, and type of arthroplasty.
Preoperative VR-12 MCS score was more predictive of 1-year postoperative VAS pain score than preoperative VAS pain score was. In other words, preoperative VR-12 MCS score accounted for more variability in outcome for 1-year postoperative VAS pain score (2.4%; ω2 = .023) than preoperative VAS pain score did (1.6%; ω2 = .015).
Table 3.Predicting ASES Function Score (Table 3)
By contrast, preoperative VAS pain score did not predict 1-year postoperative ASES Function score. Preoperative ASES Function and VR-12 MCS scores both predicted 1-year postoperative ASES Function score (P < .001). Higher preoperative ASES Function scores were associated with higher 1-year postoperative ASES Function scores. In other words, reporting better shoulder function before surgery was associated with reporting better shoulder function after surgery.
An example gives a sense of the effect size associated with the coefficient for preoperative ASES Function score. Our model predicts that, compared with a patient who reports 5 points lower on preoperative ASES Function (which ranges from 0-30), a patient who reports 5 points higher will report on average about 1 point higher on 1-year postoperative ASES Function. As in the model for postoperative pain, these associations with preoperative function and mental health scores held when controlling for age, sex, and type of arthroplasty.
As in the postoperative pain model, preoperative VR-12 MCS score was more predictive of 1-year postoperative ASES Function score than preoperative ASES Function score was. Preoperative VR-12 MCS score accounted for more of the variation that our model predicts (ω2 = .029) than preoperative ASES Function score did (ω2 = .020). We compared the risk that patients with high preoperative VR-12 MCS scores (top third of cohort) would end up with ASES Total scores below 70, below 80, or below 90 with the risk of patients with low preoperative VR-12 MCS scores (bottom third). Results appear in Table 4.
Table 4.
A significant part of the predictive ability of our model for postoperative ASES Function scores stems from the fact that a patient who undergoes rTSA (vs TSA) is predicted to have an ASES Function score 3.8 points lower 1 year after surgery (P < .001, ω2 = .083). With type of arthroplasty controlled for, female sex is associated with an ASES Function score 1.6 points lower 1 year after surgery (P < .001, ω2 = .016).
Preoperative SANE score did not predict 1-year postoperative VAS pain score or ASES Function score. In addition, when our complete model was run with 1-year postoperative SANE score as the dependent variable, preoperative SANE score did not predict 1-year postoperative SANE score. Our data provide no supporting evidence for the use of SANE scores for predictive modeling for shoulder arthroplasty.
Discussion
We prospectively gathered data to determine which factors would predict patient subjective outcomes of primary TSA and primary rTSA. We hypothesized that preoperative VR-12 MCS scores and preoperative VAS pain scores would predict postoperative pain and function as measured with those PROMs. Second, we hypothesized that better preoperative mental health (as measured with VR-12 MCS scores) would predict lower postoperative pain (VAS pain scores) and better postoperative function (ASES Function scores). Third, we hypothesized that higher preoperative pain (VAS pain scores) would correlate with higher postoperative pain (VAS pain scores) and worse postoperative function (ASES Function scores).
Our main goal is to provide patients and surgeons with a predictive model that generates insights into what patients can expect after surgery. This model is not intended to be a screening tool for operative indications, but a clinical tool for helping set expectations.
Our results showed that patients with more pain before surgery were more likely to have more pain 1 year after surgery—confirming the hypothesized relationship between pain before and after surgery. Contrary to the hypothesis, however, degree of pain before surgery was not associated with function 1 year after surgery. Our mental health hypothesis was confirmed: Patients with better preoperative mental health scores had on average less pain and better function 1 year after surgery. Not surprisingly, our model demonstrated that patients with better self-reported function before surgery had better self-reported function after surgery. Patient-reported function before surgery did not significantly affect how much pain the patient had 1 year after surgery. Although we did not hypothesize about the role of function in predicting 1-year outcomes, function is a significant factor to be considered when setting patient expectations regarding shoulder arthroplasty outcomes (Table 5).
Table 5.
Although the effect sizes of each analyzed factor are small, together our models for 1-year postoperative pain and function provide significant insight into patients’ likely outcomes 1 year after TSA and rTSA.
Table 6.
Table 7.Table 6 and Table 7 listpreoperative PROMs and baseline characteristics for 2 sample patients and the corresponding 1-year postoperative results they should expect according to our model. Patient 1 (Table 6) achieves a theoretical ASES Total score of 67, and patient 2 (Table 7) achieves a theoretical ASES Total score of 90. During discussion of surgical options, these patients should be counseled differently. If patient 1 expects a “normal” shoulder after surgery, he or she likely will be disappointed with the outcome. Tools such as those provided here can contribute to evidence-based discussions and well-informed decision making.
Many studies have found that mental health correlated with pain and function during recovery from orthopedic trauma.12-18 For example, Wylie and colleagues19 found that preoperative mental health, as measured with the 36-Item Short Form Health Survey (SF-36) MCS score, predicted patient-reported pain and function in the setting of rotator cuff injury, regardless of treatment type (operative, nonoperative). Others have found that mental health may play a role in how patients report their pain and function on various PROMs.20,21 Modalities for improving patients’ emotional health baseline may even become a preoperative requirement as the healthcare industry moves toward value-based medicine and collection of patient-related outcomes as part of reimbursement schemes.
By contrast, some studies have found that preoperative mental health did not predict postoperative outcomes. For example, Kennedy and colleagues22 found that preoperative mental health (as measured with SF-36 MCS scores) did not predict functional outcome in patients with ankle arthritis treated with ankle arthroplasty or arthrodesis. Likewise, Styron and colleagues23 found no correlation between preoperative mental health (SF-12 MCS scores) and postoperative mental health and function in TSA. Their findings contradict those of the present study and many other studies.12-18 The contradiction in findings demonstrates the need for well-designed, sufficiently powered studies of the link between preoperative mental health and postoperative outcome. Our study, with its large sample and heterogeneous population, is a start.
Two other groups (Simmen and colleagues,18 Matsen and colleagues24) have attempted to develop a model predicting outcomes of shoulder arthroplasty. Simmen and colleagues18 estimated the probability of “treatment success” 1 year after TSA. Their model had 4 factors predictive of patient outcomes. Previous shoulder surgery and age over 75 years were significantly associated with lower probability of success, whereas higher preoperative SF-36 MCS scores and higher preoperative DASH (Disabilities of the Arm, Shoulder, and Hand) Function scores were associated with higher probability of success. The authors deemed TSA successful if the patient achieved a Constant score of ≥80 out of 100. Their model predicts probability of TSA “success,” whereas our models predict particular outcome scores. Both their results and ours support the hypothesis that preoperative mental health and function scores can predict how well a patient fares after surgery. Simmen and colleagues18 based their model on a cohort of only 140 patients and reported a 33.6% success rate (47/140 surgeries).
Matsen and colleagues24 used a 1-practice cohort of 337 patients who underwent different types of arthroplasties, including TSA, rTSA, hemiarthroplasty, and ream-and-run arthroplasty. Although their focus was not preoperative PROMs predicting postoperative PROMs, they used the Simple Shoulder Test (SST) baseline score as a predictive variable. They found that 6 baseline characteristics—American Society of Anesthesiologists class I, shoulder problem unrelated to work, no prior shoulder surgery, glenoid type other than A1, humeral head not superiorly displaced on anteroposterior radiograph, and lower baseline SST score—were statistically associated with better outcomes, and they developed a model driven by these characteristics. They urged other investigators to perform the same kind of analysis with larger patient populations from multiple practices. One of the strengths of our study is its large patient population. We collected data on 1004 patients for modeling 1-year postoperative VAS pain scores and 986 patients for modeling 1-year postoperative ASES Function scores.
Our study had several limitations. First, its data came from a 42-surgeon database, and there may be variations in how these surgeons enroll patients in the registry. If some surgeons did not enroll all their surgical patients, our sample could have been subject to selection bias. Second, in developing our model, we used only patient characteristics that were available in the database. On the other hand, the heterogeneity of the surgeon sample lended external validity to the model. A third limitation was that the model always predicts better pain and function outcomes after TSA than after rTSA. In other words, it does not consider whether TSA is appropriate for a particular patient. Instead, it predicts 1-year shoulder arthroplasty outcomes.
Our goal here is not to provide outcomes information or a surgical screening tool, but to report on our use of a simple data-driven tool for setting expectations. When appropriate data become available, tools like this should be expanded to predict longer-term shoulder arthroplasty outcomes. We need more studies that combine preoperative PROMs, more baseline clinical and patient characteristics (following the Matsen and colleagues24 model), and large sample sizes.
Conclusion
The educational models presented here can help patients and surgeons learn what to expect after surgery. These models reveal the value in collecting preoperative subjective PROMs and show how a quantitative tool can help facilitate shared decision-making and set patient expectations. Separately, the effect size of each factor is small, but together a patient’s preoperative VAS pain score, ASES Function score, VR-12 MCS score, age, sex, and type of arthroplasty can provide information predictive of the patient’s self-reported pain and function 1 year after surgery.
References
1. Stacey D, Légaré F, Col NF, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2014;(1):CD001431.
2. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. Can preoperative patient-reported outcome measures be used to predict meaningful improvement in function after TKA? Clin Orthop Relat Res. 2017;475(1):149-157.
3. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. John Charnley award: preoperative patient-reported outcome measures predict clinically meaningful improvement in function after THA. Clin Orthop Relat Res. 2016;474(2):321-329.
4. Wong SE, Zhang AL, Berliner JL, Ma CB, Feeley BT. Preoperative patient-reported scores can predict postoperative outcomes after shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(6):913-919.
5. Werner BC, Chang B, Nguyen JT, Dines DM, Gulotta LV. What change in American Shoulder and Elbow Surgeons score represents a clinically important change after shoulder arthroplasty? Clin Orthop Relat Res. 2016;474(12):2672-2681.
7. Tashjian RZ, Hung M, Keener JD, et al. Determining the minimal clinically important difference for the American Shoulder and Elbow Surgeons score, Simple Shoulder Test, and visual analog scale (VAS) measuring pain after shoulder arthroplasty. J Shoulder Elbow Surg. 2017;26(1):144-148.
8. Michener LA, McClure PW, Sennett BJ. American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, patient self-report section: reliability, validity, and responsiveness. J Shoulder Elbow Surg. 2002;11(6):587-594.
9. Wong SE, Zhang AL, Berliner JL, Ma CB, Feeley BT. Preoperative patient-reported scores can predict postoperative outcomes after shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(6):913-919.
10. Williams GN, Gangel TJ, Arciero RA, Uhorchak JM, Taylor DC. Comparison of the Single Assessment Numeric Evaluation method and two shoulder rating scales. Outcomes measures after shoulder surgery. Am J Sports Med. 1999;27(2):214-221.
11. Selim AJ, Rogers W, Fleishman JA, et al. Updated U.S. population standard for the Veterans RAND 12-Item Health Survey (VR-12). Qual Life Res. 2009;18(1):43-52.
12. Ayers DC, Franklin PD, Ploutz-Snyder R, Boisvert CB. Total knee replacement outcome and coexisting physical and emotional illness. Clin Orthop Relat Res. 2005;(440):157-161.
13. Ayers DC, Franklin PD, Trief PM, Ploutz-Snyder R, Freund D. Psychological attributes of preoperative total joint replacement patients: implications for optimal physical outcome. J Arthroplasty. 2004;19(7 suppl 2):125-130.
14. Barlow JD, Bishop JY, Dunn WR, Kuhn JE; MOON Shoulder Group. What factors are predictors of emotional health in patients with full-thickness rotator cuff tears? J Shoulder Elbow Surg. 2016;25(11):1769-1773.
15. Gandhi R, Davey JR, Mahomed NN. Predicting patient dissatisfaction following joint replacement surgery. J Rheumatol. 2008;35(12):2415-2418.
16. Parr J, Borsa P, Fillingim R, et al. Psychological influences predict recovery following exercise induced shoulder pain. Int J Sports Med. 2014;35(3):232-237.
18. Simmen BR, Bachmann LM, Drerup S, Schwyzer HK, Burkhart A, Goldhahn J. Development of a predictive model for estimating the probability of treatment success one year after total shoulder replacement—cohort study. Osteoarthritis Cartilage. 2008;16(5):631-634.
19. Wylie JD, Suter T, Potter MQ, Granger EK, Tashjian RZ. Mental health has a stronger association with patient-reported shoulder pain and function than tear size in patients with full-thickness rotator cuff tears. J Bone Joint Surg Am. 2016;98(4):251-256.
20. Potter MQ, Wylie JD, Greis PE, Burks RT, Tashjian RZ. Psychological distress negatively affects self-assessment of shoulder function in patients with rotator cuff tears. Clin Orthop Relat Res. 2014;472(12):3926-3932.
21. Roh YH, Noh JH, Oh JH, Baek GH, Gong HS. To what degree do shoulder outcome instruments reflect patients’ psychologic distress? Clin Orthop Relat Res. 2012;470(12):3470-3477.
22. Kennedy S, Barske H, Wing K, et al. SF-36 mental component summary (MCS) score does not predict functional outcome after surgery for end-stage ankle arthritis. J Bone Joint Surg Am. 2015;97(20):1702-1707.
23. Styron JF, Higuera CA, Strnad G, Iannotti JP. Greater patient confidence yields greater functional outcomes after primary total shoulder arthroplasty. J Shoulder Elbow Surg. 2015;24(8):1263-1267.
24. Matsen FA, Russ SM, Vu PT, Hsu JE, Lucas RM, Comstock BA. What factors are predictive of patient-reported outcomes? A prospective study of 337 shoulder arthroplasties. Clin Orthop Relat Res. 2016;474(11):2496-2510.
References
1. Stacey D, Légaré F, Col NF, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2014;(1):CD001431.
2. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. Can preoperative patient-reported outcome measures be used to predict meaningful improvement in function after TKA? Clin Orthop Relat Res. 2017;475(1):149-157.
3. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. John Charnley award: preoperative patient-reported outcome measures predict clinically meaningful improvement in function after THA. Clin Orthop Relat Res. 2016;474(2):321-329.
4. Wong SE, Zhang AL, Berliner JL, Ma CB, Feeley BT. Preoperative patient-reported scores can predict postoperative outcomes after shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(6):913-919.
5. Werner BC, Chang B, Nguyen JT, Dines DM, Gulotta LV. What change in American Shoulder and Elbow Surgeons score represents a clinically important change after shoulder arthroplasty? Clin Orthop Relat Res. 2016;474(12):2672-2681.
7. Tashjian RZ, Hung M, Keener JD, et al. Determining the minimal clinically important difference for the American Shoulder and Elbow Surgeons score, Simple Shoulder Test, and visual analog scale (VAS) measuring pain after shoulder arthroplasty. J Shoulder Elbow Surg. 2017;26(1):144-148.
8. Michener LA, McClure PW, Sennett BJ. American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, patient self-report section: reliability, validity, and responsiveness. J Shoulder Elbow Surg. 2002;11(6):587-594.
9. Wong SE, Zhang AL, Berliner JL, Ma CB, Feeley BT. Preoperative patient-reported scores can predict postoperative outcomes after shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(6):913-919.
10. Williams GN, Gangel TJ, Arciero RA, Uhorchak JM, Taylor DC. Comparison of the Single Assessment Numeric Evaluation method and two shoulder rating scales. Outcomes measures after shoulder surgery. Am J Sports Med. 1999;27(2):214-221.
11. Selim AJ, Rogers W, Fleishman JA, et al. Updated U.S. population standard for the Veterans RAND 12-Item Health Survey (VR-12). Qual Life Res. 2009;18(1):43-52.
12. Ayers DC, Franklin PD, Ploutz-Snyder R, Boisvert CB. Total knee replacement outcome and coexisting physical and emotional illness. Clin Orthop Relat Res. 2005;(440):157-161.
13. Ayers DC, Franklin PD, Trief PM, Ploutz-Snyder R, Freund D. Psychological attributes of preoperative total joint replacement patients: implications for optimal physical outcome. J Arthroplasty. 2004;19(7 suppl 2):125-130.
14. Barlow JD, Bishop JY, Dunn WR, Kuhn JE; MOON Shoulder Group. What factors are predictors of emotional health in patients with full-thickness rotator cuff tears? J Shoulder Elbow Surg. 2016;25(11):1769-1773.
15. Gandhi R, Davey JR, Mahomed NN. Predicting patient dissatisfaction following joint replacement surgery. J Rheumatol. 2008;35(12):2415-2418.
16. Parr J, Borsa P, Fillingim R, et al. Psychological influences predict recovery following exercise induced shoulder pain. Int J Sports Med. 2014;35(3):232-237.
18. Simmen BR, Bachmann LM, Drerup S, Schwyzer HK, Burkhart A, Goldhahn J. Development of a predictive model for estimating the probability of treatment success one year after total shoulder replacement—cohort study. Osteoarthritis Cartilage. 2008;16(5):631-634.
19. Wylie JD, Suter T, Potter MQ, Granger EK, Tashjian RZ. Mental health has a stronger association with patient-reported shoulder pain and function than tear size in patients with full-thickness rotator cuff tears. J Bone Joint Surg Am. 2016;98(4):251-256.
20. Potter MQ, Wylie JD, Greis PE, Burks RT, Tashjian RZ. Psychological distress negatively affects self-assessment of shoulder function in patients with rotator cuff tears. Clin Orthop Relat Res. 2014;472(12):3926-3932.
21. Roh YH, Noh JH, Oh JH, Baek GH, Gong HS. To what degree do shoulder outcome instruments reflect patients’ psychologic distress? Clin Orthop Relat Res. 2012;470(12):3470-3477.
22. Kennedy S, Barske H, Wing K, et al. SF-36 mental component summary (MCS) score does not predict functional outcome after surgery for end-stage ankle arthritis. J Bone Joint Surg Am. 2015;97(20):1702-1707.
23. Styron JF, Higuera CA, Strnad G, Iannotti JP. Greater patient confidence yields greater functional outcomes after primary total shoulder arthroplasty. J Shoulder Elbow Surg. 2015;24(8):1263-1267.
24. Matsen FA, Russ SM, Vu PT, Hsu JE, Lucas RM, Comstock BA. What factors are predictive of patient-reported outcomes? A prospective study of 337 shoulder arthroplasties. Clin Orthop Relat Res. 2016;474(11):2496-2510.