User login
In a survey distributed to 50 member hospitals by Allen Rosenstein, MD, and his colleagues at VHA Inc. (an alliance of 2,400 nonprofit health care organizations) more than 1,500 participants responded to questions pertaining to their colleagues’ behavior.1 Of the 965 respondents to the question Have you ever witnessed disruptive behavior from a physician at your hospital?, nearly 68% said yes. Of the 675 nurses who responded to the question, 86% said they had witnessed it; almost half of the 249 physician respondents said they had witnessed it from their peers. Most respondents estimated the number of either nurses or physicians who exhibited disruptive behavior to be 1%-3%.
Of the 1,416 respondents who answered the question How often does physician disruptive behavior occur at your hospital?, 22% answered “weekly,” 26% answered “1 to 2 times per month,” and 33% answered “1 to 5 times per year.” Interestingly, 11% of the respondents said that such behavior by physicians never occurs, but 8% said it’s a daily occurrence.
—Scott Flanders, associate professor of medicine at the University of Michigan and director of the Hospitalist Program, Ann Arbor
Disruptive Behavior Defined
Disruptive behavior includes anything that interferes with the ability of a healthcare professional to effectively perform his or her duties or any behavior that undermines confidence in the hospital or its workers.2-4 In general, “disruptive” refers to behaviors that are abusive, disrespectful, sexual, angry, critical, negative, inappropriate, or unethical.2 (See “What Is Disruptive Behavior?” p. 40.) Individuals termed “impaired” are those who have active addictions or psychiatric problems and who exhibit the disruptive, intimidating, or abusive behavior.
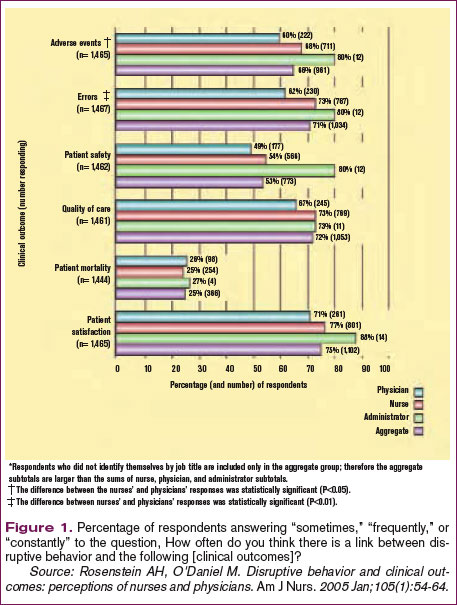
Most respondents to the above-mentioned survey reported that disruptive behavior had negative or worsening effects on stress, frustration, concentration, communication, collaboration, information transfer, and workplace relationships. (See Figure 1, p. 41.)
“Physicians whose performance persistently falters pose a substantial threat to patient safety that is often unrecognized or unsatisfactorily addressed in hospitals and other healthcare organizations,” writes Lucian Leape, MD, adjunct professor of health policy in the Department of Health Policy and Management at the Harvard School of Public Health.2
“Whoever tells you that they have not experienced any kind of disruptive behavior is either lying or … in neglect, because there are always certain types of disruptive behaviors [among healthcare workers],” says Martin Izakovic, MD, medical director, Hospitalist Program, Mercy Hospital, Iowa City, Iowa.
Effects of Disruptive Behavior
Can we go so far as to say disruptive behavior affects clinical outcomes?
“It has to,” says Scott Flanders, MD, associate professor of medicine at the University of Michigan and director of the hospitalist program, Ann Arbor, and member of SHM’s board of directors. “People clearly understand the importance of teamwork in hospital medicine. If one member of the team is dysfunctional from an emotional intelligence/behavioral standpoint, that drags down the team in its entirety and impacts patient care.”
Providing safe and effective care should be the first priority of all healthcare professionals. Excellent outcomes have been associated with procedural efficiency and the use of evidence-based standards and tools designed to reduce the likelihood of medical error. The effects of work relationships on clinical outcomes are less well documented, but attention to the matter is increasing in parallel with the focus on patient safety.3,5
Dr. Leape, one of the founders of the National Patient Safety Foundation, devotes concerted energy to making organizations aware of the need to upgrade systems to diagnose and treat this problem.2 “Physician performance failures are not rare and pose substantial threats to patient welfare and safety,” he writes. “Few hospitals respond to such failures promptly or effectively. Failure to ensure the quality and safety of the performance of colleagues is a breach of medicine’s fiduciary responsibility to the public.”6
When it comes to the issues of behavior, besides monitoring their own performance, what do hospitalists do when they come up against colleagues whose shortcomings require correction in order for the entire institution to uphold its legal obligation to each patient?
Physician, Heal Thyself
A study published by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) reported that 24% of sentinel events could be attributed to problems referred to as human factors, including communication gaps, staffing issues, and lack of teamwork.2, 5 The March 2004 issue of the Institute for Safe Medication Practice’s (ISMP) Medication Safety Alert reported that 7% of medication errors could be attributed to nurses feeling intimidated by physicians.4 And, as a response to this growing problem, the Institute of Medicine’s groundbreaking report on medical errors and patient safety, To Err is Human, shifted the focus from individual blame to that of preventing errors through efforts to “design safety into systems.”7
Dr. Flanders, who is also associate chief for the Division of General Internal Medicine for Inpatient Programs at the University of Michigan Medical Center (Ann Arbor), certainly understands the need to grapple with these types of issues. He is a member of his institution’s interdisciplinary Medical Staff Quality Committee (MSQC), which works to get a better handle on individual physician-level quality and performance.
“A lot stems from JCAHO’s increased focus on institutions doing a better job of trying to figure out, in short, who’s a good doctor and who’s a bad doctor,” he says, “And having medical staff appointments, privileging, and assessment of clinical skills be something a little more robust than just asking four of your friends if they think you’re a good doctor.”
One of the charges of the MSQC is developing a better system of tracking physicians’ clinical skills down to the individual level, which Dr. Flanders says is a difficult task. But their second charge is even more elusive to track: examining “the range of daily activities, behaviors, and actions that encompass being a physician.” As part of that, the committee deals with interpersonal relations: interactions with other staff and behavioral issues.
Make the Diagnosis, Initiate Treatment
As with most academic medical centers, when someone at MSQC observes a behavioral issue, that person’s supervisor (often a department chair) is the next place for the buck to stop. There are clearly defined lines of communication and “very robust systems” to deal with these kinds of things, says Dr. Flanders.
MSQC is assisting department chairs in dealing with a particular behavior or problem. “It is a venue to vet particular problems and solutions,” he says. Ultimately, if there are repeated transgressions and administration is not satisfied that their directives have been followed, the committee can recommend revoking a physician’s medical staff privileges and implementing a remediation plan.
Those robust systems have not differed in medical institutions for the last 50 years. “I think what has changed is people are less willing to tolerate this persistently,” says Dr. Flanders. “People used to put up with the disruptive physician, the badly behaving physician, and if he was bringing in lots of research dollars or if he was a great scientist, [they’d be more likely to] accept bad behavior.”
With the increased risk of litigation and the increasing scrutiny on patient safety, these offenses can no longer be tolerated.8
At a community hospital, the hierarchies and channels of communication for handling behavioral issues are different. Because of the different atmosphere and mood of a hospitalist department, says Dr. Izakovic, who is also adjunct clinical assistant professor, Department of Internal Medicine, University of Iowa–Carver College of Medicine, Iowa City, “plus word of mouth, it is easier to either enforce or, even more, lead by example [such that] certain behaviors are [encouraged] and certain behavior types are suppressed.”
Michael Zavarin, MD, director of the hospitalist group at Jordan Hospital in Plymouth, Mass., agrees that the environment of a community hospital may be different enough so that handling disruptive behavior also occurs differently than it does in an academic medical center.
Dr. Zavarin’s group is composed of 6.5 full-time day hospitalists and one full-time night hospitalist, as well as two nurse practitioners. Disruptive behavior in his group “really hasn’t been an issue, so I guess it is [dealt with] on an as-needed basis,” he says, and he can only speculate that the proper channel for dealing with situations involving disruptive behavior would be his institution’s medical executive committee.
When Dr. Izakovic faces situations involving disruptive behavior, he says, it is generally an instance in which a hospitalist has “a good intention, but feels pressured by overwork or patient care circumstances, or [has] difficulty communicating or handling the nursing staff … who perceive [the physician’s behavior] as being either threatening or disrespectful or just not called for.”9
He estimates that these instances occur most often when a physician’s expectations are not met regarding duties being performed in a timely manner. Formal complaints are rarely made in his group—maybe two or three times a year. In those cases, he is responsible for formal follow-up, which requires having a one-on-one conversation with the physician and reporting back to the risk management department. But he prefers doing what is necessary to avoid a situation getting to that stage. Informal behavior-related events happen at least monthly, he estimates. “I’d rather hear earlier than later, with no formal complaint, no formal channel,” says Dr. Izakovic.
Blow the Whistle
What are the political ramifications of blowing the whistle on a disruptive colleague? The University of Michigan’s MSQC was created largely to help get at that issue and to create a place where such subjects can be brought up anonymously. [It can be done] if the reporting person wishes. In most situations, there has been a concerted effort against backlash just as there is when incidents and errors are reported to improve or maintain patient safety.
“As the patient safety culture changes, and I think it is changing, it’s going to facilitate culture change on this issue, too,” says Dr. Flanders, “because I think people are beginning to recognize, appropriately so, that some of these behavioral issues are safety issues.”
Do nurses feel comfortable reporting such instances? “I think it depends on the personality,” says Dr. Izakovic. “Some do, and some feel less comfortable; there are nurses who never complain and nurses who always complain, like doctors and everybody else. But I think that the climate is changing [so] that raising your voice and pointing toward deficiency and/or imperfection is becoming, if not [socially] acceptable, then [at least] a standard of behavior.”
Behavior, Safety, and Quality
“Communication is the key to success in today’s medicine,” says Dr. Izakovic. “Specifically among hospitalists: You communicate with the family physician, the patient, the referring specialist, or specialist that you called, the family, nurses, and patients all around the hospital.” And although communication is the most important part of the hospitalist’s practice, he says, “it sometimes leads to tension, and it’s not as much the message that you want to convey as the form [you use] and how it is transferred.”
Nurses are key stakeholders in reporting these behaviors, just as they are encouraged to report errors as an expression of their professionalism. Certainly, Dr. Flanders says, reporting a behavioral incident is “a lot more personal and less tangible than reporting a wrong dose on a medication.”
He has noticed a dramatic increase in the number of messages he receives about inappropriate or dangerous behavior among physicians. Everyone has a bad day from time to time, he says, but at the end of the year, “if I have one physician who has been mentioned 15 times, that helps me assess that person overall as a professional and be able to say, ‘Listen, there may be some red flags here’ and [then we can] begin to intervene and try to change that behavior.”
Effective systems employed to adequately address performance problems should be fair, objective, and responsive, writes Dr. Leape.2,6 Strategies available to handle incidents of disruptive behavior include adopting performance standards for behavior as well as competence. All physicians should be required to acknowledge in writing that they have read and understood these standards and that persistent failure to uphold them will result in loss of clinical privileges. Adherence to standards should be monitored annually and provided confidentially to each individual. Finally, assessment and treatment programs must be available to manage all the underlying causes of sub-par performance. The long-term objective is to enable physicians to continue to practice, as opposed to attempting to “weed them out.”
Prevention
According to Balazs Zsenits, MD, director, Division of Hospital Medicine at Rochester General Hospital, Rochester, N.Y., two mechanisms should be applied when discussing the prevention of disruptive behavior.
“First, physician selection should be conducted by a thorough interview process,” he says, “including at least a full-day face-to-face interview, discussion with previous employers, assessment of team-participation experience, and communication skills.”
Also, you need to clarify your expectations by means of “written policies, leading by example, promoting this culture in meetings, etc., and proactively monitoring performance,” says Dr. Zsenits. That means talking with doctors, nurses, and families and actively looking for feedback. “This process is time-intensive and may be under-recognized during resource allocation, but I believe it is a tool that may prevent this and many other common problems from growing out of control.”
A director of a hospital medicine group may have to deal with the perception of an escalating number of complaints about physician behaviors. “The growth of a hospitalist program that goes from seeing a small fraction of patients within a hospital to seeing the majority of medical admissions creates challenges beyond just simply managing the increased number of doctors and complaints,” says Dr. Zsenits. “Our co-workers and stakeholders might develop an impression that ‘most doctor problems’ in the hospital are related to the hospitalists. Even if this is [because] the hospitalists actually take care of most patients in house, and each hospitalist takes care of many more patients than private attendings used to, avoiding the perception that this single group is associated with most complaints is a difficult task.”
Although hospitalists’ focus on teamwork and quality of care may improve the actual statistics, he adds, “some factors may create more feedback, including more complaints; for example, being new docs to patients and relatives at times of stress, and having a closer working relationship with nurses, which may [be problematic] by creating heightened expectations or [because you are working with] a young workforce … .”
Conclusion
Hospitalists can increase their capacities to observe, document, address, consult on, and refer instances of disruptive behavior appropriately. Although incidents of disruption may be relatively infrequent and may involve a few perpetrators, when they occur they should be addressed promptly and appropriately. Strategies to address the issue of disruptive behavior include conducting an organizational assessment; opening up lines of communication, including inviting nurses as well as physicians to submit anonymous notes or suggestions; and increasing staff awareness of the nature and severity of the issue.
As Dr. Flanders and colleagues have written, hospitalists should be the “fulcrum” we use to improve patient safety.10 The advantage of having just a few hospitalists influencing the healthcare of many patients can be a detriment if a colleague is a “problem doctor.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Rosenstein AH, O'Daniel M. Impact and implications of disruptive behavior in the perioperative arena. J Am Coll Surg. 2006 Jul;203(1):96-105. Epub 2006 Jun 5.
- Leape LL, Fromson JA. Problem doctors: is there a system-level solution? Ann Intern Med. 2006 Jan 17;144(2):107-115.
- Porto G, Lauve R. Disruptive clinician behavior: a persistent threat to patient safety. Patient Safety Qual Healthcare. 2006 Jul-Aug;3:16-24.
- Institute for Safe Medication Practice. Intimidation: practitioners speak up about this unresolved problem (Part I) ISMP Medication Safety Alert. Available at: www.ismp.org/MSAarticles/intimidation.htm. Accessed on October 16, 2006.
- Rosenstein AH, O'Daniel M. Disruptive behavior and clinical outcomes: perceptions of nurses and physicians. Am J Nurs. 2005 Jan;105(1):54-64; quiz 64-55.
- Leape LL. Physician self-examination. Int J Qual Health Care. 1998;10(4):289-290.
- Kohn L, Corrigan J, Donaldson M, eds. To Err is Human: Building a Safer Health System. Committee on Quality of Health Care in America, Institute of Medicine. Washington, DC: National Academies Press; 2000.
- Linney BJ. Confronting the disruptive physician. Physician Exec. 1997 Sep-Oct;23(7):55-58.
- Localio AR, Lawthers AG, Brennan TA, et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Flanders SA, Kaufman SR, Saint S. Hospitalists as emerging leaders in patient safety: targeting a few to affect many. J Patient Safety. 2005 Jun;1(2):78-82.
In a survey distributed to 50 member hospitals by Allen Rosenstein, MD, and his colleagues at VHA Inc. (an alliance of 2,400 nonprofit health care organizations) more than 1,500 participants responded to questions pertaining to their colleagues’ behavior.1 Of the 965 respondents to the question Have you ever witnessed disruptive behavior from a physician at your hospital?, nearly 68% said yes. Of the 675 nurses who responded to the question, 86% said they had witnessed it; almost half of the 249 physician respondents said they had witnessed it from their peers. Most respondents estimated the number of either nurses or physicians who exhibited disruptive behavior to be 1%-3%.
Of the 1,416 respondents who answered the question How often does physician disruptive behavior occur at your hospital?, 22% answered “weekly,” 26% answered “1 to 2 times per month,” and 33% answered “1 to 5 times per year.” Interestingly, 11% of the respondents said that such behavior by physicians never occurs, but 8% said it’s a daily occurrence.
—Scott Flanders, associate professor of medicine at the University of Michigan and director of the Hospitalist Program, Ann Arbor
Disruptive Behavior Defined
Disruptive behavior includes anything that interferes with the ability of a healthcare professional to effectively perform his or her duties or any behavior that undermines confidence in the hospital or its workers.2-4 In general, “disruptive” refers to behaviors that are abusive, disrespectful, sexual, angry, critical, negative, inappropriate, or unethical.2 (See “What Is Disruptive Behavior?” p. 40.) Individuals termed “impaired” are those who have active addictions or psychiatric problems and who exhibit the disruptive, intimidating, or abusive behavior.
Most respondents to the above-mentioned survey reported that disruptive behavior had negative or worsening effects on stress, frustration, concentration, communication, collaboration, information transfer, and workplace relationships. (See Figure 1, p. 41.)
“Physicians whose performance persistently falters pose a substantial threat to patient safety that is often unrecognized or unsatisfactorily addressed in hospitals and other healthcare organizations,” writes Lucian Leape, MD, adjunct professor of health policy in the Department of Health Policy and Management at the Harvard School of Public Health.2
“Whoever tells you that they have not experienced any kind of disruptive behavior is either lying or … in neglect, because there are always certain types of disruptive behaviors [among healthcare workers],” says Martin Izakovic, MD, medical director, Hospitalist Program, Mercy Hospital, Iowa City, Iowa.
Effects of Disruptive Behavior
Can we go so far as to say disruptive behavior affects clinical outcomes?
“It has to,” says Scott Flanders, MD, associate professor of medicine at the University of Michigan and director of the hospitalist program, Ann Arbor, and member of SHM’s board of directors. “People clearly understand the importance of teamwork in hospital medicine. If one member of the team is dysfunctional from an emotional intelligence/behavioral standpoint, that drags down the team in its entirety and impacts patient care.”
Providing safe and effective care should be the first priority of all healthcare professionals. Excellent outcomes have been associated with procedural efficiency and the use of evidence-based standards and tools designed to reduce the likelihood of medical error. The effects of work relationships on clinical outcomes are less well documented, but attention to the matter is increasing in parallel with the focus on patient safety.3,5
Dr. Leape, one of the founders of the National Patient Safety Foundation, devotes concerted energy to making organizations aware of the need to upgrade systems to diagnose and treat this problem.2 “Physician performance failures are not rare and pose substantial threats to patient welfare and safety,” he writes. “Few hospitals respond to such failures promptly or effectively. Failure to ensure the quality and safety of the performance of colleagues is a breach of medicine’s fiduciary responsibility to the public.”6
When it comes to the issues of behavior, besides monitoring their own performance, what do hospitalists do when they come up against colleagues whose shortcomings require correction in order for the entire institution to uphold its legal obligation to each patient?
Physician, Heal Thyself
A study published by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) reported that 24% of sentinel events could be attributed to problems referred to as human factors, including communication gaps, staffing issues, and lack of teamwork.2, 5 The March 2004 issue of the Institute for Safe Medication Practice’s (ISMP) Medication Safety Alert reported that 7% of medication errors could be attributed to nurses feeling intimidated by physicians.4 And, as a response to this growing problem, the Institute of Medicine’s groundbreaking report on medical errors and patient safety, To Err is Human, shifted the focus from individual blame to that of preventing errors through efforts to “design safety into systems.”7
Dr. Flanders, who is also associate chief for the Division of General Internal Medicine for Inpatient Programs at the University of Michigan Medical Center (Ann Arbor), certainly understands the need to grapple with these types of issues. He is a member of his institution’s interdisciplinary Medical Staff Quality Committee (MSQC), which works to get a better handle on individual physician-level quality and performance.
“A lot stems from JCAHO’s increased focus on institutions doing a better job of trying to figure out, in short, who’s a good doctor and who’s a bad doctor,” he says, “And having medical staff appointments, privileging, and assessment of clinical skills be something a little more robust than just asking four of your friends if they think you’re a good doctor.”
One of the charges of the MSQC is developing a better system of tracking physicians’ clinical skills down to the individual level, which Dr. Flanders says is a difficult task. But their second charge is even more elusive to track: examining “the range of daily activities, behaviors, and actions that encompass being a physician.” As part of that, the committee deals with interpersonal relations: interactions with other staff and behavioral issues.
Make the Diagnosis, Initiate Treatment
As with most academic medical centers, when someone at MSQC observes a behavioral issue, that person’s supervisor (often a department chair) is the next place for the buck to stop. There are clearly defined lines of communication and “very robust systems” to deal with these kinds of things, says Dr. Flanders.
MSQC is assisting department chairs in dealing with a particular behavior or problem. “It is a venue to vet particular problems and solutions,” he says. Ultimately, if there are repeated transgressions and administration is not satisfied that their directives have been followed, the committee can recommend revoking a physician’s medical staff privileges and implementing a remediation plan.
Those robust systems have not differed in medical institutions for the last 50 years. “I think what has changed is people are less willing to tolerate this persistently,” says Dr. Flanders. “People used to put up with the disruptive physician, the badly behaving physician, and if he was bringing in lots of research dollars or if he was a great scientist, [they’d be more likely to] accept bad behavior.”
With the increased risk of litigation and the increasing scrutiny on patient safety, these offenses can no longer be tolerated.8
At a community hospital, the hierarchies and channels of communication for handling behavioral issues are different. Because of the different atmosphere and mood of a hospitalist department, says Dr. Izakovic, who is also adjunct clinical assistant professor, Department of Internal Medicine, University of Iowa–Carver College of Medicine, Iowa City, “plus word of mouth, it is easier to either enforce or, even more, lead by example [such that] certain behaviors are [encouraged] and certain behavior types are suppressed.”
Michael Zavarin, MD, director of the hospitalist group at Jordan Hospital in Plymouth, Mass., agrees that the environment of a community hospital may be different enough so that handling disruptive behavior also occurs differently than it does in an academic medical center.
Dr. Zavarin’s group is composed of 6.5 full-time day hospitalists and one full-time night hospitalist, as well as two nurse practitioners. Disruptive behavior in his group “really hasn’t been an issue, so I guess it is [dealt with] on an as-needed basis,” he says, and he can only speculate that the proper channel for dealing with situations involving disruptive behavior would be his institution’s medical executive committee.
When Dr. Izakovic faces situations involving disruptive behavior, he says, it is generally an instance in which a hospitalist has “a good intention, but feels pressured by overwork or patient care circumstances, or [has] difficulty communicating or handling the nursing staff … who perceive [the physician’s behavior] as being either threatening or disrespectful or just not called for.”9
He estimates that these instances occur most often when a physician’s expectations are not met regarding duties being performed in a timely manner. Formal complaints are rarely made in his group—maybe two or three times a year. In those cases, he is responsible for formal follow-up, which requires having a one-on-one conversation with the physician and reporting back to the risk management department. But he prefers doing what is necessary to avoid a situation getting to that stage. Informal behavior-related events happen at least monthly, he estimates. “I’d rather hear earlier than later, with no formal complaint, no formal channel,” says Dr. Izakovic.
Blow the Whistle
What are the political ramifications of blowing the whistle on a disruptive colleague? The University of Michigan’s MSQC was created largely to help get at that issue and to create a place where such subjects can be brought up anonymously. [It can be done] if the reporting person wishes. In most situations, there has been a concerted effort against backlash just as there is when incidents and errors are reported to improve or maintain patient safety.
“As the patient safety culture changes, and I think it is changing, it’s going to facilitate culture change on this issue, too,” says Dr. Flanders, “because I think people are beginning to recognize, appropriately so, that some of these behavioral issues are safety issues.”
Do nurses feel comfortable reporting such instances? “I think it depends on the personality,” says Dr. Izakovic. “Some do, and some feel less comfortable; there are nurses who never complain and nurses who always complain, like doctors and everybody else. But I think that the climate is changing [so] that raising your voice and pointing toward deficiency and/or imperfection is becoming, if not [socially] acceptable, then [at least] a standard of behavior.”
Behavior, Safety, and Quality
“Communication is the key to success in today’s medicine,” says Dr. Izakovic. “Specifically among hospitalists: You communicate with the family physician, the patient, the referring specialist, or specialist that you called, the family, nurses, and patients all around the hospital.” And although communication is the most important part of the hospitalist’s practice, he says, “it sometimes leads to tension, and it’s not as much the message that you want to convey as the form [you use] and how it is transferred.”
Nurses are key stakeholders in reporting these behaviors, just as they are encouraged to report errors as an expression of their professionalism. Certainly, Dr. Flanders says, reporting a behavioral incident is “a lot more personal and less tangible than reporting a wrong dose on a medication.”
He has noticed a dramatic increase in the number of messages he receives about inappropriate or dangerous behavior among physicians. Everyone has a bad day from time to time, he says, but at the end of the year, “if I have one physician who has been mentioned 15 times, that helps me assess that person overall as a professional and be able to say, ‘Listen, there may be some red flags here’ and [then we can] begin to intervene and try to change that behavior.”
Effective systems employed to adequately address performance problems should be fair, objective, and responsive, writes Dr. Leape.2,6 Strategies available to handle incidents of disruptive behavior include adopting performance standards for behavior as well as competence. All physicians should be required to acknowledge in writing that they have read and understood these standards and that persistent failure to uphold them will result in loss of clinical privileges. Adherence to standards should be monitored annually and provided confidentially to each individual. Finally, assessment and treatment programs must be available to manage all the underlying causes of sub-par performance. The long-term objective is to enable physicians to continue to practice, as opposed to attempting to “weed them out.”
Prevention
According to Balazs Zsenits, MD, director, Division of Hospital Medicine at Rochester General Hospital, Rochester, N.Y., two mechanisms should be applied when discussing the prevention of disruptive behavior.
“First, physician selection should be conducted by a thorough interview process,” he says, “including at least a full-day face-to-face interview, discussion with previous employers, assessment of team-participation experience, and communication skills.”
Also, you need to clarify your expectations by means of “written policies, leading by example, promoting this culture in meetings, etc., and proactively monitoring performance,” says Dr. Zsenits. That means talking with doctors, nurses, and families and actively looking for feedback. “This process is time-intensive and may be under-recognized during resource allocation, but I believe it is a tool that may prevent this and many other common problems from growing out of control.”
A director of a hospital medicine group may have to deal with the perception of an escalating number of complaints about physician behaviors. “The growth of a hospitalist program that goes from seeing a small fraction of patients within a hospital to seeing the majority of medical admissions creates challenges beyond just simply managing the increased number of doctors and complaints,” says Dr. Zsenits. “Our co-workers and stakeholders might develop an impression that ‘most doctor problems’ in the hospital are related to the hospitalists. Even if this is [because] the hospitalists actually take care of most patients in house, and each hospitalist takes care of many more patients than private attendings used to, avoiding the perception that this single group is associated with most complaints is a difficult task.”
Although hospitalists’ focus on teamwork and quality of care may improve the actual statistics, he adds, “some factors may create more feedback, including more complaints; for example, being new docs to patients and relatives at times of stress, and having a closer working relationship with nurses, which may [be problematic] by creating heightened expectations or [because you are working with] a young workforce … .”
Conclusion
Hospitalists can increase their capacities to observe, document, address, consult on, and refer instances of disruptive behavior appropriately. Although incidents of disruption may be relatively infrequent and may involve a few perpetrators, when they occur they should be addressed promptly and appropriately. Strategies to address the issue of disruptive behavior include conducting an organizational assessment; opening up lines of communication, including inviting nurses as well as physicians to submit anonymous notes or suggestions; and increasing staff awareness of the nature and severity of the issue.
As Dr. Flanders and colleagues have written, hospitalists should be the “fulcrum” we use to improve patient safety.10 The advantage of having just a few hospitalists influencing the healthcare of many patients can be a detriment if a colleague is a “problem doctor.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Rosenstein AH, O'Daniel M. Impact and implications of disruptive behavior in the perioperative arena. J Am Coll Surg. 2006 Jul;203(1):96-105. Epub 2006 Jun 5.
- Leape LL, Fromson JA. Problem doctors: is there a system-level solution? Ann Intern Med. 2006 Jan 17;144(2):107-115.
- Porto G, Lauve R. Disruptive clinician behavior: a persistent threat to patient safety. Patient Safety Qual Healthcare. 2006 Jul-Aug;3:16-24.
- Institute for Safe Medication Practice. Intimidation: practitioners speak up about this unresolved problem (Part I) ISMP Medication Safety Alert. Available at: www.ismp.org/MSAarticles/intimidation.htm. Accessed on October 16, 2006.
- Rosenstein AH, O'Daniel M. Disruptive behavior and clinical outcomes: perceptions of nurses and physicians. Am J Nurs. 2005 Jan;105(1):54-64; quiz 64-55.
- Leape LL. Physician self-examination. Int J Qual Health Care. 1998;10(4):289-290.
- Kohn L, Corrigan J, Donaldson M, eds. To Err is Human: Building a Safer Health System. Committee on Quality of Health Care in America, Institute of Medicine. Washington, DC: National Academies Press; 2000.
- Linney BJ. Confronting the disruptive physician. Physician Exec. 1997 Sep-Oct;23(7):55-58.
- Localio AR, Lawthers AG, Brennan TA, et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Flanders SA, Kaufman SR, Saint S. Hospitalists as emerging leaders in patient safety: targeting a few to affect many. J Patient Safety. 2005 Jun;1(2):78-82.
In a survey distributed to 50 member hospitals by Allen Rosenstein, MD, and his colleagues at VHA Inc. (an alliance of 2,400 nonprofit health care organizations) more than 1,500 participants responded to questions pertaining to their colleagues’ behavior.1 Of the 965 respondents to the question Have you ever witnessed disruptive behavior from a physician at your hospital?, nearly 68% said yes. Of the 675 nurses who responded to the question, 86% said they had witnessed it; almost half of the 249 physician respondents said they had witnessed it from their peers. Most respondents estimated the number of either nurses or physicians who exhibited disruptive behavior to be 1%-3%.
Of the 1,416 respondents who answered the question How often does physician disruptive behavior occur at your hospital?, 22% answered “weekly,” 26% answered “1 to 2 times per month,” and 33% answered “1 to 5 times per year.” Interestingly, 11% of the respondents said that such behavior by physicians never occurs, but 8% said it’s a daily occurrence.
—Scott Flanders, associate professor of medicine at the University of Michigan and director of the Hospitalist Program, Ann Arbor
Disruptive Behavior Defined
Disruptive behavior includes anything that interferes with the ability of a healthcare professional to effectively perform his or her duties or any behavior that undermines confidence in the hospital or its workers.2-4 In general, “disruptive” refers to behaviors that are abusive, disrespectful, sexual, angry, critical, negative, inappropriate, or unethical.2 (See “What Is Disruptive Behavior?” p. 40.) Individuals termed “impaired” are those who have active addictions or psychiatric problems and who exhibit the disruptive, intimidating, or abusive behavior.
Most respondents to the above-mentioned survey reported that disruptive behavior had negative or worsening effects on stress, frustration, concentration, communication, collaboration, information transfer, and workplace relationships. (See Figure 1, p. 41.)
“Physicians whose performance persistently falters pose a substantial threat to patient safety that is often unrecognized or unsatisfactorily addressed in hospitals and other healthcare organizations,” writes Lucian Leape, MD, adjunct professor of health policy in the Department of Health Policy and Management at the Harvard School of Public Health.2
“Whoever tells you that they have not experienced any kind of disruptive behavior is either lying or … in neglect, because there are always certain types of disruptive behaviors [among healthcare workers],” says Martin Izakovic, MD, medical director, Hospitalist Program, Mercy Hospital, Iowa City, Iowa.
Effects of Disruptive Behavior
Can we go so far as to say disruptive behavior affects clinical outcomes?
“It has to,” says Scott Flanders, MD, associate professor of medicine at the University of Michigan and director of the hospitalist program, Ann Arbor, and member of SHM’s board of directors. “People clearly understand the importance of teamwork in hospital medicine. If one member of the team is dysfunctional from an emotional intelligence/behavioral standpoint, that drags down the team in its entirety and impacts patient care.”
Providing safe and effective care should be the first priority of all healthcare professionals. Excellent outcomes have been associated with procedural efficiency and the use of evidence-based standards and tools designed to reduce the likelihood of medical error. The effects of work relationships on clinical outcomes are less well documented, but attention to the matter is increasing in parallel with the focus on patient safety.3,5
Dr. Leape, one of the founders of the National Patient Safety Foundation, devotes concerted energy to making organizations aware of the need to upgrade systems to diagnose and treat this problem.2 “Physician performance failures are not rare and pose substantial threats to patient welfare and safety,” he writes. “Few hospitals respond to such failures promptly or effectively. Failure to ensure the quality and safety of the performance of colleagues is a breach of medicine’s fiduciary responsibility to the public.”6
When it comes to the issues of behavior, besides monitoring their own performance, what do hospitalists do when they come up against colleagues whose shortcomings require correction in order for the entire institution to uphold its legal obligation to each patient?
Physician, Heal Thyself
A study published by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) reported that 24% of sentinel events could be attributed to problems referred to as human factors, including communication gaps, staffing issues, and lack of teamwork.2, 5 The March 2004 issue of the Institute for Safe Medication Practice’s (ISMP) Medication Safety Alert reported that 7% of medication errors could be attributed to nurses feeling intimidated by physicians.4 And, as a response to this growing problem, the Institute of Medicine’s groundbreaking report on medical errors and patient safety, To Err is Human, shifted the focus from individual blame to that of preventing errors through efforts to “design safety into systems.”7
Dr. Flanders, who is also associate chief for the Division of General Internal Medicine for Inpatient Programs at the University of Michigan Medical Center (Ann Arbor), certainly understands the need to grapple with these types of issues. He is a member of his institution’s interdisciplinary Medical Staff Quality Committee (MSQC), which works to get a better handle on individual physician-level quality and performance.
“A lot stems from JCAHO’s increased focus on institutions doing a better job of trying to figure out, in short, who’s a good doctor and who’s a bad doctor,” he says, “And having medical staff appointments, privileging, and assessment of clinical skills be something a little more robust than just asking four of your friends if they think you’re a good doctor.”
One of the charges of the MSQC is developing a better system of tracking physicians’ clinical skills down to the individual level, which Dr. Flanders says is a difficult task. But their second charge is even more elusive to track: examining “the range of daily activities, behaviors, and actions that encompass being a physician.” As part of that, the committee deals with interpersonal relations: interactions with other staff and behavioral issues.
Make the Diagnosis, Initiate Treatment
As with most academic medical centers, when someone at MSQC observes a behavioral issue, that person’s supervisor (often a department chair) is the next place for the buck to stop. There are clearly defined lines of communication and “very robust systems” to deal with these kinds of things, says Dr. Flanders.
MSQC is assisting department chairs in dealing with a particular behavior or problem. “It is a venue to vet particular problems and solutions,” he says. Ultimately, if there are repeated transgressions and administration is not satisfied that their directives have been followed, the committee can recommend revoking a physician’s medical staff privileges and implementing a remediation plan.
Those robust systems have not differed in medical institutions for the last 50 years. “I think what has changed is people are less willing to tolerate this persistently,” says Dr. Flanders. “People used to put up with the disruptive physician, the badly behaving physician, and if he was bringing in lots of research dollars or if he was a great scientist, [they’d be more likely to] accept bad behavior.”
With the increased risk of litigation and the increasing scrutiny on patient safety, these offenses can no longer be tolerated.8
At a community hospital, the hierarchies and channels of communication for handling behavioral issues are different. Because of the different atmosphere and mood of a hospitalist department, says Dr. Izakovic, who is also adjunct clinical assistant professor, Department of Internal Medicine, University of Iowa–Carver College of Medicine, Iowa City, “plus word of mouth, it is easier to either enforce or, even more, lead by example [such that] certain behaviors are [encouraged] and certain behavior types are suppressed.”
Michael Zavarin, MD, director of the hospitalist group at Jordan Hospital in Plymouth, Mass., agrees that the environment of a community hospital may be different enough so that handling disruptive behavior also occurs differently than it does in an academic medical center.
Dr. Zavarin’s group is composed of 6.5 full-time day hospitalists and one full-time night hospitalist, as well as two nurse practitioners. Disruptive behavior in his group “really hasn’t been an issue, so I guess it is [dealt with] on an as-needed basis,” he says, and he can only speculate that the proper channel for dealing with situations involving disruptive behavior would be his institution’s medical executive committee.
When Dr. Izakovic faces situations involving disruptive behavior, he says, it is generally an instance in which a hospitalist has “a good intention, but feels pressured by overwork or patient care circumstances, or [has] difficulty communicating or handling the nursing staff … who perceive [the physician’s behavior] as being either threatening or disrespectful or just not called for.”9
He estimates that these instances occur most often when a physician’s expectations are not met regarding duties being performed in a timely manner. Formal complaints are rarely made in his group—maybe two or three times a year. In those cases, he is responsible for formal follow-up, which requires having a one-on-one conversation with the physician and reporting back to the risk management department. But he prefers doing what is necessary to avoid a situation getting to that stage. Informal behavior-related events happen at least monthly, he estimates. “I’d rather hear earlier than later, with no formal complaint, no formal channel,” says Dr. Izakovic.
Blow the Whistle
What are the political ramifications of blowing the whistle on a disruptive colleague? The University of Michigan’s MSQC was created largely to help get at that issue and to create a place where such subjects can be brought up anonymously. [It can be done] if the reporting person wishes. In most situations, there has been a concerted effort against backlash just as there is when incidents and errors are reported to improve or maintain patient safety.
“As the patient safety culture changes, and I think it is changing, it’s going to facilitate culture change on this issue, too,” says Dr. Flanders, “because I think people are beginning to recognize, appropriately so, that some of these behavioral issues are safety issues.”
Do nurses feel comfortable reporting such instances? “I think it depends on the personality,” says Dr. Izakovic. “Some do, and some feel less comfortable; there are nurses who never complain and nurses who always complain, like doctors and everybody else. But I think that the climate is changing [so] that raising your voice and pointing toward deficiency and/or imperfection is becoming, if not [socially] acceptable, then [at least] a standard of behavior.”
Behavior, Safety, and Quality
“Communication is the key to success in today’s medicine,” says Dr. Izakovic. “Specifically among hospitalists: You communicate with the family physician, the patient, the referring specialist, or specialist that you called, the family, nurses, and patients all around the hospital.” And although communication is the most important part of the hospitalist’s practice, he says, “it sometimes leads to tension, and it’s not as much the message that you want to convey as the form [you use] and how it is transferred.”
Nurses are key stakeholders in reporting these behaviors, just as they are encouraged to report errors as an expression of their professionalism. Certainly, Dr. Flanders says, reporting a behavioral incident is “a lot more personal and less tangible than reporting a wrong dose on a medication.”
He has noticed a dramatic increase in the number of messages he receives about inappropriate or dangerous behavior among physicians. Everyone has a bad day from time to time, he says, but at the end of the year, “if I have one physician who has been mentioned 15 times, that helps me assess that person overall as a professional and be able to say, ‘Listen, there may be some red flags here’ and [then we can] begin to intervene and try to change that behavior.”
Effective systems employed to adequately address performance problems should be fair, objective, and responsive, writes Dr. Leape.2,6 Strategies available to handle incidents of disruptive behavior include adopting performance standards for behavior as well as competence. All physicians should be required to acknowledge in writing that they have read and understood these standards and that persistent failure to uphold them will result in loss of clinical privileges. Adherence to standards should be monitored annually and provided confidentially to each individual. Finally, assessment and treatment programs must be available to manage all the underlying causes of sub-par performance. The long-term objective is to enable physicians to continue to practice, as opposed to attempting to “weed them out.”
Prevention
According to Balazs Zsenits, MD, director, Division of Hospital Medicine at Rochester General Hospital, Rochester, N.Y., two mechanisms should be applied when discussing the prevention of disruptive behavior.
“First, physician selection should be conducted by a thorough interview process,” he says, “including at least a full-day face-to-face interview, discussion with previous employers, assessment of team-participation experience, and communication skills.”
Also, you need to clarify your expectations by means of “written policies, leading by example, promoting this culture in meetings, etc., and proactively monitoring performance,” says Dr. Zsenits. That means talking with doctors, nurses, and families and actively looking for feedback. “This process is time-intensive and may be under-recognized during resource allocation, but I believe it is a tool that may prevent this and many other common problems from growing out of control.”
A director of a hospital medicine group may have to deal with the perception of an escalating number of complaints about physician behaviors. “The growth of a hospitalist program that goes from seeing a small fraction of patients within a hospital to seeing the majority of medical admissions creates challenges beyond just simply managing the increased number of doctors and complaints,” says Dr. Zsenits. “Our co-workers and stakeholders might develop an impression that ‘most doctor problems’ in the hospital are related to the hospitalists. Even if this is [because] the hospitalists actually take care of most patients in house, and each hospitalist takes care of many more patients than private attendings used to, avoiding the perception that this single group is associated with most complaints is a difficult task.”
Although hospitalists’ focus on teamwork and quality of care may improve the actual statistics, he adds, “some factors may create more feedback, including more complaints; for example, being new docs to patients and relatives at times of stress, and having a closer working relationship with nurses, which may [be problematic] by creating heightened expectations or [because you are working with] a young workforce … .”
Conclusion
Hospitalists can increase their capacities to observe, document, address, consult on, and refer instances of disruptive behavior appropriately. Although incidents of disruption may be relatively infrequent and may involve a few perpetrators, when they occur they should be addressed promptly and appropriately. Strategies to address the issue of disruptive behavior include conducting an organizational assessment; opening up lines of communication, including inviting nurses as well as physicians to submit anonymous notes or suggestions; and increasing staff awareness of the nature and severity of the issue.
As Dr. Flanders and colleagues have written, hospitalists should be the “fulcrum” we use to improve patient safety.10 The advantage of having just a few hospitalists influencing the healthcare of many patients can be a detriment if a colleague is a “problem doctor.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Rosenstein AH, O'Daniel M. Impact and implications of disruptive behavior in the perioperative arena. J Am Coll Surg. 2006 Jul;203(1):96-105. Epub 2006 Jun 5.
- Leape LL, Fromson JA. Problem doctors: is there a system-level solution? Ann Intern Med. 2006 Jan 17;144(2):107-115.
- Porto G, Lauve R. Disruptive clinician behavior: a persistent threat to patient safety. Patient Safety Qual Healthcare. 2006 Jul-Aug;3:16-24.
- Institute for Safe Medication Practice. Intimidation: practitioners speak up about this unresolved problem (Part I) ISMP Medication Safety Alert. Available at: www.ismp.org/MSAarticles/intimidation.htm. Accessed on October 16, 2006.
- Rosenstein AH, O'Daniel M. Disruptive behavior and clinical outcomes: perceptions of nurses and physicians. Am J Nurs. 2005 Jan;105(1):54-64; quiz 64-55.
- Leape LL. Physician self-examination. Int J Qual Health Care. 1998;10(4):289-290.
- Kohn L, Corrigan J, Donaldson M, eds. To Err is Human: Building a Safer Health System. Committee on Quality of Health Care in America, Institute of Medicine. Washington, DC: National Academies Press; 2000.
- Linney BJ. Confronting the disruptive physician. Physician Exec. 1997 Sep-Oct;23(7):55-58.
- Localio AR, Lawthers AG, Brennan TA, et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Flanders SA, Kaufman SR, Saint S. Hospitalists as emerging leaders in patient safety: targeting a few to affect many. J Patient Safety. 2005 Jun;1(2):78-82.